Embed Size (px)
Citation preview

at SciVerse ScienceDirect
Atherosclerosis 226 (2013) 291e295
Contents lists available
Atherosclerosis
journal homepage: www.elsevier .com/locate/atherosclerosis
Subclinical atherosclerosis and hyperandrogenemia are independent risk factorsfor increased epicardial fat thickness in patients with PCOS and idiopathichirsutism
Evrim Cakir a,*, Mehmet Do�gan b, Oya Topaloglu a, Mustafa Ozbek a, Erman Cakal a,Mustafa Gokhan Vural a, Ekrem Yeter b, Tuncay Delibasi a
aDepartment of Endocrinology and Metabolic Diseases, Diskapi Training and Research Hospital, Demetevler 1. cadde, 81-10, Altindag, TR-06200, Ankara, TurkeybDepartment of Cardiology, Diskapi Training and Research Hospital, Ankara, Turkey
a r t i c l e i n f o
Article history:Received 13 September 2012Received in revised form2 November 2012Accepted 5 November 2012Available online 15 November 2012
Keywords:Polycystic ovary syndromeEpicardial fat thicknessCarotid intima-media thicknessInsulin resistanceCardiovascular disease risk
* Corresponding author. Tel.: þ90 505 2692468; faE-mail address: [email protected] (E. Cakir
0021-9150/$ e see front matter � 2012 Elsevier Irelahttp://dx.doi.org/10.1016/j.atherosclerosis.2012.11.004
a b s t r a c t
Objective: Polycystic ovary syndrome (PCOS) is one of the most common endocrine disorders affectingreproductive-age women and is reported to be associated with an increased risk of cardiovasculardisease and early atherosclerosis. Epicardial fat thickness (EF) is clinically related to subclinical athero-sclerosis and visceral fat changes. Therefore, the objective of this study is to compare the carotid arteryintima-media thickness (CIMT), EF and cardiometabolic risk factors in patients with PCOS, patients withidiopathic hirsutism (IH) and healthy controls.Methods: This cross-sectional controlled study was conducted in a training and research hospital. Thestudy population consisted of 50 reproductive-age PCOS women, 34 women with IH and 39 controlsubjects. We evaluated anthropometric, hormonal and metabolic parameters as well as CIMT and EFmeasurements in PCOS patients, IH patients and controls.Results: The mean fasting insulin, HOMA-IR, hsCRP, GGT, CIMT, and EF levels were significantly higher inpatients with PCOS and IH (p < 0.05). A significant positive correlation was found between EF and age,BMI, WHR, Ferriman Gallwey score (FG), fasting insulin, HOMA-IR, triglyceride, total cholesterol, LDL-C,17 OH progesterone, free testosterone, CIMT, hsCRP, and GGT, whereas a significant negative correlationwas observed between EF and HDL-C (p < 0.05). In the multiple linear regression analyses, EF was foundto be associated with the FG (b coefficient: 0.389, p < 0.001), CIMT (b coefficient: 0.376, p < 0.001) andfree testosterone levels (b coefficient: 0.173, p < 0.038).Conclusion: EF appears to be a marker that will enable the detection of the cardiometabolic response inpatients with PCOS and IH, even at an early stage.
� 2012 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Polycystic ovary syndrome (PCOS) is one of the most commonendocrine disorder affecting at least 5e10% of women ofreproductive age [1]. PCOS is characterized by hyperandrogenism,menstrual disturbance, anovulation, infertility and obesity [2] andis reported to be associated with an increased risk of cardiovasculardisease (CVD) [3] and early atherosclerosis [4]. Hyperinsulinemiaand insulin resistance are frequent findings in PCOS patients andhave relationships with low-grade chronic inflammation [5] andthe increased risk of CVD [6].
Idiopathic hirsutism (IH) is diagnosed in patients with hirsutismwho have normal menstrual cycles, normal serum androgenconcentrations and no identifiable cause of hirsutism [7].
x: þ90 3123368920.).
nd Ltd. All rights reserved.
Epicardial fat thickness (EF) is clinically related to abdominalvisceral adiposity, coronary artery disease, subclinical atheroscle-rosis, cardiac morphology, and visceral fat changes during weightloss intervention. Additionally, the EF has been shown to bea metabolically active organ and a source of several bioactive adi-pokines [8e11].
The aim of this study is to evaluate the EF measurement and itsassociation between cardiometabolic factors in patients with PCOSand IH.
2. Materials and methods
We studied 50 patients with PCOS, 34 patients with IH and 39age- and body mass index (BMI)-matched healthy controls. Theprotocol was approved by the local ethics committee. All patientsgave written consent. All patients were female and non-smokers.

E. Cakir et al. / Atherosclerosis 226 (2013) 291e295292
The diagnosis of PCOS was made according to the RotterdamEuropean Society for Human Reproduction and Embryology/American Society for Reproductive Medicineesponsored PCOSConsensus Workshop Group [12]. The revised diagnostic criteria ofPCOS are as follows, with at least two of the following beingrequired:
1. Oligo and/or anovulation that is a menstrual disturbance2. Clinical and/or biochemical signs of hyperandrogenism3. Polycystic ovarian appearance on ultrasound
The hirsute patients with normal, regular menstrual cyclesand normal circulating androgen levels were classified as havingIH [7].
Those participants who had a smoking history, diabetes melli-tus, hyperprolactinemia, congenital adrenal hyperplasia, androgen-secreting tumors, thyroid disorders, Cushing syndrome (as deter-mined by a 1 mg dexamethasone suppression test), infectiousdisease, hypertension, or hepatic or renal dysfunction wereexcluded from the study. Patients were also excluded if they hadused confoundingmedications, including oral contraceptive agents,antilipidemic drugs, hypertensive medications, and insulin-sensitizing drugs, within 3 months before enrollment.
The control group (n ¼ 39) consisted of healthy patients whowere admitted to the check-up unit without any systemic disorder.All of the women in the control group had a hirsutism score of <8.All women in the control group had regular menses, every 21e35days. None of the women in the control group had polycysticovaries on ultrasound.
Weight and height were measured in light clothing withoutshoes. The BMI was calculated by dividing the weight by the squareof the height (kg/m2). Thewaist circumferencewasmeasured at thenarrowest level between the costal margin and iliac crest, and thehip circumference was measured at the widest level over thebuttocks while the subjects were standing and breathing normally.The waist-to-hip ratio (WHR) was then calculated.
The degree of hirsutism was determined by the FerrimaneGallwey (FG) score [13]. The BMI, WHR and hirsutism scores wereassessed by a single investigator for all of the subjects.
3. Echocardiographic EF measurement
All patients underwent 2D Doppler echocardiography witha Philips IE-33 system and S5-1 transducer (1e5 mHz, Philips,Bothell, WA, USA). Echocardiographically, EF is generally identifiedas the relatively echo-free space between the outer wall of themyocardium and the visceral layer of the pericardium; its thick-ness is measured perpendicularly on the free wall of the rightventricle at end-systole in 3 cardiac cycles. Because it iscompressed during diastole, the EF thickness is best measured atend-systole at the point on the free wall of the right ventricle atwhich the ultrasound beam is oriented in a perpendicular manner,using the aortic annulus as an anatomic landmark. The averagevalue of 3 cardiac cycles from each echocardiographic view wasdetermined [8].
4. Measurement of Carotid Intima-Media Thickness (CIMT)
CIMT was derived from a non-invasive ultrasound of thecommon carotid arteries, using a high-resolution ultrasoundmachine (Sonoline G 40, Siemens) with a 7.5 MHz mechanicalsector transducer. The intima-media thickness was defined as thedistance between the blood-intima and media-adventitia bound-aries on B-mode imaging.
4.1. Biochemical evaluation
Venous blood samples were obtained in the follicular phase ofa spontaneous or progesterone-inducedmenstrual cycle. Before thestudy, blood samples were drawn from each patient after a 12 hovernight fasting for the determination of the hormones, lipidprofile, high-sensitive C- reactive protein (hs-CRP) levels, insulinlevels, and glucose levels.
Plasma glucose was determined by the glucose oxidase/peroxi-dase method (Gordion Diagnostic, Ankara, Turkey). The serum levelsof follicle-stimulating hormone (FSH) (normal range: 3e10.9 mIU/mL), luteinizing hormone (LH) (normal range: 2.1e12.8 mIU/mL),prolactin (normal range: 3.1e29.8 ng/mL), estradiol (normal range:18.9e246.7 pg/mL), dehydroepiandrosterone sulfate (DHEAS)(normal range: 35e430 mq/dL), total testosterone (T) (normal range:14.2e73.1 ng/dl), insulin (normal range: 3e25 mU/L), and thyroidstimulating hormone (TSH) (normal range: 0.5e4.78 mIU/L) weremeasured with specific electrochemiluminescence immunoassays(Elecsys 2010 Cobas, Roche Diagnostics, Mannheim, Germany).Serum 17 hydroxyprogesterone (17 OH progesterone) (normalrange: 0.1e2.5 ng/mL) and free testosterone (FT) (normal range: 1.1e3.3 pg/mL)weremeasured by radioimmunoassays. The levels of totalcholesterol, high density lipoprotein cholesterol (HDL-C), andtriglycerides (TG) were determined with enzymatic colorimetricassays by spectrophotometry (Bio Systems S.A., Barcelona, Spain).The low density lipoprotein cholesterol (LDL-C) level was calculatedusing the Friedewald formula.
Serum hs-CRP (normal range: 0e3 mg/L) was determined usinghigh-sensitivity CRP immunonephelometry (BN, Dade-Behring;Marburg, Germany). The cut-off value for hsCRP was taken as1.5 mg/L [14]. The homocysteine levels were assayed by a competi-tive immunoassay (Immulite 2000 XP) (normal range: 5e12 mmol/L).The gamma glutamyl transferase (GGT) (normal range: 0e38 U/L)levels were measured by a spectrophotometric technique.
Insulin resistance was calculated using the homeostasis modelassessment insulin resistance index (HOMA-IR) [15], according tothe following formula: fasting plasma glucose (mmol/L) � fastingserum insulin (mU/mL)/22.5. The cut-off value for HOMA-IR wastaken as 2.7 [16].
4.2. Statistical analyses
The collected data were entered into SPSS version 17. Contin-uous data were shown as means � SD. Chi-squared tests were usedto compare differences in rates. Normally distributed variableswere compared using the Student T test. Data that were not nor-mally distributed were compared by the MannWhitney U test. Thedata are expressed as means � SD or medians with interquartileranges as appropriate. The degree of association between variableswas calculated by the Pearson correlation coefficient or Spearmanrank correlation coefficient. The multiple linear regression usingthe enter method was used to adjust the EF with respect to age andBMI. A p value lower than 0.05 was accepted as statisticallysignificant, and all computed p values were two-tailed.
5. Results
Clinical and endocrinological parameters were screened in thepatients with PCOS and IH and in the healthy control subjects(Table 1).We studied 50 patients with PCOS (mean age 22.56� 3.88years, range 18e33 years; BMI, 25.32 � 4.33 kg/m2), 34 patientswith IH (mean age 23.14 � 5.60 years, range 18e33 years; BMI,25.36 � 5.36 kg/m2) and 39 age- and BMI-matched healthy controlgroup (mean age 22.82 � 4.35 years, range 18e32 years; BMI,23.30 � 3.36 kg/m2).

Table 1The biochemical data in polycystic ovary syndrome (PCOS) patients, idiopathichirsutism patients and healthy controls.a
PCOS Idiopathichirsutism
Control P
(n ¼ 50) (n ¼ 34) (n ¼ 39)
Glucose, mg/dL 84.70 � 8.92 86.64 � 8.86 88.00 � 8.91 0.218_Insülin, m IU/mL 15.57 � 9.2# 16.01 � 8.77# 10.26 � 5.26U 0.003HOMA-IR 3.27 � 2.04# 3.45 � 1.94# 2.25 � 1.04U 0.007Total cholesterol,
mg/dL167.5 � 26.9 165.2 � 38.5 157.3 � 27.3 0.289
Triglyceride, mg/dL 99.5(24e287) # 94(35e245) # 69(35e323) U 0.010HDL-C, mg/dL 49.64 � 12.91# 46.39 � 8.73# 54.05 � 14.00U 0.032LDL-C, mg/dL 95.74 � 23.54 86.53 � 24.18 86.53 � 24.18 0.173hsCRP, mg/L 2.12 � 1.84# 1.92 � 1.71# 1.17 � 1.39U 0.027Homocysteine,
mmol/L10.47 � 5.72 12.72 � 5.23 11.34 � 7.83 0.290
GGT, U/L 11(1e95) # 14.5(2e47) # 7.5(3e27) U 0.001
HOMA-IR: homeostasis model assessment insulin resistance index; HDL-C: highdensity lipoprotein cholesterol; LDL-C: Low density lipoprotein cholesterol; hs-CRP:high-sensitive C- reactive protein; GGT: gamma glutamyltransferase.
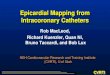
a Different symbols in each row indicate significantly different groups.Fig. 1. The mean epicardial fat thickness between groups EF: Epicardial fat thickness,PCOS: Policystic ovary syndrome, IH: Idiopathic hirsutism.
E. Cakir et al. / Atherosclerosis 226 (2013) 291e295 293
5.1. Comparing parameters between groups
The mean fasting insulin, HOMA-IR, TG, FT, T, 17 OH proges-terone, DHEAS, hsCRP, GGT, CIMT, and EF levels were significantlyhigher and the estradiol and HDL levels were significantly lower inthe patients with PCOS and IH (p < 0.05) (Table 2). The highest EFand CIMT values were observed in the IH patients. Although thedifferences were significantly higher compared with the controlgroup (p < 0.001 for both EF and CIMT), these values were notsignificantly different between the PCOS and IH groups (p¼ 0.84 forEF and p ¼ 0.57 for CIMT) (Figs. 1 and 2).
5.2. The correlations between EF, CIMT and cardiometabolicparameters
A significant positive correlation was found between the EF andage, BMI, WHR, FG, fasting insulin, HOMA-IR, TG, total cholesterol,LDL-C, 17 OH progesterone, FT, CIMT, hsCRP, and GGT, whereasa significant negative correlation was found between the EF andHDL-C.
5.3. Comparing the EF and CIMT measurements in groups based onthe HOMA-IR and hsCRP levels and the FG score
The participants were divided into 2 groups according to theHOMA-IR levels. The cut-off point was 2.7 [16]. Those participants
Table 2The hormonal data in polycystic ovary syndrome (PCOS) patients, idiopathic hirsutism p
PCOS Idi
(n ¼ 50) (n
TSH, mIU/L 1.9(0.45e4.5) 1.7FSH, mIU/mL 5.31 � 1.88 5.7LH, mIU/mL 6.01 � 2.69 5.4Estradiol, pg/mL 49(10e164) # 51PRL, ng/mL 9.95(10.8e45) 9.2Free testosterone, pg/mL 2.64 � 1.31# 2.2Total testosterone, ng/mL 58.46 � 18.28# 5217-OH progesterone, ng/mL 1.49(0.1e5.1) # 1.2DHEAS, mq/dL 255.9 � 135.9# 25CIMT, mm 4.44 � 0.66# 4.5EF, mm 4.61 � 1.22# 4.7
TSH: thyroid stimulating hormone; FSH: follicle-stimulating hormone; LH: luteinizing hormedia thickness; EF: epicardial fat thickness.
a Different symbols in each row indicate significantly different groups.
who had an HOMA-IR greater than 2.7 had significantly higher EFand CIMT measurements. Additionally, the EF and CIMT measure-ments were higher in the groups with a higher FG score (FG score�8) and higher hsCRP level. The hsCRP cut-off value was 1.5 mg/L,based on the study by Kilic et al., which included Turkish pop-ulation values [14] (Table 3).
5.4. Multiple linear regression analyses
After adjusting for age and BMI with multiple linear regressionanalyses, the EF level was positively correlated with FG, FT andCIMT (p < 0.05) (Table 4). CIMT was obtained as an independentrisk factor for EF (Fig. 3).
6. Discussion
The results of the present study demonstrate that the mean EFand CIMT levels were higher in patients with PCOS and IH.Furthermore, the EF showed an independent association with FT,CIMT and FG. The EF also showed significant correlations withcardiometabolic parameters independently of age and BMI.
A recent sub-study of the Women’s Ischemia Evaluation Study(WISE) [17] showed that women with PCOS had an increasednumber of cardiovascular events. In this study, CVDwas found to bepositively correlated with FT. In addition, the event-free survival(including fatal and nonfatal events) was significantly lower in
atients and healthy controls.a
opathic hirsutism Control P
¼ 34) (n ¼ 39)
5(0.84e5.18) 1.63(0.5e3.9) 0.2368 � 1.96 5.79 � 2.04 0.4282 � 2.66 5.23 � 2.48 0.349(11.9e164) # 65(7e217)U <0.001(4.7e35) 10.6(1e26) 0.990 � 0.99# 1.38 � 0.51U <0.001.60 � 17.12# 42.42 � 13.29U <0.001(0.13e4.2) #U 0.9(0.1e4.5)U 0.014.4 � 110.1# 173.46 � 71.59U 0.0017 � 0.56# 3.76 � 0.47U <0.0015 � 1.34# 2.94 � 0.88U <0.001
mone; PRL: prolactin DHEAS: dehydroepiandrosterone sulfate; CIMT: carotid intima

Table 4Results of the multiple linear regression analyze.
Independent variables Model coefficient P
B Std. Error
(Constant) �2.735 1.775 0.126Age 0.017 0.023 0.459BMI 0.022 0.031 0.491WHR �0.114 1.842 0.951FG 0.089 0.018 0.000Insulin 0.070 0.064 0.274HOMA-IR �0.370 0.280 0.189Triglyceride 0.001 0.003 0.628Total cholesterol �0.004 0.009 0.626LDL-C 0.012 0.009 0.201Free testosterone 0.018 0.010 0.020CIMT 0.739 0.204 0.000hsCRP 0.044 0.072 0.537GGT 0.004 0.009 0.668
Dependent variable: EF.BMI: Body mass index; WHR: Waist hip ratio; FG: Ferriman Gallwey score; HOMA-IR: homeostasis model assessment insulin resistance index; LDL-C: Low densitylipoprotein cholesterol; CIMT: carotid intima media thickness; hs-CRP: high-sensitive C- reactive protein; GGT: gamma glutamyltransferase. P values > 0.05 (inbold) predict the independent risk factors for EF.
Fig. 2. Carotid intima media thickness between groups.
E. Cakir et al. / Atherosclerosis 226 (2013) 291e295294
PCOS women compared with non-PCOS women. In the presentstudy, cardiometabolic parameters including HOMA-IR, TG, FT,DHEAS, GGT, hsCRP and CIMT, were significantly higher in patientswith PCOS and IH and were positively correlated with the EF.
Furthermore, the CVD risk markers, including insulin, HOMA-IR,homocysteine, EF and CIMT levels, were found to be higher in the IHpatients compared with the PCOS patients, although these differ-ences were not significant. These increases are thought to be due tothe effects of increased androgen sensitivity, such as hyper-androgenemia, on CVD risk. Additionally, an FG score that reflectsandrogen effects showed an independent association with the EF.
In the study by Victor et al., an association was found betweeninsulin resistance and impaired endothelial and mitochondrialoxidative metabolism. They concluded that the inflammatory stateis related to insulin resistance in PCOS patients and that this stateaffects endothelial function [18]. In the current study, hsCRP levelsand insulin resistance were positively correlated with the EF,consistent with this hypothesis.
There are few studies about pathophysiology and the role of EFon coronary atherosclerosis. The EF tissue has been shown to causesome cytokine secretion and protein expression [11,19]. The level ofEF in women with known coronary heart disease was correlatedwith the severity of the disorder [20,21].
A recent study showed that EF was positively correlated withthe scoring of diseased coronary arteries, low-density lipoprotein
Table 3The comparison of the epicardial fat thickness and carotid intimamedia thickness inthe FG, HOMA-IR and hsCRP groups.
Variable CIMT P EF P
Mean � Standarddeviation
Mean � Standarddeviation
FG<8 3.87 � 0.54 <0.001 3.18 � 1.11 <0.001�8 4.51 � 0.62 4.74 � 1.23HOMA-IR<2.7 4.00 � 0.56 <0.001 3.72 � 1.37 <0.001�2.7 4.56 � 0.67 4.49 � 1.30hsCRP<1.5 4.08 � 0.66 <0.001 3.86 � 1.40 0.011�1.5 4.53 � 0.61 4.52 � 1.34
cholesterol, BMI and serum TG levels, consistent with the presentstudy. In this study, the mean EF level was 5.4 � 1.9 mm in the CADgroup and 4.4 � 1.8 mm in the normal group (p ¼ 0.0001) [21].
A significant correlation was found between the EF and arterialstiffness measured by the cardio-ankle vascular index in a study byPark et al. [22]. In another study, EF was significantly associatedwith vascular risk factors and coronary calcification [23]. In somerecent studies, an elevated EF was shown to be an independent riskfactor for myocardial ischemia, obstructive coronary artery diseaseand coronary artery calcification [24e26]. The physiopathology ofthe role of EF in vascular disease is still unclear. However, it isthought to be due to the release of several proteins. The release ofapolipoprotein A-I and glutathione S-transferase Pwere found to besignificantly higher from the EF tissue [27]. In the present study, theEF was positively correlated with the CIMT, which is accepted asa marker for subclinical atherosclerosis, and CIMT was also shownto be an independent risk factor for an increased EF.
Fig. 3. The correlation between Epicardial Fat Thickness (EF) and Carotid Intima MediaThickness (CIMT).

E. Cakir et al. / Atherosclerosis 226 (2013) 291e295 295
Echocardiographic EF measurements provide some advantageswhen used to assess the cardiometabolic risk, being an objective,quantified, non-invasive, direct measurement of visceral fat tissueand a less expensive test than other techniques, such as magneticresonance or computerized tomography [28].
GGT has been reported to be related to the incidence of andmortality from cardiovascular diseases [29,30]. We observed thatthe GGT levels were higher in patients with PCOS and IH and werecorrelated with EF.
Epicardial fat might have a predictive role for detecting the car-diometabolic risk in potential diseases. Additionally, the EF measure-ment is a non-invasive tool and easy to perform to determine thecardiovascular risk in at-risk patients. A higher EF measurement hasbeen found to be associated with inflammation and cardiometabolicrisk. Clinical and biochemical hyperandrogenemia showed an inde-pendent association with the EF. Therefore, the EF appears to bea marker that will enable the detection of the cardiometabolicresponse in patients with PCOS and IH, even at an early stage.
Acknowledgments
Nothing to declare.
Appendix A. Supplementary material
Supplementary material related to this article can be found athttp://dx.doi.org/10.1016/j.atherosclerosis.2012.11.004.
References
[1] Norman RJ, Dewailly D, Legro RS, et al. Polycystic ovary syndrome. Lancet2007;370:685e97.
[2] Pasquali R, Gambineri A, Pagotto U. The impact of obesity on reproduction inwomen with polycystic ovary syndrome. BJOG 2006;113:1148e59.
[3] Orio Jr F, Palomba S, Spinelli L, et al. The cardiovascular risk of young womenwith polycystic ovary syndrome: an observational, analytical, prospectivecase-control study. J Clin Endocrinol Metab 2004;89:3696e701.
[4] Kelly CJ, Speirs A, Gould GW, et al. Altered vascular function in young womenwith polycystic ovary syndrome. J Clin Endocrinol Metab 2002;87:742e6.
[5] Escobar-Morreale HF, Luque-Ramirez M, San Millan JL. The molecular-geneticbasis of functional hyperandrogenism and the polycystic ovary syndrome.Endocr Rev 2005;26:251e82.
[6] Legro RS. Polycystic ovary syndrome and cardiovascular disease: a prematureassociation? Endocr Rev 2003;24:302e12.
[7] Azziz R, Carmina E, Sawaya ME. Idiopathic hirsutism. Endocr Rev 2000;21:347e62.
[8] Iacobellis G, Assael F, Ribaudo MC, et al. Epicardial fat from echocardiog-raphy: a new method for visceral adipose tissue prediction. Obes Res 2003;11:304e10.
[9] Iacobellis G, Ribaudo MC, Zappaterreno A, et al. Relation between epicardialadipose tissue and left ventricular mass. Am J Cardiol 2004;94:1084e7.
[10] Jeong JW, Jeong MH, Yun KH, et al. Echocardiographic epicardial fat thicknessand coronary artery disease. Circ J 2007;71:536e9.
[11] Mazurek T, Zhang L, Zalewski A, et al. Human epicardial adipose tissue isa source of inflammatory mediators. Circulation 2003;108:2460e6.
[12] Revised 2003 consensus on diagnostic criteria and long-term health risksrelated to polycystic ovary syndrome. Fertil Steril 2004;81:19e25.
[13] Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women.J Clin Endocrinol Metab 1961;21:1440e7.
[14] Kilic T, Ural E, Oner G, et al. [Which cut-off value of high sensitivity C- reactiveprotein is more valuable for determining long- term prognosis in patientswith acute coronary syndrome?]. Anadolu Kardiyol Derg 2009;9:280e9.
[15] Matthews DR, Hosker JP, Rudenski AS, et al. Homeostasis model assessment:insulin resistance and beta-cell function from fasting plasma glucose andinsulin concentrations in man. Diabetologia 1985;28:412e9.
[16] Gokcel A, Ozsahin AK, Sezgin N, et al. High prevalence of diabetes in Adana,a southern province of Turkey. Diabetes Care 2003;26:3031e4.
[17] Shaw LJ, Bairey Merz CN, Azziz R, et al. Postmenopausal women with a historyof irregular menses and elevated androgen measurements at high risk forworsening cardiovascular event-free survival: results from the NationalInstitutes of HealtheNational Heart, Lung, and Blood Institute sponsoredWomen’s Ischemia Syndrome Evaluation. J Clin Endocrinol Metab 2008;93:1276e84.
[18] Victor VM, Rocha M, Banuls C, et al. Induction of oxidative stress and humanleukocyte/endothelial cell interactions in polycystic ovary syndrome patientswith insulin resistance. J Clin Endocrinol Metab 2011;96:3115e22.
[19] Iacobellis G, Pistilli D, Gucciardo M, et al. Adiponectin expression in humanepicardial adipose tissue in vivo is lower in patients with coronary arterydisease. Cytokines 2005;29:251e5.
[20] Baker AR, Silva NF, Quinn DW, et al. Human epicardial adipose tissueexpresses a pathogenic profile of adipocytokines in patients with cardiovas-cular disease. Cardiovasc Diabetol 2006;5:1.
[21] Shemirani H, Khoshavi M. Correlation of echocardiographic epicardial fatthickness with severity of coronary artery disease e an observational study.Anadolu Kardiyol Derg 2012;12:200e5.
[22] Park HE, Choi SY, Kim HS, Kim MK, Cho SH, Oh BH. Epicardial fat reflectsarterial stiffness: assessment using 256-slice multidetector coronarycomputed tomography and cardio-ankle vascular index. J Atheroscler Thromb2012;19:570e6.
[23] de Vos AM, Prokop M, Roos CJ, et al. Peri-coronary epicardial adipose tissue isrelated to cardiovascular risk factors and coronary artery calcification in post-menopausal women. Eur Heart J 2008;29:777e83.
[24] Nakazato R, Dey D, Cheng VY, et al. Epicardial fat volume and concurrentpresence of both myocardial ischemia and obstructive coronary arterydisease. Atherosclerosis 2012;221:422e6.
[25] Yerramasu A, Dey D, Venuraju S, et al. Increased volume of epicardial fat is anindependent risk factor for accelerated progression of sub-clinical coronaryatherosclerosis. Atherosclerosis 2012;220:223e30.
[26] Nakanishi R, Rajani R, Cheng VY, et al. Increase in epicardial fat volume isassociated with greater coronary artery calcification progression in subjects atintermediate risk by coronary calcium score: a serial study using non-contrastcardiac CT. Atherosclerosis 2011;218:363e8.
[27] Salgado-Somoza A, Teijeira-Fernandez E, Fernandez AL, et al. Changes in lipidtransport-involved proteins of epicardial adipose tissue associated withcoronary artery disease. Atherosclerosis 2012;224:492e9.
[28] Iacobellis G, Ribaudo MC, Assael F, et al. Echocardiographic epicardial adiposetissue is related to anthropometric and clinical parameters of metabolicsyndrome: a new indicator of cardiovascular risk. J Clin Endocrinol Metab2003;88:5163e8.
[29] Meisinger C, Doring A, Schneider A, et al. Serum gamma-glutamyltransferaseis a predictor of incident coronary events in apparently healthy men from thegeneral population. Atherosclerosis 2006;189:297e302.
[30] Hozawa A, Okamura T, Kadowaki T, et al. gamma-Glutamyltransferasepredicts cardiovascular death among Japanese women. Atherosclerosis 2007;194:498e504.














![Hirsutism (androgen excess) warda [compatibility mode]](https://img.pdfslide.net/doc/110x75/559d189d1a28ab64558b469c/hirsutism-androgen-excess-warda-compatibility-mode.jpg)