Embed Size (px)
Citation preview

Sudden death of neuromyelitis optica: A case report of clinical missed diagnosis
Luo Zhuo1, Shaohua Zhu1, Tingyi Sun1, Rongshuai Wang1, Liang Ren1, Liang Liu1,2*
_________________________________________________________________________________________ Abstract: Deaths of clinical miss-diagnosed diseases are caused by various reasons. Similar symptoms shared by different diseases and the recent medical history could affect the judgement of clinicians sometimes, especially when the disease is unusually found. We present a case of sudden death in hospital. Patient was admitted with sudden visual loss and quadriplegia. He died suddenly without certain pathogenesis next day. The medical history showed he had head injury recently. The autopsy revealed scattered inflammatory demyelination in optic nerves and spinal cord. Postmortem serological testing showed positive result of neuromyelitis optica-IgG. Therefore, the cause of death is severe respiratory distress due to acute neuromyelitis optica. Key Words: neuromyelitis optica; autopsy; sudden death; forensic pathology.
1) Department of Forensic Medicine, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China*Corresponding author: M.D.,Ph.D., Department of Forensic Medicine, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, China, Key Laboratory of Evidence Science, China University of Political Science and Law, Ministry of Education, Beijing, China. 100040, E-mail: [email protected], Fax: +8627836926382) Key Laboratory of Evidence Science, China University of Political Science and Law, Ministry of Education, Beijing, China
Rom J Leg Med [20] 247-250 [2012]DOI: 10.4323/rjlm.2012.247© 2012 Romanian Society of Legal Medicine
247
Sudden deaths due to unrecognized disease in hospital are not infrequent and always
concerned by forensic pathologists. Clinically missed diagnoses of disease are attributed to various reasons. The unusual diseases, different entities that share the same manifestations or the recent medical history of injury may affect the accurate diagnosis. We report a case of sudden death during hospitalization due to clinically unrecognized disease. The forensic examination revealed the cause of death was acute neuromyelitis optica, which is seldom reported in the field of forensic medicine.
CASE REPORT
A 52-year-old male was sent to hospital with sudden onset of visual loss and loss of strength of lower extremities. He reported a history of head injury due to a fight nearly one month ago but denied any headache, nausea or seizure at this time. Physical examinations showed vital
signs within the normal range(temperature: 35.8°C, pulse rate: 58 beats per minute, respiratory: 14 breaths per minute, blood pressure: 113/67mmHg), stiff neck, lower extremity weakness, urinary retention, and sensory impairment under T12 level. Computerized tomography (CT) scan of the brain was unremarkable. In the next day, the patient suddenly appeared cyanosis and was admitted to the intensive care unit with respiratory failure. Despite resuscitation efforts with intubation were performed immediately, he progressed to unconsciousness and ensuing death. Clinical diagnosis was undetermined. Therefore, a medicolegal examination was required for investigating the cause of death.
AUTOPSY FINDINGS
The body was thawed and absence of rigor. External examination of body revealed a well-developed and medium-nourished male. The body length was 169cm.
Liu L. et al. Sudden death of neuromyelitis optica: A case report of clinical missed diagnosis
248
Livor mortis were distributed in the posterior dependent portions of the body. Obvious cyanosis of lips and finger nails were found. A 4 cm long remote scar was found to the right side of the occipital scalp with haemorrhage. No skull fracture was seen. The rest
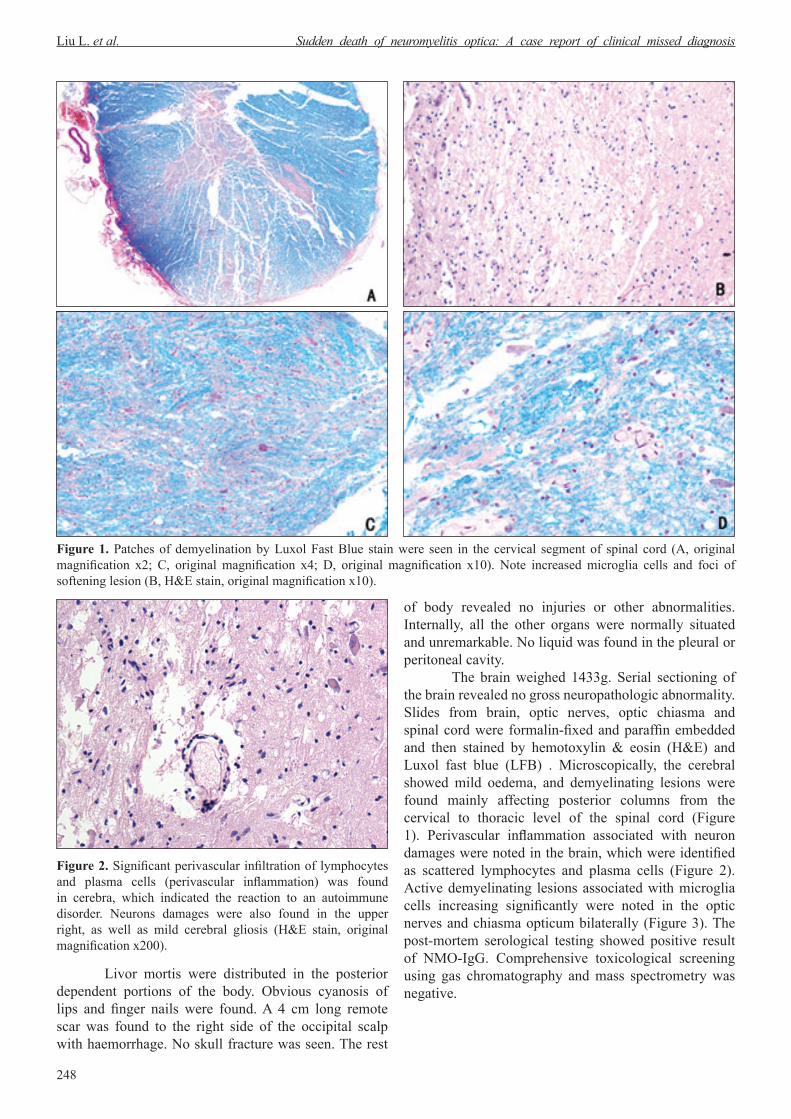
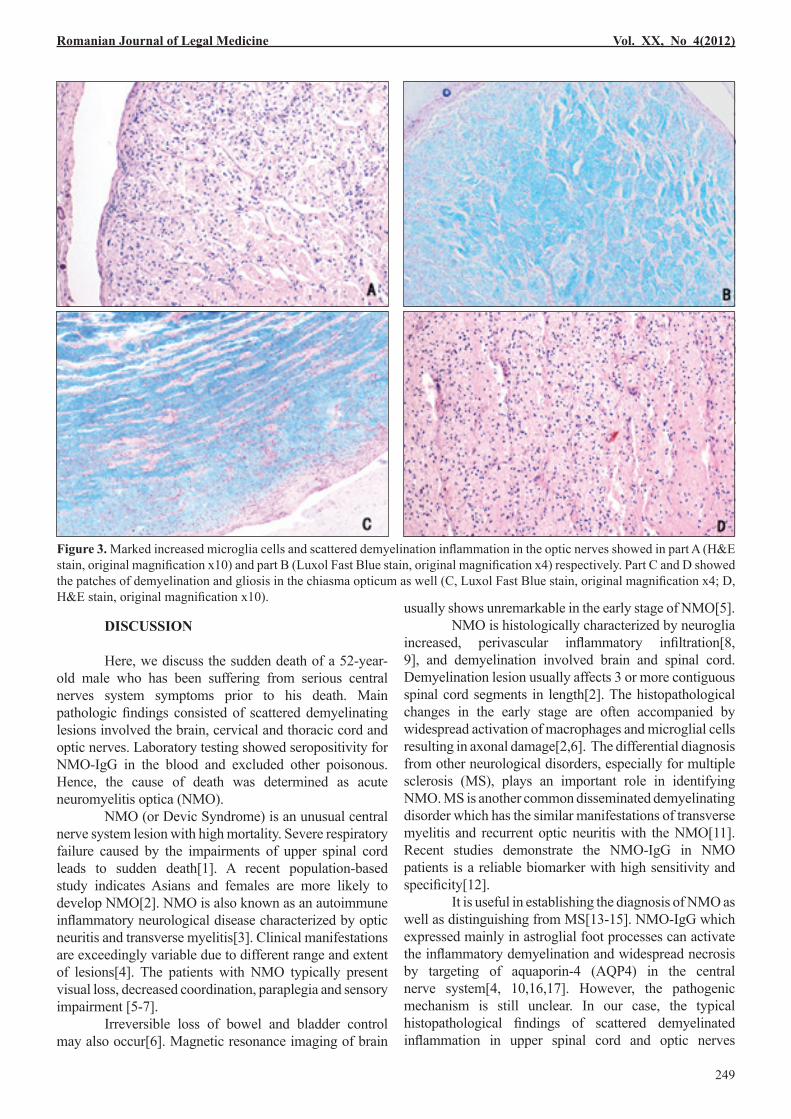
of body revealed no injuries or other abnormalities. Internally, all the other organs were normally situated and unremarkable. No liquid was found in the pleural or peritoneal cavity. The brain weighed 1433g. Serial sectioning of the brain revealed no gross neuropathologic abnormality. Slides from brain, optic nerves, optic chiasma and spinal cord were formalin-fixed and paraffin embedded and then stained by hemotoxylin & eosin (H&E) and Luxol fast blue (LFB) . Microscopically, the cerebral showed mild oedema, and demyelinating lesions were found mainly affecting posterior columns from the cervical to thoracic level of the spinal cord (Figure 1). Perivascular inflammation associated with neuron damages were noted in the brain, which were identified as scattered lymphocytes and plasma cells (Figure 2). Active demyelinating lesions associated with microglia cells increasing significantly were noted in the optic nerves and chiasma opticum bilaterally (Figure 3). The post-mortem serological testing showed positive result of NMO-IgG. Comprehensive toxicological screening using gas chromatography and mass spectrometry was negative.
Figure 1. Patches of demyelination by Luxol Fast Blue stain were seen in the cervical segment of spinal cord (A, original magnification x2; C, original magnification x4; D, original magnification x10). Note increased microglia cells and foci of softening lesion (B, H&E stain, original magnification x10).
Figure 2. Significant perivascular infiltration of lymphocytes and plasma cells (perivascular inflammation) was found in cerebra, which indicated the reaction to an autoimmune disorder. Neurons damages were also found in the upper right, as well as mild cerebral gliosis (H&E stain, original magnification x200).
DISCUSSION
Here, we discuss the sudden death of a 52-year-old male who has been suffering from serious central nerves system symptoms prior to his death. Main pathologic findings consisted of scattered demyelinating lesions involved the brain, cervical and thoracic cord and optic nerves. Laboratory testing showed seropositivity for NMO-IgG in the blood and excluded other poisonous. Hence, the cause of death was determined as acute neuromyelitis optica (NMO). NMO (or Devic Syndrome) is an unusual central nerve system lesion with high mortality. Severe respiratory failure caused by the impairments of upper spinal cord leads to sudden death[1]. A recent population-based study indicates Asians and females are more likely to develop NMO[2]. NMO is also known as an autoimmune inflammatory neurological disease characterized by optic neuritis and transverse myelitis[3]. Clinical manifestations are exceedingly variable due to different range and extent of lesions[4]. The patients with NMO typically present visual loss, decreased coordination, paraplegia and sensory impairment [5-7]. Irreversible loss of bowel and bladder control may also occur[6]. Magnetic resonance imaging of brain
usually shows unremarkable in the early stage of NMO[5]. NMO is histologically characterized by neuroglia increased, perivascular inflammatory infiltration[8, 9], and demyelination involved brain and spinal cord. Demyelination lesion usually affects 3 or more contiguous spinal cord segments in length[2]. The histopathological changes in the early stage are often accompanied by widespread activation of macrophages and microglial cells resulting in axonal damage[2,6]. The differential diagnosis from other neurological disorders, especially for multiple sclerosis (MS), plays an important role in identifying NMO. MS is another common disseminated demyelinating disorder which has the similar manifestations of transverse myelitis and recurrent optic neuritis with the NMO[11]. Recent studies demonstrate the NMO-IgG in NMO patients is a reliable biomarker with high sensitivity and specificity[12]. It is useful in establishing the diagnosis of NMO as well as distinguishing from MS[13-15]. NMO-IgG which expressed mainly in astroglial foot processes can activate the inflammatory demyelination and widespread necrosis by targeting of aquaporin-4 (AQP4) in the central nerve system[4, 10,16,17]. However, the pathogenic mechanism is still unclear. In our case, the typical histopathological findings of scattered demyelinated inflammation in upper spinal cord and optic nerves
Romanian Journal of Legal Medicine Vol. XX, No 4(2012)
249
Figure 3. Marked increased microglia cells and scattered demyelination inflammation in the optic nerves showed in part A (H&E stain, original magnification x10) and part B (Luxol Fast Blue stain, original magnification x4) respectively. Part C and D showed the patches of demyelination and gliosis in the chiasma opticum as well (C, Luxol Fast Blue stain, original magnification x4; D, H&E stain, original magnification x10).

250
Liu L. et al. Sudden death of neuromyelitis optica: A case report of clinical missed diagnosis
by specific stain and the positive serological results of NMO-IgG strongly demonstrated the conclusion of NMO according to the latest diagnostic criteria[7,13]. Clinical features of this case were noteworthy, including typical bilateral visual loss, quadriplegia and bladder dysfunction, unremarkable premonitory symptoms, negative radiographical findings of the brain, rapid deterioration to severe respiratory failure and death. According to the investigation of the medical history, a record of 17 days hospitalization due to injuries caused by street fight was documented prior to his last admission in hospital. Treatment for the scalp laceration and rib fractures were performed. Neither intracranial haemorrhage nor central nerve system abnormalities were found at that time. When he was re-admitted with the arising of visual and spinal cord symptoms, clinicians reviewed the records of injuries and considered about the complications of the previous head injury. They tried to relieve the symptoms but finally failed. The pathogenesis was not yet determined till the patient died. Clinically missed diagnosis of disease may be attributed to various reasons. In this present case, the recent history of head injury interfered with the clinicians’ judgement of the symptoms. Neurological manifestations from traumatic lesions vary and they are easily confused with other central nerve system disorders. Delayed
deaths or symptoms after minor head injury without unconsciousness were infrequently reported. Auer and his colleagues[18] had ever described a case that the victim died unexpectedly seven weeks after the minor head injury due to the vertebral artery injury and haemorrhagic infarction. In such cases of delayed death after head injury, the major pathological findings included infarction, thrombi and haemorrhage in cerebra[19]. In the present case, no significant findings revealing recent traumatic lesions of the central nerve system were seen both grossly and microscopically. NMO can pose a diagnostic challenge to both clinicians and forensic pathologists when dealing with such case because myriad of disorders could show similar symptoms of NMO, including the multiple sclerosis and neuropathological disorders following head trauma[4]. It is not that common to have such a case that the NMO happened to occur after a head injury. In most cases, an accurate diagnosis of NMO can be made based on a thorough medical history investigation followed by a complete neuropathological examination and serological testing[20]. The present case illustrates the death may occur a considerable time after the injury due to autoimmune diseases which could have nothing to do with the previous injuries. Complete forensic examination should be performed to find out the accurate cause of death.
References1. Carod Artal FJ, Brenner C, Melo M, del Negro MC, Pereira R. Devic's neuromyelitis optica. Presentation of 2 new cases and review of
the bibliography. Neurologia. 2000 Aug-Sep;15(7):307-12.2. Wingerchuk DM. Diagnosis and treatment of neuromyelitis optica. Neurologist. 2007 Jan;13(1):2-11.3. Nakamura M, Misu T, Fujihara K, Miyazawa I, Nakashima I, Takahashi T, et al. Occurrence of acute large and edematous callosal lesions
in neuromyelitis optica. Mult Scler. 2009 Jun;15(6):695-700.4. Hazin R, Khan F, Bhatti MT. Neuromyelitis optica: current concepts and prospects for future management. Curr Opin Ophthalmol. 2009
Nov;20(6):434-9.5. Cree B. Neuromyelitis optica: diagnosis, pathogenesis, and treatment. Curr Neurol Neurosci Rep. 2008 Sep;8(5):427-33.6. Matiello M, Jacob A, Wingerchuk DM, Weinshenker BG. Neuromyelitis optica. Curr Opin Neurol. 2007 Jun;20(3):255-60.7. Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica.
Neurology. 2006 May 23;66(10):1485-9.8. Almekhlafi MA, Clark AW, Lucchinetti CF, Zhang Y, Power C, Bell RB. Neuromyelitis optica with extensive active brain involvement:
an autopsy study. Arch Neurol. 2011 Apr;68(4):508-12.9. Parratt JD, Prineas JW. Neuromyelitis optica: a demyelinating disease characterized by acute destruction and regeneration of perivascular
astrocytes. Mult Scler. 2010 Oct;16(10):1156-72.10. de Seze J, Arndt C, Jeanjean L, Zephir H, Blanc F, Labauge P, Bouyon M, Ballonzoli L, Fleury M, Vermersch P, Speeg, C. Relapsing
inflammatory optic neuritis: is it neuromyelitis optica? Neurology. 2008 May 27;70(22):2075-6.11. Pandit L. Transverse myelitis spectrum disorders. Neurol India. 2009 Mar-Apr;57(2):126-33.12. Lennon VA, Wingerchuk DM, Kryzer TJ. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis.
Lancet 2004;364:2106–2112.13. Jacob A. Neuromyelitis optica - an update: 2007-2009. Ann Indian Acad Neurol. 2009 Oct;12(4):231-7.14. Misu T, Fujihara K, Kakita A, Konno H, Nakamura M, Watanabe S, et al. Loss of aquaporin 4 in lesions of neuromyelitis optica: distinction
from multiple sclerosis. Brain. 2007 May;130(Pt 5):1224-34.15. Roemer SF, Parisi JE, Lennon VA, Benarroch EE, Lassmann H, Bruck W, et al. Pattern-specific loss of aquaporin-4 immunoreactivity
distinguishes neuromyelitis optica from multiple sclerosis. Brain. 2007 May;130(Pt 5):1194-205.16. Hinson SR, Pittock SJ, Lucchinetti CF, Roemer SF, Fryer JP, Kryzer TJ, Lennon VA. Pathogenic potential of IgG binding to water channel
extracellular domain in neuromyelitis optica. Neurology. 2007 Dec 11;69(24):2221-31.17. Roemer SF, Parisi JE, Lennon VA, Benarroch EE, Lassmann H, Bruck W, Mandler RN, Weinshenker BG, Pittock SJ, Wingerchuk DM,
Lucchinetti CF. Pattern-specific loss of aquaporin-4 immunoreactivity distinguishes neuromyelitis optica from multiple sclerosis. Brain. 2007 May;130(Pt 5):1194-205.
18. Auer RN, Krcek J, Butt JC. Delayed symptoms and death after minor head trauma with occult vertebral artery injury. J Neurol Neurosurg Psychiatry. 1994 Apr;57(4):500-2.
19. Denton S, Mileusnic D. Delayed sudden death in an infant following an accidental fall: a case report with review of the literature. Am J Forensic Med Pathol. 2003 Dec;24(4):371-6.
20. Jarius S, Paul F, Franciotta D, Aktas O, Hohlfeld R, Zipp F, Vincent A. Revised diagnostic criteria for neuromyelitis optica--incorporation of NMO-IgG status. Nat Clin Pract Neurol. 2007 May;3(5):E1.





























