Embed Size (px)
Citation preview

1061
and ketosis thus calling on fat stores to supply the substratefor energy metabolism with consequent sparing of proteinand aminoacids. Your leading article 3 commented on thispossibility as well.
Perhaps a similar situation applies from time to time inthe patient with kwashiorkor-namely, increased secretionof insulin in response to carbohydrate ingestion withsuppression of lipolysis and ketosis and ultimately a re-bound demand for aminoacids as a source of gluconeo-genesis. Adaption to prolonged fasting and dependenceupon ketones and fatty acids takes time and acute changesmay not allow time for maximum conservation of proteinto occur. 4
Montefiore-Morrisania Affiliation,168th Street and Gerard Avenue,
Bronx, New York 10452,U.S.A. ROBERT MATZ.
SUSCEPTIBILITY OF BACTEROIDESFRAGILIS TO CO-TRIMOXAZOLE
SIR,-It is gratifying to note that Phillips and Warren 5have confirmed our findings that some strains of Bac-teraides fragilis are sensitive to co-trimoxazole. May I beallowed to correct the impression given in their paper thatour work was inadequate or incomplete, with the follow-ing details ? We estimated minimal inhibitory concentra-tions (M.l.c.s) separately for trimethoprim and sulphon-amide using an inoculum of 104-106 viable organisms onDST (Oxoid) agar plus 5% lysed horse blood and varyingquantities of each drug. A multiple replicator with 1 mm.loops was used for inoculation, and the tests were controlledwith a plain plate containing no antimicrobial agent. TheOxford staphylococcus was used as the control organism.We did these tests several times on 77 strains, but did nottest for fractional inhibitory concentrations (F.I.C.S). Ourresults clearly indicated that the active agent was thesulphonamide not the trimethoprim. The results for 20strains are given in the accompanying table. Some of thestrains were tested by Miss Pamela Waterworth who kindlychecked our findings and suggested that the M.l.c.s weredependent to a large extent on the size of the inoculumused in the tests. This was later confirmed by Dr Bushbywho tested 6 of our strains, and found that they were moresensitive to trimethoprim than in our tests. He also men-tioned that there was potentiation between the two drugs.In fact we could detect the potentiation effect with somestrains on disc-sensitivity testing. 10% of strains isolatedfrom 1500 patients in our hospitals were resistant to co-trimoxazole and all of these were resistant to sulphon-amides with M.l.c.s greater than 512 µg. per ml. Approxi-mately 90% of such resistant strains were isolated frompatients who had been treated with sulphonamides usuallyfor preoperative bowel preparation. Since strains resistantto co-trimoxazole have been encountered in large num-bers elsewhere, 7 find it necessary to perform sensitivitytests on strains of B. fragilis isolated from infections beforerecommending therapy, and I use the Stokes method ofdisc sensitivity testing which is always adequate in routinepractice. Details of our work were not given in the paper 8to which Phillips and Warren refer because the subjectmatter of the paper was primarily clinical. The other
report to which they refer without giving the referencewas a short letter 7.
3. Lancet, 1973, ii, 366.4. Cahill, G. F. Diabetes, 1971, 20, 785.5. Phillips, I., Warren, C. Lancet, May 4, 1974, p. 827.6. Okubadejo, O. A., Green, P. J., Payne, D. J. H. Br. med. J. 1973,
ii, 212.7. Leigh, D. A. Lancet, 1973, ii, 1081.8. Okubadejo, O. A., Green, P. J., Payne, D. J. H. ibid. 1973, i, 147.
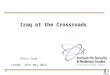
MINIMAL INHIBITORY CONCENTRATIONS OF TRIMETHOPRIM AND
SULPHAMETHOXAZOL FOR B. fragilis STRAINS AND THEIR SENSI-TIVITY TO CO-TRIMOXAZOLE (DISC TESTS)
* Stokes method was used for this test.S = sensitive. R = resistant.
Finally, Phillips and Warren suggested that co-trim-oxazole therapy might give good results in the treatmentof B.fragilis infections; in this hospital 5 patients have beenso treated and have responded well.
St. Mary’s General Hospital,Milton Road,Portsmouth. O. A. OKUBADEJO.
SUBNORMALITY AT THE CROSSROADS
SIR,—Perhaps I may have one more word on this
subject (April 27, p. 814). Dr Robinson is mistaken whenhe says that the term " subnormality
" is creeping back intothe terminology of the medical profession. This term isnot a medical term and was introduced into the MentalHealth Act 1959. In fact, it is still necessary to use this termon legal documents when certification is required.
In recent years a variety of paramedical staff have comeinto hospitals for the mentally handicapped and are con-tinuing to exert considerable influence in the daily routine.This is a good thing from the point of view of the patientsbut it does make the job less attractive from the con-sultant’s point of view, because doctors tend to be indivi-dualistic in their approach to medicine.As far as the future is concerned, perhaps I might quote
from my address to the Royal Society of Health in April,1972:" From the point of view of the consultant in mental handicap,
the next ten years will be a period of profound change." Diagnosis of early mental handicap will be made by the
paediatrician. Education will be the responsibility of the localauthority education department. Residential care will be theresponsibility of the Director of Social Services and the medicalcare of residents will be carried out by the general practitioners.The subnormal psychopath will probably be treated by thegeneral psychiatrist in the psychiatric unit attached to the districtgeneral hospital." What of the future of the consultant in subnormality?
Without question, he will quietly follow the Dodo into extinctionand by 1992 he will probably have disappeared without trace."
Claypenny Hospital,Easingwold, Yorks Y06 3PR. J. NEWCOMBE.