Embed Size (px)
Citation preview

Communication Sciences and Disorders
Supervisory Manual
Revised 2009

Table of Contents Page I. Purpose of Manual 4 II. T.U. Masters Program: Academic and Clinical Requirements 5 III. Prerequisites to Field Practica 5 IV. Roles of the Supervision Team 5 V. Grading 7 VI. Support for Continuing Education 7 VII. Philosophy of Supervision 8 VIII. Code of Ethics 13 IX. Cultural and Linguistic Diversity 13

Appendices
Student Summary A-1
Contracts A-3
Training Experience Evaluation Form (TEEF) A-6
Grading of Clinical Courses A-17
Record of Daily Hours A-20
Student Evaluation of Clinical Practicum A-21
Field Supervisor's Evaluation of Practicum A-23
TU Supervisor's Evaluation of Practicum A-24
ASHA Technical Report: Clinical Supervision in A-25
Speech-Language Pathology
Code of Ethics of ASHA A-43

I. Purpose of Manual
The purpose of this manual is to provide the field supervisor with information that will facilitate the success of the supervisory process for both supervisees and supervisors. The information presented will: 1. explain the department’s philosophy of supervision, supported by historical and recent research in this area.
2. explain the department’s expectations of the clinical experience. 3. provide specific information regarding the Temple University Masters Degree in Speech-Language-Hearing. 4. identify the personnel with whom the field supervisor must interact.
5. clarify the paperwork which must be completed by the supervisor and student clinician; and 6. briefly describe strategies to assist in clinical supervision.

II. Temple University Masters Degree Program The Masters Degree program at Temple University Department of Communication Sciences and Disorders is a comprehensive educational program designed to educate clinical professionals. Educating future speech-language pathologists requires the blending of a broad range of academic coursework and supervised experiences in clinical settings in which to apply academic training to clinical processes. Academic and clinical education is interwoven inextricably. The objective of clinical education is to prepare the graduate to work competently with a broad spectrum of clinical populations, clients of all ages, from all socioeconomic and cultural backgrounds, with all varieties of speech, language, and hearing disorders and in a variety of settings. During their initial clinical experiences in graduate school, the students usually remain at Temple University Speech-Language-Hearing Center (TUSLHC) for clinical training and are supervised by Temple University faculty. When considered appropriate by the faculty, the students then receive clinical supervision in outside the TUSLHC in sites such as medical settings (acute care and rehabilitation hospitals), schools, clinics, private agencies, and private practices, as well as specialized clinics at Temple University. The M.A. program achieves its breadth through its graduate courses (required and core) and through practica; it achieves its depth through it elective courses and specialized practicum experiences. Clinical education is viewed to be of equal importance as academic coursework and supervision is viewed as “clinical teaching.” It is the unique role of the field supervisor to provide clinical teaching to our students in various settings. The depth of training and strength of our product, the clinicians, is attributed in large part to the experiences and supervision received in “the field.” We gratefully acknowledge the importance of your role and hope that in supervising students you receive back an intellectual and emotional stimulation, and the satisfaction that you are helping to mold the future generation of speech-language pathologists. III. Prerequisites to Field Practica Before a student is assigned a field practicum s/he usually has successfully completed two semesters of clinical training at the TUSLHC and an evaluation has been made by Temple University faculty that the student is competent to begin outside field placements. Academic coursework relevant and necessary to the field experience is determined by the field site in conjunction with the Temple University clinical education coordinator, and a student must have completed these academic and clinical requirements prior to beginning that field practicum. If an exception to this policy needs to be made, it must be done through discussion between the Director of Clinical Education, the Temple University clinical supervisor and the field supervisor. Field supervisors also can have input into student competencies in other ways: by making suggestions regarding the content of academic courses via the Field Supervisors’ Advisory Committee (a committee of clinicians from a variety of field affiliates which meets monthly at Temple University) , through clinical teaching throughout the field experience, e.g. staff in-services, conferences about specific clinical application of theoretical issues, and through completion of the Field Supervisor’s Evaluation of Clinical Practicum. IV. Roles of the Supervision Team FIELD SUPERVISOR: The primary clinical supervisor working directly with the student clinician in the daily tasks of clinical teaching. As outlined in the Temple University practicum contract (p. A-3,4,5), the field supervisor will: 1) participate in formulating the contract; 2) observe the student in

assessment and treatment of clients/patients; 3) review clinical writing; 4) provide verbal and/or written feedback on assessment, treatment, and writing; 5) complete and discuss mid-term and final Training Experience Evaluation Form (TEEF); and 6) submit final TEEF with recommended grade in conjunction with the Temple supervisor to the student’s academic advisor. Along with the experiences of working directly with the clients/patients, the field supervisor will suggest at contract time (and arrange for) experiences which will supplement training in the knowledge of the specific population, such as: observing other speech-language pathologists or audiologists, classroom teachers, physical and occupational therapists, physicians and surgery, participating in team or departmental meetings, attending in-services on related topics, counseling families, and participating in IEP meetings. As noted in the contract addendum, ASHA minimum requirements of direct supervision of direct supervision of the student is 25% of each therapy or diagnostic session. TEMPLE UNIVERSITY SUPERVISOR: The liaison between the affiliate (field) supervisor and Temple University. The Temple University supervisor makes the initial contact with the field supervisory by phone the week prior to the start of the practicum, to confirm the days/times of the practicum schedule. Within the first 3 weeks of the semester, s/he will go to the affiliate site to formulate a contract with the field supervisor and the Temple student. The Temple University supervisor is available to observe the student in direct clinical work at the field site. The Temple University supervisor will give direct feedback to the student and the field supervisor regarding the observation and can assist or make suggestions regarding supervisory goal setting and direction to the student. At all times, the Temple University supervisor's role is to serve as mediator of the student clinician and field supervisor when unresolved problems arise. Unresolved issues should be communicated immediately to the Temple University supervisor, and a (triad) conference set up as a forum for discussion. Assignment of grades is assisted by the Temple University supervisor, and s/he is usually present at the final TEEF.
STUDENT: Will 1) bring forms (see Appendix 1-13) to the field supervisor to organize the paperwork of the practicum experience; 2) participate in the writing of the contract; and 3) become familiar with expected policies and procedures of the affiliate agency (including health regulations) and expectations of performance in the practicum. During the semester, s/he (as outlined in the contract) will 4) complete required direct and indirect patient contact; 5) write required documentation; 6) complete assigned (and other relevant) reading materials; 7) participate in other field instruction experiences relevant to the population; and 8) participate in the midterm and final TEEF. The student should be phased into more and more independent clinical work, with the field supervisor facilitating and giving feedback, but at no time should serve the function of a staff speech-language pathologist. Practica are not equivalent to internships. The student will document clinical hours (which will be verified by the field supervisor). At the completion of the semester, s/he will submit the final TEEF to the Temple University supervisor and complete an evaluation of the field practicum site and supervisor.
DIRECTOR OF CLINICAL EDUCATION AND CLINICAL SERVICES: Arranges and schedules practica with affiliate agencies in the months prior to the beginning of the semester and provides (if necessary) insurance documentation.

V. Grading
Students participating in clinical practicum are enrolled for a specific course, receive academic credits, and are given a grade for their performance in the practicum. The Training Experience Evaluation Form (TEEF) (Appendix-10, 11, 12, 13) is completed by the field supervisor, with feedback prior to completion and/or direct involvement of the Temple University supervisor, and is discussed in person with the student at midterm and again at the end of the clinical experience. The Temple University supervisor is available for consultation for the final TEEF. This evaluation form outlines the student’s strengths and weaknesses and serves as a tool to focus the student on future goals for his/her own clinical growth. The final grade will be determined by the Temple University supervisor based on the recommendation of the Field Supervisor (A through F, including minuses and pluses) at the completion of the practicum. Grades are assigned by a Temple faculty member for legal purposes and to attempt to eliminate any bias that can occur because of the interpersonal nature of this process. Although assigning a grade is, in part, a subjective measure, the TEEF and handout "Grading of Clinical Courses" (Appendix p. 17) detail guidelines to provide consistency in grading clinical performance. Grades should be given with consideration to the student's previous clinical experiences and academic coursework, as well as reflect growth throughout the current semester.
Grading is a difficult, yet important form of feedback and documentation. Because of the interpersonal relationship and bond that often forms in the supervisory dyad, assigning a grade is sometimes a difficult decision. If both parties know in advance what the process entails and what forms are available to support grading decisions, personal bias can be avoided. We encourage supervisors to be honest, yet fair in having grades reflect true performance.
VI. Support for Continuing Education
The Department of Communication Sciences and Disorders provides compensation in the form of support for continuing professional education to those professionals contributing to graduate education by the supervision of our students in the field. This support is in the form of "credits" toward attendance at an annual Communiversity Conference sponsored by the Department of Communication Sciences and Disorders that earn ASHA CEUs. These credits are granted to supervising clinicians for use in the year that the supervision takes place. Professionals participating in continuing education activities must meet all prerequisites for these activities. Credits do not apply toward academic credit at Temple University.
Professionals wishing to participate in continuing education activities by using their accrued credits must submit their voucher received from the Director of Clinical Education when they register for the Annual Communiversity Conference. Participant must be present for the entire activity and complete ASHA forms for CEUs. The Department of Communication Sciences and Disorders will submit all paperwork. The participant is responsible for his/her own participation in the ASHA Registry for Continuing Education.

VII. Philosophy of Supervision
The Bridge Between Academic Instruction and Independent Clinical Function in the Process of Becoming a Clinician
Our philosophy of supervision is drawn from various theories which are presented
briefly in the following section. There are areas in supervision that are neither black nor white but represent a blending of shades and/or roles. It is our responsibility as supervisors to be aware of the need for education and nurturing in “the supervisory process”, a separate phenomenon from the “the clinical process”. A look at definitions of clinical supervision from significant publications in speech-language pathology and audiology over the years sees clinical supervisors as central to the process of becoming a clinician but shows the nature of the process to be evolving.
Villareal (1964): The role of an effective supervisor should transcend the mere monitoring
of the student’s clinical activities. It should include the informal teaching of clinical content, the demonstration of clinical techniques, and the mature counseling of the student in relation to his clinical training.
Van Riper (1965): The process through which students are turned into clinicians. Turton (1973): Supervision can be viewed as a process wherein one person is responsible
for changing the knowledge and skill level of another. Rassi (1978): Its aim is to teach a student in a one-to-one situation how to apply his
academic knowledge in a practical clinical setting. The ultimate goal is to transform a student into an independent clinician.
Anderson (1988): Supervision is a process that consists of a variety of patterns of behavior,
the appropriateness of which depends upon the needs, competencies, expectation, and philosophies of the supervisor and supervisee and the specifics of the situation (task, client, setting, and other variables). The goals of the supervisory process are the professional growth and development of the supervisee and the supervisor, which it is assumed will result ultimately in optimal service to clients.
Farmer and Farmer (1989): A necessary, artistic/scientific and changing process composed
of three components (constituents, concepts, and contexts) that interact within the professional, research, educational, administrative, and clinical domains of speech-language pathology and audiology to assure initial and continuing training of competent professionals who can provide quality services for education or health care consumers. Supervisors, who are specialists in the communication disorders profession, require training to meet the standards of quality set by the ASHA Committee of Supervision.
Casey, Smith, and Ulrich (1988): The concept of clinical supervision embodies the notion of
shared responsibility for development of clinical skills and professional self-growth through close observation and rigorous analysis. It is operationalized as a continuum of purpose and roles with three stages and an ongoing shift in the relative dominance of supervisor and supervisee. Movement along the continuum is achieved through the application of specific, overlapping components in the supervisory process. Self-supervision is defined as both an end-product of clinical supervision and a process for the role of a supervisee at any stage.

All of these definitions agree that clinical supervision involves a supervisor (identified below
as the “S'or”) and a supervisee (”the S'ee”). The instructional relationship between the S'or and the S'ee is most typically dyadic (i.e., the delicate dyad) (Figure 1). The dyadic relationship, at its best, involves what has been called an I-Thou, rather than an I-It, relationship. The hallmarks of an I-Thou relationship are two people of equal status engaged in a common task. The relationship has as its foundation, free flowing communication which is open and honest.
FIGURE 1. THE DELICATE DYAD
S’OR S’EE
An I-Thou relationship is difficult to achieve when at the very onset the S'ee is often not the equal of the S'or in experience, expertise, or power. The relationship is further complicated because there is always a client involved; a client for whom the S'ee must provide clinical services in another I-Thou dyadic relationship, but for whom the S'or has clinical, ethical, and legal responsibility. The delicate dyad has now become the even more delicate triad (Figure 2).
FIGURE 2 – THE MORE DELICATE TRIAD
S’OR
CLIENT S’EE
Add to the picture, at field sites, the presence of a university supervisor, and it is no
wonder the relationships are viewed as complex and in need of nurture. The delicate triad has become a most delicate quatrad (Figure 3). In fact, this figure is often further elaborated by the addition of the client's family and other professionals.
FIGURE 3 – THE MOST DELICATE QUATRAD
S’OR CLIENT S’OR UNIV S’EE
Thus, clinical supervision must devote time not only to the clinical process, the art and science
of effectively providing speech, language, and audiology services to the client, but also to the supervisory process, the art and science of effectively sharing in a dyadic relationship between S'or and S'ee so that the S'ee becomes independent of the S'or and self-supervisory. Indeed the thirteen tasks

of supervision, as described by the Committee on Supervision of ASHA in 1985 (Table 1), are equally divided between services to the clinical and the supervisory process. Yet, research and our own experience tell us that in the supervision of students, in clinical practicum, we devote much more time to the clinical process.
TABLE 1. THE TASKS OF SUPERVISION (ASHA, 1985) Position Statement: Clinical Supervision in Speech-Language Pathology and Audiology
CLINICAL SUPERVISORY
TASK PROCESS PROCESS 1.0 Effective Working Relationship X
with Supervisee 2.0 Clinical Goals & Objectives X 3.0 Assessment Skills X 4.0 Management Skills X 5.0 Demonstrating & Participating X X 6.0 Observing & Analyzing X X 7.0 Clinical & Supervisory Records X X 8.0 Supervisory Conferences X 9.0 Evaluation of Clinical Performance X 10.0 Reporting, Writing, & Editing X 11.0 Ethical, Legal, Reimbursement X 12.0 Professional Conduct X 13.0 Research Skills X X The exact nature of the process known as clinical supervision varies with each S'or-S'ee dyad,
depending on a myriad of variables. For example, with different clinical settings (hospital-based, school-based, clinical-based, home-based), with different client types (varying with different communication disorders, across the life span of different clients from the neonate to the geriatric patient, with different client personality types), with differing levels of experience for both the S'or and the S'ee and with differing reasons for the supervision (student education, CFY supervision, on-the-job performance evaluations).
Jean Anderson has attempted to develop a model of supervision which will account for
these variables. Her model is based on current state of the art clinical practice and on existing research concerning the supervisory process. It offers a visual model on which to locate each specific S'or-S'ee dyad at varying points in time, which in turn dictates the nature of the supervisory interaction and process.

FIGURE 4. COMPOSITE STAGES OF SUPERVISIONS AND APPROPRIATE STYLES FOR EACH STAGE
(Taken from McCrea, E., and Brasseur, J. (2003) The Supervisory Process in Speech-Language Pathology and Audiology. Boston, MA: Pearson Education, Inc, p.27.) Stages Evaluation Transitional Self- Feedback Supervision Styles Direct/Active Collaborative Consultative Supervisor Supervisee Peer
As a S'ee moves from the Evaluation-Feedback Stages through the Transitional Stages and
into the Self-Supervision Stage, the nature of the supervisory process changes. Anderson describes the Evaluation-Feedback Stage as one in which the S'or uses a direct-active style which the S'ee uses a passive-listening style (1988, p. 53). In other words, it is the S'or who provides the direction, feedback, and evaluation for both the clinical process and the supervisory process. While beginning students need this authoritarian approach, Anderson sees the aim of the S'or and the S'ee to leave this stage as quickly as possible (1988, p. 52). In the Transitional Stages, the responsibility for both the clinical process and the supervisory process is shared; it is a democratic process with roles arrived by consensus. The S'ee and the S'or collaborate and exchange leader and follower roles depending on tasks and interactions. Students in certain educational sites and with certain types of clients may remain in a Transitional Stage even at the completion of a practicum for all or certain of the tasks of the clinical and supervisory processes; in fact, professionals also remain in this stage for certain clients, communication disorder types, tasks, and/or interventions. In the Self-Supervision Stage, the S'ee assumes the dominant role and functions independently in both clinical and supervisory tasks using a S'ee (who may be a peer or colleague) as a consultant by request. Casey, Smith, and Ulrich point out that it is not for self-analysis and knows how to ask for help and evaluate the appropriateness of the response from the S'or (1988, p.10). Stages of the continuum are not time bound (Anderson, 1988, p.62). Typically, we move through these stages in sequence, but easily shift back into earlier stages in different settings, with

different client types, with changing interactions, and with different tasks (Russell & Engle, 1977). Certainly students return to an Evaluation-Feedback Stage at the onset of each new clinical placement, but typically shift into Transitional Stages more quickly in direct relationship to the amount of previous practicum experience they have had. The Supervisory Process Because we understand the clinical process (that which goes on between client and clinician), we also know much about the supervisory process (that which goes on between the S'or and S'ee). Both processes involve the same components: understanding, planning, observing, analyzing, and integrating (Anderson, 1988, p.63-66). Specifically, they apply to the supervisory process as follows. It is necessary for the S'or and S'ee to have ongoing discussions of the nature of the supervisory process, to consider where they fall on the supervisory continuum, to share their expectations, to define roles, to verbalize their anxieties and concerns, and to be as open and honest as possible in their communication. This is understanding the supervisory process. We learn about the supervisory process and grow in our skills as both S'or and S'ee when we plan for the supervisory process as well as the clinical process. When will supervision take place? How will data be collected? Who will collect the data? How will it be analyzed? Data are collected through observation, which is not synonymous with evaluation. Both the S'or and S'ee should be involved in the process of observing; both the clinical and supervisory session should be observed. Checklists, written notes, audio and video tapes are but some of the possible procedures. Our literature contains many tools to assist in observation and to minimize bias. A plan should be agreed upon for how the data are to be analyzed. With the S'ee begin the process, or will the S'or provide the initial feedback? Will the feedback be verbal or written? Will the focus be on the positive or negative? Will peers be involved in a group's procedure? How will the S'ee become independent in this process, or self-supervisory? What hypotheses can be drawn? Finally, we come full circle and are back at the start. What does this mean and where do we go from here? In the process of integration, we plan for supervision all over again. The more explicit we can make the supervisory process and interaction between S'ee and S'or, the better the chance of growth for both S'ee and S'or. There are many ways to obtain continuing education in the area of supervision. Informally, Temple University's faculty stands ready to problem solve supervisory issues and serves as a resource of further information. The Department also provides formal education in the area of supervision. Half-day in-services for field supervisors will be provided at Temple at its Communiversity conference and is recommended for each field supervisor to attend at least once before supervising students. In addition, there will be an open meeting for all supervisors, periodically, for communication of specific information and also to in-service supervisors in the topic of clinical supervision. Temple University faculty also welcomes, and encourages collaboration in research in this very important topic area.

A field supervisors' advisory committee (Supervisor Advisory Committee) has been established as a forum to communicate questions and concerns to the Department of Communication Sciences and Disorders and as a vehicle to obtain feedback regarding content of academic courses. Membership in special interest groups in clinical supervision through ASHA and Pennsylvania Speech-Language-Hearing Association (PSHA) is also recommended. VIII. Code of Ethics The ASHA Code of Ethics provides a moral framework for Speech-Language Pathologists and Audiologists to function. The purpose is to ensure that quality professional care is provided uniformly across the profession. It is to be taken seriously and recognized as an important teaching tool for student clinicians. Exposure to the ethical standards during the initial clinical experience develops a professional moral foundation which the student can build upon in later practica. It is through observing the supervisor's response to ethical situations that the supervisee will learn to incorporate a strong moral character into interactions with clients. The most recent ASHA Code of Ethics is included in the appendix of this manual. IX. Cultural and Linguistic Diversity As we move into an age of increasing cultural and linguistic diversity, it becomes important for us as clinical supervisors to understand and promote the acceptance of other cultures and languages as represented by the clients we serve and the student clinicians we supervise. Cultural characteristics must be recognized as having equal value to those of other cultures. In situations where cultural and linguistic knowledge is limited, supervisors and supervisees are encouraged to expand their understanding of these differences, especially in the area of communication (pragmatics, narrative style, etc.) and cultural values (attitudes toward disabled children, role of family in treatment, etc.). It is important for supervisors and supervisees to respect the values of every individual's cultural origin or preference and language. We further encourage the acceptance of individuals regardless of gender, socioeconomic status, race, age, or sexual orientation. Our goal in supervision is to develop competent clinicians, sensitive to the communication needs of a growing, diverse society.

TEMPLE UNIVERSITY
DEPARTMENT OF COMMUNICATION SCIENCES
STUDENT SUMMARY NAME: _____________________ DATE: ____________________ UNDERGRADUATE DEGREE
DEGREE: ______________________ YEAR: _______________ SCHOOL:____________________________________________ MAJOR: _____________________________________________
I. Speech and hearing coursework to date: (include relevant undergraduate and graduate
courses by course title) II. Clinical Education Experiences to date: (include all settings and brief description of
clinical activities)

III. Employment History: IV. Current Schedule: (list academic courses and times, other practicum assignments and schedules, and work commitments)

TEMPLE UNIVERSITY DEPARTMENT OF SPEECH-LANGUAGE-HEARING
CONTRACT FOR SPEECH & LANGUAGE PRACTICUM
STUDENT Name Semester_________________ Year____________ Phone ( ) _____________ Email address: _________________________________ Assignment I will keep the following schedule during this practicum assignment: Number of weeks Dates Time *Dates absent from practicum From M Clinician Supervisor T To W R F My special areas of interest are: I have met the academic and clinical training requirements for this assignment:________(see Student
Summary) I agree to follow schedules and procedures of the affiliated agency. I will complete the Record of Daily Clinical Hours according to department procedures and submit this
with the completed TEEF to the T.U. Supervisor. _________ I will submit the TEEF for completion by appropriate parties prior to the end of the semester. I will complete and review with my field supervisor the field evaluation report. A copy of this evaluation
shall be submitted to the T.U. Field Supervisor in order for my final grade to be posted. ______ FIELD SUPERVISOR Name (as listed with ASHA) ___ _______ ASHA Account Number CCC-SLP CCC-A State: _______ Phone ( ) EXT. Email address: _______________________ Training will include: Child emphasis Adult emphasis Mixed Type of cases will include:
Diagnostics Aural Rehabilitation Articulation Family Education/Counseling Language Dysphagia Fluency Cognitive Deficits Voice _______Staffings _______________________________ Other
*Standard excused absences include: comprehensive exams, mini-seminars, spring break, and holidays.

FIELD SUPERVISOR ( continued) Other Aspects of Training (If checked, please describe.)
Related professional experience Administrative experiences Observation Therapy Planning Report Writing Other ___________________________________________________________________
My supervision, instruction, and evaluation methods will include:
Observation (See addendum for ASHA requirements) Being available for questions & discussion Individual Conference __________________________ Mid-term TEEF ______________________________ Demonstration _______________________________ Assigned Readings ____________________________ _____Other ______________________________________
TEEF will be completed by the Field Supervisor or Jointly prior to the termination of the semester. I agree to release the student from practicum to complete academic coursework, attend mini-seminars, and/or partake in comprehensive exams at Temple University. TEMPLE UNIVERSITY SUPERVISOR Name (as listed with ASHA) ASHA Account Number ___________ CCC-SLP________CCC-SLP_________ State: ________ Phone ( ) Email address: __________________________ I will be responsible for: (If checked, please describe.)
Discussion and agreement of terms of contract Making field visits for observation & discussion with student Arranging independent conferences at TU with student Acting as "liaison" between student and affiliation personnel Participating in evaluation of student in training Discussing the completed TEEF with student and recommending a grade to student's faculty advisor Submission of contract and field evaluation report to Coordinator of Clinical Education Other
CEU credits earned by Field Affiliate can be used for tuition remission at the Annual Communiversity Conference offered by the Department of Communication Sciences and Disorders at Temple University (0.6 CEUs). Student _________________________________ Field Supervisor _____________________________ TU Supervisor _____________________________________ Today’s Date_______________
1/09

TEMPLE UNIVERSITY DEPARTMENT OF COMMUNICATION SCIENCES AND DISORDERS
Addendum to Audiology & Speech Language Pathology Contracts.
In order to maintain our accreditation by the Council of Academic Accreditation (CAA) of ASHA, Temple University’s training program in Speech Language Pathology and Audiology is required to satisfy the following minimal requirements regarding supervision of clinical practicum at field sites. IV-C The applicant for certification in speech-language pathology must complete a minimum for
400 clock hours of supervised clinical experience in the practice of speech-language pathology. Twenty-five hours must be spent in clinical observation, and 375 hours must be spent in direct client/patient contact.
• Only direct contact with the client or the client's family in assessment, management, and/or
counseling can be counted toward practicum.
IV-E Supervision must be provided by individuals who hold the Certificate of Clinical
Competence in the appropriate area of practice. The amount of supervision must be appropriate to the student's level of knowledge, experience, and competence. Supervision must be sufficient to ensure the welfare of the client/patient.
• Direct supervision must be in real time (on-site or on closed circuit TV monitoring of the
student clinician).
• At least 25% of the total contact with each client/patient by a student clinician must be directly supervised and must take place periodically throughout the practicum. These minimum requirements should be adjusted upward if the student's level of knowledge, experience, and competence warrants.
• A supervisor must be available to consult as appropriate for the client's/patient's disorder with a student providing clinical services as part of the student's clinical education. Supervision of clinical practicum must include direct observation, guidance, and feedback to permit the student to monitor, evaluate, and improve performance and to develop clinical competence.
• All clinical practicum hours must be supervised by individuals who hold a current CCC in the professional area in which the practicum hours are being obtained. Only the supervisor who actually observes the student in a clinical session is permitted to verify the credit given to the student for the clinical practicum hours.

Temple University Speech-Language-Hearing Center (TUSLHC) Training Experience Evaluation Form (TEEF)
(Revised 7/05) I. Student . Semester/Year . Academic Advisor . Training/Practicum Course Number . Semester/Year Registered . Other TEEFs for this course number? Yes ___No___
II. Practicum Assignment Name of Practicum Site .
Field Clinical Supervisor . ASHA# . State License# . T.U. Clinical Supervisor . ASHA# . State License# .
III. Training/Practicum Hours Training Hours Practicum Hours
Hours of Dx Hours or Tx Area Evaluation Screening Individual Group Total Practicum Hours1. Language
Adult
Child 2. Articulation Adult
Child 3. Voice Adult
Child 4. Fluency Adult
Child 5. Dysphagia Adult
Child 6. Hearing Adult
Child 7. Staffing* Adult
Child
Observation • Dx ______ • Tx ______
Conference • Supervisory ______ • Other ______
Planning/Prep ______
Reports ______
Administration (specify activity/hours) • ____________________ ____________________ • ____________________ ____________________ • ____________________ ____________________
Other (specify activity/hours) • ____________________ ____________________ • ____________________ ____________________ • ____________________ ____________________
Total Training Hours ______
Totals
* A staffing is a discussion and formulation of evaluation and treatment plans and/or recommendations with or without the client present. Hours accrued in patient or family counseling go under the disorder area and are not recorded as staffing.
IV. Description of Practicum and Training Experience (e.g., types of cases, duties and responsibilities, and ancillary experiences). [Note: You may want to refer to your contract.]
V. Evaluation Summary Specific Strengths:
Needs Additional Experience In:
Recommended Letter Grade: ________ (Refer to Guidelines on page 2.) Student . Field Supervisor: . T.U. Supervisor .

Temple University Speech-Language-Hearing Center (TUSLHC) Training Experience Evaluation Form (TEEF)
(Revised 7/05)
Description and Directions • This TEEF, adapted from the ASHA Clinical Fellowship Skills Inventory (CFSI), is designed to evaluate the skills of the graduate level student clinician
(SC). [Note: The ASHA CFSI is used to evaluate clinical fellows during their year of supervised work experience.]
• The purpose of the TEEF is to assist the clinical supervisor in assessing the SC’s performance and to guide the SC to improve and strengthen his/her clinical skills throughout the training experience.
• As does the CSFI, this TEEF covers four areas: (a) evaluation, (b) treatment, (c) management, and (d) interaction.
• For each skill area there is a 5-point rating scale. Please note the following. - The SC’s performance should be evaluated according to the descriptors provided. - Not all skill areas will be covered by every practicum experience. (If a skill area is not covered, check “NA”.) - The SC may not receive ratings of 4 or 5 and still receive a satisfactory recommended grade. (Performance evaluation and grading are not
equivalent. For grading of the course, see guidelines below.)
• The clinical supervisor is required to complete the TEEF twice during the practicum (i.e., at both a midterm evaluation [ME] and a final evaluation [FE]).
• At the end of the semester, the clinical supervisor recommends a letter grade for the SC’s practicum experience in consultation with the TU supervisor using the following grading guidelines. (These guidelines for grading also appear in the “Grading of Clinical Courses” section of the Temple University MA Manual for Communication Sciences which can be accessed on-line at <http://www.temple.edu/commsci/mamanual>.)
Grading Guidelines for Clinical Courses • A and A minus indicate work of superior quality.
A: exceeds all mandated requirements; majority of clinical competencies exceed the quality and expectations for students at this level of training; shows minimal need for direct or prescriptive instructions; shows excellent ability applying previous or ongoing coursework and experiences, and/or is able to hypothesize and appropriately apply conceptual and/or theoretical constructs to treatment, even when specific content has not been taught; shows the ability to recognize, analyze, and revise relevant aspects of treatment; shows insightful observational and interpretive skills; shows excellent awareness of client’s perspective and needs.
A-: exceeds most and satisfies all mandated requirements; majority of clinical competencies surpass the quality and expectations for students at this level of training; requires occasional direct or perspective instruction but generally extrapolates and applies generatively very quickly; shows ability to create own procedures; shows very good ability to recognize, analyze, and revise relevant aspects of treatment given occasional feedback; shows good observational and interpretive skills; shows good awareness of client’s perspective and needs.
• B+, B and B minus indicate work of satisfactory quality. B+: exceeds some and satisfies all mandated requirements; clinical competencies show steady growth; shows ability to abstract and generatively
apply outlined principles of treatment given examples; integrates and utilizes the information provided; learns quickly from past mistakes in attempting to explain behavior conceptually/theoretically; showing steady growth in observational and interpretive skills; is developing good ability to recognize and revise relevant aspects of treatment given feedback.
B: has satisfied all mandated requirements; shows steady growth in a specified set of clinical competencies; requires frequent direct or prescriptive information, but can integrate and utilize information provided given intermittent review; understands and attempts to apply information given regarding: conceptual, theoretical constructs; is beginning to show growth in observational and interpretive skills; now recognizes some aspects of treatment which need revision given feedback; shows emerging awareness of client’s perspective and needs.
B-: has satisfied most, but not all, mandated requirements; is beginning to show growth in a specified set of clinical competencies; requires direct or prescriptive information; requires assistance integrating and utilizing the information provided; requires direct assistance applying information conceptually/theoretically; requires assistance in observational and interpretive skills, and in assessing client’s perspective and needs; incorporates suggested revisions; continues to need help recognizing the necessity and rationale for revisions.
• C+, C and C minus indicate work of marginal quality. (Clinical practicum hours are not accrued for any experience given these grades.) C+: has satisfied only a few of the mandated requirements; is showing minimum growth only in very few clinical competencies; requires a great deal of
direct and prescriptive information; needs much assistance integrating and utilizing the information provided; requires much time and attention in applying information conceptually/theoretically; requires a great deal of assistance in observational and interpretive skills in assessing client’s perspective and needs; appears to benefit only from such assistance; in the main, does not appropriately incorporate suggested revisions; interprets suggestions with only a minimal understanding of why revisions are necessary relative to this client; shows only occasional instances of ability to independently recognize need or rationale for revisions.
C: has inadequately attempted to meet most mandated requirements; is not yet showing growth in a specified set of clinical competencies; requires repeated direct or prescriptive information; needs repeated assistance integrating and utilizing information provided; shows little evidence of abstracting underlying principles of treatment; requires repeated direct assistance applying information conceptually/theoretically; requires repeated assistance in observational and interpretive skills, and in assessing client’s perspective and needs; does not appear to benefit from such assistance.
C-: has not met most mandated requirements; shows little growth in any area of case management; despite repeated prescriptive information, shows complete dependence on supervisor to determine goals, rationales, procedures and techniques appropriate for this client’s treatment; relies totally on supervisor to collect and analyze data; shows no independent ability to recognize or understand need or rationale for revisions.
Page 2 of 11
TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
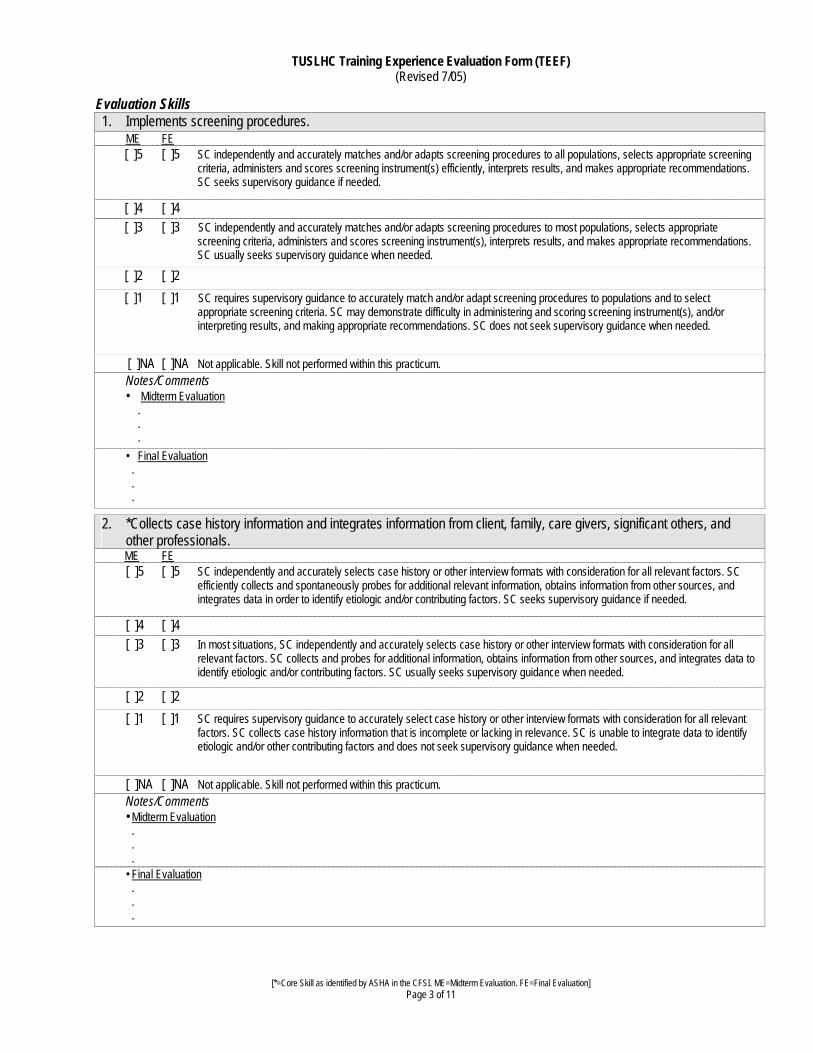
Evaluation Skills 1. Implements screening procedures.
ME FE [ ]5 [ ]5 SC independently and accurately matches and/or adapts screening procedures to all populations, selects appropriate screening criteria, administers and scores screening instrument(s) efficiently, interprets results, and makes appropriate recommendations. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 SC independently and accurately matches and/or adapts screening procedures to most populations, selects appropriate screening criteria, administers and scores screening instrument(s), interprets results, and makes appropriate recommendations. SC usually seeks supervisory guidance when needed. [ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to accurately match and/or adapt screening procedures to populations and to select appropriate screening criteria. SC may demonstrate difficulty in administering and scoring screening instrument(s), and/or interpreting results, and making appropriate recommendations. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
2. *Collects case history information and integrates information from client, family, care givers, significant others, and other professionals.
ME FE [ ]5 [ ]5 SC independently and accurately selects case history or other interview formats with consideration for all relevant factors. SC efficiently collects and spontaneously probes for additional relevant information, obtains information from other sources, and integrates data in order to identify etiologic and/or contributing factors. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently and accurately selects case history or other interview formats with consideration for all relevant factors. SC collects and probes for additional information, obtains information from other sources, and integrates data to identify etiologic and/or contributing factors. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to accurately select case history or other interview formats with consideration for all relevant
factors. SC collects case history information that is incomplete or lacking in relevance. SC is unable to integrate data to identify etiologic and/or other contributing factors and does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation] Page 3 of 11

TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
3. *Selects and implements evaluation procedures (nonstandardized tests, behavioral observations, and standardized
tests).
ME FE [ ]5 [ ]5 SC independently selects a comprehensive assessment battery with consideration for all relevant factors. SC efficiently and
accurately administers the battery and consistently scores tests accurately. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently selects an adequate assessment battery (i.e., basic procedures needed to define problem adequately) with consideration for all relevant factors. SC administers the battery, scores tests accurately, and usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to select evaluation procedures that are appropriate and complete. SC may administer and/or
score tests inaccurately and does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
4. *Adapts interviewing and testing procedures to meet individual client needs.
ME FE [ ]5 [ ]5 SC independently and accurately recognizes when testing procedures need to be adapted to accommodate needs unique to
specific clients. Effectively implements appropriate adaptations, and makes maximum use of all available resources to provide for unusual situations. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently and accurately recognizes when testing procedures need to be adapted to accommodate needs unique to specific clients and implements appropriate modifications. May need assistance in accessing available resources. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to recognize the need for and/or to adapt procedures to accommodate individual needs. SC
does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation] Page 4 of 11
TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
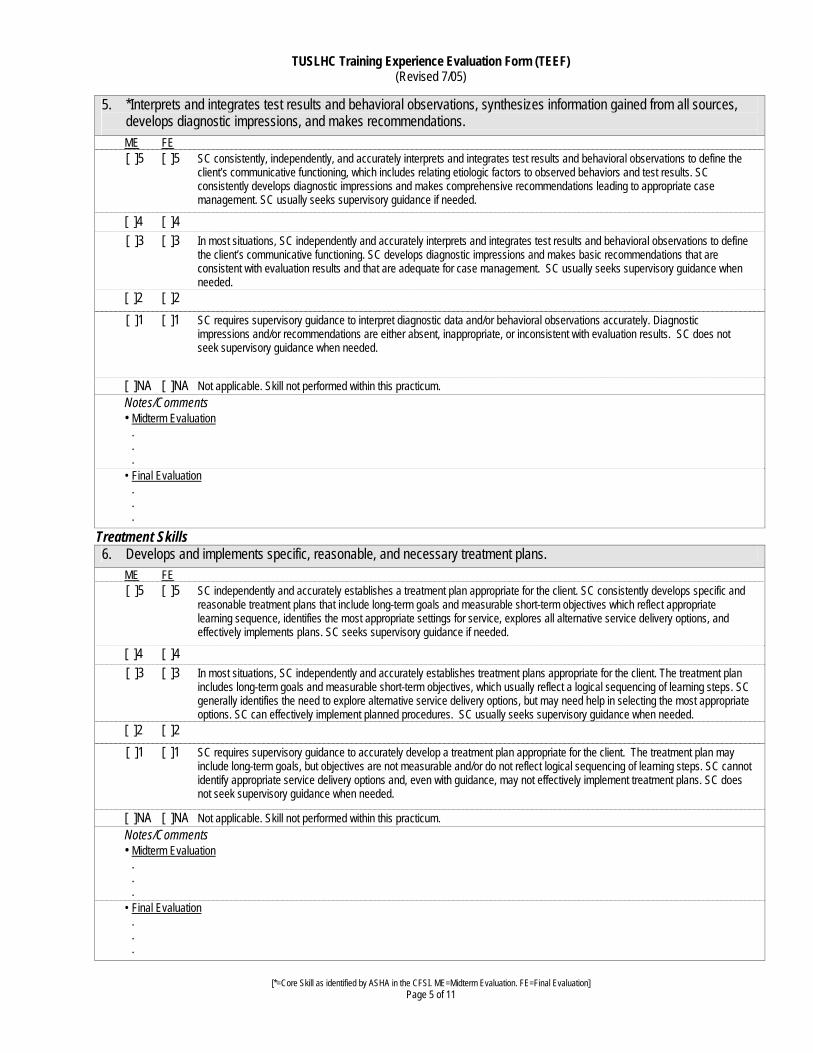
5. *Interprets and integrates test results and behavioral observations, synthesizes information gained from all sources, develops diagnostic impressions, and makes recommendations.
ME FE [ ]5 [ ]5 SC consistently, independently, and accurately interprets and integrates test results and behavioral observations to define the client’s communicative functioning, which includes relating etiologic factors to observed behaviors and test results. SC consistently develops diagnostic impressions and makes comprehensive recommendations leading to appropriate case management. SC usually seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently and accurately interprets and integrates test results and behavioral observations to define the client’s communicative functioning. SC develops diagnostic impressions and makes basic recommendations that are consistent with evaluation results and that are adequate for case management. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to interpret diagnostic data and/or behavioral observations accurately. Diagnostic
impressions and/or recommendations are either absent, inappropriate, or inconsistent with evaluation results. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
Treatment Skills
6. Develops and implements specific, reasonable, and necessary treatment plans.
ME FE [ ]5 [ ]5 SC independently and accurately establishes a treatment plan appropriate for the client. SC consistently develops specific and reasonable treatment plans that include long-term goals and measurable short-term objectives which reflect appropriate learning sequence, identifies the most appropriate settings for service, explores all alternative service delivery options, and effectively implements plans. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently and accurately establishes treatment plans appropriate for the client. The treatment plan includes long-term goals and measurable short-term objectives, which usually reflect a logical sequencing of learning steps. SC generally identifies the need to explore alternative service delivery options, but may need help in selecting the most appropriate options. SC can effectively implement planned procedures. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to accurately develop a treatment plan appropriate for the client. The treatment plan may
include long-term goals, but objectives are not measurable and/or do not reflect logical sequencing of learning steps. SC cannot identify appropriate service delivery options and, even with guidance, may not effectively implement treatment plans. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation]
Page 5 of 11

TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
7. Selects/develops and implements intervention strategies for treatment of communication and related disorders.
ME FE [ ]5 [ ]5 SC independently selects/develops and implements comprehensive intervention strategies that take into consideration all
unique characteristics and communication needs of the client. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently selects/develops and implements intervention strategies relevant to the communication disorder and the unique characteristics of the client. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to select/develop and/or implement intervention strategies relevant to the needs of the client.
SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
8. *Selects/develops and uses intervention materials and instrumentation for treatment of communication and related disorders.
ME FE [ ]5 [ ]5 SC independently and consistently selects/develops materials and instrumentation for which there is a clear rationale and uses these materials and instrumentation creatively and effectively to enhance the treatment process. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently selects/develops materials and instrumentation that are relevant to the communication disorder and uses materials and/or instrumentation effectively. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to select materials and/or instrumentation that are appropriate to the treatment objectives,
client, and/or the activity. Once selected, SC may not use materials and/or instrumentation effectively. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation] Page 6 of 11

TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
9. *Plans and implements a program of periodic monitoring of the client’s communicative functioning through the use of appropriate data collections systems. Interprets and uses data to modify treatment plans, strategies, materials, and/or instrumentation to meet the needs of the client.
ME FE [ ]5 [ ]5 SC independently develops and implements a comprehensive program of periodic monitoring of the client’s communicative
functioning and collects and interprets data accurately. Uses this information to effectively modify treatment plans, strategies, materials, and/or instrumentation to meet the needs of the client. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently develops and implements a program of periodic monitoring of the client’s communicative functioning. Collects and interprets data accurately and uses this information to modify treatment plans, strategies, materials, and/or instrumentation to meet the needs of the client. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to plan and implement a program of periodic monitoring of the client’s communicative
functioning. SC does not collect useful and/or accurate data in order to modify treatment plans, strategies, materials, and/or instrumentation to meet the needs of the client. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
10. *Adapts intervention procedures, strategies, materials, and instrumentation to meet individual client needs.
ME FE [ ]5 [ ]5 SC independently and consistently adapts intervention procedures, strategies, materials, and instrumentation to accommodate
needs unique to specific clients. Makes maximum use of all available resources to provide for unusual situations. SC effectively implements appropriate adaptations and seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 SC recognizes when intervention procedures, strategies, materials, and/or instrumentation need to be adapted to accommodate needs unique to specific clients. May need assistance in making appropriate adaptations. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to recognize the need for adaptation of intervention procedures, strategies, materials, and/or
instrumentation to accommodate needs unique to specific clients. SC may have difficulty implementing identified adaptations and does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation] Page 7 of 11

TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
Management Skills 11. *Schedules and prioritizes direct and indirect service activities, maintains client records, and documents professional contacts and clinical reports in a timely manner.
ME FE [ ]5 [ ]5 SC independently and consistently prioritizes activities, schedules client contacts and meetings, maintains client records
accurately, and makes and documents professional contacts in a timely manner. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 SC independently prioritizes most activities, consistently schedules client contacts and meetings, maintains client records accurately, and usually makes and documents professional contacts in a timely manner. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to prioritize activities, schedule client contacts and meetings, maintain client records, and
make professional contacts in a timely manner. SC does not seek supervisory guidance when needed. [ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
12. Complies with program administrative and other regulatory policies such as required due process documentation, reports, service statistics, and budget requests.
ME FE [ ]5 [ ]5 SC independently and consistently complies with administrative and regulatory policy requirements and does so in a timely and
accurate manner. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently complies with administrative and other regulatory policy requirements, although SC may need help with complex reports. Most information requested is provided in an accurate and timely manner. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to comply with administrative and other regulatory policy requirements. Information
requested may be inaccurate and/or does not meet established time lines. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation]
Page 8 of 11

TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
13. Uses local, state, national, and funding agency regulations to make decisions regarding service eligibility and, if applicable, third-party reimbursement.
ME FE [ ]5 [ ]5 SC independently and accurately makes service eligibility decisions that are based on appropriate regulations and follows
applicable mandates. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC independently and accurately makes service eligibility decisions that are based on appropriate regulations and follows applicable mandates. SC usually seeks supervisory guidance when needed. [ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to make service eligibility decisions that are based on appropriate regulations. May not be able
to follow applicable mandates even with direction. SC does not seek supervisory guidance when needed. [ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
Interaction Skills 14. *Demonstrates communication skills (including listening, speaking, nonverbal communication, and writing) that take into consideration the communication needs as well as the cultural values of the client, the family, care givers, significant others, and other professionals.
ME FE [ ]5 [ ]5 SC independently presents information accurately, clearly, logically, and concisely. Oral communications, written reports, and letters are always appropriate for the needs of the audience. SC uses terminology and phrasing consistent with the semantic competency of the audience and includes accurate and complete information, listens carefully to clients and others, takes initiative in providing appropriate clarifications when needed, and demonstrates appropriate nonverbal communication style. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 SC usually presents information clearly, logically, and concisely. Oral communications, written reports, and letters are appropriate in most situations in that terminology and phrasing are consistent with the semantic competency of the audience.
SC includes information that is accurate and/or complete. Listens to clients and others but may have difficulty providing appropriate clarification when needed. SC acknowledges the impact of own nonverbal communication style but may have difficulty demonstrating this consistently. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC does not present information clearly, logically, and concisely. Oral communication, written reports, and letters are inappropriate for the needs of the audience. SC uses terminology and phrasing inconsistent with the semantic competency of
the audience and includes information that is inaccurate and/or incomplete. Does not listen carefully to clients and others and fails to provide appropriate clarification when needed. SC demonstrates inappropriate nonverbal communication style. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation] Page 9 of 11

TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
15. *Identifies and refers clients for related services including audiological, educational, medical, psychological, social, and vocational, as appropriate.
ME FE [ ]5 [ ]5 SC consistently identifies the need for and makes appropriate client referrals. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC identifies the need for client referrals but may need some assistance in locating specific referral sources. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to identify the need for client referrals and/or to make appropriate referrals. SC does not seek
supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
16. *Collaborates with other professionals in matters relevant to case management.
ME FE [ ]5 [ ]5 SC consistently listens to input from others, makes appropriate decisions based on shared information, and initiates activities
and contributes information that promote mutual problem-solving. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC listens carefully to input from others, makes appropriate decisions based on shared information, usually participates in activities and contributes information that promote mutual problem-solving. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC requires supervisory guidance to effectively identify the need to consult or collaborate with other professionals in case
management activities. Does not make decisions based on shared information and/or focus on mutual problem-solving activities. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation] Page 10 of 11

TUSLHC Training Experience Evaluation Form (TEEF) (Revised 7/05)
17. *Provides counseling and supportive guidance regarding the client’s communication disorder to client, family, care givers, and significant others.
ME FE [ ]5 [ ]5 SC listens, reflects, and explains information using terminology appropriate to the audience. SC monitors understanding by
asking questions and encouraging interaction among all participants. Engages client/family in problem-solving activities. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 SC listens but may show some difficulty reflecting and/or explaining information using terminology appropriate to the audience. SC monitors understanding by asking questions but may have some difficulty encouraging interaction among all participants. SC attempts to engage client/family in problem-solving activities. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC does not listen, reflect, and/or explain information appropriately and does not use terminology appropriate to the audience.
SC does not monitor understanding by asking questions and/or encouraging interaction among all participants. Does not engage client/family in problem-solving activities. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
18. Plans and implements educational programs for other professionals and the general public to facilitate acceptance and treatment of disabilities associated with communication disorders.
ME FE [ ]5 [ ]5 With consideration of the needs of the audience, SC independently and consistently provides clear and meaningful educational
information to facilitate the acceptance and treatment of disabilities associated with communication disorders. SC seeks supervisory guidance if needed.
[ ]4 [ ]4
[ ]3 [ ]3 In most situations, SC considers the needs of the audience and independently provides clear and meaningful educational information to facilitate the acceptance and treatment of disabilities associates with communication disorders. SC usually seeks supervisory guidance when needed.
[ ]2 [ ]2 [ ]1 [ ]1 SC does not consider the needs of the audience and requires supervisory guidance to provide educational information that
facilitates the acceptance and treatment of disabilities associated with communication disorders. SC does not seek supervisory guidance when needed.
[ ]NA [ ]NA Not applicable. Skill not performed within this practicum. Notes/Comments • Midterm Evaluation . . . • Final Evaluation . . .
[*=Core Skill as identified by ASHA in the CFSI. ME=Midterm Evaluation. FE=Final Evaluation]
Page 11 of 11

TEMPLE UNIVERSITY Department of Communication Sciences and Disorders
GRADING OF CLINICAL COURSES The guidelines below are meant to provide consistency in grading clinical performance. In deciding which descriptors are most appropriate, careful consideration should be given to the student's academic coursework, clinical training, and prior experience with the population at hand. A particular grade is earned when the performance descriptors in a grade category apply.
A AND A MINUS INDICATE WORK OF SUPERIOR QUALITY
A: o Exceeds all mandated requirements; o Majority of clinical competencies exceed the quality and expectations for students at this
level of training; o Shows minimal need for direct or prescriptive instruction; o Shows excellent ability applying previous or ongoing coursework and experiences,
and/or is able to hypothesize and appropriately apply conceptual and/or theoretical constructs to treatment, even when specific content has not been taught;
o Shows the ability to recognize, analyze, and revise relevant aspects of treatment; shows insightful observational and interpretive skills;
o Shows excellent awareness of client's perspective and needs. A Minus :
o Exceeds most and satisfies all mandated requirements; o Majority of clinical competencies surpass the quality and expectations for students at this
level of training; o Requires occasional direct or perspective instruction but generally extrapolates and
applies generatively very quickly; o Shows ability to create own procedures; o Shows very good ability applying previous or ongoing coursework and experiences,
conceptual or theoretical constructs to treatment given general, non-prescriptive information;
o Shows good ability to recognize, analyze, and revise relevant aspects of treatment given occasional feedback;
o Shows good observational and interpretive skills; o Shows good awareness of client's perspective and needs.

B PLUS, B AND B MINUS INDICATE WORK OF SATISFACTORY QUALITY
B Plus:
o Exceeds some and satisfies all mandated requirements; o Clinical competencies show steady growth; o Shows ability to abstract and generatively apply outlined principles of treatment given
examples; o Integrates and utilizes the information provided; o Learns quickly from past mistakes in attempting to explain behavior
conceptually/theoretically; Showing steady growth in observational and interpretive skills;
o Is developing good ability to recognize and revise relevant aspects of treatment given feedback.
B:
o Has satisfied all mandated requirements; o Shows steady growth in a specified set of clinical competencies; o Requires frequent direct or respective information, but can integrate and utilize
information provided given intermittent review; o Understands and attempts to apply information given regarding: conceptual, theoretical
constructs; o Is beginning to show growth in observational and interpretive skills; o Now recognizes some aspects of treatment which need revision given feedback; o Shows emerging awareness of client's perspective and needs.
B Minus:
o Has satisfied most, but not all, mandated requirements; o Is beginning to show growth in a specified set of clinical competencies; requires direct or
prescriptive information; o Requires assistance integrating and utilizing the information provided; o Requires direct assistance applying information conceptually/theoretically; Requires
assistance in observational and interpretive skills, and in assessing client's perspective and needs;
o Incorporates suggested revisions; continues to need help recognizing the necessity and rationale for revisions.

C PLUS, C AND C MINUS INDICATE WORK OF MARGINAL QUALITY
C Plus: o Has satisfied only a few of the mandated requirements; o Is showing minimum growth only in very few clinical competencies; o Requires a great deal of direct and prescriptive information; needs much assistance
integrating and utilizing the information provided; requires much time and attention in applying information conceptually/theoretically;
o Requires a great deal of assistance in observational and interpretive skills in assessing client's perspective and needs; appears to benefit only from such assistance;
o Interprets suggestions with only a minimal understanding of why revisions are necessary relative to this client; generally, does not appropriately incorporate suggested revisions;
o Shows only occasional instances of ability to independently recognize need or rationale for revisions.
C:
o Has inadequately attempted to meet most mandated requirements; o Is not yet showing growth in a specified set of clinical competencies; o Requires repeated direct or prescriptive information; needs repeated assistance
integrating and utilizing information provided; shows little evidence of abstracting underlying principles of treatment;
o Requires repeated direct assistance applying information conceptually/theoretically; requires repeated assistance in observational and interpretive skills, and in assessing client's perspective and needs;
o Does not appear to benefit from such assistance. C Minus:
o Has not met most mandated requirements; o Shows little growth in any area of case management; o Despite repeated prescriptive information, shows complete dependence on supervisor to
determine goals, rationales, procedures and techniques appropriate for this client's treatment; relies totally on supervisor to collect and analyze data;
o Shows no independent ability to recognize or understand need or rationale for revisions.
F INDICATES FAILURE F:
o Requirements have not been met despite intensive corrective feedback and supervisor support; Records and reports are incomplete;
o Shows minimal ability to change irresponsible behavior or to grow clinically; o Should be discouraged from continuing in a clinical discipline.

Semester: __________________ Page __________ of _________
TEMPLE UNIVERSITY
DEPARTMENT OF COMMUNICATION SCIENCES
RECORD OF DAILY CLINICAL HOURS
STUDENT : ___________________________________ PRACTICUM SITE: __________________________________________ SUPERVISOR: (Print)____________________________ ASHA # : __________ Signature: _______________________ AGE CATEGORY( check one, use separate sheets for different age categories, if needed): ADULT CHILD Date Language Articulation Voice Fluency Dysphagia Audiology Related
Disorders Staffing Super
Initials Dx TX obs Dx Tx obs Dx Tx obs Dx Tx obs Dx Tx obs Dx Tx
Total
Times are to be entered in increments of quarter (.25) hours, nothing less than .25 hours (or 15 minutes) are to be counted or split. Staffing time is to include only client centered (not supervisory) conferencing as mandated by ASHA. There is a limit of 25 hours for Staffing which can be included in the total count of clinical hours. None of Staffing time goes toward minimum distributions for disorders or age categories. Activities in related disorders also does not go toward minimum distribution counts. Counseling with client or significant others is Diagnostic or Treatment contact (depending on activity) not Staffing and so is entered in Disorder and age category.

TEMPLE UNIVERSITY
DEPARTMENT OF COMMUNICATION SCIENCES
STUDENT EVALUATION OF CLINICAL PRACTICUM SITE: _____________________________________________________________
SUPERVISOR(S):____________________________________________________ STUDENT’S NAME (optional) ____________________________________ SEMESTER DATE:________________________ Use the following scale to evaluate your practicum experience and your field supervisor. SCALE 1* POOR 2* FAIR 3 GOOD 4 EXCELLENT N/A NOT APPLICABLE * please explain on reverse side PRACTICUM SITE 1. Practicum met expectations (type of caseload, workload, documentation) _____________ 2. Academic preparation _____________ 3. On-site orientation to practicum _____________ 4. Consistency of supervision _____________ 5. Balance between clinical contact hours vs. other clinical responsibilities _____________ 6. Benefit of related interdisciplinary experiences _____________ 7. Overall rating of practicum experience _____________
Commentary A. What were the strong points of this practicum?

B. How do you think this practicum could have been better? C. If you were offered a position at this site would you accept? Why or Why not?
D. What was the most important thing you learned about yourself during this practicum? SUPERVISION 1. Amount of supervision received _____________ 2. Usefulness of feedback (oral, written) _____________ 3. Frequency of feedback _____________ 4. Ability to share knowledge with you _____________ 5. Sensitivity of supervisor to your feelings and problems _____________ 6. Flexibility of supervisor _____________ 7. Overall rating of supervisor _____________
A. What are the most positive characteristics of your supervisor? B. How can your supervisor be more effective? C. What was the most important thing you learned from your supervisor?
Please provide details for ratings below 3 (good) on Practicum Site or Supervisor.

Field Supervisor’s Evaluation of Practicum Practicum Site:___________________________ Semester:__________________ Please answer the following questions as completely as possible. 1. Describe the student’s responsibilities at this practicum site. 2. How was the Temple University supervisor helpful in this practicum experience? 3. What skills was the student able to apply in this practicum setting? 4. To what extent did the student work with other professionals at this practicum
site? 5. How would you describe the student’s preparation for this practicum experience? 6. What suggestions do you have for improving this experience for:
A. Future Students
B. Supervisors C. Faculty
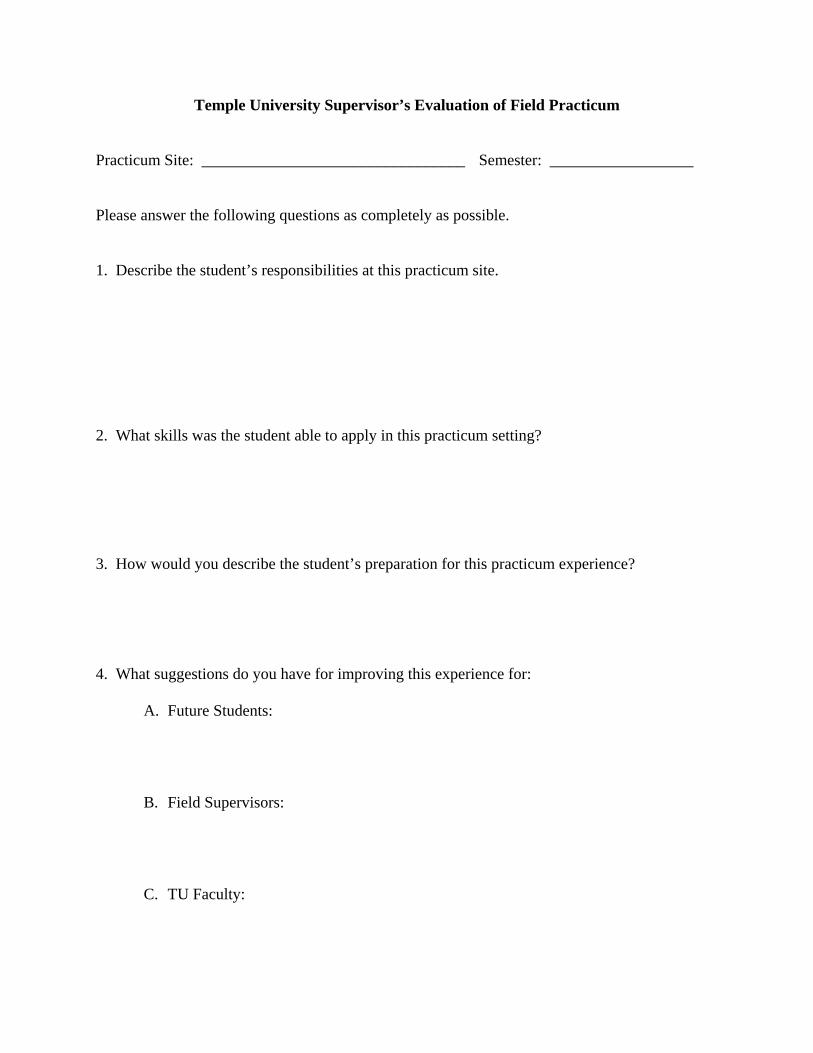
Temple University Supervisor’s Evaluation of Field Practicum Practicum Site: _________________________________ Semester: __________________ Please answer the following questions as completely as possible. 1. Describe the student’s responsibilities at this practicum site. 2. What skills was the student able to apply in this practicum setting? 3. How would you describe the student’s preparation for this practicum experience? 4. What suggestions do you have for improving this experience for:
A. Future Students:
B. Field Supervisors:
C. TU Faculty:

Clinical Supervision in Speech-LanguagePathology
Ad Hoc Committee on Supervision in Speech-Language Pathology
Reference this material as: American Speech-Language-Hearing Association. (2008). Clinical Supervisionin Speech-Language Pathology [Technical Report]. Available from www.asha.org/policy.
Index terms: supervision
doi:10.1044/policy.TR2008-00296
© Copyright 2008 American Speech-Language-Hearing Association. All rights reserved.
Disclaimer: The American Speech-Language-Hearing Association disclaims any liability to any party for the accuracy, completeness, oravailability of these documents, or for any damages arising out of the use of the documents and any information they contain.

About ThisDocument
This technical report was developed by the Ad Hoc Committee on Supervision inSpeech-Language Pathology of the American Speech-Language-HearingAssociation (ASHA). Members of the committee were Lisa O'Connor (chair),Christine Baron, Thalia Coleman, Barbara Conrad, Wren Newman, Kathy Panther,and Janet E. Brown (ex officio). Brian B. Shulman, vice president for professionalpractices in speech-language pathology (2006–2008), served as the monitoringofficer. This document was approved by the Board of Directors on March 12, 2008.
****
Introduction Because of increasing amounts of data from studies on supervision, advances intechnology, and a greater understanding of the value of interpersonal factors in thesupervisory process, there was a need to update ASHA's 1985 position statementClinical Supervision in Speech-Language Pathology and Audiology (ASHA,1985b). This 2008 technical report accompanies an updated position statement andknowledge and skills document for the profession of speech-language pathology(ASHA 2008a, 2008b). Although the principles of supervision (also called clinicalteaching or clinical education) are common to both professions, the updateddocuments address only speech-language pathology because of differences in pre-service education and practice between the two professions.
The 1985 position statement identified specified competencies for supervisors,with an emphasis on clinical supervision of students. This 2008 technical reportaddresses supervision across the spectrum of supervisees, with the exception ofspeech-language pathology assistants. Professionals looking for guidance insupervising support personnel should refer to the ASHA position statement,guidelines, and knowledge and skills documents on this topic (ASHA, 2002,2004b, 2004e).
As stated in ASHA's position statement on clinical supervision in speech-languagepathology (ASHA, 2008a), “clinical supervision (also called clinical teaching orclinical education) is a distinct area of practice in speech-language pathology and ...is an essential component in the education of students and the continualprofessional growth of speech-language pathologists” (p. 1). Clinical supervisionis also a collaborative process, with shared responsibility for many of the activitiesthroughout the supervisory experience.
At some point in their career, many speech-language pathologists (SLPs) will beinvolved in a role that involves supervising students, clinical fellows, practicingSLPs, and/or paraprofessionals. Many of these SLPs do not have formal trainingor preparation in supervision. Recognizing the importance and complexityinvolved in the supervisory process, it is critical that increased focus be devotedto knowledge of the issues and skills in providing clinical supervision across thespectrum of a professional career in speech-language pathology. The purpose ofthis technical report is to highlight key principles and issues that reflect theimportance and the highly skilled nature of providing exemplary supervision. It isnot intended to provide a comprehensive text on how to become a supervisor. Thecompanion document Knowledge and Skills Needed by Speech-Language
Clinical Supervision in Speech-Language Pathology Technical Report
1
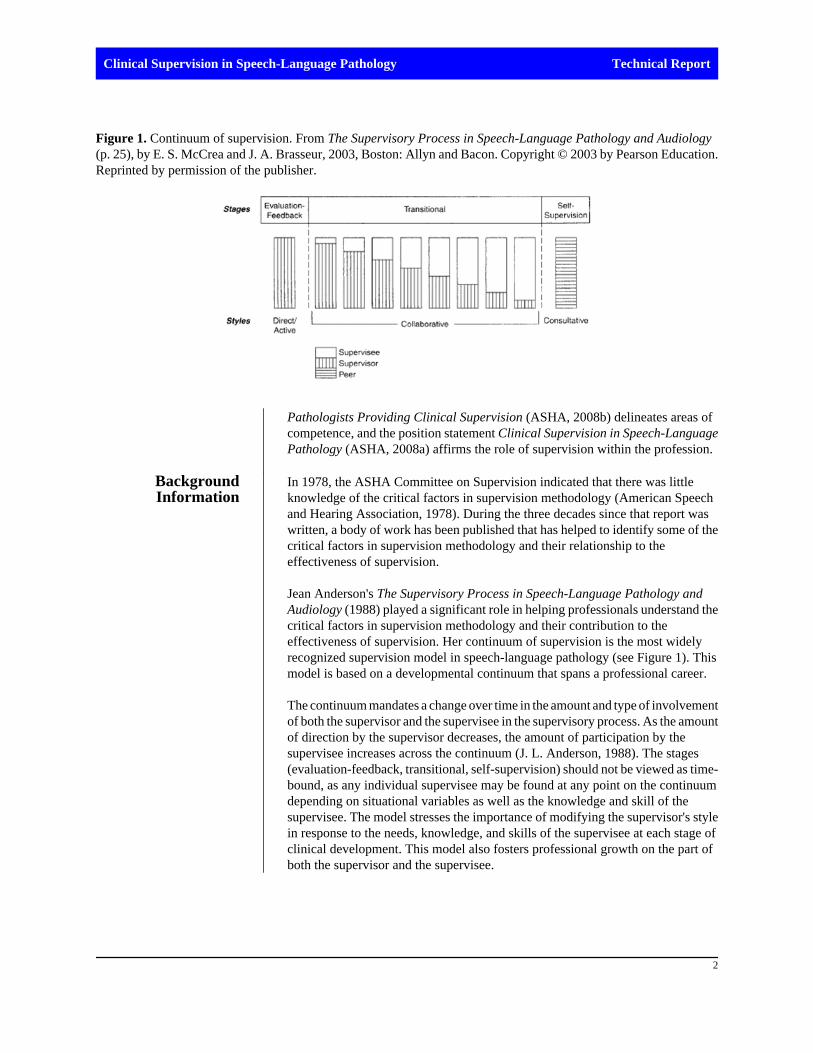
Pathologists Providing Clinical Supervision (ASHA, 2008b) delineates areas ofcompetence, and the position statement Clinical Supervision in Speech-LanguagePathology (ASHA, 2008a) affirms the role of supervision within the profession.
BackgroundInformation
In 1978, the ASHA Committee on Supervision indicated that there was littleknowledge of the critical factors in supervision methodology (American Speechand Hearing Association, 1978). During the three decades since that report waswritten, a body of work has been published that has helped to identify some of thecritical factors in supervision methodology and their relationship to theeffectiveness of supervision.
Jean Anderson's The Supervisory Process in Speech-Language Pathology andAudiology (1988) played a significant role in helping professionals understand thecritical factors in supervision methodology and their contribution to theeffectiveness of supervision. Her continuum of supervision is the most widelyrecognized supervision model in speech-language pathology (see Figure 1). Thismodel is based on a developmental continuum that spans a professional career.
The continuum mandates a change over time in the amount and type of involvementof both the supervisor and the supervisee in the supervisory process. As the amountof direction by the supervisor decreases, the amount of participation by thesupervisee increases across the continuum (J. L. Anderson, 1988). The stages(evaluation-feedback, transitional, self-supervision) should not be viewed as time-bound, as any individual supervisee may be found at any point on the continuumdepending on situational variables as well as the knowledge and skill of thesupervisee. The model stresses the importance of modifying the supervisor's stylein response to the needs, knowledge, and skills of the supervisee at each stage ofclinical development. This model also fosters professional growth on the part ofboth the supervisor and the supervisee.
Figure 1. Continuum of supervision. From The Supervisory Process in Speech-Language Pathology and Audiology(p. 25), by E. S. McCrea and J. A. Brasseur, 2003, Boston: Allyn and Bacon. Copyright © 2003 by Pearson Education.Reprinted by permission of the publisher.
Clinical Supervision in Speech-Language Pathology Technical Report
2

In addition to the publications from acknowledged experts in the profession, ASHAhas provided guidance in the area of supervision through standards, the Code ofEthics, and Issues in Ethics statements. These documents are described below inthe sections Standards, Regulations, and Legal Issues and Ethical Considerationsin Supervision.
Research onSupervision
As the profession of speech-language pathology has advanced, evidence-basedknowledge about practice in clinical disorders has developed through experimentaland descriptive research. However, there is little empirical evidence in the area ofsupervision (Spence, Wilson, Kavanagh, Strong, & Worrall, 2001), especially asit relates to client outcomes. Knowledge about supervision in speech-languagepathology has primarily come from descriptive studies documented in texts byacknowledged experts, conference proceedings, and personal and sharedexperience. The results of descriptive studies have led to the identification of someof the behaviors that supervisors need to modify in order to be less directive andto facilitate high levels of critical thinking in supervisees (Dowling, 1995; Strike-Roussos, 1988, 1995, as cited in McCrea and Brasseur, 2003). Another majorsource of information about supervision comes from the research literature fromother professions. McCrea and Brasseur (2003) examined the work of Rogers(1951), Carkhuff (1967, 1969), Leddick and Barnard (1980), and Hart (1982) inpsychology; Fiedler (1967) in business management; Kagan (1970) in social work;and Cogan (1973) and Goldhammer (1969; Goldhammer, Anderson, & Kajewski,1980) in education to show the extent to which other disciplines have contributedto our knowledge of effective supervision, and to emphasize the shared coreprinciples of supervision reagardless of the discipline and/or service deliverysetting (Dowling, 2001).
Definition ofSupervision
In 1988 Jean Anderson offered the following definition of the supervisory process:
Supervision is a process that consists of a variety of patterns of behavior,the appropriateness of which depends on the needs, competencies,expectations and philosophies of the supervisor and the supervisee and thespecifics of the situation (tasks, client, setting and other variables). Thegoals of the supervisory process are the professional growth anddevelopment of the supervisee and the supervisor, which it is assumed willresult ultimately in optimal service to clients. (p. 12)
Anderson's definition is still consistent with the goals of the process but needssome expansion. ASHA's position statement (1985b) noted that “effective clinicalteaching” involves the development of self-analysis, self-evaluation, and problem-solving skills on the part of the individual being supervised. Self-analysis and self-evaluation are important activities for the supervisor as well. Therefore, Anderson'sdefinition may be expanded to include the following:
Professional growth and development of the supervisee and the supervisorare enhanced when supervision or clinical teaching involves self-analysisand self-evaluation. Effective clinical teaching also promotes the use ofcritical thinking and problem-solving skills on the part of the individualbeing supervised.
Clinical Supervision in Speech-Language Pathology Technical Report
3

Critical thinking is based on building hypotheses, collecting data, and analyzingoutcomes. A supervisor can facilitate the critical thinking abilities of superviseesthrough collecting data and facilitating problem solving. Engaging in this processwill also help supervisees assess the quality of their service delivery. The DataCollection in Supervision section that follows provides further information on thistopic.
The following sections discuss key issues that affect supervision or influence thesupervisory process.
Supervision AcrossSettings
Professional, clinical, and operational demands across practice settings vary;however, the supervisory process can be viewed as basically the same whereverspeech-language pathology services are delivered. Client populations as well asequipment, tools, and techniques used to provide clinical services can differ acrossthe practice settings. Nevertheless, the dynamics of the supervisory relationshipand the components of the supervisory process are similar regardless of worksetting.
Often the supervisor is also responsible for day-to-day operations and programmanagement. These supervisors with management responsibilities are accountableto multiple stakeholders (e.g., administrators, regulatory agencies, consumers,employees, and payers). These supervisors also have an obligation to provideclinical teaching to supervisees at all levels of their career. Clinical education maybe managed directly by the supervisor, facilitated as a collaborative activity by thesupervisor, or delivered in peer training formats (e.g., through literature reviewand discussion, or continuing education). Methods may vary according to the needsof the clinical population, developmental level of the supervisee, supervisor andsupervisee teaching/learning styles and preferences, economics, and practicesetting. The basic objective of professional growth and development for both thesupervisor and supervisee remains at the core of the supervisory process.
Technology inSupervision
Although technology is not a new concept in supervision, the ways in whichtechnology may be used have changed immensely. It can allow one message to bereceived by many at one time (through an e-mail list) or it can provide support tojust one supervisee through the use of two-way videoconferencing (i.e., “e-supervision”). Through the use of technology, information can be delivered at adistance in real time or be archived for users to retrieve at their convenience. Manyforms of technology can be used to support communication and clinical teaching,particularly the Internet, which facilitates the use of e-mail, e-mail lists, instantmessaging, Web sites/pages, videoconferencing, video software, Weblogs (or“blogs”), and podcasting. The Appendix provides examples of current uses oftechnology for supervision. When one uses technology in supervision (e.g.,videoconferencing) it is important to be aware of and follow regulatory guidelinesinvolving confidentiality.
The Influence ofPower in Supervision
Power has been defined as the ability of one party to change or control the behavior,attitudes, opinions, objectives, needs, and values of another party (Rahim, 1989).Although different models and descriptions of power are described in the literature,some researchers have acknowledged the importance of modifying supervisees'behavior using social and interpersonal influence processes. One form of social
Clinical Supervision in Speech-Language Pathology Technical Report
4

influence is power (Wagner & Hess, 1999). According to Robyak, Goodyear, andPrange (1987), supervisors' power influences trainees to change their clinicalbehaviors. Other disciplines have extensively investigated social power becauseof the influence that power has on subordinates' compliance, motivation,satisfaction, task commitment, job performance, and interpersonal conflicts(Wagner & Hess, 1999).
Understanding the influence of social power on the supervisory relationship isimportant. Supervisors hold the power of grading, signing off on clinical hours,conducting performance evaluations, and making promotion decisions. Lack ofawareness of the influence of power can result in intimidation and a reluctance onthe part of the supervisee to participate actively in the supervisory experience.
Individuals from diverse cultural and/or linguistic backgrounds may responddifferently to the power dynamic (e.g., to people they perceive to be in roles ofauthority). They may behave in ways that may be interpreted as inappropriate bythose who are unfamiliar with their culture and/or background (Coleman, 2000).Therefore, it is important for supervisors to know when to consult someone whocan serve as a cultural mediator or advisor concerning effective strategies forculturally appropriate interactions with individuals (clients and supervisees) fromspecific backgrounds.
Mentoring inSupervision
The terms mentoring and supervision are not synonymous but are often usedinterchangeably (Urish, 2004). Mentoring is typically defined as a relationshipbetween two people in which one person (the mentor) is dedicated to the personaland professional growth of the other (the mentee) (Robertson, 1992). While thisdefinition may sound similar to the relationship of the supervisor and thesupervisee, the primary focus of supervision is accountability for the supervisee'sperformance (e.g., providing grades or conducting performance evaluations;documenting professional behavior and clinical performance). In contrast,mentoring focuses on creating effective ways to build skills, influence attitudes,and cultivate aspirations. Mentors advise, tutor, sponsor, and instill a professionalidentity in mentees. Mentoring is an intense interaction between two people, wherethe mentor has authority and power based on experience. To highlight theimportance of the mentoring role, the 2005 ASHA Standards for ClinicalCertification references mentoring. In some sections the terminology has beenchanged from supervision to mentoring and from clinical fellowship supervisor toclinical fellowship mentor (Council for Clinical Certification in Audiology andSpeech-Language Pathology [CFCC], 2005).
Some aspect of mentoring should be involved in all supervisory relationships, thedegree being dependent on supervisory style, the amount of experience and skilllevel of the supervisee, and factors associated with the practice setting. Supervisorswho maintain a “direct-active” style of supervision as described by J. L. Anderson(1988) are less likely to address the mentoring aspect of supervision. The “direct-active” style focuses mainly on growth in performance rather than on the personalgrowth of the supervisee. “Collaborative” or “consultative” styles, as described byJ. L. Anderson (1988), better facilitate the ability to address the mentoring aspectof supervision. Mentoring is most appropriate when supervisees have moved intothe advanced level of the “transitional stage” and/or the self-supervision stage onthe Anderson continuum.
Clinical Supervision in Speech-Language Pathology Technical Report
5

Training in SupervisionMany professionals are thrust into the role of supervisor or clinical educatorwithout adequate preparation or training (J. L. Anderson, 1988; Dowling, 2001;McCrea & Brasseur, 2003; Spence et al., 2001). They become “overnightsupervisors” and are forced to draw on their own past experiences as supervisees,positive or negative, as a source for their own techniques and methodologies.Supervisors in all practice settings may also have unrealistic expectationsconcerning the academic and clinical preparation of supervisees, particularlystudents.
Dowling (2001) and McCrea and Brasseur (2003) discussed research in speech-language pathology by Culatta and Seltzer (1976), Irwin (1975, 1976), McCrea(1980), Roberts and Smith (1982), and Strike-Roussos (1988, 1995) indicating thatsupervisors who engage in supervisory conferences/meetings without formalsupervisory training tend to dominate talk time, problem solving, and strategydevelopment. These supervisors tend to use the same direct style of supervisionwith all supervisees regardless of their knowledge or skill levels, and withoutregard for the supervisee's learning style, which can lead to passive superviseeinvolvement and dependence on the supervisor (J. L. Anderson, 1988). Further, adirect style of supervision diminishes the need for the supervisee to use criticalthinking and problem-solving skills. Supervisors should seek training on thesupervisory process so that they can learn about differing supervisory styles anddevelop competence in supervision. This will help ensure the use of strategies andbehaviors that promote supervisee learning and development. ASHA's Knowledgeand Skills Needed by Speech-Language Pathologists Providing ClinicalSupervision (ASHA, 2008b) lists competencies for effective supervision. Trainingin supervision can be obtained through course work, continuing educationprograms, self-study, peer mentoring, and resources from ASHA (e.g., productsand/or continuing education offerings) and from Special Interest Division 11,Administration and Supervision.
Supervisor AccountabilityQuite often, the effectiveness of a supervisor is determined by asking thesupervisee to evaluate the clinical instructor. While such evaluations do have someimportance, few supervisees have sufficient understanding of the supervisoryprocess to know what to expect of a supervisor. Further, unless completeanonymity is ensured, the likelihood of receiving honest feedback may bequestioned. Therefore, supervisors should also evaluate their own behaviorsrelative to the supervisory process. Given the lack of validated guidelines foraccomplishing such self-evaluation, supervisors must devise their own methods ofdata collection (McCrea & Brasseur, 2003) or turn to resources from other fields.Casey (1985) and colleagues (Casey, Smith, & Ulrich, 1988) developed a self-assessment guide to assist supervisors in determining their effectiveness inacquiring the 13 tasks and 81 associated competencies contained in the 1985position statement (ASHA, 1985b). Analyzing the results allows the supervisor toidentify supervisory objectives, decide on certain procedures, and determinewhether goals were accomplished.
Clinical Supervision in Speech-Language Pathology Technical Report
6

Studying the supervisory process in relation to one's own behavior is anopportunity for the supervisor to develop a personalized quality assurancemechanism, and a way to ensure accountability. Making a decision to improve asa supervisor also promotes job satisfaction, self-fulfillment, and ethical behavior,and prevents burnout (Dowling, 2001).
Data Collection in SupervisionObjective data about the supervisee's performance adds credibility and facilitatesthe supervisory process (J. L. Anderson, 1988; Shapiro, 1994). According to J. L.Anderson (1988) and Shapiro (1994), data collection methods can include ratingscales, tallying behaviors, verbatim recording, interaction analysis, andindividually designed methods. A number of tools have also been developed foranalysis of behaviors and self-assessment (J. L. Anderson, 1988; Casey et al., 1988;Dowling, 2001; McCrea & Brasseur, 2003; Shapiro, 1994). Results from theanalysis of this data can be applied both to the supervisee's clinical interactionswith clients as well as to behaviors of the supervisor and supervisee duringsupervisory conferences. Analysis of both the supervisee and supervisor'sbehaviors during supervisory conferences can yield valuable insights to improvethe interactions and outcomes of the supervisory experience for both individuals.
To be effective at their job, supervisors must be concerned about their own learningand development. Studying one's own behavior in supervisory process not onlyfacilitates accountability in clinical teaching, but also is an opportunity forsupervisors to examine their own behavior in order to improve their effectivenessin supervision.
Communication Skills in SupervisionAlthough supervisors may collect data and analyze the behaviors of supervisees,success in facilitating a supervisee's development may ultimately rest on thesupervisor's skill in communicating effectively about these behaviors. While thereare many resources that discuss interpersonal communication, McCrea andBrasseur (2003) briefly reviewed the literature in speech-language pathology onthe interpersonal aspects of the supervisory process, citing Pickering (1979, 1984,1987, 1990), Caracciolo and colleagues (1978), Crago (1987), Hagler, Casey, andDesRochers (1989), McCrea (1980), McCready and colleagues (1987, 1996), andGhitter (1987). All of these researchers found a relationship between theinterpersonal skills of supervisors and the clinical effectiveness of the supervisees.In their review of the literature, McCrea and Brasseur noted the importance of asupervisor's skill in communication. Adopting an effective communication stylefor each supervisee was shown to affect the supervisees' willingness to participatein conferences, share ideas and feelings, and positively change clinical behaviors.Ghitter (1987, as cited in McCrea & Brasseur, 2003) reported that whensupervisees perceive high levels of unconditional positive regard, genuineness,empathic understanding, and concreteness, their clinical behaviors change inpositive directions.
The ability to communicate effectively is viewed by many as an aptitude or aninnate skill that people possess without any training. However, many professionalsoperate at a level of effectiveness far below their potential (Adler, Rosenfeld, &Proctor, 2001). There are also potential barriers to clear and accuratecommunication (e.g., age, gender, social and economic status, and cultural/
Clinical Supervision in Speech-Language Pathology Technical Report
7

linguistic background). Further information addressing such barriers is includedin the sections Generational Differences and Cultural and LinguisticConsiderations in Supervision). Training in interpersonal communication is animportant component of supervisory training. Growth in the interpersonal domainwill enhance supervisors' proficiencies in interacting with clinicians in a helpfulmanner.
Standards, Regulations, and Legal IssuesVarious external groups provide guidance for or regulation of supervision inspeech-language pathology, particularly with respect to students and clinicalfellows. ASHA's standards for certification and accreditation, state licensure laws,and federal/state reimbursement programs set minimum standards for the amountof supervision provided to individuals who are not certified SLPs.
At the preprofessional level, the Standards for Accreditation of GraduateEducation Programs in Audiology and Speech-Language Pathology (Council onAcademic Accreditation in Audiology and Speech-Language Pathology [CAA],2004) require competent and ethical conduct of faculty, including on-site and off-site faculty. The standards also require programs to demonstrate that “Clinicalsupervision is commensurate with the clinical knowledge and skills of eachstudent…” (Standard 3.5B; CAA, 2004).
Standards and Implementation Procedures for the Certificate of ClinicalCompetence address the requirements for direct and indirect supervision ofstudents (CFCC, 2005). The standards require that student supervision be providedby a certified SLP, and that at least 25% of a student's total contact with each clientbe directly observed. The amount of supervision “should be adjusted upward if thestudent's level of knowledge, experience, and competence warrants” (CFCC,2005). Standards for clinical fellows require 36 mentoring activities, including 18hours of on-site direct client contact observation. Both sets of standards may beupdated periodically.
Regulation by state licensure boards is separate from ASHA requirements;therefore, all students, clinical fellows, and certified clinical practitioners must beaware of and adhere to ASHA certification requirements as well as their state'srequirements. Licensure laws regulate the provision of SLP services within thestate; for SLPs practicing in schools, different or additional standards may also berequired. States' requirements for student supervision may in some cases exceedASHA's requirements.
Supervisors also must be aware of regulations for student supervision issued bypayers such as the Centers for Medicare and Medicaid Services (CMS). Forservices delivered to Medicare beneficiaries under Part B, Medicare guidanceexplicitly states that the qualified SLP must be in the room at all times and beactively engaged in directing the treatment provided by the student (CMS, 2003,chapter 15, section 230B.1). There is an exception for services to Part Abeneficiaries residing in a skilled nursing facility where “line of sight” supervisionof the student by the qualified SLP is required instead of “in the room.”
Clinical Supervision in Speech-Language Pathology Technical Report
8

The nature of the supervisory relationship includes a vicarious liability for theactions of the supervisee. Supervisors hold full responsibility for the behavior,clinical services, and documentation of the student clinician. For their ownprotection as well as to foster the growth of students and protect the welfare ofclients, supervisors must be fully involved and aware of the performance of thestudent and address any issues that could affect patient outcomes or satisfaction.
Ethical Considerations in SupervisionASHA's Code of Ethics (2003) provides a framework for ethical behavior ofsupervisors across supervisory responsibilities. Principle of Ethics I states thatclient welfare must always be held paramount. Accordingly, the supervisor mustprovide appropriate supervision and adjust the amount and type of supervisionbased on the supervisee's performance. The supervisor ensures that the superviseefulfills professional responsibilities such as maintaining confidentiality of clientinformation, documenting client records in an accurate and timely manner, andcompleting other professional activities. In addition, the supervisor has anobligation to inform the client of the name and credentials of individuals (such asstudents) involved in their treatment.
Principle of Ethics II addresses issues of professional competence, and its rulesstate that professionals should only engage in those aspects of the profession thatare within their scope of competence. Accordingly, supervisors should seektraining in the area of effective supervisory practices to develop their competencein this area. Supervisors also have the responsibility to ensure that client servicesare provided competently by supervisees whether they are students, clinicalfellows, or practicing clinicians. In addition, the rules state that treatment delegatedto clinical fellows, students, and other nonprofessionals must be supervised by acertified speech-language pathologist.
Principle of Ethics IV addresses the ethical responsibility to maintain “harmoniousinterprofessional and intraprofessional relationships” and not abuse their authorityover students (ASHA, 2003). See the section The Influence of Power inSupervision for further discussion of this issue.
Issues in Ethics statements are developed by ASHA's Board of Ethics to provideguidance on specific issues of ethical conduct. Statements related to supervisioninclude Fees for Clinical Service Provided by Students and Clinical Fellows(ASHA, 2004a), Supervision of Student Clinicians (ASHA, 2004d), andResponsibilities of Individuals Who Mentor Clinical Fellows (2007).
Supervisors should also be cognizant of the problems that may arise fromdeveloping a social relationship with a supervisee in addition to their supervisoryrelationship. Although working together may provide opportunities forsocialization beyond professional activities, supervisors must be comfortable inaddressing a supervisee's performance without being influenced by theirrelationship outside the work setting.
King (2003) identified situations where ethical misconduct in the area ofsupervision may occur. Although King's comments were directed to thesupervision of students, these concerns can be applied to all supervisoryrelationships. According to King, situations of potential misconduct can include,
Clinical Supervision in Speech-Language Pathology Technical Report
9

but are not limited to, failure to provide a sufficient amount of supervision basedon the performance of the supervisee, failure to educate and monitor thesupervisee's protection of patient confidentiality, failure to verify appropriatecompetencies before delegating tasks to supervisees, failure to demonstrate benefitto the patient based on outcomes, and failure to provide self-assessment tools andopportunities to supervisees.
Supervision by Other ProfessionalsIncreasingly, ASHA-certified SLPs and clinical fellows may work in settingswhere their direct supervisor may be an administrator or an individual from anotherprofession. Evaluation of clinical skills by that individual is not appropriate,according to ASHA's position statement on Professional Performance Appraisalby Individuals Outside the Professions of Speech-Language Pathology andAudiology (ASHA, 1993). Peer appraisal and/or self-evaluation are recommendedas alternatives. In addition, guidelines on the Professional Performance ReviewProcess for the School-Based Speech-Language Pathologist (ASHA, 2006) wererecently developed to help address this frequently occurring situation in schools.
Access to Clinical ExternshipsPracticing SLPs participate in the training and development of those who areentering the profession. However, pressures within the workplace have createdchallenges to students gaining access to externship sites (McAllister, 2005).Students are considered by some clinicians and administrators to be a drain onexisting resources. The pace of the work, productivity demands, complexity ofclients, and program specialization can limit an organization's willingness toembrace the task of student training (McAllister, 2005). In some cases, anexternship supervisor's expectations of a student's knowledge and skills may beunrealistic and/or not met. Requirements for specified levels of supervisionimposed by regulatory agencies (e.g., CMS) have also been identified as barriersto accepting students.
Staffing shortages can also limit student placement opportunities. Student trainingis often one of the casualties of inadequate staffing in the workplace. Veteran SLPshave much to offer students and other supervisees, but these individuals may workon a part-time or as-needed basis. Organizations that implement flexible workschedules to retain seasoned employees may refuse student placements becausethey believe they cannot accommodate the students' scheduling needs (McAllister,2005). An unfortunate irony exists because sites that do not offer student externshipplacements are less likely to successfully recruit qualified SLPs.
McAllister (2005) posited the need for innovative solutions in the following areas.A shift in training models may be necessary in some cases to provide moreopportunities for student placements. Ingenuity and collaboration betweenuniversities and work sites can ultimately produce innovative scheduling,supervisory incentives, and exploration of new supervisory models that may allowfor excellent training opportunities. Cooperative partnerships between theuniversities, work sites, and clinicians are needed to develop collaborative trainingmodels appropriate to work site demands and pressures. Universities can play akey role in assisting work sites in experimenting with and evaluating innovativetraining models and in educating potential and existing supervisors on bestpractices in clinical education.
Clinical Supervision in Speech-Language Pathology Technical Report
10

Cultural and Linguistic Considerations in SupervisionThe population of the United States is becoming increasingly diverse. Supervisorswill interact more frequently with individuals from backgrounds that are differentfrom their own. As they interact with others, supervisors will have to take intoaccount culturally based behaviors, values, and belief systems to be successful intheir interactions. No universal communication, learning, or behavioral style isused by all people. Many cultural values have a significant impact on how andwhen individuals choose to communicate, how they behave in various settings,and how they prefer to learn. Differences in cultural values have an impact on thenature and effectiveness of all aspects of clinical interactions, including supervisor-supervisee relationships. Supervisors must take into consideration culturally basedbehaviors and learning styles of supervisees if their interactions with them are tobe successful (Coleman, 2000).
Shapiro, Ogletree, and Brotherton (2002) reported research findings that mostfaculty were viewed as not being prepared for engaging in the supervisory processeven with students from mainstream backgrounds. This problem is even morewidespread in view of previous findings that most SLPs do not believe they areprepared to work effectively with clients from culturally and linguistically diversebackgrounds (ASHA, 1985a; Carey, 1992; Coleman & Lieberman, 1995; Keough,1990). The lack of understanding and/or appreciation for culturally andlinguistically diverse clients could also have a significant impact on the nature ofinteractions these professionals have with other nontraditional students, such asolder students or returning students (McAllister, 2005).
Supervisors who supervise individuals from culturally and linguistically diversebackgrounds should develop competencies that will help them engage inappropriate clinical education practices (ASHA, 1998a, 1998b, 2004c, 2005).Many researchers across disciplines have addressed the issue of culturallyappropriate clinical intervention strategies (Adler, 1993; N. B. Anderson, 1992,Battle, 1993, Cheng, 1987, Langdon & Cheng, 1992). One of the first suggestionsin most of these sources is that the service provider conduct a self-inventory of hisor her cultural awareness and sensitivity. Resources for cultural competenceawareness assessment may be obtained through ASHA and/or literature review.Recognizing that behavior may be influenced by culture allows supervisors todevelop a better understanding of variations among people.
Generational DifferencesThe coexistence of multiple generations in the workforce presents uniquechallenges in supervision. Differences in values and expectations of one generationversus another can result in misinterpretations and misunderstandings duringsupervisor–supervisee interactions. McCready (2007) noted that various authors(Kersten, 2002; Lancaster & Stillman, 2002; and Raines, 2002, 2003) havementioned that the disparities among generations today are deeper and morecomplex than in the past. According to Lancaster and Stillman (2002), there arefour separate and distinct generations working together today: the Traditionalists(born between 1900 and 1945), the Baby Boomers (born 1946–1964), theGeneration Xers (born 1965–1980), and the Millennials (1981–1999). People,places, events, and symbols not only define each of these generational cohorts but
Clinical Supervision in Speech-Language Pathology Technical Report
11

profoundly influence their values and expectations. Supervisors therefore need tobe prepared to understand and accommodate attitudes and behaviors that maydiffer from their own.
McCready (2007) described ways in which supervisors across work settings canbridge the generation gap and facilitate improved communication. One suggestionis to form study groups to investigate the research in this area; the group could thenpresent their findings to a larger group within the work setting (McCready, 2007).The supervisor can also engage in discussions about the generations representedin the work setting and how generational characteristics may and may not applyto specific individuals (McCready, 2007). Such discussion might includegenerational characteristics that can lead to miscommunication andmisunderstandings in interactions with clients and supervisors.
Supervising Challenging SuperviseesStudents who are admitted to graduate programs in communication sciences anddisorders have successfully passed through a very competitive screening processusing a variety of selection criteria such as Graduate Record Examination scores,undergraduate grade point averages, and letters of recommendation. Most of thesestudents perform well in their academic courses and clinical assignments.However, most training programs periodically encounter students who presentspecial challenges during the supervisory process (Shapiro et al., 2002) and areoften referred to as “marginal” students. Dowling (1985, as cited in Dowling, 2001)described marginal students as individuals who “cannot work independently, areunable to formulate goals and procedures, have basic gaps in conceptualunderstanding, and cannot follow through with suggestions” (p. 162). Given theimpact on students, programs, clients, and the professions, working effectivelywith marginal students deserves serious and systematic consideration (Shapiro etal., 2002). These same issues may apply to supervisees of varying experience levelsand in all practice settings.
One characteristic that is frequently reported about these challenging superviseesis their lack of ability to accurately evaluate their skill level (Kruger & Dunning,1999, as cited in McCrea & Brasseur, 2003). Using the supervisory conference/meeting can be critically important in assisting them in evaluating their ownperformance (Dowling, 2001). During these meetings, supervisors need to givespecific feedback based on data collected about the supervisee's performance andprovide concrete assistance in planning and strategy development (Dowling,2001). Eventually, however, the supervisee must learn to engage in self-analysisand self-evaluation to develop an understanding of his or her own performance.
Summary This document defines supervision and highlights key issues that reflect thecomplexity of providing exemplary supervision. Acquiring competency as asupervisor is essential to developing supervisory behaviors and activities that arecritical to the training of professionals. Such supervisory training may not beprovided as part of graduate education programs; therefore, SLPs must look tocontinuing education opportunities, peer learning and mentoring, and self-studyusing literature that focuses on the supervisory process (J. L. Anderson, 1988;Casey et al., 1988; Dowling, 2001; McCrea & Brasseur, 2003; Shapiro, 1994;Shapiro & Anderson, 1989). Although there may be opportunities to learn fromother disciplines that also use supervisory practices, preparation in the supervisory
Clinical Supervision in Speech-Language Pathology Technical Report
12

process specific to speech-language pathology is critically important. McCrea andBrasseur (2003) and Dowling (2001) discussed ways in which preparation in thesupervisory process can be implemented. The models discussed in these texts rangefrom inclusion of information in early clinical management courses to doctorallevel preparation. Training that is included as part of academic and clinical trainingof professionals and extended to supervisors at off-campus practicum sites willenhance the supervisors' effectiveness (Dowling, 1992; and Dowling, 1993, 1994,as cited in McCrea & Brasseur, 2003). ASHA's Knowledge and Skills Needed bySpeech-Language Pathologists Providing Clinical Supervision (ASHA, 2008b)delineates specific areas of competence deemed necessary to the provision ofeffective supervision.
Research Directions Systematic study and investigation of the supervisory process is necessary toexpand the evidence base from which increased knowledge about supervision andthe supervisory process will emerge. Topics for further research may include thefollowing:
• exploring different supervisory approaches that promote problem solving, self-analysis, and self-evaluation to develop clinical effectiveness;
• identifying essential components of training effective supervisors;• examining the efficacy of supervisory training on supervisor/supervisee
satisfaction and competence;• identifying the basic behaviors/skills that supervisors should use in their
interactions with supervisees that are essential to an effective workingrelationship;
• examining how supervisory style affects the development of clinicalcompetence;
• examining different methods to develop more efficient models of supervision;• examining supervisor behaviors that enhance supervisee growth (e.g.,
examining the process for negotiating and mutually agreeing on targets forchange and measuring the impact that supervisor change has on thesupervisee's professional growth) or training supervisors to use specificinterpersonal skills (e.g, empathy, active listening) and then measuring howsuch skills enhance supervisee growth (McCrea & Brasseur, 2003);
• examining the effectiveness and efficiency of technology in deliveringsupervision;
• examining the impact of supervision on client outcomes;• examining supervisory approaches and communication styles with supervisees
in consideration of gender, age, cultural, and linguistic diversity;• examining aspects of the supervisory process (i.e., understanding, planning,
observing, analyzing, and integrating) and the relationship of each to thesuccess of the supervisory experience (McCrea & Brasseur, 2003).
References Adler, S. (1993). Nonstandard language: Its assessment in multicultural communicationskills in the classroom. Boston: Allyn & Bacon.
Adler, S., Rosenfeld, L. B., & Proctor, R. F. (2001). Interplay: The process of interpersonalcommunication. New York: Harcourt.
American Speech and Hearing Association. (1978). Current status of supervision of speech-language pathology and audiology [Special Report]. Asha, 20, 478–486.
American Speech-Language-Hearing Association. (1985a). Clinical management ofcommunicatively handicapped minority language populations [Position Statement].Available from www.asha.org/policy.
Clinical Supervision in Speech-Language Pathology Technical Report
13

American Speech-Language-Hearing Association. (1985b). Clinical supervision in speech-language pathology and audiology [Position Statement]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (1993). Professional performanceappraisal by individuals outside the professions of speech-language pathology andaudiology [Position Statement]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (1998a). Students and professionals whospeak English with accents and nonstandard dialects: Issues and recommendations[Position Statement]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (1998b). Students and professionals whospeak English with accents and nonstandard dialects: Issues and recommendations[Technical Report]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2002). Knowledge and skills forsupervisors of speech-language pathology assistants. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2003). Code of ethics (Revised).Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2004a). Fees for clinical serviceprovided by students and clinical fellows [Issues in Ethics]. Available fromwww.asha.org/policy.
American Speech-Language-Hearing Association. (2004b). Guidelines for the training,use, and supervision of speech-language pathology assistants. Available fromwww.asha.org/policy.
American Speech-Language-Hearing Association. (2004c). Knowledge and skills neededby speech-language pathologists and audiologists to provide culturally andlinguistically appropriate services [Knowledge and Skills]. Available fromwww.asha.org/policy.
American Speech-Language-Hearing Association. (2004d). Supervision of studentclinicians [Issues in Ethics]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2004e). Training, use, and supervisionof support personnel in speech-language pathology [Position Statement]. Availablefrom www.asha.org/policy.
American Speech-Language-Hearing Association. (2005). Cultural competence [Issues inEthics]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2006). Professional performancereview process for the school-based speech-language pathologist [Guidelines].Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2007). Responsibilities of individualswho mentor clinical fellows [Issues in Ethics]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2008a). Clinical supervision in speech-language pathology [Position Statement]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2008b). Knowledge and skills neededby speech-language pathologists providing clinical supervision. Available fromwww.asha.org/policy.
Anderson, J. L. (1988). The supervisory process in speech language pathology andaudiology. Austin, TX: Pro-Ed.
Anderson, N. B. (1992). Understanding cultural diversity. American Journal of Speech-Language Pathology, 1, 11–12.
Battle, D. (1993). Communication disorders in multicultural populations. Boston:Butterworth-Heinemann.
Carey, A. I. (1992). Get involved: Multiculturally. Asha, 34, 3–4.Casey, P. (1985). Supervisory skills self-assessment. Whitewater: University of Wisconsin.Casey, P., Smith, K., & Ulrich, S. (1988). Self supervision: A career tool for audiologists
and speech-language pathologists (Clinical Series No. 10). Rockville, MD: NationalStudent Speech Language Hearing Association.
Clinical Supervision in Speech-Language Pathology Technical Report
14

Centers for Medicare and Medicaid Services Medicare benefit policy manual. 2003Retrieved December 13, 2008, from http://www.cms.hhs.gov/manuals/downloads/bp102c15.pdf
Cheng, L. (1987). Assessing Asian language performance. Gaithersburg, MD: AspenPublishers.
Coleman, T. J. (2000). Clinical management of communication disorders in culturallydiverse children. Needham Heights, MA: Allyn & Bacon.
Coleman, T. J., & Lieberman, R. J. (1995, November). Preparing speech-languagepathologists for work with diverse populations: A survey . Paper presented at the AnnualConvention of the American Speech-Language-Hearing Association, Anaheim, CA.
Council for Clinical Certification in Audiology and Speech-Language Pathology. (2005).Membership and certification handbook of the American Speech-Language-HearingAssociation. Retrieved December 28, 2007, from www.asha.org/about/membership-certification/handbooks/slp/slp_standards.htm
Council on Academic Accreditation in Audiology and Speech-Language Pathology. (2004).Standards for accreditation of graduate education programs in audiology and speech-language pathology programs. Available from www.asha.org/policy.
Dowling, S. (1992). Implementing the supervisory process: Theory and practice.Englewood Cliffs, NJ: Prentice-Hall.
Dowling, S. (1995). Conference question usage: Impact of supervisory training. In R. Gillam(Ed.), The supervisors' forum (Vol. 2, pp. 11–14). Nashville, TN: Council of Supervisorsin Speech-Language Pathology and Audiology.
Dowling, S. (2001). Supervision: Strategies for successful outcomes and productivity.Needham Heights, MA: Allyn & Bacon.
Dudding, C., & Justice, L. (2004). An e-supervision model: Videoconferencing as a clinicaltraining tool. Communication Disorders Quarterly, 25(3), 145–151.
Keough, K. (1990). Emerging issues for the professions in the 1990s. Asha, 32, 55–58.King, D. (2003, May 27). Supervision of student clinicians: Modeling ethical practice for
future professionals. The ASHA Leader, 8, 26.Lancaster, L., & Stillman, D. (2002). When generations collide. New York: Harper
Business.Langdon, H. W., & Cheng, L. (1992). Hispanic children and adults with communication
disorders. Gaithersburg, MD: Aspen Publishers.McAllister, L. (2005). Issues and innovations in clinical education. Advances in Speech-
Language Pathology, 7(3), 138–148.McCrea, E. S., & Brasseur, J. A. (2003). The supervisory process in speech-language
pathology and audiology. Boston: Allyn & Bacon.McCready, V. (2007). Generational differences: Do they make a difference in supervisory
and administrative relationships? Perspectives in Administration and Supervision, 17(3), 6–9.
Rahim, M. A. (1989). Relationships of leader power to compliance and satisfaction withsupervision: Evidence from a national sample of managers. Journal of Management,15, 495–516.
Robertson, S. C. (1992). Find a mentor or be one. Bethesda, MD: American OccupationalTherapy Association.
Robyak, J. E., Goodyear, R. K., & Prange, M. (1987). Effects of supervisors' sex, focus andexperience on preferences for interpersonal power bases. Counselor Education andSupervision, 26, 299–309.
Shapiro, D. A. (1994). Interaction analysis and self-study: A single-case comparison of fourmethods of analyzing supervisory conferences. Language, Speech, and Hearing Servicesin Schools, 25, 67–75.
Shapiro, D. A., & Anderson, J. L. (1989). One measure of supervisory effectiveness inspeech-language pathology and audiology. Journal of Speech and Hearing Disorders,54, 549–557.
Clinical Supervision in Speech-Language Pathology Technical Report
15

Shapiro, D. A., Ogletree, B. T., & Brotherton, W. D. (2002). Graduate students withmarginal abilities in communication sciences and disorders: Prevalence, profiles, andsolutions. Journal of Communication Disorders, 35, 421–451.
Spence, S., Wilson, J., Kavanagh, D., Strong, J., & Worrall, L. (2001). Clinical supervisionin four mental health professions: A review of the evidence. Behavior Change, 18, 135–155.
Strauss, W., & Howe, N. (1992). Generations: The history of America's future 1584 to2069. New York: Morrow.
Urish, C. (2004). Ongoing competence through mentoring. Bethesda, MD: AmericanOccupational Therapy Association.
Wagner, B. T., & Hess, C. H. (1999). Supervisors' use of social power with graduatesupervisees in speech-language pathology. Journal of Communication Disorders, 32,361–368.
Clinical Supervision in Speech-Language Pathology Technical Report
16

Appendix
Uses of Current Technology for SupervisionE-mail with attachments: The primary benefit of using electronic mail is the speed of delivery versus traditional mail.If contacting the supervisor by phone is difficult, an e-mail message may be sent instead. With e-mail, the supervisorhas the option of responding at his or her convenience rather than trying to schedule a phone call or a face-to-facemeeting with the supervisee when only a short response may be required. Lesson plans, sample individualized educationprogram goals, diagnostic reports, and so on may be attached and submitted to the supervisor for his or her review andcomment.
E-mail lists: Sending messages via e-mail to a closed list of supervisees. Each supervisee has the opportunity to askquestions, pose problems, or ask for suggested resources from peers. This can be extremely powerful in learning fromeach other's experiences and sharing innovative ideas or tried-and-true therapy techniques.
Instant messaging: The individual can see which other individuals are available at their computer through “buddy”icons and contact them through instant messaging. A group can communicate in an instant messaging conference, orthe SLP can converse with his or her supervisor instantly rather than waiting for the supervisor to check e-mail.
Web sites/Web pages: Information pertinent to supervisees (such as frequently asked questions on licensure renewal,guidelines on service delivery options, or frequently used forms) is placed on the supervisor's Web site. The superviseescan access the information when needed. Supervisees can suggest what materials, links, or resources they would findhelpful to have uploaded to the supervisor's site.
E-supervision: Using two-way videoconferencing to supervise graduate students in a public school setting is oneexample of electronic supervision according to Dudding and Justice (2004). The equipment costs of videoconferencingare offset by the productivity in clinical instruction. Dudding and Justice reported that electronic supervision allowsfor more flexibility in scheduling and a reduction in travel costs while also increasing the student's knowledge andappreciation for technology.
Video software: Embedding a visual message within an e-mail or on a Web site provides access to information whenit is needed, and the message can be archived for later reference as well. With the use of video software, the supervisorcan easily video record a message while also embedding photos or graphics into the message. The software requires asimple mounted camera on the computer to video record the supervisor's message. The message can be an update ontherapy techniques or a short training on the use of new forms, for example. Once recorded, it can be embedded intoan e-mail and sent out to all of the supervisees or archived on a Web site to be accessed when needed. This expeditesthe training process by only recording and delivering the message one time and makes the information available whenthe supervisee has time to retrieve the information, which can differ for all involved.
Weblogs: Journal entries displayed in reverse chronological order. The supervisor and others can leave comments orstatements of support for the supervisee in this interactive format.
Clinical Supervision in Speech-Language Pathology Technical Report
17

Code of Ethics
Reference this material as: American Speech-Language-Hearing Association. (2003). Code of Ethics [Ethics].Available from www.asha.org/policy.
Index terms: ethics
DOI: 10.1044/policy.ET2003-00166Rev. 01/1/2003
© Copyright 2003 American Speech-Language-Hearing Association. All rights reserved.
Disclaimer: The American Speech-Language-Hearing Association disclaims any liability to any party for the accuracy, completeness, oravailability of these documents, or for any damages arising out of the use of the documents and any information they contain.

Preamble The preservation of the highest standards of integrity and ethical principles is vitalto the responsible discharge of obligations by speech-language pathologists,audiologists, and speech, language, and hearing scientists. This Code of Ethics setsforth the fundamental principles and rules considered essential to this purpose.
Every individual who is (a) a member of the American Speech-Language-HearingAssociation, whether certified or not, (b) a nonmember holding the Certificate ofClinical Competence from the Association, (c) an applicant for membership orcertification, or (d) a Clinical Fellow seeking to fulfill standards for certificationshall abide by this Code of Ethics.
Any violation of the spirit and purpose of this Code shall be considered unethical.Failure to specify any particular responsibility or practice in this Code of Ethicsshall not be construed as denial of the existence of such responsibilities or practices.
The fundamentals of ethical conduct are described by Principles of Ethics and byRules of Ethics as they relate to the conduct of research and scholarly activitiesand responsibility to persons served, the public, and speech-language pathologists,audiologists, and speech, language, and hearing scientists.
Principles of Ethics, aspirational and inspirational in nature, form the underlyingmoral basis for the Code of Ethics. Individuals shall observe these principles asaffirmative obligations under all conditions of professional activity.
Rules of Ethics are specific statements of minimally acceptable professionalconduct or of prohibitions and are applicable to all individuals.
Principle of Ethics I Individuals shall honor their responsibility to hold paramount the welfare ofpersons they serve professionally or participants in research and scholarly activitiesand shall treat animals involved in research in a humane manner.
Rules of EthicsA. Individuals shall provide all services competently.B. Individuals shall use every resource, including referral when appropriate, to
ensure that high-quality service is provided.C. Individuals shall not discriminate in the delivery of professional services or
the conduct of research and scholarly activities on the basis of race or ethnicity,gender, age, religion, national origin, sexual orientation, or disability.
D. Individuals shall not misrepresent the credentials of assistants, technicians, orsupport personnel and shall inform those they serve professionally of the nameand professional credentials of persons providing services.
E. Individuals who hold the Certificates of Clinical Competence shall notdelegate tasks that require the unique skills, knowledge, and judgment that arewithin the scope of their profession to assistants, technicians, supportpersonnel, students, or any nonprofessionals over whom they have supervisoryresponsibility. An individual may delegate support services to assistants,technicians, support personnel, students, or any other persons only if thoseservices are adequately supervised by an individual who holds the appropriateCertificate of Clinical Competence.
Code of Ethics Ethics
1
F. Individuals shall fully inform the persons they serve of the nature and possibleeffects of services rendered and products dispensed, and they shall informparticipants in research about the possible effects of their participation inresearch conducted.
G. Individuals shall evaluate the effectiveness of services rendered and ofproducts dispensed and shall provide services or dispense products only whenbenefit can reasonably be expected.
H. Individuals shall not guarantee the results of any treatment or procedure,directly or by implication; however, they may make a reasonable statement ofprognosis.
I. Individuals shall not provide clinical services solely by correspondence.J. Individuals may practice by telecommunication (for example, telehealth/e-
health), where not prohibited by law.K. Individuals shall adequately maintain and appropriately secure records of
professional services rendered, research and scholarly activities conducted,and products dispensed and shall allow access to these records only whenauthorized or when required by law.
L. Individuals shall not reveal, without authorization, any professional orpersonal information about identified persons served professionally oridentified participants involved in research and scholarly activities unlessrequired by law to do so, or unless doing so is necessary to protect the welfareof the person or of the community or otherwise required by law.
M. Individuals shall not charge for services not rendered, nor shall theymisrepresent services rendered, products dispensed, or research and scholarlyactivities conducted.
N. Individuals shall use persons in research or as subjects of teachingdemonstrations only with their informed consent.
O. Individuals whose professional services are adversely affected by substanceabuse or other health-related conditions shall seek professional assistance and,where appropriate, withdraw from the affected areas of practice.
Principle of Ethics II Individuals shall honor their responsibility to achieve and maintain the highestlevel of professional competence.
Rules of EthicsA. Individuals shall engage in the provision of clinical services only when they
hold the appropriate Certificate of Clinical Competence or when they are inthe certification process and are supervised by an individual who holds theappropriate Certificate of Clinical Competence.
B. Individuals shall engage in only those aspects of the professions that are withinthe scope of their competence, considering their level of education, training,and experience.
C. Individuals shall continue their professional development throughout theircareers.
D. Individuals shall delegate the provision of clinical services only to: (1) personswho hold the appropriate Certificate of Clinical Competence; (2) persons inthe education or certification process who are appropriately supervised by an
Code of Ethics Ethics
2

individual who holds the appropriate Certificate of Clinical Competence; or(3) assistants, technicians, or support personnel who are adequately supervisedby an individual who holds the appropriate Certificate of Clinical Competence.
E. Individuals shall not require or permit their professional staff to provideservices or conduct research activities that exceed the staff member'scompetence, level of education, training, and experience.
F. Individuals shall ensure that all equipment used in the provision of services orto conduct research and scholarly activities is in proper working order and isproperly calibrated.
Principle of EthicsIII
Individuals shall honor their responsibility to the public by promoting publicunderstanding of the professions, by supporting the development of servicesdesigned to fulfill the unmet needs of the public, and by providing accurateinformation in all communications involving any aspect of the professions,including dissemination of research findings and scholarly activities.
Rules of EthicsA. Individuals shall not misrepresent their credentials, competence, education,
training, experience, or scholarly or research contributions.B. Individuals shall not participate in professional activities that constitute a
conflict of interest.C. Individuals shall refer those served professionally solely on the basis of the
interest of those being referred and not on any personal financial interest.D. Individuals shall not misrepresent diagnostic information, research, services
rendered, or products dispensed; neither shall they engage in any scheme todefraud in connection with obtaining payment or reimbursement for suchservices or products.
E. Individuals' statements to the public shall provide accurate information aboutthe nature and management of communication disorders, about theprofessions, about professional services, and about research and scholarlyactivities.
F. Individuals' statements to the public—advertising, announcing, and marketingtheir professional services, reporting research results, and promoting products—shall adhere to prevailing professional standards and shall not containmisrepresentations.
Principle of Ethics IV Individuals shall honor their responsibilities to the professions and theirrelationships with colleagues, students, and members of allied professions.Individuals shall uphold the dignity and autonomy of the professions, maintainharmonious interprofessional and intraprofessional relationships, and accept theprofessions' self-imposed standards.
Rules of EthicsA. Individuals shall prohibit anyone under their supervision from engaging in any
practice that violates the Code of Ethics.B. Individuals shall not engage in dishonesty, fraud, deceit, misrepresentation,
sexual harrassment, or any other form of conduct that adversely reflects on theprofessions or on the individual's fitness to serve persons professionally.
C. Individuals shall not engage in sexual activities with clients or students overwhom they exercise professional authority.
Code of Ethics Ethics
3

D. Individuals shall assign credit only to those who have contributed to apublication, presentation, or product. Credit shall be assigned in proportion tothe contribution and only with the contributor's consent.
E. Individuals shall reference the source when using other persons' ideas,research, presentations, or products in written, oral, or any other mediapresentation or summary.
F. Individuals' statements to colleagues about professional services, researchresults, and products shall adhere to prevailing professional standards and shallcontain no misrepresentations.
G. Individuals shall not provide professional services without exercisingindependent professional judgment, regardless of referral source orprescription.
H. Individuals shall not discriminate in their relationships with colleagues,students, and members of allied professions on the basis of race or ethnicity,gender, age, religion, national origin, sexual orientation, or disability.
I. Individuals who have reason to believe that the Code of Ethics has beenviolated shall inform the Board of Ethics.
J. Individuals shall comply fully with the policies of the Board of Ethics in itsconsideration and adjudication of complaints of violations of the Code ofEthics.
Code of Ethics Ethics
4










![supervisory Policy Manual - Hong Kong Monetary · Supervisory Policy Manual RE-1 Recovery Planning V1 – [20.06.14] 1 This module should be read in conjunction with the Introduction](https://img.pdfslide.net/doc/110x75/5b06e1257f8b9ae9628da77a/supervisory-policy-manual-hong-kong-policy-manual-re-1-recovery-planning-v1-.jpg)


















