Embed Size (px)
Citation preview

Centre for Research Excellencein Integrated Quality Improvement
RE IQI....................
...........................
...............
.....................
.........................
.........
.......
Can Innovation Platform in
Indigenous Primary Health Care
Submission to ‘Closing the Gap Refresh’
April 2018

This submission was initially drafted by Jodie Bailie, Alison Laycock and Professor Ross Bailie, with further input provided by the listed signatories (see p.2). We acknowledge the active support, enthusiasm and commitment of both the founding members and the new partners and collaborators of the Centre for Research Excellence in Integrated Quality Improvement (CRE–IQI).
The CRE–IQI is funded by the National Health and Medical Research Council (Grant ID #1078927).
For more information, contact Professor Ross Bailie:
University Centre for Rural Health The University of Sydney 61 Uralba Street, Lismore, NSW 2480
E [email protected] T +61 2 6620 7231
CRE–IQI website http://www.ucrh.edu.au/cre-iqi/ Twitter @CRE_IQI

Centre for Research Excellence in Integrated Quality Improvement 1
Closing the Gap Refresh A Joint Initiative of the Council of Australian Governments Department of Prime Minister and Cabinet Australian Government, Canberra
This submission is made on behalf of the Centre for Research Excellence in Integrated Quality Improvement. The CRE–IQI is a national research collaboration that builds on decades of experience and commitment to improving Aboriginal and Torres Strait Islander health through strengthening comprehensive primary health care (PHC) delivery. This submission provides input to the Taskforce established in the Department of Prime Minister and Cabinet to refresh the Closing the Gap agenda.
Led by the University Centre for Rural Health, and funded by the National Health and Medical Research Council, the CRE–IQI (2014–2019) is a national, open collaboration between researchers, policy and service delivery partners who have a long-standing commitment to improving Aboriginal and Torres Strait Islander health. As a national collaboration, we aim to improve Aboriginal and Torres Strait Islander health outcomes by strengthening health systems through supporting the use of continuous quality improvement (CQI), a systematic way of using data to guide changes to increase the efficiency and effectiveness of organisational systems.
Evidence shows that using CQI to strengthen health systems in the Aboriginal and Torres Strait Islander PHC context is effective in improving health outcomes.1
We have collated and analysed CQI data provided by 175 Aboriginal and Torres Strait Islander PHC centres across Australia.2 This dataset includes more than 56,000 patient records in a number of areas of care including preventive health;3–5 maternal health;6–8 mental health and wellbeing;9 chronic illness care;10–13 rheumatic heart disease;14,15 sexual health;16 and child health.17,18 These CQI data provide the most comprehensive picture of the quality of PHC that Aboriginal and Torres Strait Islander people receive around Australia.19,20 Our collaboration makes a prominent contribution to original research on CQI in primary health care internationally, with more than 50 papers published in the peer-reviewed literature over the past 10 years.21
We are an open collaboration of many organisations working together to address the aims of the CRE–IQI and ultimately to improve health outcomes. Our submission is made on behalf almost 30 signatories from more than 10 academic institutions and health authorities. The list of signatories can be found overleaf.

Submission to ‘Closing the Gap Refresh’2
Signatories
This submission is made on behalf of the Centre for Research Excellence in Integrated Quality Improvement by the Chief Investigators and other individuals affiliated with the CRE–IQI who appear below (in alphabetical order).
Name Organisation
Associate Professor Deborah Askew The University of Queensland
Ms Jodie Bailie University Centre for Rural Health, University of Sydney
Professor Ross Bailie University Centre for Rural Health, University of Sydney
Associate Professor Roxanne Bainbridge Central Queensland University
Associate Professor Jacqueline Boyle Monash Centre for Health Research and Implementation, Monash University
Dr Paul Burgess Northern Territory Department of Health
Dr Karen Carlisle James Cook University
Professor Alan Cass Menzies School of Health Research, Charles Darwin University
Ms Louise Clark Menzies School of Health Research, Charles Darwin University
Dr Frances Cunningham Menzies School of Health Research, Charles Darwin University
Professor Chris Doran Central Queensland University
Ms Lynnette Feeney University Centre for Rural Health, University of Sydney
Ms Kerryn Harkin University Centre for Rural Health, University of Sydney
Professor Gillian Harvey The University of Adelaide
Professor Sabina Knight James Cook University
Dr Ru Kwedza University Centre for Rural Health, University of Sydney
Dr Erika Langham Central Queensland University
Professor Sarah Larkins James Cook University
Ms Alison Laycock Menzies School of Health Research, Charles Darwin University
Dr Veronica Matthews University Centre for Rural Health, University of Sydney
Associate Professor Janya McCalman Central Queensland University
Dr Barbara Nattabi WA Centre for Rural Health, The University of Western Australia
Associate Professor Megan Passey Menzies School of Health Research, Charles Darwin University
Professor David Peiris The George Institute for Global Health, University of NSW
Dr Nikki Percival University of Technology Sydney
Dr Shanthi Ramanathan Hunter Medical Research Institute, University of Newcastle
Associate Professor Andrew Searles Hunter Medical Research Institute, University of Newcastle
Dr Natalie Strobel The University of Western Australia
Professor Komla Tsey James Cook University

Centre for Research Excellence in Integrated Quality Improvement 3
1 What does Closing the Gap mean to us?
As a collaborative group of researchers, health practitioners, managers and policy makers, we are individually and collectively committed to addressing inequities in health outcomes between Aboriginal and Torres Strait Islander people and non-Indigenous Australians. We welcome the setting of targets for the Closing the Gap agenda as they assist in maintaining a focus on how we are improving health and the determinants of good health and wellbeing. They also ensure accountability for the government to achieve these targets. Ensuring that Aboriginal and Torres Strait Islander people have access to high-quality health care through a strong comprehensive primary health care model is vital if we are to improve health outcomes and close the gap.
In this submission we respond to the following questions posed by Closing the Gap Refresh in its discussion paper and on its website:
1 What does Closing the Gap mean to us?
2 What indicators should governments focus on to best support the needs and aspirations of Aboriginal and Torres Strait Islander peoples?
3 How can governments, Aboriginal and Torres Strait Islander people, and businesses work more effectively together?
4 To help close the gap, what is needed to support Aboriginal and Torres Strait Islander community leadership and decision making?
5 What resources, including data or information, are needed to help communities and develop and drive local action?
2 What indicators should governments focus on to best support the needs and aspirations of Aboriginal and Torres Strait Islander peoples?
Key points
2.1 Outcome indicators, such as mortality and morbidity, are heavily influenced by social and economic determinants and structural inequalities; further work is needed to identify key measures related to social and economic determinants of health, and ensuring accountability for development in these areas.
2.2 Indicators need to be developed through a participatory approach with success identified by Aboriginal and Torres Islander people.
2.3 Indicators of process and structures (for example, equity of access to Medicare funding) in health care should receive priority attention, as these are most directly within the influence of health service organisations.
2.4 Continuous Quality Improvement has been successfully applied in the Australian Aboriginal and Torres Strait Islander PHC setting including in non-clinical areas of work that have direct bearing on the social determinants of health.
2.5 Embedded CQI processes support a structured and systematic process to review progress towards meeting outcome, process and structure indicators at a local, regional and national level.
CRE–IQI Submission to Closing the Gap Refresh

Submission to ‘Closing the Gap Refresh’4
2.1 Outcome indicators, such as mortality and morbidity, are heavily influenced by social and economic determinants of health and structural inequalities; further work is needed to identify key measures related to social and economic determinants of health, and ensuring accountability for development in these areas.
We recognise the importance of high-level ‘outcome’ indicators to measure the quality of care, such as mortality and morbidity. However, these outcome indicators are heavily influenced by many factors other than health care quality, such as social determinants and structural inequalities. Between one-third and one-half of the health gap between Aboriginal and Torres Strait Islander and non-Indigenous Australians is estimated to be associated with differences in socioeconomic position. Also important are health behaviours, physical environments, education, food security, community infrastructure, resources and capacities, environmental stewardship, cultural continuity, and the historical and contemporary effects of colonisation, racism, social exclusion, loss of land and the Stolen Generations. Governments should monitor key social and cultural determinants of health, and implement related measures in areas such as housing, the justice system and access to land. Indicators in these areas should be as definitive as possible with standardised national definitions to allow for valid comparisons. They should form part of a carefully considered ‘mix’ of high-level outcome, process and structure indicators to drive measurable improvements in health care delivery and social determinants of health.
2.2 Indicators need to be developed in a participatory approach with success identified by Aboriginal and Torres Islander people.
Whatever the indicators, they need to be developed through a participatory approach with success being defined by Aboriginal and Torres Strait Islander people themselves.
2.3 Indicators of process and structures (for example, equity of access to Medicare funding) in health care should receive priority attention, as these are most directly within the influence of health service organisations.
To evaluate the quality of care being delivered, Donabedian in his landmark article in 1966 proposed using a triad of structure, process and outcome indicators.22,23 ‘Outcome’ – what happens to the patient; ‘structure’ – the settings and systems through which care takes place; and ‘process’ – the components of care delivered, generally reflecting best practice or evidence-based care. More recent international evidence continues to confirm the importance of process indicators in increasing quality in health care.24,25
We believe that strengthening the PHC model should also involve the removal of barriers to care that are inherent in the current Medicare system. For example, in the Northern Territory more than 70 per cent of Aboriginal people live in remote and very remote areas. Their distance from medical care ensures they face systematic barriers to accessing health service through the Medicare Benefits Schedule rules that rely on fee for service and face-to-face consultation with a GP. Increasing flexibility of payment models for care in this area may help drive innovations and incentivise the retention of health staff.
These concepts continue to be the nucleus of CQI approaches, and together they provide a framework for designing and implementing CQI. We outline below how we have applied ‘triad-informed’ CQI approaches in the Aboriginal and Torres Strait Islander PHC setting and further expanded into other areas such as housing, health promotion and food supply. We suggest developing a triad of outcome, process and structure indicators to ensure that Closing the Gap targets are met.
2.4 Continuous Quality Improvement has been successfully applied in the Australian Aboriginal and Torres Strait Islander PHC setting including in non-clinical areas of work that have direct bearing on the social determinants of health.
CQI in health care is a systematic and structured way of using data to guide changes in how health care is organised, structured or designed. CQI approaches in PHC have enabled adherence to best practice guidelines and improved patient attendance, which can be seen clearly in Figures 1–11 (pp.11–19).1,12 Implementation of CQI approaches in the Aboriginal and Torres Strait Islander PHC setting has also resulted in a CQI workforce, appropriate health system supports, and engagement with other organisations and community members.26
Since 2005, we have been implementing CQI processes in collaboration with Aboriginal and Torres Strait Islander PHC centres (both community-controlled and government-operated health services) across remote, regional and urban sites throughout Australia. Between 2010 and 2014, 175 Aboriginal and Torres Strait Islander PHC centres provided de-identified clinical audit data derived from the use of CQI tools and processes.2 These CQI data provide the most comprehensive picture to date of the quality of Aboriginal and Torres Strait Islander PHC, and our research provides valuable lessons and perspectives for improving health outcomes.20,21

Centre for Research Excellence in Integrated Quality Improvement 5
Drawing on the evidence base of best practice health care, CQI tools were developed to cover a range of priority aspects of PHC, including: preventive health; child health; chronic illness care; maternal health; rheumatic heart disease; and mental health and wellbeing. CQI audit tools in health promotion, sexual health and youth health were later additions. Accompanying the clinical and health promotion audit tools are structured systems assessment tools designed to support Aboriginal and Torres Strait Islander PHC services in assessing and improving their health care systems.27
Additionally, CQI processes provide an iterative, interactive and systemic method for extending improvement processes beyond clinical service delivery to address social and emotional wellbeing, social and cultural determinants of health,28 and health promotion.29,30 We have successfully applied CQI approaches to social determinants of health more broadly,28,31 including community food supply,32 housing33 and education.34
Our proposal for a stronger focus on the indicators of social determinants of health, and some of the structural inequalities that impact on health and wellbeing, is thereby based on evidence that the application of CQI processes has been successful in improving not only clinical care but also the delivery of care and services beyond the clinical realm to address social determinants.
2.5 Embedded CQI processes support a structured and systematic process to review progress towards meeting outcome, process and structure indicators at a local, regional and national level.
The current focus on national-level changes to address inequity means that successes or difficulties at the local level or in specific geographical areas may be obscured. Furthermore, the focus on the national level also suggests a uniformity in aspirations and outcomes for Aboriginal and Torres Strait Islander people across Australia. Through our research collaboration we have demonstrated how CQI data can be collected at the local level, where health service teams identify priorities that are locally relevant; at the regional level, where local CQI data is aggregated to inform regional decisions; and then at a national level.35,36
Embedding CQI, therefore, supports a structured process to identify and review progress towards meeting outcome, process and structure indicators at local, regional and national levels. Use of systematic processes to identify and review progress towards meeting process indicators at these three levels will be vital to monitor the implementation and strengthening of a range of systems with the potential to improve health outcomes through acting effectively together.
3.1 Promote multidisciplinary networks – such as ‘innovation platforms’ – to problem solve collectively, build capacity and learning, and foster system-wide learning and change.
Efforts to strengthen health systems require the engagement of diverse, multidisciplinary stakeholder networks working across different levels of the health system, and beyond health care sector, to problem solve collectively, to build the capacity and learning of stakeholders, and to foster system-wide planning, evaluation and translation of research.37,38 To work effectively, such networks must include Aboriginal and Torres Strait Islander people, families and communities.
Networks have been promoted as providing a general mechanism for exchanging information, spreading good practice, promoting experimentation and creating knowledge.39 Of most relevance to this submission, they may also be useful in addressing complex issues or ‘wicked’ problems, such as prevention and control of chronic diseases, the solutions to which go beyond the role and capability of any one agency.40
Many networks are focused on one professional group or one part of the health system and are primarily established to address a specific local-level problem or to implement evidence-based practice. However, recent publications renew the call for expanded multidisciplinary networks that have a systems-wide lens, and that include policy makers, researchers and health services.41 Within this systems-wide approach, there may also be a need for focused effort on specific health problems.
3 How can governments, Aboriginal and Torres Strait Islander people, and businesses work more effectively together?
Key points
3.1 Promote multidisciplinary networks – such as ‘innovation platforms’ – to problem solve collectively, build capacity and learning, and foster system-wide learning and change.
3.2 Ensure that work carried out in an Aboriginal and Torres Strait Islander context underpins the development of a ‘Partnership Learning Model’ to achieve large-scale improvement in quality of care and population health outcomes.
3.3 Strengthen community–health service linkages with increased support for Aboriginal and Torres Strait Islander governance.

Submission to ‘Closing the Gap Refresh’6
We advocate for the use of multidisciplinary networks – such as ‘innovation platforms’ – across all levels of the health system to problem solve and identify collective solutions. In this process, the health system should be broadly defined to include sectors that have an important role in health, but that do not regard health as their core responsibility (including sectors such as housing, education, business). Innovation platforms describe a form of network that aims to overcome challenges occurring at the interface of systems by bringing together people from different parts of the system.42,43 They are promoted as being different to other networks, mainly due to their diverse stakeholder composition and their focus on problem solving that requires a systems response (i.e. between components and levels of the system). Our experience with the operation of the CRE–IQI as an innovation platform demonstrates the potential for this type of approach in Aboriginal and Torres Strait Islander health care. However, they do rely on good relationships and a clear focus.
Other mechanisms to consider for multidisciplinary networks include alliance contracting and accountable care organisations that make different parties financially accountable to each other for the success of program delivery. Payment methods for the latter need to be structured so that such entities are not penalised for achieving better patient outcomes. These approaches are active in the United States and the United Kingdom and are being investigated in Australia by New South Wales health authorities.
3.2 Ensure that work carried out in an Aboriginal and Torres Strait Islander context underpins the development of a ‘Partnership Learning Model’ to achieve large-scale improvement in quality of care and population health outcomes.
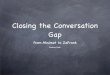
Work carried out as part of previous collaborative work in the Aboriginal and Torres Strait Islander PHC context underpinned the development of a Partnership Learning Model to achieve large-scale improvement in quality of care and population health outcomes (see Diagram 1).44 It shows how improved population health outcomes can be achieved through synergies between comprehensive primary health care, integrated CQI, system-based research networks, and system-based participatory action research.
Diagram 1: Partnership Learning Model
A learning model for large-scale change
Comprehensive primary health
care
System-based research networks
System-based participatory
research
Integrated quality
improvement
Population health impact
Heatlth systems strengthening
Knowledge translation
Systems thinking
Large-scale change

Centre for Research Excellence in Integrated Quality Improvement 7
3.3 Strengthen community–health service linkages with increased support for Aboriginal and Torres Strait Islander governance.
Health care systems need to look beyond conventional boundaries to identify better ways to deliver care to the populations they serve. Many now recognise that only 10–20% of gain in health outcomes is contributed by health care services, with a much larger share determined by social and cultural factors.45,46 Efforts to improve the quality of clinical care can be enhanced by extending policy support and resourcing for integrating CQI vertically in linkages between PHC services with governments and community members, and horizontally by linking and advocating with other sectors to improve the social and cultural determinants of Aboriginal and Torres Strait Islander health.28
For CQI initiatives to have maximum effect in improving the quality of health service delivery in Aboriginal and Torres Strait Islander settings it is important to support local-level leadership and decision making in this area. This requires some decentralisation of health care planning functions, including control of budgets, to local community structures. The support needed for Aboriginal and Torres Strait Islander governance at this level is discussed below.
4 To help close the gap, what is needed to support Aboriginal and Torres Strait Islander community leadership and decision making?
Key points
4.1 Strong and consistent policy support for CQI in Aboriginal and Torres Strait Islander health care.
4.2 An agenda shaped by evidence and data, especially at the local level.
4.3 Increased emphasis on local action and place-based solutions, which will require access to local-level data to facilitate local decision making and accountability.
4.4 Organisational and clinical capacity building in the use of data to support high-quality care delivery.
4.5 Regional support for the effective use of data.
The following outline of approaches and evidence from our CRE–IQI research and experience will support the essential Aboriginal and Torres Strait Islander community leadership and decision making needed at all levels of the health system.
4.1 Strong and consistent policy support for CQI in Aboriginal and Torres Strait Islander health care.
To work with health services caring for Aboriginal and Torres Strait Islander clients, there is a requirement for strong policy support for CQI and the development of support structures at the local and regional levels. Our research has demonstrated that progressive uptake of evidence-based CQI activities and steady improvements or maintenance of high-quality care occurred where there was long-term policy and infrastructure support for CQI.1,12 Long-term commitment and decision-making structures that support Aboriginal and Torres Strait Islander leadership in CQI research, policy and strategy development will ensure that services are responsive to community needs.
4.2 An agenda shaped by evidence and data, especially at the local level.
Through our research we have been able to demonstrate that for Aboriginal and Torres Strait Islander PHC services participating in CQI in three or more cycles there was a general increase in the quality of care. This can be seen clearly in Figures 1–11 (pp.11–19).1,12 The policy support, and the local and regional levels support structures referred to above, will ensure that services continue to strengthen evidence-based CQI activities. Participating services will be able to collect accurate data across the scope of best practice care, to identify the priority gaps collectively, and to share knowledge and co-develop tailored solutions to address priority gaps in care.
Ensuring that Aboriginal and Torres Strait Islander people have access to high-quality health care through a strong comprehensive primary health care model is vital if we are to improve health outcomes and close the gap.

Submission to ‘Closing the Gap Refresh’8
4.3 Increased emphasis on local action and place-based solutions, which will require access to local-level data to facilitate local decision making and accountability.
Calls for a Closing the Gap agenda to be shaped by data and evidence, and informed through access to local-level data, also has implications for associated monitoring and evaluation. It provides an opportunity for evaluation design to be iterative and Aboriginal and Torres Strait Islander led, to use local-level data and to build evaluative capacity at the local level for the use and interpretation of data.
4.4 Organisational, clinical and individual capacity building in the use of data to support high-quality care delivery.
Further investment is required in systems development and practitioner training in the effective use of clinical information systems47 and decision support tools;36 for example, recall and reminder systems and cardiovascular risk assessment calculators.3,48 Clinical information systems are viewed as being in place and having the required functionalities to support high-quality care. However, it is acknowledged that there is significant scope for improving the consistent recording of Aboriginal and or Torres Strait Islander identification in the records,47,49 and for the collection of additional items in preventive care, in standardised screening items for nutrition and physical activity, and in the key social determinants of health. Ongoing staff training in the use of these clinical information systems is essential for the effective use of these systems. Emphasis on the training of Aboriginal and Torres Strait Islander staff in the use of clinical information systems and CQI will help to build and sustain community capacity in using data for decision making to improve care.
4.5 Regional support for the effective use of data.
Involvement in participatory interpretation of local-level data builds evaluation capacity and skills in using data to inform decision making at a number of levels. In the Northern Territory, where there is funding for regional CQI support structures, the use of CQI audit tools and processes has resulted in increased workforce capabilities, capacities and enthusiasm to deliver best practice primary health care.50 Furthermore, consistent and sustained policy and infrastructure support for CQI has resulted in a progressive uptake of evidence-based CQI activities and a marked improvement in health care performance compared to that of other jurisdictions.1
5 What resources, including data or information, are needed to help communities and develop and drive local action?
The following resources or approaches are needed to help communities, and to develop and drive local action.
5.1 Local-level data engages communities in interpretation and planning for place-based solutions and action.
Our recommendations for addressing the previous question emphasise the importance of access to local-level data for supporting Aboriginal and Torres Strait Islander community leadership and decision making. These data are relevant for developing community-driven local action to help in Closing the Gap. Resourcing local action involves local-level training in the effective use of clinical information systems,3,36,51 and the resourcing of regional structures and processes that can facilitate and support development and action.
Key points
5.1 Local-level data engages communities in interpretation and planning for place-based solutions and action.
5.2 CQI approaches and principles embedded in non-clinical and clinical aspects of health care, consistent with Aboriginal and Torres Strait Islander community definitions of health.
5.3 CQI approaches and processes are inherently inclusive and participatory.
5.4 Access to accurate and timely data across the full scope of best practice for PHC required for community- and data-driven action, and critical gaps in the collecting and recording of client data in clinical information systems addressed.
5.5 Regional structures and multidisciplinary networks resourced to strengthen capacity and support locally driven solutions and action.
5.6 Robust evaluation designs to guide ongoing improvement.

Centre for Research Excellence in Integrated Quality Improvement 9
5.2 CQI approaches and principles embedded in non-clinical and clinical aspects of health care, consistent with Aboriginal and Torres Strait Islander community definitions of health.
Consistent with an Aboriginal and Torres Strait Islander holistic approach to health, action to improve care needs to encompass not just the physical wellbeing of an individual but also the social, emotional and cultural wellbeing of communities. Embedding CQI approaches and principles in the non-clinical as well as clinical aspects of health care supports communities to develop and drive action that reflects cultural understandings of health. The CQI tools and processes we have developed to help address social determinants of health such as food supply, housing and education offer practical resources for community priority setting and action.29,32,52
5.3 CQI approaches are inherently inclusive and participatory.
As outlined above, CQI tools offer practical resources and processes for community-driven local action. CQI facilitators can support participatory interpretation of local-level data with community, health service teams and regional support teams. Such processes can encourage and facilitate community participation in local health care planning and quality improvement through the development, implementation and evaluation of tailored strategies.
5.4 Access to accurate and timely data across the full scope of best practice for PHC required for community- and data-driven action, and critical gaps in the collecting and recording of client data in clinical information systems addressed.
Access is needed to accurate and timely data across the full scope of best practice for PHC, not just high-level Key Performance Indicators. The CQI tools we have developed assess care across the scope of best practice, with teams then able to identify gaps in local service delivery and develop strategies to address these. There is a need to build further capability to extract indicator data, as it is currently not possible to extract these data electronically across the scope of best practice care.47 As previously highlighted, staff training in the effective use of clinical information systems is also needed.3,36,51
Furthermore, there are critical gaps in the collecting and recording of client data in clinical information systems. The inconsistencies in data required for the calculation of many key indicators of access and quality of care places serious constraints on the meaningful use of data extracted from
electronic clinical information systems. There is a need for greater attention to the quality of denominator data, and to consistency in the recording of Aboriginal and Torres Strait Islander status, if we are to realise the potential benefits of clinical information systems for patient care, service planning, improvement and policy. We propose a quality improvement approach for enhancing data quality.47
5.5 Regional structures and multidisciplinary networks resourced to strengthen capacity and support locally driven solutions and action.
Regional structures and resources need to be in place to support local-level data collection, analysis, interpretation, action planning and implementation.3,53 Resources are also needed for two-way capacity strengthening at the local, regional and national levels in the use and interpretation of data for priority setting, and for collaborative planning and implementation to consider and respond to community priorities. Use of multidisciplinary networks such as ‘innovation platforms’42 facilitate knowledge sharing and problem solving for local and collective action.
5.6 Robust evaluation designs to guide ongoing improvement.
Evaluation plays a key role in supporting program decision making by helping us to understand whether a program is working and in what context, and when it’s not working and why. Well-planned and executed evaluation provides evidence for improved program design, delivery and outcomes. It is also essential in supporting the expansion of innovative programs and continuing existing programs that are shown to be successful.
We recommend that any investment in Closing the Gap strategies undergo an extensive evaluation that includes an assessment of process, outcome and economic indicators. In our CRE–IQI we are employing three evaluation approaches – a social network analysis, developmental evaluation techniques, and an economic and impact assessment.54

Submission to ‘Closing the Gap Refresh’10
Supporting Data
Data are presented by audit cycle and include data for the same cohort of health centres that have conducted the different audits in at least three audit cycles. All 11 Figures indicate the impact of duration of participation in CQI on the delivery of care according to best practice guidelines. Note that ‘Audit Cycle 1’ represents baseline audit data, ‘Audit Cycle 2’ represents the first follow-up audit and so on.
CQI data from Aboriginal and Torres Strait Islander PHC services are presented for the following areas of care: preventive health, child health, chronic illness care, maternal health, and rheumatic heart disease and acute rheumatic fever.
The composite indicator includes a range of services in accordance with best practice guidelines. The overall health centre systems’ figures are an average score of the various domain scores that make up the total systems assessment (i.e. delivery system design, information systems and decision support, self-management support, links with the community, other health services and other resources, and organisational influence and integration).27 Higher scores reflect better function.
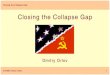
An important focus of our work has been understanding the variation between health centres over time in the delivery of care in accordance with best practice guidelines. ‘Box and whisker plots’ (or box plots) are a useful way of presenting data on variation in a graphical form that should assist with interpretation.
Box plots are used to show variation between health centres, such as:
× Health centres with the minimum and maximum mean percentage in recorded delivery of care in accordance with best practice guidelines (ends of whiskers show highest value if no outliers).
× Outliers – health centres that are far away from most others in the dataset (or a distance that is greater than 1.5 times the length of the box).
× The level of variation between health centres in recorded delivery of care by dividing scores into quarters:
— the box represents the middle 50 per cent of health centres, and the line within the box represents the median (or middle health centre);
— the ‘whisker’ at the top of the box (and outliers if present) represents the top 25 per cent of health centres;
— the ‘whisker’ at the bottom of the box (and outliers if present) represents the bottom 25 per cent of health centres; and
— the longer the box plot, the greater the range of care delivery (or variation) between health centres.
In assessing data trends, it is helpful to focus on:
a the trend for the mean (average) and median (middle) values for health centres – in particular, whether the mean and median are increasing, staying steady or decreasing; and
b the trend in the variation between health centres – in particular, whether the variation is getting less (shorter boxes, shorter whiskers) and, importantly, whether there is an improvement in the values for the health centres at the lower end of the range (higher level for the bottom end of whiskers under boxes).
1 2Audit Cycle
% of services delivered
3
100
80
60
40
20
0
Outlier
Outlier
Highest value
Median (middle value)
Trend line
Mean (average value)75th quartile
Top 1/4 of data
Bottom 1/4of data
Middle 1/2 of data
(within box)
Middle value
25th quartile
Lowest value

Centre for Research Excellence in Integrated Quality Improvement 11
For health centres that completed three or more audit cycles for preventive health, there were improvements over successive audit cycles, albeit small, in the mean level of care according to best practice guidelines. There was little evidence of narrowing in the variation between health centres over successive audit cycles.
Preventive health care
Overall delivery of preventive health care
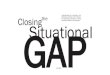
Figure 1 shows trends in a composite indicator of overall service delivery to well clients in accordance with best practice guidelines. The composite indicator includes services such as physical checks, clinical examinations and brief interventions. Indicators that reflect follow-up actions for abnormal findings have not been included in the composite indicator as they relate to specific sub-groups of the patient population.
Figure 1: Mean health centre overall service delivery to well clients, by audit cycle for health centres that have at least 3 years of audit data (n = number of health centres; number of client records audited who attended in previous 24 months)
Overall adherence to preventive care composite figure includes the following indicators: weight, waist circumference, blood pressure, urinalysis, blood glucose level, sexually transmitted infections (gonorrhoea and chlamydia, syphilis), pap smear, oral health, nutrition, physical activity, smoking and alcohol status recorded, brief intervention if smoker and/or high-risk alcohol user
% of clients
100
80
60
40
20
0
4 (n=59; 2,080)3 (n=90; 3,328)2 (n=90; 3,004)1 (n=90; 2,838)Audit Cycle

Submission to ‘Closing the Gap Refresh’12
Key reference: Bailie J, Matthews V, Laycock A, Schultz R, Bailie R. Priority Evidence–Practice Gaps in Preventive Health Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research, 2016. Accessed 28 February 2018 at: http://apo.org.au/node/645995
Links to protocol and audit tool: https://www.menzies.edu.au/page/Resources/Preventive_Services_clinical_audit/
Overall systems assessment score for preventive health care
For health centres that completed three or more systems assessments for preventive health care, there were improvements in the average overall Systems Assessment Tool (SAT) score over successive audit cycles. There was no clear trend in variation for all health centres that had completed at least three audit cycles, but there was less variation between those health centres that had completed four audit cycles compared to those that had completed three.
Figure 2: Overall system assessment score for preventive health care, by year for all health centres and by cycle for health centres that have at least 3 years of systems assessment data (n = number of health centres that conducted a systems assessment)
Overall score is the average of each of the domain scores that make up the total systems assessment (i.e. delivery system design, information systems and decision support, self-management support, links with the community and other health services, and other resources and organisational influence and integration)
SAT Score
11
9
7
5
3
10
8
6
4
2
1
4 (n=46)3 (n=77)2 (n=77)1 (n=77)Audit Cycle

Centre for Research Excellence in Integrated Quality Improvement 13
Key reference: Bailie R, Matthews V, Bailie J, Laycock A. Priority Evidence–Practice Gaps in Aboriginal and Torres Strait Islander Child Health: Final Report. Brisbane: Menzies School of Health Research, 2014. Accessed 28 February 2018 at: http://apo.org.au/node/5565918
Link to audit tool and protocol: https://www.menzies.edu.au/page/Resources/Child_health_clinical_audit/
Child health
Overall delivery of child health care
Figure 3 shows trends in a composite indicator of overall service delivery to children in accordance with best practice guidelines. For health centres that had completed three or more audit cycles, there is an overall increase in delivery of care in line with best practice guidelines in successive audit cycles (Figure 3).
There is evidence of improvement over successive audit cycles for overall child health care, with a reduction in variation for overall child health. There is also a narrowing in the variation across health centres in the 4th and 5th audit cycles, with a notable improvement in those health centres with the lowest levels of overall delivery of care.
Figure 3: Mean per cent child health delivery to children who attended in previous 12 months, by audit cycle for health centres that have at least 3 years of audit data (n = number of health centres; number of records audited of children who attended in previous 12 months)
Overall adherence to child care composite figure includes the following indicators: weight, height, head circumference, hip exam, testes check, ear exam, breastfeeding, nutrition advice, Sudden Infant Death Syndrome prevention, and developmental check
% of service delivery to children who attended in last 12 months
100
80
60
40
20
0
4 (n=38; 1,045) 5 (n=17; 505)3 (n=71; 1,856)2 (n=71; 1,839)1 (n=71; 1,900)Audit Cycle

Submission to ‘Closing the Gap Refresh’14
Overall systems assessment for child health care
For health centres that participated in three or more audit cycles, the scores for overall systems assessment show improvement and decreasing variation between health centres over successive cycles, with an increase in scores for health centres at the lower end of the range.
Figure 4: Overall system assessment score for child health, by year for all health centres and by cycle for health centres that have at least 3 years of systems assessment data(n = number of health centres that conducted a systems assessment)
Overall score is the average of each of the domain scores that make up the total systems assessment (i.e. delivery system design, information systems and decision support, self-management support, links with the community and other health services, and other resources and organisational influence and integration)
SAT Score
11
9
7
5
3
10
8
6
4
2
1
4 (n=19 5 (n=4)3 (n=57)2 (n=57)1 (n=57)Audit Cycle
Chronic illness care
Overall delivery of chronic illness care
The composite indicators for each chronic condition include services such as chronic disease management plans, vaccinations, physical checks, clinical examinations and brief interventions. Follow-up actions for abnormal findings have not been included as they relate to specific subgroups of the patient population.
For health centres that completed three or more audit cycles for type 2 diabetes, chronic kidney disease and hypertension, there were trends of improvement in the mean and median level of care according to best practice guidelines. For chronic kidney disease and type 2 diabetes there was a narrowing in the variation between health centres across the first three audit cycles, with a notable improvement in those health centres with the lowest levels of overall delivery of care.

Centre for Research Excellence in Integrated Quality Improvement 15
Figure 5: Mean health centre overall service delivery to clients with type 2 diabetes, chronic kidney disease or hypertension by audit cycle for health centres that have at least 3 years of audit data(n = number of health centres; number of client records audited who attended in previous 12 months)
Overall adherence to best practice indicators present in the vascular and metabolic clinical audit tool including: current chronic disease management plan, chronic disease management/medication discussion, influenza and pneumococcal vaccination, weight and waist circumference (within 6 months), Body Mass Index, blood pressure (within 6 months), nutrition and physical activity advice, albumin-to-creatinine ratio, estimated glomerular filtration rate, full lipid profile, total cholesterol, tobacco and alcohol use with brief intervention/s if required. In addition, for type 2 diabetes: visual acuity, dilated eye check, feet check and HbA1c (within 6 months); for hypertension: dilated eye check and blood glucose level; and for chronic kidney disease: blood glucose level
% of T2D patients
100
80
60
40
20
0
4 (n=55; 1,620) 5 (n=35; 982)3 (n=54; 1,483)2 (n=56; 1,350)1 (n=53; 1,059)Audit Cycle
% of CKD patients
100
80
60
40
20
0
3 (n=10; 201)2 (n=10; 237)1 (n=10; 187)Audit Cycle
% of HT patients
100
80
60
40
20
0
3 (n=23; 675)2 (n=23; 673)1 (n=23; 474)Audit Cycle

Submission to ‘Closing the Gap Refresh’16
Key reference: Matthews V, Connors C, Laycock A, Bailie J, Bailie R. Priority Evidence–Practice Gaps in Chronic Illness Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research, 2015. Accessed 28 February 2018 at: http://apo.org.au/node/5439513
Links to protocol and audit tool: https://www.menzies.edu.au/page/Resources/Vascular_and_Metabolic_Syndrome_Management/
Overall systems assessment for chronic illness care
For health centres that had participated in three or more audit cycles, there was some improvement in the mean and the median scores over successive cycles including improvement in scores for health centres at the lower end of the range.
Figure 6: Overall system assessment score for chronic illness care, by year for all health centres and by cycle for health centres that have at least 3 years of systems assessment data(n = number of health centres that conducted a systems assessment)
Overall score is the average of each of the domain scores that make up the total systems assessment (i.e. delivery system design, information systems and decision support, self-management support, links with the community and other health services, and other resources and organisational influence and integration)
SAT Score
11
9
7
5
3
10
8
6
4
2
1
4 (n=37)3 (n=80)2 (n=80)1 (n=80)Audit Cycle
Maternal health
Overall delivery of maternal health care
Two composite indicators are presented showing delivery of antenatal and postnatal services in accordance with best practice guidelines (see Figures 7 and 8). The antenatal composite includes recording of risk factors, routine antenatal checks, laboratory investigations, and brief interventions and counselling. The postnatal composite includes brief intervention and counselling for new mothers.
For health centres that completed three or more maternal health audit cycles, there were improvements in the mean level of overall service delivery related to pregnancy care. There was no evidence of reduced variation between health centres over successive audit cycles.
There were improvements in the mean level of overall service delivery related to postnatal care. However, there was no evidence of reduced variation between health centres over successive audit cycles.

Centre for Research Excellence in Integrated Quality Improvement 17
Figure 7: Mean health centre overall service delivery for antenatal care, audit cycle for health centres that have at least 3 years of audit data(n = number of health centres; number of client records audited)
Figure 8: Mean health centre overall service delivery for postnatal care, by audit year for all health centres and by audit cycle for health centres that have at least 3 years of audit data(n = number of health centres; number of client records audited)
Overall adherence to antenatal care composite figure includes the following indicators present in the maternal health audit tool: ≥7 antenatal visits, estimated gestational age ≤13 weeks at first antenatal visit, blood pressure (1st, 2nd & 3rd trimester), urinalysis (1st & 2nd trimester), Body Mass Index (1st trimester), fundal height (2nd & 3rd trimester), foetal movements (3rd trimester), blood glucose (2nd trimester), documentation of blood group, antibody status, rubella, Hepatitis B status, Mid-stream urine, full blood examination, Syphilis serology, Human immunodeficiency virus, PCR test, smoking status recorded (1st & 3rd trimester), drinking status recorded (1st & 3rd trimester), social risk assessment, emotional wellbeing assessment, discussion on plans for care and birthing, nutrition, breastfeeding, domestic and social environment and cultural considerations
Overall adherence to postnatal care composite figure includes the following indicators present in the maternal health audit tool: brief interventions and counselling for smoking, nutrition, breastfeeding, infection prevention, injury prevention, Sudden Infant Death Syndrome prevention, alcohol and other substance abuse, physical activity, mood (depression), contraception, domestic and social environment, social and family support, financial situation, housing condition and food security
% of clients
100
80
60
40
20
0
4 (n=28; 465)3 (n=45; 790)2 (n=44; 758)1 (n=45; 886)Audit Cycle
% of clients with record of postnatal visit
100
80
60
40
20
0
4 (n=28; 391)3 (n=43; 630)2 (n=43; 434)1 (n=44; 492)Audit Cycle

Submission to ‘Closing the Gap Refresh’18
Key reference: Gibson-Helm M, Bailie J, Matthews V, Laycock A, Boyle J, Bailie R. Priority Evidence–Practice Gaps in Maternal Health Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research; 2016. Accessed 6 March at: http://apo.org.au/node/658718
Links to protocol and audit tool: https://www.menzies.edu.au/page/Resources/Maternal_health_clinical_audit/
Overall systems assessment for maternal health care
For health centres that completed three or more systems assessments for maternal health, there were improvements in the average overall SAT score but no evidence of a change in variation.
Figure 9: Overall system assessment score for maternal care, by year for all health centres and by cycle for health centres that have at least 3 years of systems assessment data(n = number of health centres that conducted a systems assessment)
Overall score is the average of each of the domain scores that make up the total systems assessment (i.e. delivery system design, information systems and decision support, self-management support, links with the community and other health services, and other resources and organisational influence and integration)
SAT Score
11
9
7
5
3
10
8
6
4
2
1
4 (n=19)3 (n=42)2 (n=42)1 (n=42)Audit Cycle
Rheumatic heart disease / Acute rheumatic fever
Overall service delivery for RHD/ARF care
For health centres that completed three audit cycles for RHD/ARF prevention and care, there were improvements, albeit small, in the mean level of care according to best practice guidelines. There was little evidence of narrowing in the variation between health centres over successive audit cycles.]
Overall systems assessment for RHD / ARF care
For health centres that completed three systems assessments, there was a small improvement in the mean overall SAT score. There was no clear trend in variation for all health centres that had completed three audit cycles.
Key reference: Bailie J, Matthews V, Laycock A, Bailie R. Priority Evidence–Practice Gaps in Aboriginal and Torres Strait Islander Acute Rheumatic Fever and Rheumatic Heart Disease Care: Final Report. Brisbane: Menzies School of Health Research, 2016. Accessed 6 March at: http://apo.org.au/node/7091715
Links to protocol and audit tool: https://www.menzies.edu.au/page/Resources/Acute_Rheumatic_Fever_Rheumatic_Heart_Disease_Clinical_Audit/

Centre for Research Excellence in Integrated Quality Improvement 19
Figure 10: Mean health centre overall service delivery to RHD/ARF clients by audit cycle for health centres that have at least 3 years of audit (n = number of health centres; number of clients records audited)
Figure 11: Overall system assessment score for RHD/ARF, by year for all health centres and by cycle for health centres that have at least 3 years of systems assessment data(n = number of health centres that conducted a systems assessment)
Overall adherence to RHD/ARF care composite figure includes the following best practice indicators present in the RHD audit tool: RHD classification recorded in health summary; record of current and complete RHD/ARF management plan; record of planned frequency of benzathine penicillin G (BPG) injections (if client prescribed regular BPG injections); ≥80% of BPG injections received (if client prescribed regular injections and there is record of planned frequency); record of active recall if <80% of injections received; timely doctor and specialist review and echocardiogram (according to recommended schedule based on RHD classification); and record of client education (provided within the last 12 months)
Overall score is the average of each of the domain scores that make up the total systems assessment (i.e. delivery system design, information systems and decision support, self-management support, links with the community and other health services, and other resources and organisational influence and integration)
% of clients
100
80
60
40
20
0
3 (n=19; 388)2 (n=19; 400)1 (n=19; 407)Audit Cycle
SAT Score
11
9
7
5
3
10
8
6
4
2
1
3 (n=16)2 (n=16)1 (n=16)Audit Cycle

Submission to ‘Closing the Gap Refresh’20
References
1 Bailie R, Matthews V, Larkins S, et al. Impact of policy support on uptake of evidence-based continuous quality improvement activities and the quality of care for Indigenous Australians: a comparative case study. BMJ Open 2017;7(10). doi: 10.1136/bmjopen-2017-016626.
2 Bailie R, Si D, Shannon C, et al. Study protocol: national research partnership to improve primary health care performance and outcomes for Indigenous peoples. BMC Health Serv Res 2010;10:129. doi: 10.1186/1472-6963-10-129 [published online: 2010/05/21].
3 Bailie J, Matthews V, Laycock A, et al. Improving preventive health care in Aboriginal and Torres Strait Islander primary care settings. Globalization and Health 2017;13(1):48. doi: 10.1186/s12992-017-0267-z.
4 Bailie C, Matthews V, Bailie J, et al. Determinants and gaps in preventive care delivery for Indigenous Australians: A cross-sectional analysis. Frontiers in Public Health 2016;4. doi: 10.3389/fpubh.2016.00034.
5 Bailie J, Matthews V, Laycock A, et al. Priority Evidence–Practice Gaps in Preventive Health Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research, 2016.
6 Gibson-Helm ME, Teede HJ, Rumbold AR, et al. Continuous quality improvement and metabolic screening during pregnancy at primary health centres attended by Aboriginal and Torres Strait Islander women. The Medical Journal of Australia 2015;203(9):369–70.
7 Gibson-Helm ME, Bailie J, Matthews V, et al. Identifying evidence-practice gaps and strategies for improvement in Aboriginal and Torres Strait Islander maternal health care. PloS One 2018;13(2):e0192262.
8 Gibson-Helm M, Bailie J, Matthews V, et al. Priority Evidence–Practice Gaps in Maternal Health Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research, 2016.
9 Matthews V, Bailie J, Laycock A, et al. Priority Evidence–Practice Gaps in Mental Health and Wellbeing Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research, 2016.
10 Schierhout G, Matthews V, Connors C, et al. Improvement in delivery of type 2 diabetes services differs by mode of care: a retrospective longitudinal analysis in the Aboriginal and Torres Strait Islander primary health care setting. BMC Health Services Research 2016;16(1):560.
11 Matthews V, Connors C, Laycock A, et al. Chronic Illness Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research, 2015.
12 Matthews V, Schierhout G, McBroom J, et al. Duration of participation in continuous quality improvement: a key factor explaining improved delivery of type 2 diabetes services. BMC Health Services Research 2014;14(1):578. doi: 10.1186/s12913-014-0578-1.
13 Matthews V, Connors C, Laycock A, et al. Priority Evidence–Practice Gaps in Chronic Illness Care for Aboriginal and Torres Strait Islander People: Final Report. Brisbane: Menzies School of Health Research, 2015.
14 Ralph AP, Fittock M, Schultz R, et al. Improvement in rheumatic fever and rheumatic heart disease management and prevention using a health centre-based continuous quality improvement approach. BMC Health Services Research 2013;13(1):525.
15 Bailie J, Matthews V, Laycock A, et al. Priority Evidence–Practice Gaps in Aboriginal and Torres Strait Islander Acute Rheumatic Fever and Rheumatic Heart Disease Care: Final Report. Brisbane: Menzies School of Health Research, 2016.
16 Nattabi B, Matthews V, Bailie J, et al. Wide variation in sexually transmitted infection testing and counselling at Aboriginal primary health care centres in Australia: analysis of longitudinal continuous quality improvement data. BMC Infectious Diseases 2017;17(1). doi: 10.1186/s12879-017-2241-z.
17 McAullay D, McAuley K, Bailie R, et al. Sustained participation in annual continuous quality improvement activities improves quality of care for Aboriginal and Torres Strait Islander children. Journal of Paediatrics and Child Health:n/a-n/a. doi: 10.1111/jpc.13673.
18 Bailie R, Matthews V, Bailie J, et al. Priority Evidence–Practice Gaps in Aboriginal and Torres Strait Islander Child Health: Final Report. Brisbane: Menzies School of Health Research, 2014.
19 Bailie J, Schierhout G, Cunningham F, et al. Quality of Primary Health Care for Aboriginal and Torres Strait Islander People in Australia: Key Research Findings and Messages for Action from the ABCD National Research Partnership. Brisbane: Menzies School of Health Research, 2015.
20 Bailie J, Yule J, Schierhout G, et al. Partnering to Improve Aboriginal and Torres Strait Islander Primary Health Care: ABCD National Research Partnership Project. Brisbane: Menzies School of Health Research, 2015.
21 Bailie R, Bailie J, Larkins S, et al. Editorial: Continuous quality improvement (CQI) – advancing understanding of design, application, impact, and evaluation of CQI approaches. Frontiers in Public Health 2017;5(306). doi: 10.3389/fpubh.2017.00306.
22 Ayanian JZ, Markel H. Donabedian’s lasting framework for health care quality. The New England Journal of Medicine 2016;375(3):205–07.

Centre for Research Excellence in Integrated Quality Improvement 21
23 Donabedian A. Evaluating the quality of medical care. The Milbank Quarterly 2005;83(4):691–729.
24 Moore GF, Audrey S, Barker M, et al. Process evaluation of complex interventions: Medical Research Council guidance. British Medical Journal 2015;350. doi: 10.1136/bmj.h1258.
25 Abel G, Saunders CL, Mendonca SC, et al. Variation and statistical reliability of publicly reported primary care diagnostic activity indicators for cancer: a cross-sectional ecological study of routine data. BMJ Qual Saf 2017:bmjqs-2017-006607.
26 Woods C, Carlisle K, Larkins S, et al. Exploring systems that support good clinical care in Indigenous primary health-care services: a retrospective analysis of longitudinal systems assessment tool data from high-improving services. Frontiers in Public Health 2017;5(45). doi: 10.3389/fpubh.2017.00045.
27 Cunningham FC, Ferguson-Hill S, Matthews V, et al. Leveraging quality improvement through use of the Systems Assessment Tool in Indigenous primary health care services: a mixed methods study. BMC Health Services Research 2016;16(1):583. doi: 10.1186/s12913-016-1810-y.
28 McCalman J, Bailie R, Bainbridge R, et al. Continuous quality improvement and comprehensive primary health care: a systems framework to improve service quality and health outcomes. Frontiers in Public Health 2018;6(76). doi: 10.3389/fpubh.2018.00076.
29 Percival N, O’Donoghue L, Lin V, et al. Improving health promotion using quality improvement techniques in Australian Indigenous primary health care. Frontiers in Public Health 2016;4(53). doi: 10.3389/fpubh.2016.00053.
30 O’Donoghue L, Percival N, Laycock A, et al. Evaluating Aboriginal and Torres Strait Islander health promotion activities using audit and feedback. Australian Journal of Primary Health 2014;20(4):339–44. doi: https://doi.org/10.1071/PY14048.
31 McDonald EL, Bailie R, Michel T. Development and trialling of a tool to support a systems approach to improve social determinants of health in rural and remote Australian communities: the healthy community assessment tool. International Journal for Equity in Health 2013;12(1):15. doi: 10.1186/1475-9276-12-15.
32 Brimblecombe J, van den Boogaard C, Wood B, et al. Development of the good food planning tool: A food system approach to food security in indigenous Australian remote communities. Health & Place 2015;34:54–62. doi: 10.1016/j.healthplace.2015.03.006 [published online: 2015/04/29].
33 Bailie RS, Wayte KJ. A continuous quality improvement approach to Indigenous housing and health. Environmental Health: The Journal of the Australian Institute of Environmental Health 2006;6(2):36–41.
34 McCalman J, Bainbridge R, Russo S, et al. Psycho-social resilience, vulnerability and suicide prevention: impact evaluation of a mentoring approach to modify suicide risk for remote Indigenous Australian students at boarding school. BMC Public Health 2016;16(1):98. doi: 10.1186/s12889-016-2762-1.
35 Laycock A, Bailie J, Matthews V, et al. Interactive dissemination: engaging stakeholders in the use of aggregated quality improvement data for system-wide change in Australian Indigenous primary health care. Frontiers in Public Health 2016;4. doi: 10.3389/fpubh.2016.00084.
36 Bailie J, Laycock A, Matthews V, et al. System-level action required for wide-scale improvement in quality of primary health care: synthesis of feedback from an interactive process to promote dissemination and use of aggregated quality of care data. Frontiers in Public Health 2016;4. doi: 10.3389/fpubh.2016.00086.
37 Gilson L. Health Policy and System Research: A Methodology Reader. Geneva: World Health Organization, 2013.
38 De Savigny D, Adam T. Systems Thinking for Health Systems Strengthening. Geneva: World Health Organization, 2009.
39 Health Foundation. Effective Networks for Improvement: Developing and Managing Effective Networks to Support Quality Improvement in Healthcare. London: Health Foundation, 2014.
40 Ferlie E, Fitzgerald L, McGiven G, et al. Making Wicked Problems Governable? The Case of Managed Networks in Health Care. Oxford: Oxford University Press, 2013.
41 Nix M, McNamara P, Genevro J, et al. Learning collaboratives: insights and a new taxonomy from AHRQ’s two decades of experience. Health Affairs 2018;37(2):205–12.
42 Bailie J, Cunningham F, Bainbridge R, et al. Comparing and contrasting ‘innovation platforms’ with other forms of professional networks for strengthening primary health care systems for Indigenous Australians. BMJ Global Health; in press.
43 Schut M, Andersson J, Dror I, et al. Guidelines for Innovation Platforms in Agricultural Research for Development. Ibada: International Institute of Tropical Agriculture and Wageningen University, 2017.
44 Bailie R, Matthews V, Brands J, et al. A systems-based partnership learning model for strengthening primary healthcare. Implementation Science 2013;8(1):143. doi: 10.1186/1748-5908-8-143.
45 Booske BC, Athens JK, Kindig DA, et al. Different Perspectives for Assigning Weights to Determinants of Health. Madison, WI: University of Wisconsin Population Health Institute, 2010

Submission to ‘Closing the Gap Refresh’22
46 McGinnis JM, Williams-Russo P, Knickman JR. The case for more active policy attention to health promotion. Health Affairs (Project Hope) 2002;21(2):78–93. doi: 10.1377/hlthaff.21.2.78 [published online: 2002/03/20].
47 Bailie R, Bailie J, Chakraborty A, et al. Consistency of denominator data in electronic health records in Australian primary healthcare services: enhancing data quality. Australian Journal of Primary Health 2015;21(4):450–59.
48 Matthews V, Burgess CP, Connors C, et al. Integrated clinical decision support systems promote absolute cardiovascular risk assessment: an important primary prevention measure in Aboriginal and Torres Strait Islander primary health care. Frontiers in Public Health 2017;5(233). doi: 10.3389/fpubh.2017.00233.
49 de Witt A, Cunningham FC, Bailie R, et al. Identification of Australian Aboriginal and Torres Strait Islander cancer patients in the primary health care setting. Frontiers in Public Health 2017;5:199. doi: 10.3389/fpubh.2017.00199.
50 Allen and Clarke Consulting Group. Evaluation of the Northern Territory Continuous Quality Improvement (CQI) Investment Strategy: Final Report. Canberra: Australian Government Department of Health, 2013.
51 Bailie J, Matthews V, Laycock A, et al. Rigorous follow-up systems for abnormal results are essential to improve health outcomes for Aboriginal and Torres Strait Islander people. Australian Journal of Primary Health 2018;24:1–3.
52 McCalman J, Bailie R, Bainbridge R, et al. Continuous quality improvement and comprehensive primary healthcare: a systems framework to improve service quality and health outcomes. Frontiers in Public Health 2018;6:76.
53 Newham J, Schierhout G, Bailie R, et al. ‘There’s only one enabler; come up, help us’: staff perspectives of barriers and enablers to continuous quality improvement in Aboriginal primary health-care settings in South Australia. Australian Journal of Primary Health 2016;22(3):244–54. doi: https://doi.org/10.1071/PY14098.
54 Ramanathan S, Reeves P, Deeming S, et al. Encouraging translation and assessing impact of the Centre for Research Excellence in Integrated Quality Improvement: rationale and protocol for a research impact assessment. BMJ Open 2017;7(12). doi: 10.1136/bmjopen-2017-018572.
ARF acute rheumatic fever
BPG benzathine penicillin G
CQI continuous quality improvement
CRE–IQI Centre for Research Excellence in Integrated Quality Improvement
PHC primary health care
RHD rheumatic heart disease
SAT systems assessment tool
Acronyms