Successes and Evolving Challenges Posed by the Comprehensive In Vitro Proarrhythmia (CiPA) Initiative
Gary Gintant
Dept. Integrative Pharmacology
Integrated Sciences and Technology
AbbVie
For the CiPA Initiative
Outline
• Introduction and Rationale for CiPA Definition and Overarching Goals Scientific Underpinnings
• Components: Progress and Challenges Ionic Currents In Silico Reconstruction Stem-Cell Derived Cardiomyocytes Compound Selection/Regulatory
• Paths Forward and Conclusions
2 CiPA – SPS Webinar April 16, 2015 © 2015
CiPA: Comprehensive In Vitro Proarrhythmia Assay
Goal: Develop a new in vitro paradigm for cardiac safety evaluation of new drugs that provides a more accurate and comprehensive mechanistic-based assessment of proarrhythmic potential
- focus on proarrhythmia (not QT prolongation) to improve specificity compared to preclinical hERG and clinical TQT studies
How? - Define drug effects on multiple human cardiac currents, - Characterize integrated electrophysiologic response using in silico reconstructions of human ventricular electrophysiology, - Verify effects on human stem-cell derived ventricular myocytes
3 CiPA – SPS Webinar April 16, 2015 © 2015
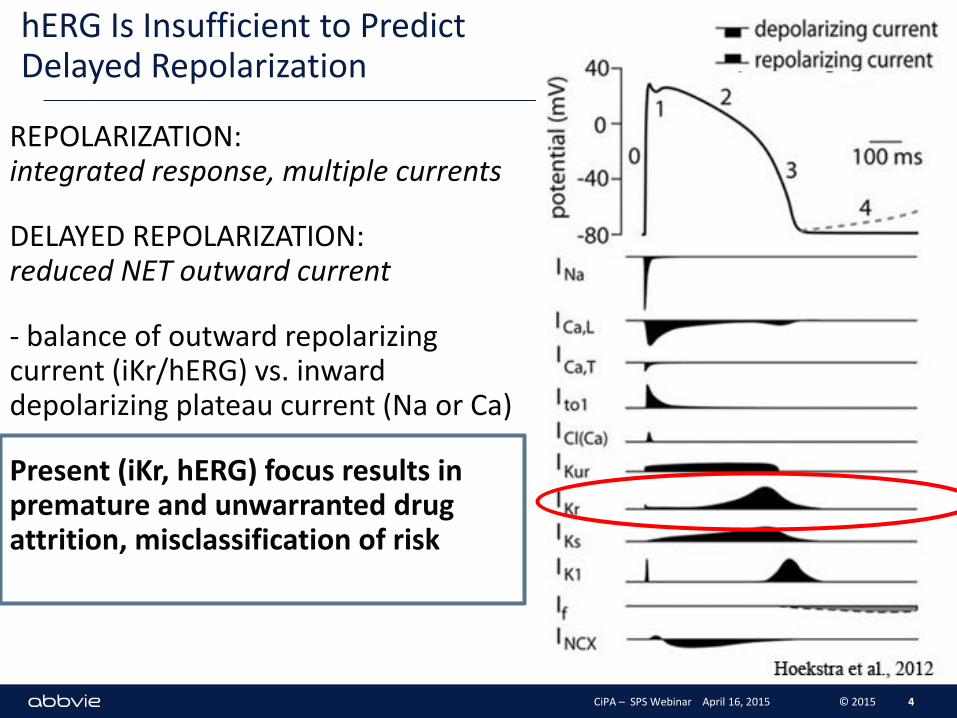
hERG Is Insufficient to Predict Delayed Repolarization
REPOLARIZATION: integrated response, multiple currents
DELAYED REPOLARIZATION: reduced NET outward current
- balance of outward repolarizing current (iKr/hERG) vs. inward depolarizing plateau current (Na or Ca)
Present (iKr, hERG) focus results in premature and unwarranted drug attrition, misclassification of risk
4 CiPA – SPS Webinar April 16, 2015 © 2015
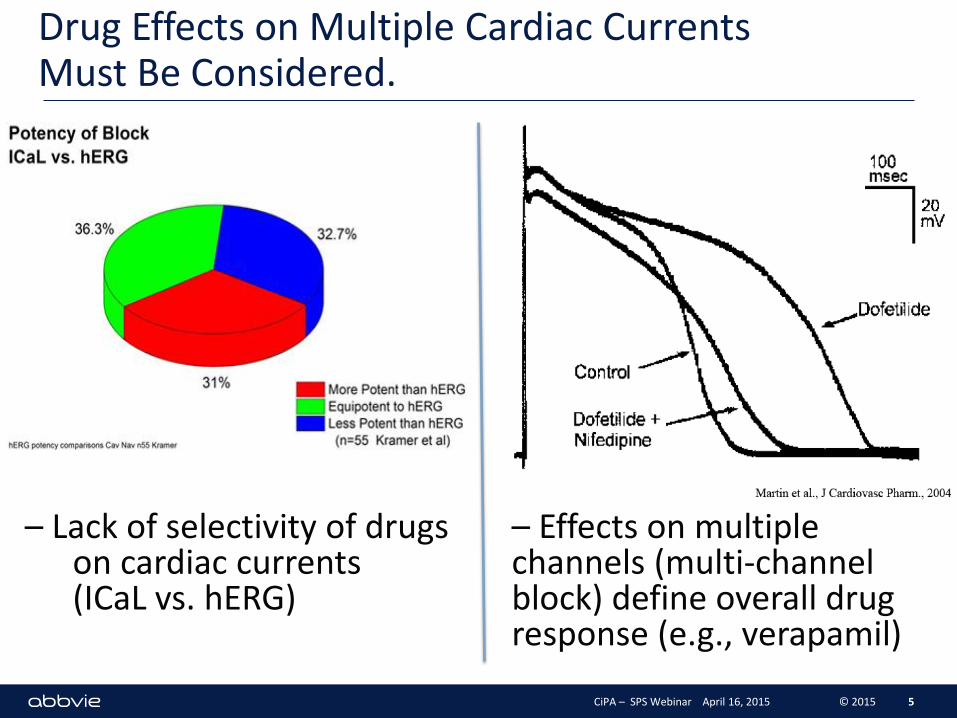
Drug Effects on Multiple Cardiac Currents Must Be Considered.
5
– Lack of selectivity of drugs on cardiac currents (ICaL vs. hERG)
– Effects on multiple channels (multi-channel block) define overall drug response (e.g., verapamil)
CiPA – SPS Webinar April 16, 2015 © 2015
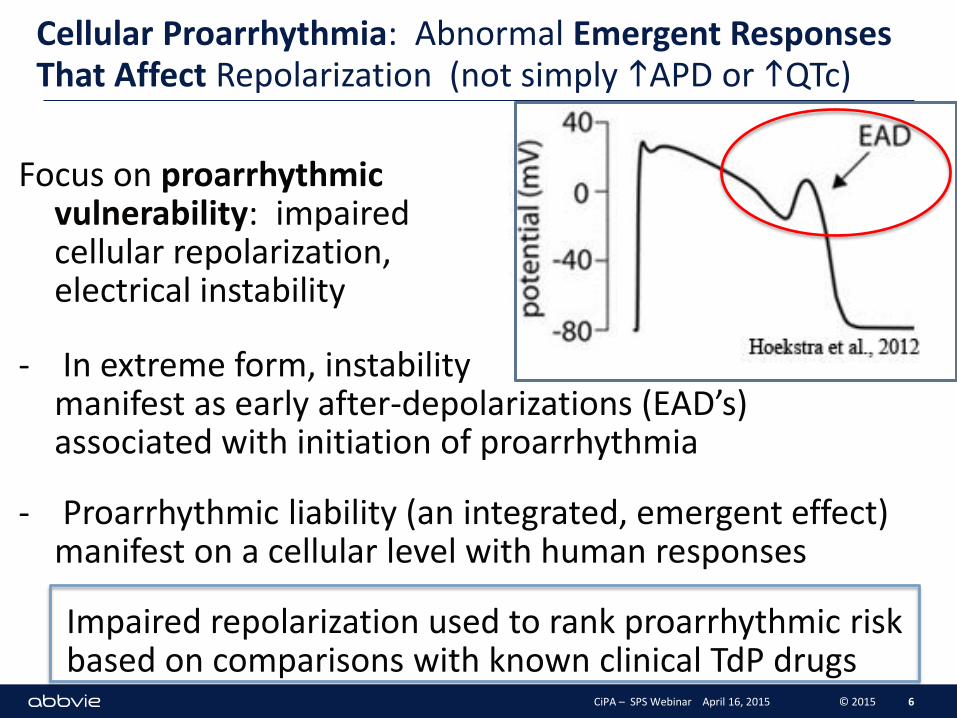
Cellular Proarrhythmia: Abnormal Emergent Responses That Affect Repolarization (not simply hAPD or hQTc)
Focus on proarrhythmic vulnerability: impaired cellular repolarization, electrical instability and l
- In extreme form, instability manifest as early after-depolarizations (EAD’s) associated with initiation of proarrhythmia
- Proarrhythmic liability (an integrated, emergent effect) manifest on a cellular level with human responses
Impaired repolarization used to rank proarrhythmic risk based on comparisons with known clinical TdP drugs
6 CiPA – SPS Webinar April 16, 2015 © 2015
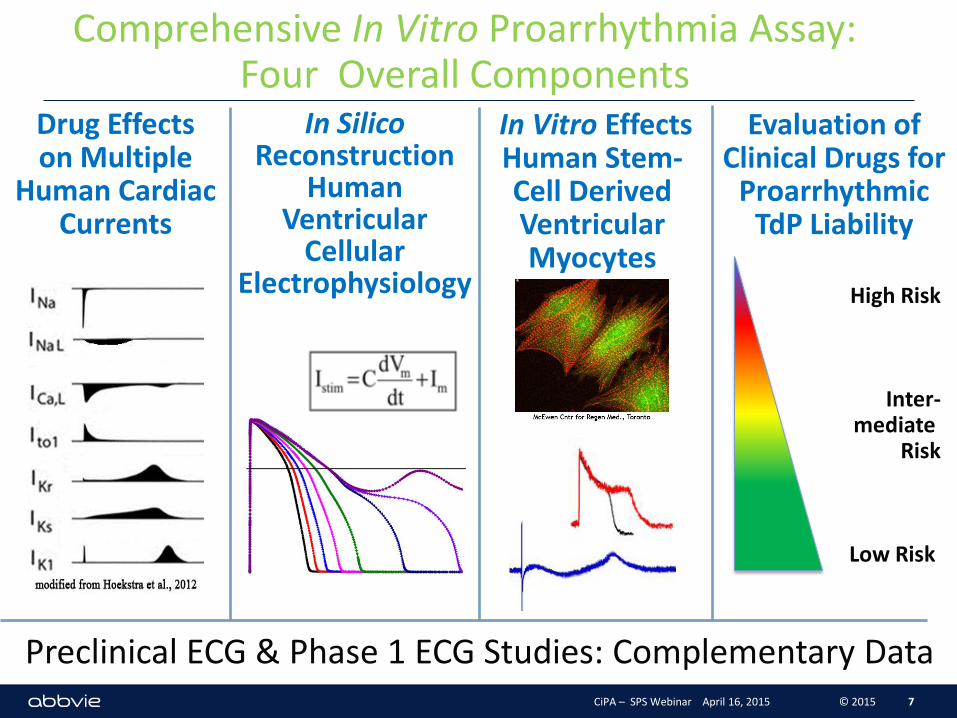
Comprehensive In Vitro Proarrhythmia Assay: Four Overall Components
Evaluation of Clinical Drugs for
Proarrhythmic TdP Liability
7
Drug Effects on Multiple
Human Cardiac Currents
In Silico Reconstruction
Human Ventricular
Cellular Electrophysiology
In Vitro Effects Human Stem-Cell Derived Ventricular Myocytes
High Risk
Inter- mediate
Risk
Low Risk
Preclinical ECG & Phase 1 ECG Studies: Complementary Data CiPA – SPS Webinar April 16, 2015 © 2015
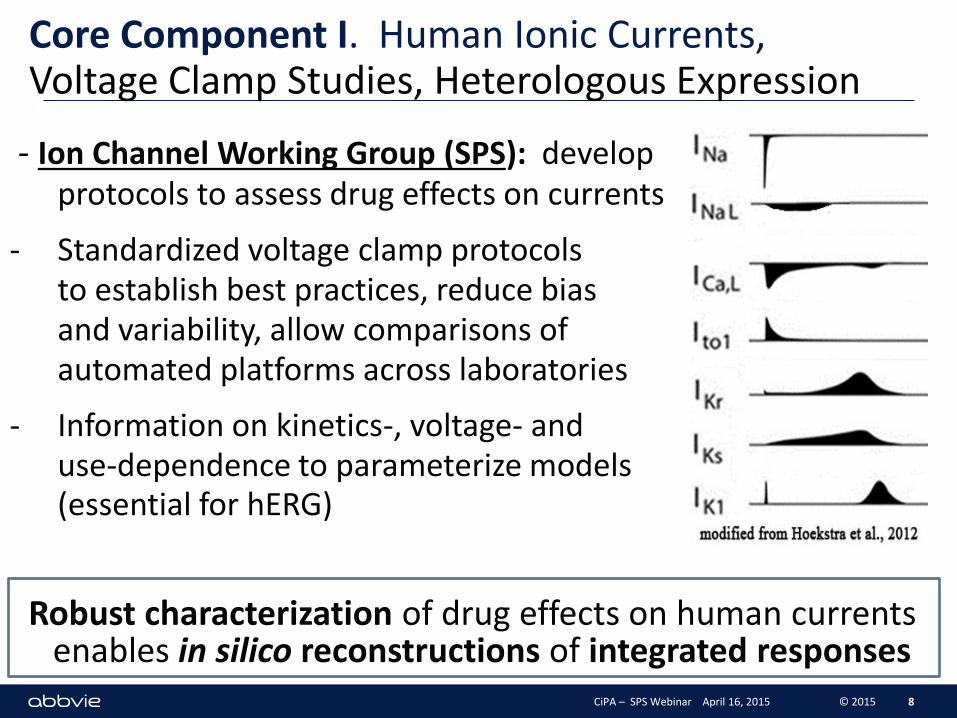
Core Component I. Human Ionic Currents, Voltage Clamp Studies, Heterologous Expression
- Ion Channel Working Group (SPS): develop protocols to assess drug effects on currents
- Standardized voltage clamp protocols to establish best practices, reduce bias and variability, allow comparisons of automated platforms across laboratories
- Information on kinetics-, voltage- and use-dependence to parameterize models for (essential for hERG)
Robust characterization of drug effects on human currents enables in silico reconstructions of integrated responses
8 CiPA – SPS Webinar April 16, 2015 © 2015
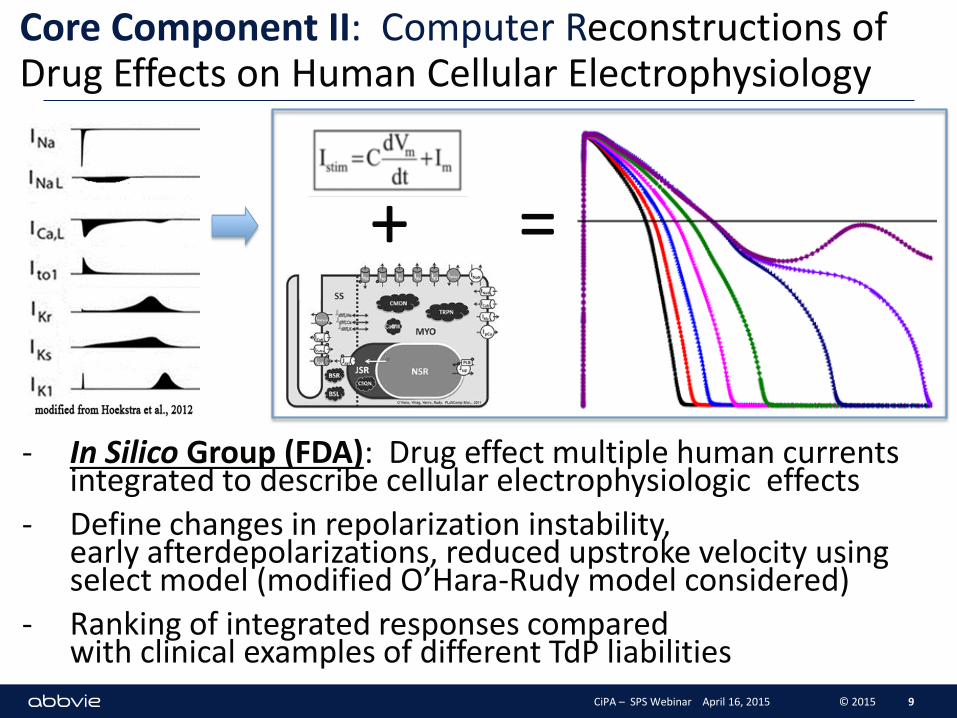
- In Silico Group (FDA): Drug effect multiple human currents integrated to describe cellular electrophysiologic effects
- Define changes in repolarization instability, early afterdepolarizations, reduced upstroke velocity using select model (modified O’Hara-Rudy model considered)
- Ranking of integrated responses compared with clinical examples of different TdP liabilities
Core Component II: Computer Reconstructions of Drug Effects on Human Cellular Electrophysiology
9
+ =
CiPA – SPS Webinar April 16, 2015 © 2015
Core Component II. Computer Reconstructions: Progress (FDA Lead)
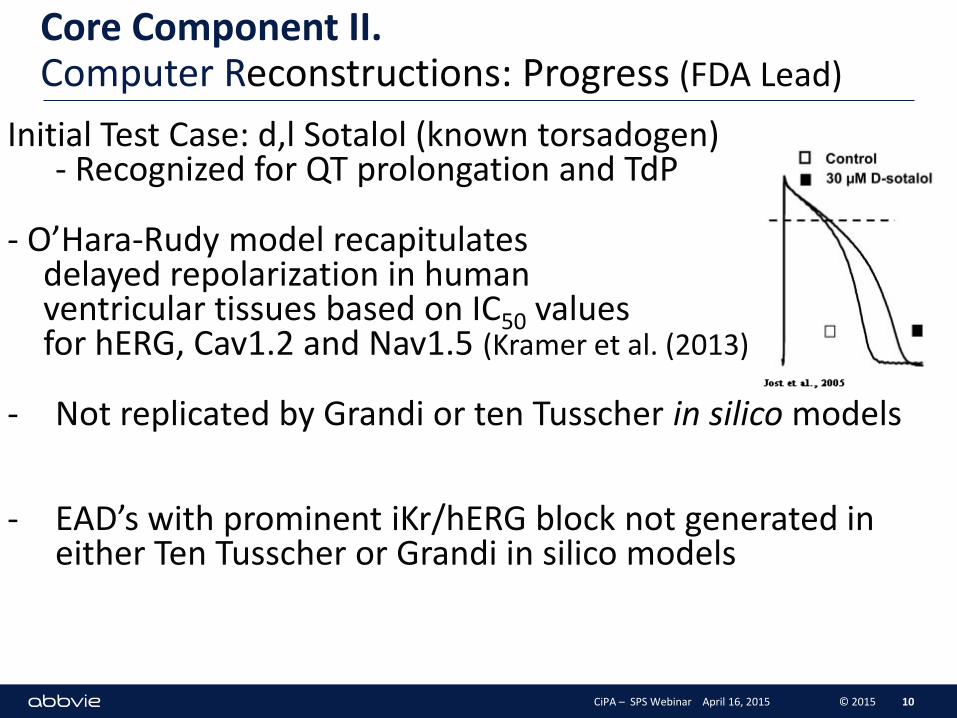
Initial Test Case: d,l Sotalol (known torsadogen) - Recognized for QT prolongation and TdP
- O’Hara-Rudy model recapitulates delayed repolarization in human ventricular tissues based on IC50 values for hERG, Cav1.2 and Nav1.5 (Kramer et al. (2013)
- Not replicated by Grandi or ten Tusscher in silico models
- EAD’s with prominent iKr/hERG block not generated in either Ten Tusscher or Grandi in silico models
10 CiPA – SPS Webinar April 16, 2015 © 2015
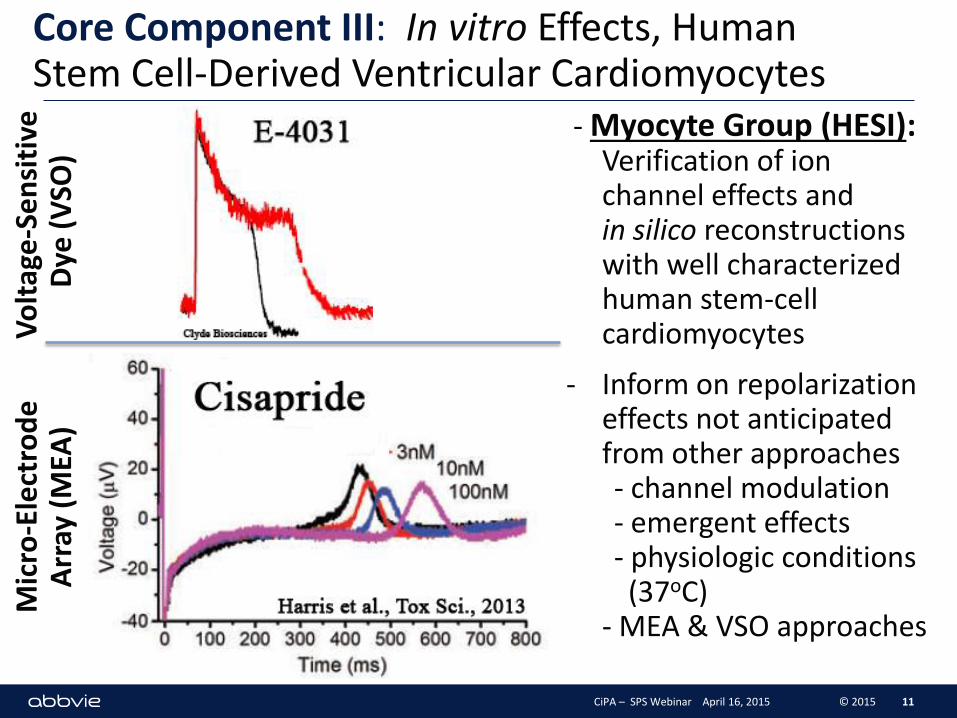
Core Component III: In vitro Effects, Human Stem Cell-Derived Ventricular Cardiomyocytes
- Myocyte Group (HESI): Verification of ion channel effects and in silico reconstructions with well characterized human stem-cell cardiomyocytes
- Inform on repolarization effects not anticipated from other approaches - channel modulation - emergent effects - physiologic conditions (37oC) - MEA & VSO approaches
11
Vo
ltag
e-S
en
siti
ve
Dye
(V
SO)
Mic
ro-E
lect
rod
e
Arr
ay (
MEA
)
CiPA – SPS Webinar April 16, 2015 © 2015
Core Component III. Cardiomyocytes- Microelectrode Array (MEA) Pilot Study
12 CiPA – SPS Webinar April 16, 2015 © 2015
12 site Pilot Study
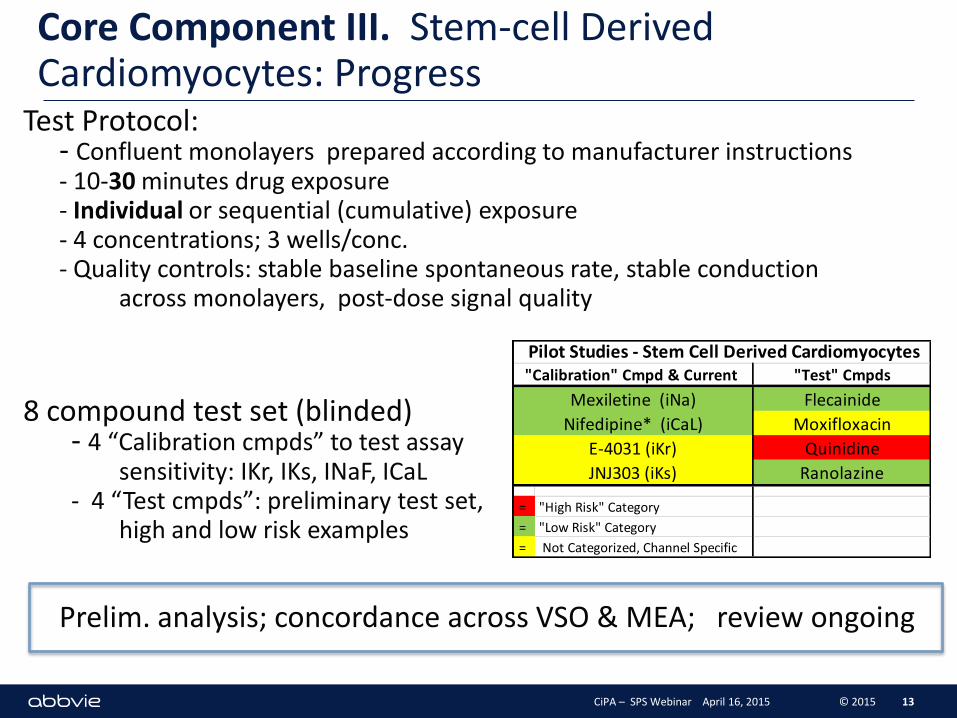
Core Component III. Stem-cell Derived Cardiomyocytes: Progress
Test Protocol: - Confluent monolayers prepared according to manufacturer instructions - 10-30 minutes drug exposure - Individual or sequential (cumulative) exposure - 4 concentrations; 3 wells/conc. - Quality controls: stable baseline spontaneous rate, stable conduction across monolayers, post-dose signal quality
8 compound test set (blinded) - 4 “Calibration cmpds” to test assay sensitivity: IKr, IKs, INaF, ICaL - 4 “Test cmpds”: preliminary test set, high and low risk examples
Prelim. analysis; concordance across VSO & MEA; review ongoing
13
"Test" Cmpds
Flecainide
Moxifloxacin
Quinidine
Ranolazine
= "High Risk" Category
= "Low Risk" Category
= Not Categorized, Channel Specific
Mexiletine (iNa)
Nifedipine* (iCaL)
E-4031 (iKr)
JNJ303 (iKs)
Pilot Studies - Stem Cell Derived Cardiomyocytes"Calibration" Cmpd & Current
CiPA – SPS Webinar April 16, 2015 © 2015
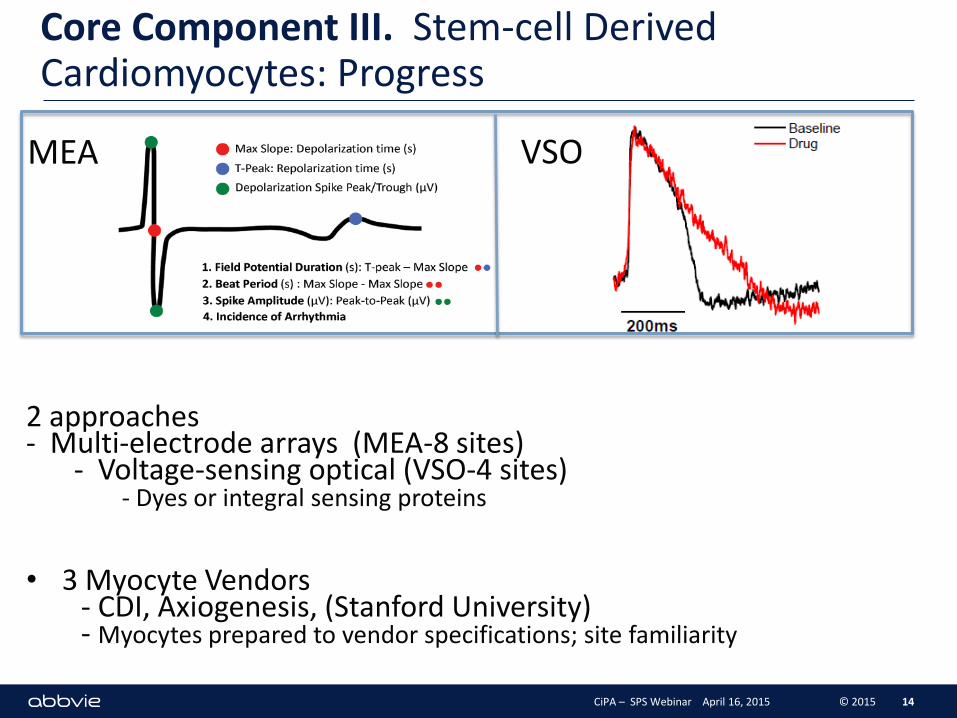
Core Component III. Stem-cell Derived Cardiomyocytes: Progress
2 approaches - Multi-electrode arrays (MEA-8 sites) - Voltage-sensing optical (VSO-4 sites) - Dyes or integral sensing proteins
• 3 Myocyte Vendors - CDI, Axiogenesis, (Stanford University) - Myocytes prepared to vendor specifications; site familiarity
14
MEA VSO
CiPA – SPS Webinar April 16, 2015 © 2015
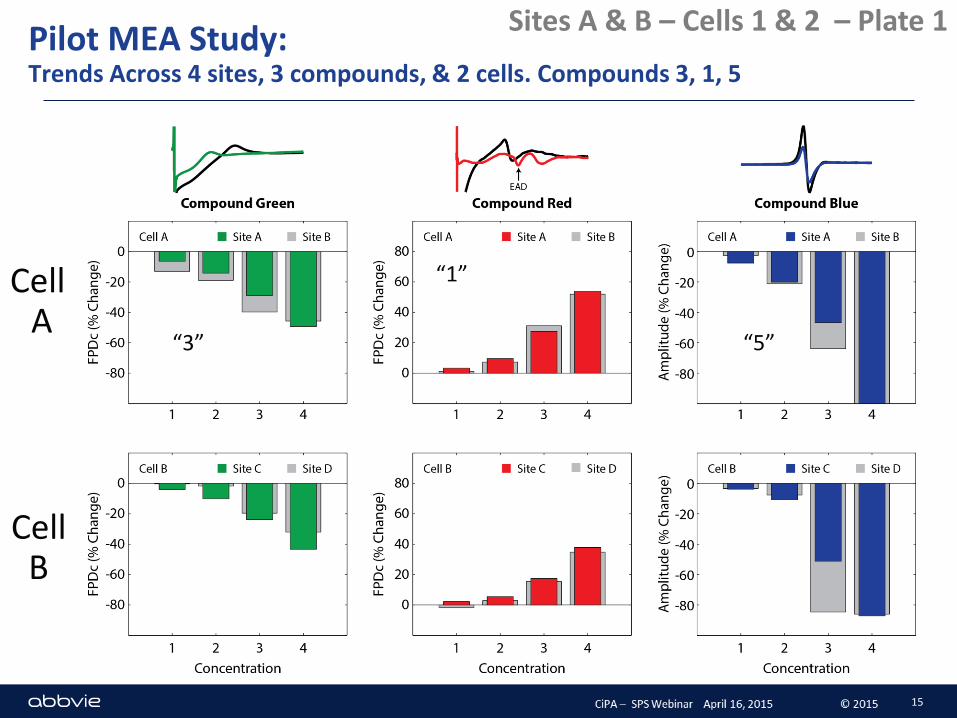
Pilot MEA Study: Trends Across 4 sites, 3 compounds, & 2 cells. Compounds 3, 1, 5
Sites A & B – Cells 1 & 2 – Plate 1
“3”
“1”
“5”
15
Cell A
Cell B
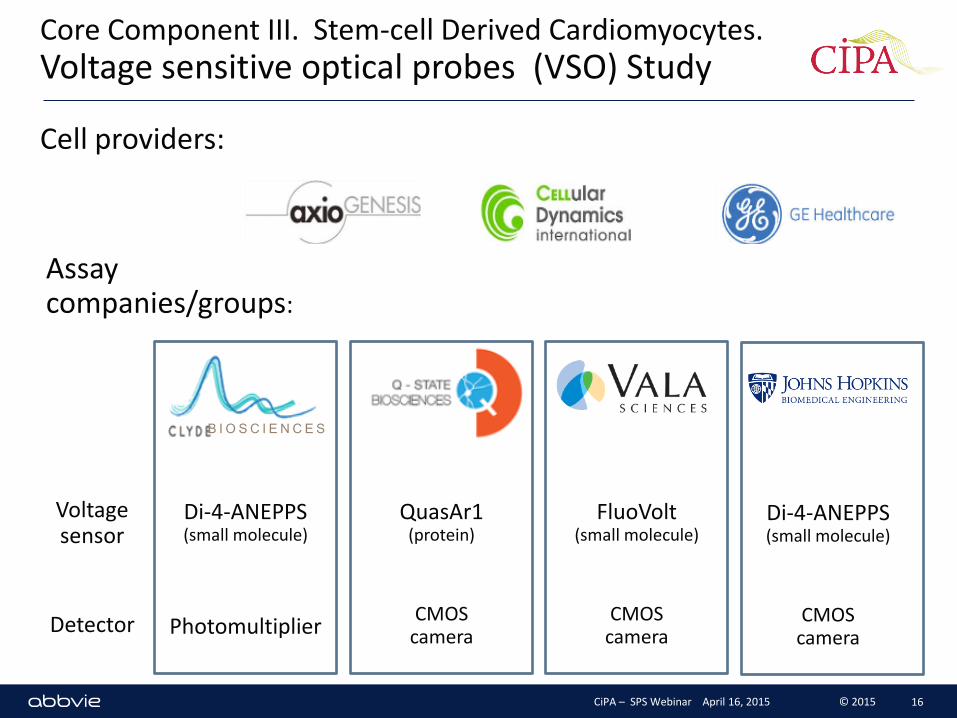
Core Component III. Stem-cell Derived Cardiomyocytes. Voltage sensitive optical probes (VSO) Study
Cell providers:
Assay companies/groups:
Voltage sensor
Detector
QuasAr1 (protein)
CMOS camera
FluoVolt (small molecule)
CMOS camera
Di-4-ANEPPS (small molecule)
CMOS camera
Di-4-ANEPPS (small molecule)
Photomultiplier
B I O S C I E N C E S
CiPA – SPS Webinar April 16, 2015 © 2015 16
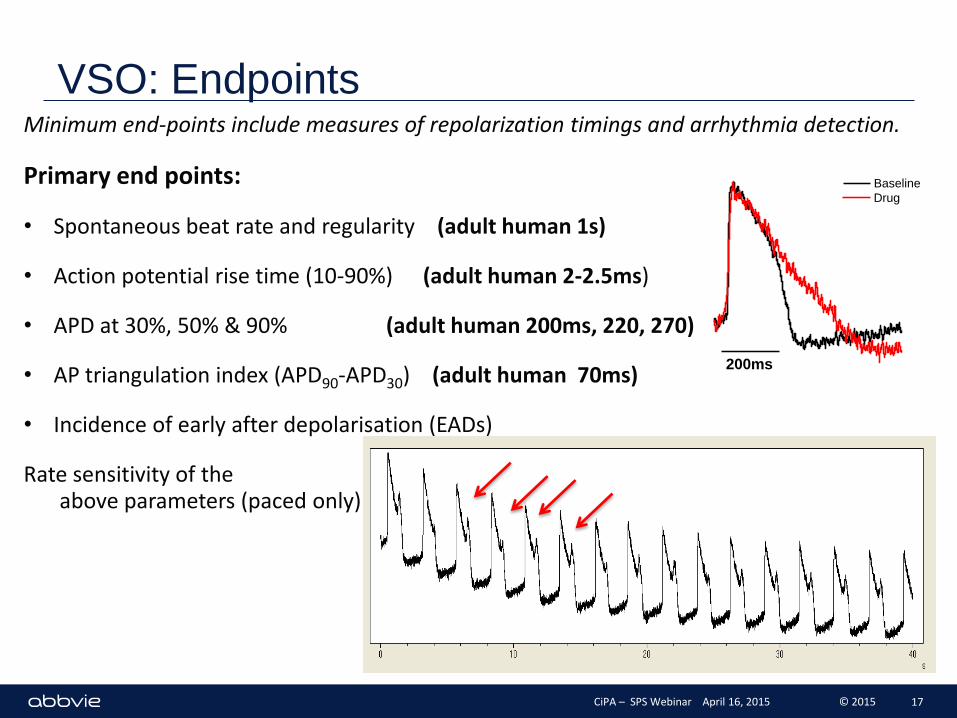
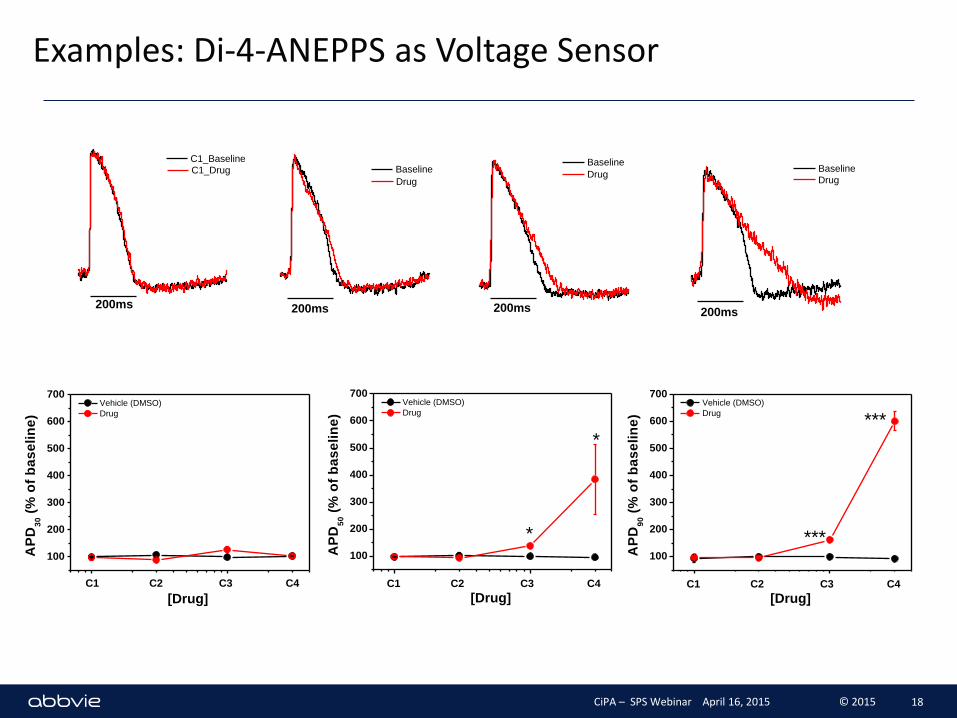
VSO: Endpoints Minimum end-points include measures of repolarization timings and arrhythmia detection.
Primary end points:
• Spontaneous beat rate and regularity (adult human 1s)
• Action potential rise time (10-90%) (adult human 2-2.5ms)
• APD at 30%, 50% & 90% (adult human 200ms, 220, 270)
• AP triangulation index (APD90-APD30) (adult human 70ms)
• Incidence of early after depolarisation (EADs)
Rate sensitivity of the above parameters (paced only)
200ms
Baseline
Drug
CiPA – SPS Webinar April 16, 2015 © 2015 17
C1_Baseline
200ms
C1_Drug
200ms
Baseline
Drug
200ms
Baseline
Drug
200ms
Baseline
Drug
100
200
300
400
500
600
700
AP
D3
0 (
% o
f b
as
eli
ne
)
Vehicle (DMSO)
Drug
[Drug]
C1 C2 C3 C4
100
200
300
400
500
600
700
*
*
AP
D5
0 (
% o
f b
as
eli
ne
)
Vehicle (DMSO)
Drug
[Drug] C1 C2 C3 C4
100
200
300
400
500
600
700
***
***
AP
D9
0 (
% o
f b
as
eli
ne
)
Vehicle (DMSO)
Drug
[Drug] C1 C2 C3 C4
Examples: Di-4-ANEPPS as Voltage Sensor
CiPA – SPS Webinar April 16, 2015 © 2015 18
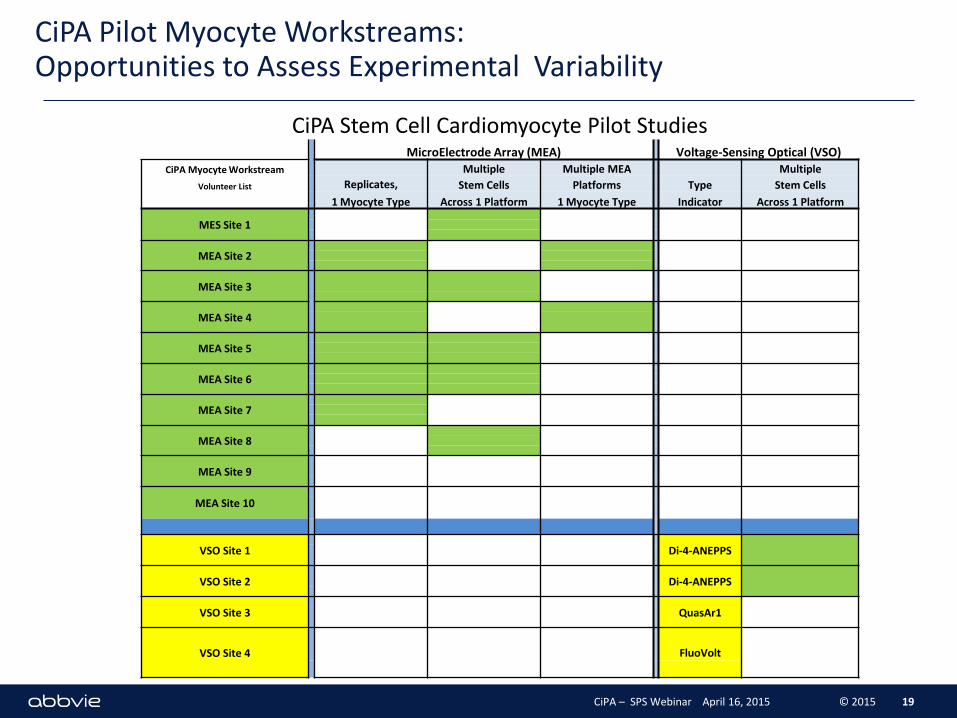
CiPA Pilot Myocyte Workstreams: Opportunities to Assess Experimental Variability
19
CiPA Stem Cell Cardiomyocyte Pilot Studies MicroElectrode Array (MEA) Voltage-Sensing Optical (VSO)
CiPA Myocyte Workstream Multiple Multiple MEA Multiple
Volunteer List Replicates, Stem Cells Platforms Type Stem Cells
1 Myocyte Type Across 1 Platform 1 Myocyte Type Indicator Across 1 Platform
MES Site 1
MEA Site 2
MEA Site 3
MEA Site 4
MEA Site 5
MEA Site 6
MEA Site 7
MEA Site 8
MEA Site 9
MEA Site 10
VSO Site 1
Di-4-ANEPPS
VSO Site 2
Di-4-ANEPPS
VSO Site 3
QuasAr1
VSO Site 4
FluoVolt
CiPA – SPS Webinar April 16, 2015 © 2015
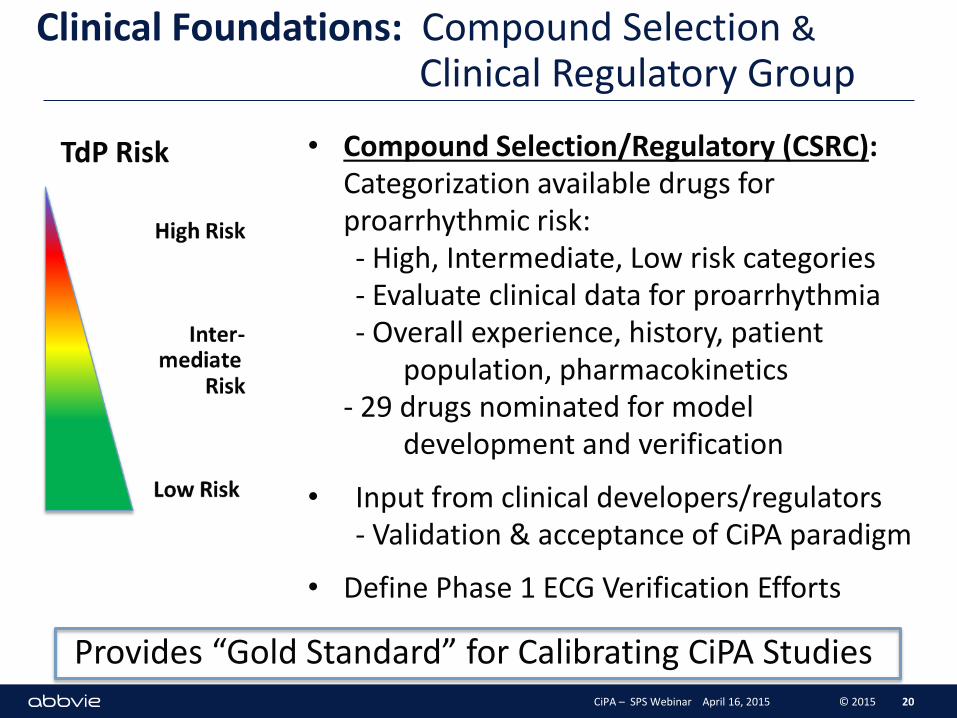
Clinical Foundations: Compound Selection & Clinical Regulatory Group
• Compound Selection/Regulatory (CSRC): Categorization available drugs for proarrhythmic risk: - High, Intermediate, Low risk categories - Evaluate clinical data for proarrhythmia - Overall experience, history, patient population, pharmacokinetics - 29 drugs nominated for model development and verification
• Input from clinical developers/regulators - Validation & acceptance of CiPA paradigm
• Define Phase 1 ECG Verification Efforts
20
TdP Risk
CiPA – SPS Webinar April 16, 2015 © 2015
Provides “Gold Standard” for Calibrating CiPA Studies
Criteria for Compound Selection
- No prominent proarrhythmic / active metabolites
- Good solubility
- Defined cellular electrophysiology
- Ranking compounds based on clinically demonstrated torsadogenic risk and proarrhythmic incidence - published reports, FDA AERS database, additional data sources, expert opinion
- Compounds grouped into ‘high’, ‘intermediate’ and ‘very low’ (i.e., none) risk categories - Intermediate risk compounds grouped into one category - ‘Very low’ risk no discernable risk
- Culled from much larger list of candidates 21 CiPA – SPS Webinar April 16, 2015 © 2015
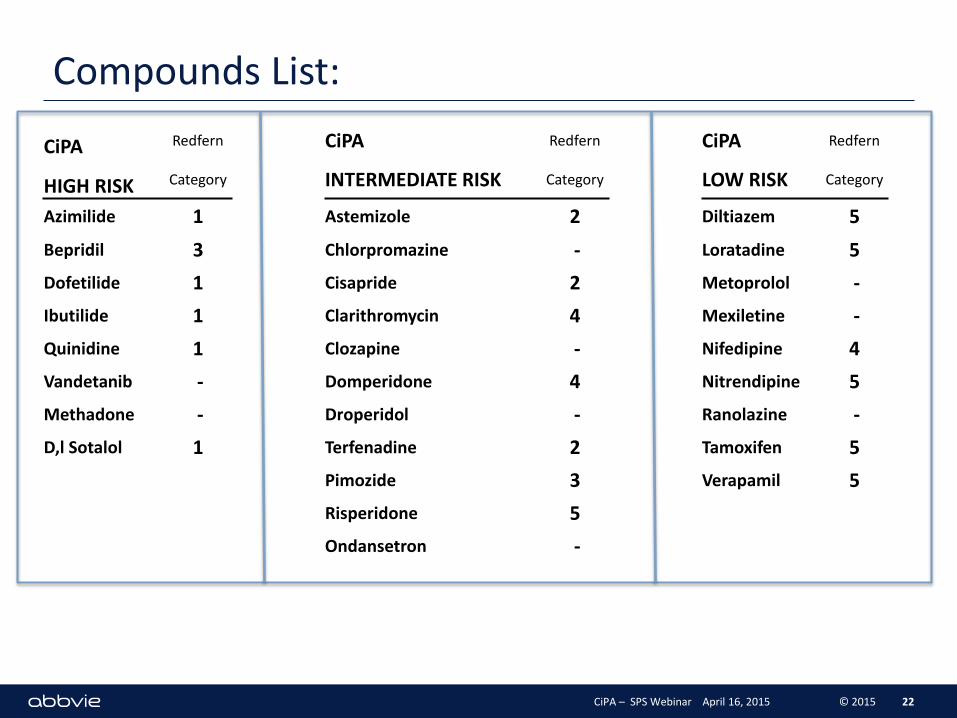
Compounds List:
22
CiPA Redfern CiPA Redfern CiPA Redfern
HIGH RISK Category INTERMEDIATE RISK Category LOW RISK Category
Azimilide 1 Astemizole 2 Diltiazem 5
Bepridil 3 Chlorpromazine - Loratadine 5
Dofetilide 1 Cisapride 2 Metoprolol -
Ibutilide 1 Clarithromycin 4 Mexiletine -
Quinidine 1 Clozapine - Nifedipine 4
Vandetanib - Domperidone 4 Nitrendipine 5
Methadone - Droperidol - Ranolazine -
D,l Sotalol 1 Terfenadine 2 Tamoxifen 5
Pimozide 3 Verapamil 5
Risperidone 5
Ondansetron -
CiPA – SPS Webinar April 16, 2015 © 2015
Group Efforts Against Timelines
Parties Involved:
Cardiac Safety Research Consortium: Cmpd Selection Team FDA: In Silico Working Group ILSI-HESI: Myocyte Stem Cell Working Group Safety Pharm. Society: Ion Channel Working Group
J-iCSA – 2015(?)
Regulators: FDA, Health Canada, EMEA, Japan Japanese Safety Pharmacology Society Academic Contributors Vendors and Suppliers
Timelines: Progress Review: 1Q 2016
23 CiPA – SPS Webinar April 16, 2015 © 2015
Future Activities: CiPA 2015
Refinement-Evaluations of Voltage Clamp Protocols
Preliminary test of In Silico Reconstructions Based on Ionic Current Studies
Assessment of CiPA Stem Cell Cardiomyocyte Pilot Study Results - Planning / Initiation of Validation Studies - Define set of validation compounds - Consult/collaborate/compare with J-iCSA
Further discussion with Regulators - Expectations of CiPA Package of regulators, industry - Relation to eQT Clinical Efforts - How to integrate in vitro/in silico preclinical results with emerging clinical eQT approaches
24 CiPA – SPS Webinar April 16, 2015 © 2015
CiPA: proarrhythmic risk assessment based on mechanistic understanding of integrated, cellular emergent drug effects on multiple human cardiac currents
Expectations: - reduce unwarranted attrition early candidates - enable rapid progression of low risk TdP drugs to phase 1 studies (and confirmatory clinical ECG findings)
25 CiPA – SPS Webinar April 16, 2015 © 2015
Recommended