Embed Size (px)
Citation preview

© 2018 American Medical Association. All rights reserved.
Supplementary Online Content
Birch DG, Bernstein PS, Iannacone A, et al. Effect of oral valproic acid vs placebo for vision loss
in patients with autosomal dominant retinitis pigmentosa: a randomized phase 2 multicenter
placebo-controlled clinical trial. JAMA Ophthamol. Published online June 7, 2018.
doi:10.1001/jamaophthalmol.2018.1171
eMethods. Supplemental methods
eResults. Supplemental results
eFigure 1. VPA Black Box warning
eFigure 2. Static perimetry test locations
eFigure 3. Examples of visual fields
eTable 1. Major eligibility criteria
eTable 2. Randomization and study completion
eTable 3. Daily dosing schedule
eTable 4. Dosage weight by schedule
eTable 5. Screen failures
eTable 6. Summary of genetic mutations by treatment arm
eTable 7. Mean (SD) of visual field area by treatment arm at baseline
eTable 8. Adverse events by treatment arm
This supplementary material has been provided by the authors to give readers additional
information about their work.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eMethods. Supplemental methods
Study organization, oversight and regulatory compliance
The study sponsors were the Foundation Fighting Blindness (Columbia, MD) and the US
Department of Defense (Fort Detrick, MD). Endpoint measures were read (masked to treatment
assignment) by a central reading center (Casey Reading Center, Casey Eye Institute, Oregon
Health & Science University). Trial coordination, data management, site monitoring, medical
monitoring and statistical analysis were performed by The Emmes Corporation, Rockville, MD.
Drug supplies, storage, labeling and disposition was managed by Catalent Pharma Solutions
(10381 Decatur Road Philadelphia PA 19154). Genotyping was performed by GeneDx (207
Perry Parkway, Gaithersburg, MD 20877), clinical chemistry analysis was performed by local
laboratories, VPA levels were measured at LabConnect (100 LabConnect Lane, Johnson City,
TN 37615). Data and safety monitoring oversight was provided by an independent Data and
Safety Monitoring Committee, a central institutional review board (Western IRB, 1019 39th
Avenue SE Suite 120, Puyallup, WA 98374-2115) and local IRBs for the clinical sites. Owing to
the funding mechanism, oversight was also provided by the Human Research Protection Office,
U.S. Army Medical Research and Materiel Command, 810 Schreider Street, Fort Detrick, MD
21702-5000).
Primary endpoint considerations
Perhaps the most important consideration for a clinical therapeutic trial is the choice of the
primary endpoint. Selection of a primary functional endpoint for a clinical trial for an inherited
retinal degeneration depends upon factors related to the putative therapeutic agent, disease
stage and severity of disease, pathogenesis, action and basis of the potential benefit of the
drug, and anticipated cellular or tissue capacity of the participant to respond to the
intervention. Earlier-stage RP may be potentially more treatable than late-stage disease since
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
the latter would require photoreceptor regeneration in a tissue that shows minimal replicative
capacity. Other points that need to be considered include patient selection, the time required to
administer the test, test-retest variability, and the suitability of the endpoint for not only a given
trial but also the long-term follow-up study that often follows.
For kinetic perimetry, the decision about which test target to choose as primary endpoint is
influenced by the patient population to be studied, participant inclusion and exclusion criteria,
and whether the trial is powered to detect a significant improvement or a worsening over the
observation interval. To detect a significant improvement, the primary endpoint selected should
be sufficiently abnormal to allow for detection of an increase in the isopter area, whereas to
detect a significant worsening, the primary endpoint should be abnormal but sufficiently intact to
detect a change in the decrease over time. As discussed in the main manuscript, the motivation
for performing the study was the claim of an improvement in field sensitivity as detected by
kinetic perimetry. Because the VPA study was powered to detect an improvement in sensitivity,
in order to detect clinically significant improvement in the treatment arm, the ideal participants
should already have substantial defects in the primary endpoint.
Theoretically, of the three test target sizes (I4e, III4e, and V4e) most frequently used, the most
sensitive test target for detecting an improvement or worsening following drug administration for
early disease is the I4e test target (smallest size). Indeed, one study found that the I4e isopter
area was the most sensitive of the three to detect significant progression in 16 patients with RP
over a 2-year follow-up period.9 The I4e test target isopter area, however, typically becomes
abnormal early in inherited retinal diseases such as RP and often within a few years becomes
too impaired to reliable detect either an increase in isopter area indicating improvement or a
less rapid decrease indicating slowing of progression. The III4e test target (mid-size target) is
optimal for late early-stage to mid-stage disease, and is often still measurable in late-stage
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
disease. The V4e test target (largest target) is optimal for studies of patients who have mostly
late mid-stage to late-stage disease. Many patients with early and some with mid-stage disease
may have, at most, minimal or very modest field loss, respectively, with the V4e test
target.10 The III4e test target appears the best single choice for detection of change in kinetic
field for participants with early-to-late stage disease.
Thus, the I4e test target would be an acceptable endpoint for treatment of a relatively short-term
trial of a candidate that has a high likelihood of efficacy in very early disease. For the primary
endpoint of a treatment trial of mostly or exclusively mid-to-late stage disease, the V4e test
target may be suitable. When the trial includes participants of a wide variety of severity, often
all three test-target isopters are measured, even if only one is chosen as the primary endpoint.
This and the above comments, support the choice of the III4e test target as the primary
endpoint.
References
1. Berson EL, Rosner B, Weigel-DiFranco C, et al. Disease progression in patients with
dominant retinitis pigmentosa and rhodopsin mutations. Invest Ophthalmol Vis Sci
2002;43(9):3027-36.
2. Clemson CM, Tzekov R, Krebs M, et al. Therapeutic potential of valproic acid for retinitis
pigmentosa. Br J Ophthalmol 2011;95(1):89-93.
Participant Randomization
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
The randomization plan was developed and stored at the Coordinating Center together with the
randomization list. A secure Internet-based eligibility, enrollment and randomization system was
integrated into the electronic data capture (EDC) system to control and document the
randomization assignments. Investigators accessed the EDC system to enroll and randomize
qualified participants. Upon randomization, the investigator was informed of the drug kit number
to provide to the participant.
Study medication and dosing
The study drug was a soft gel 250 mg valproic acid capsule, and the placebo had the same
color, size, shape, feel and smell as the study drug and was filled with peanut oil, the identical
excipient in the study drug. In the event of a missed dose, the participant would continue dosing
at the next dose and inform the site of date and dose missed. After a weight change, the
participant’s dose was adjusted according to the dosing schedule in Supplemental eTable 3.
No weight-based adjustments above 500 mg were made for females of child-bearing potential.
These participants continued to receive no more than 500mg per day. Weight was recorded at
each scheduled visit, and participants were to notify the site of any substantial weight gain or
loss (± 10kgs or 22lbs) between scheduled visits.
At each in-clinic visit (except Weeks 52 and 65), participants were given a sufficient number of
capsules to last until the next scheduled visit plus at least a 15-day overage allowance.
Participants were followed up with phone calls at weeks 1, 4, 13, 17, 22, 30, 35, 43 and 48. The
purpose of these phone calls was to assess adherence to study medication, review adverse
events, schedule additional clinic visits if needed, and clarify study procedures. Participants
were followed for a period of 13 weeks after the participant completed study drug (VPA or
placebo) one-year post-baseline.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
Study drug exposure
Assessments of the actual exposure to medication were based on the drug accountability data.
A capsule count was performed at every post-baseline in-clinic visit and was used to calculate
number of capsules taken. Percent treatment exposure was calculated as the dose taken
divided by the protocol-recommended dose according to weight and child-bearing potential.
Percent compliance with study medication was calculated as the number of capsules
administered divided by the expected number of capsules administered. Participants who
experienced dose reductions or temporary dose stoppages due to AEs or expired study drug
had their expected number of capsules reduced for the compliance calculation.
Quality control measures for perimetry performance
To compensate for the intrinsic variability in the measurement of visual fields, participants had to
demonstrate reliability in both kinetic and static visual field test-taking at the screening visit by
performing visual field replicates. It was prospectively determined that there needed to be a
difference of 20% or less in the III4e isopter-area on two consecutively-performed visual field
tests in both eyes. If the difference was greater than 20%, then a third session was performed,
and if the difference was less than 20% compared with either of the two prior fields, then
eligibility was met.
For static perimetry, reliability was assessed using the “Reliability Factor” (RF) value, a general
measure of participant performance. This value was automatically calculated by the Octopus
visual test apparatus from the positive and negative catch trial questions and is the sum of the
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
false positive answers and false negative answers, divided by the total number of catch trial
questions as follows: RF = [false positive responses + false negative responses] / [false positive
presentations + false negative presentations] expressed as a percentage. An RF of 0 indicates
no false positive or negative responses. False negative responses are more frequent than
normal in the low retinal sensitivity areas of eyes affected with retinitis pigmentosa, and false
negative responses represent the greatest contributor to an elevated RF in these participants.
Accordingly, if false positives were no greater than 10% of false positive presentations, visual
fields were accepted with an RF of 25% and, in some instances 30%, if the false positive rate
was acceptably low. The RF value was assessed at Screening where only one session was
required. If the RF value was greater than 20%, or had greater than 10% false positives for
either eye, then up to two additional sessions were performed. SP was performed in duplicate at
baseline and then once at weeks 26 and 52.
Power and sample size calculation
To determine the sample size for this study, data from Berson and colleagues1 were used in
which longitudinal rates of change in untreated participants with dominant retinitis pigmentosa
and rhodopsin mutations were calculated (n=27, decline=-0.0449 deg2/year, SE=0.0076,
SD=0.0395). Clemson2 saw a substantial improvement in visual field area within 6 months in
VPA-treated RP participants. A sample size of 35 in each treatment group provided 80% power
to detect a 60% treatment effect (placebo mean change of -0.0449, VPA mean change of -
0.0180), assuming a two-sided α=0.05 and equal standard deviation of 0.0395. Assuming a
10% drop-out, the sample size increased to 40 per group. To account for the possibility of
enrollment of siblings in the study, an additional 5 participants were added to adjust for the small
intraclass correlation that these siblings may create in the outcomes. This results in a final
sample size of 45 per treatment group and a total of 90 participants. Sample size calculations
were conducted using SAS 9.2 (Power and Sample Size Module, SAS Institute, Cary, NC).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eResults. Supplemental results
Treatment exposure and compliance
73 (81.1%) participants completed 12 months on study without prematurely stopping study
medication, with 38 (86.4%) in the Placebo arm and 35 (76.1%) in the VPA arm. Seventeen
(18.9%) participants stopped the study drug early (6 in the Placebo arm and 11 in the VPA arm).
The average daily dose, either placebo or drug, taken by participants was higher in the Placebo
arm, with a mean of 655.0 mg compared with 603.8 mg in the VPA arm. The mean ‘treatment
exposure’ in the Placebo arm was about 8% higher than the VPA arm, 89.7% versus 81.3%, but
the mean compliance rate was the about same in both treatment arms (94.2% in the Placebo
arm versus 94.7% in the VPA arm). Of the 89 participants with available drug accountability
data (1 participant did not return for any post-baseline visits), 61 (68.5%) had greater than or
equal to 90% treatment exposure and greater than or equal to 90% compliance.
Safety Assessments
In total, there were 364 treatment emergent adverse events reported, with 157 events in the
placebo arm and 207 events in the VPA arm. In the VPA arm, 97.8% of participants
experienced at least one AE, with 93.2% in the Placebo arm. Most events were of mild (69.0%)
or moderate severity (25.0%), but there were 12 severe events (5.8%) reported in the VPA arm
and 9 (5.7%) severe events reported in the Placebo arm. The single death due to a motor
vehicle accident reported in the VPA arm was not considered related to the use of VPA. Forty
events (25.5%) reported in the Placebo arm and 97 events (46.9%) in the VPA arm were
considered related to the study product. Two events each in the Placebo arm and VPA arm
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
were considered related to study procedure. Supplemental eTable 8 provides a summary of
the treatment emergent AEs on a participant level by treatment arm based on MedDRA-coded
System Organ Class (SOC) and Preferred Term. The most frequently reported SOCs were
infections and infestations (44.4%), gastrointestinal disorders (40.0%) and eye disorders
(40.0%). Gastrointestinal events were reported more frequently in the VPA arm (52.2%)
compared to the Placebo arm (27.3%). Of the clinical chemistry parameters, the notable
treatment-emergent deviations were the findings of a clinically significant elevated blood
ammonia level in 7 participants in the VPA arm compared to 3 participants within the placebo
arm, as well as clinically significant elevations in liver function tests in 9 and 2 participants in the
VPA and placebo arms, respectively.
Best-corrected visual acuity was measured for each eye throughout the study as a safety
assessment. Baseline letter score was slightly less in the placebo group (mean letter score: 75
OD, 73 OS) as compared with the VPA group (mean letter score: 79 OD, 78 OS). There was no
change in visual acuity throughout the study in either group (mean change from baseline in
letter score ranged from -0.3 to 1.3 in the placebo arm and from -1.4 to 0.5 in the VPA arm) and
no safety issues affecting acuity were detected.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eFigure 1. VPA Black Box warning
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
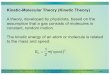
eFigure 2. Static perimetry test locations
The W164 grid has 164 test locations shown here as zeros from 55° nasally to 80° temporally.
Testing typically takes about 17 to 20 minutes per eye.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eFigure 3. Examples of visual fields
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 1. Major eligibility criteria
(A) Inclusion criteria
To be eligible for the study, participants must fulfill all of the following criteria:
1. Age 18 years, no upper age limit
2. Males and non-child bearing females must weigh ≥40 Kg and ≤158.9 Kg;
Females of child bearing potential must weigh ≥40 Kg and ≤74.9 Kg.
3. Diagnosis of Retinitis Pigmentosa (RP) including photoreceptor degeneration
established by visual field constriction, night blindness, marked reduction of
ERG responses, and the clinical signs of RP including waxy pallor of the optic
nerve, vascular attenuation and/or the presence of intraretinal pigment on
clinical examination.
4. Visual acuity of greater than or equal to 35 letters in at least one eye as
measured by the EVA-ETDRS (equivalent to 20/200 on a Snellen chart).
5. Autosomal dominant form of RP confirmed by genotyping. Participants with a
familial history of genotyped adRP may be randomized while awaiting
genotype confirmation.
6. Female participants of childbearing potential and male participants able to
father children must have (or have a partner who has) had a hysterectomy or
vasectomy, be completely abstinent from intercourse or must commit to
practice at least two acceptable methods of contraception to minimize the
chance of pregnancy during the study and for the 13-week period after
stopping the study drug. Acceptable methods of contraception include
hormonal contraception (i.e., birth control pills, injected hormones, dermal
patch or vaginal ring), intrauterine device, barrier methods (diaphragm,
condom) with spermicide, or surgical sterilization (tubal ligation).
7. Female participants of childbearing potential must have a negative urine
pregnancy test at study entry and throughout the duration of the study.
(B) Exclusion Criteria
Potential participants meeting any of the following criteria will be excluded from the
study:
1. Medical problems that make consistent follow-up over the treatment period
unlikely (e.g. stroke, severe MI, end stage malignancy), or in general a poor
medical risk because of other systemic diseases or active uncontrolled
infections.
2. Other retinal diseases: Glaucoma, retinal inflammatory disease (CME is
allowable), cataract worse than +2 NS, or herpes simplex virus of the eye.
3. Intact visual field of 5⁰ or less.
4. Participant unable to provide reliable perimetry measurements in both eyes for
both static and kinetic visual field, as determined by the Reading Center.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
5. Diabetes.
6. History of cancer (other than non-melanoma skin cancer) diagnosed, or
requiring treatment within the past 2 years.
7. A hemoglobin concentration, a platelet count or an absolute neutrophil count
below the lower limit of normal at study entry. The limits of normal are defined
by each site and are agreed to by the medical monitor.
8. Suspected liver dysfunction determined by having alanine aminotransferase
(ALT), aspartate aminotransferase (AST) and bilirubin values elevated above
the upper limit of normal.
9. History of pancreatitis by clinical features and/or laboratory abnormalities in the
last 12 months.
10. Renal dysfunction based on serum creatinine using the Modification of Diet in
Renal Disease (MDRD) equation.
11. Urea cycle disorders.
12. History of neurological conditions including epilepsy, history of brain injury,
encephalitis, or any organic brain syndrome.
13. History of schizophrenia, schizoaffective disorder, bipolar disorder, suicidality
or organic mental disorders.
14. Currently receiving valproic acid or other anti-convulsants.
15. Sensitive to or have ever had an allergic reaction to valproic acid.
16. Sensitive to or have ever had an allergic reaction to peanuts as peanut oil is an
inactive ingredient in valproic acid capsules and the placebo.
17. Has taken one of the following drugs at least 2 weeks prior to randomization as
these drugs are specifically known to interact with valproic acid: aspirin (daily
prophylactic use of ‘low-dose’ aspirin (≤81 mg) is not excluded), felbamate,
rifampin, amitriptyline/nortriptyline, carbamazepine, clonazepam, diazepam,
ethosuximide, lamotrigine, phenobarbital, primidone, phenytoin, tolbutamide,
topiramate, warfarin, or zidovudine.
18. Pregnant women.
19. Lactating mothers who are breast feeding their babies.
20. RP patients involved in other clinical trials within the last 3 months.
21. Require enrollment by consent of a legally authorized representative.
22. Persons who are unable to read are not allowed to consent for themselves or
others to participate in this study.
23. The potential participant lives in the same household as a current participant in
this protocol.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 2. Randomization and study completion
Treatment Arm
Placebo VPA Total
Number of Randomized Participants 44 46 90
Number of Study Completers (Week 65 Safety Visit) 42 (95.5%) 37 (80.4%) 79 (87.8%)
Number of Early Terminations 2 (4.5%) 9 (19.6%) 11 (12.2%)
Reasons for Early Termination
Death 0 (0%) 1 (11.1%) 1 (9.1%)
Lost to follow-up 1 (50.0%) 3 (33.3%) 4 (36.4%)
Participant request/refusal due to AE 1 (50.0%) 2 (22.2%) 3 (27.3%)
Participant request/refusal due to other reason 0 (0%) 3 (33.3%) 3 (27.3%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 3. Daily dosing schedule
Total Daily Dose (mg) Number of Capsules
Dose 1 Dose 2 Dose 3
250 1 0 0
500 1 1 0
750 1 1 1
1000 1 1 2
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 4. Dosage weight by schedule
Pounds (lbs) Kilograms (Kg)
Gender /
Child bearing
Potential
Total Daily Dose
(mg)
< 87.9 < 39.9 Males and Females Not eligible for study *
88 – 164.9 40 – 74.9 Males and Females 500
165+ 75+ Females of
childbearing potential
Not eligible for study *
165 – 197.9 75 – 89.9 Males / non
childbearing females
750
198 – 349.9 90 – 158.9 Males / non
childbearing females
1000
≥ 350 ≥ 159 Males / non
childbearing females
Not eligible for study *
* Males and non-childbearing females must be ≥ 88 lbs and ≤ 349.9 lbs and females of
childbearing potential must be ≥ 88 lbs and ≤ 164.9 lbs on day of randomization in order to be
eligible for enrollment into the study. If a participant who originally met the weight criteria at time
of enrollment falls outside of these weight criteria during the course of the trial, clinical judgment
will be used to determine whether the participant may continue in the study.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 5. Screen failures
Total
Number of Screen Failures 101
Reasons for Screen Failure*
Participant withdrew 18 (17.8%)
Unreliable visual field test 2 (2.0%)
Visual field results 4 (4.0%)
Medical/ocular history 7 (6.9%)
Laboratory test values out-of-range 13 (12.9%)
Weight out-of-range 6 (5.9%)
Not genetically characterized as autosomal dominant RP 34 (33.7%)
Prohibited medication 2 (2.0%)
Participant is pregnant 2 (2.0%)
Did not complete screening within 12 week window 29 (28.7%)
Other 1 (1.0%)
* Percentages are calculated based on the denominator of number of screen failures. The sum
of the percentages over the categories may exceed 100% if one or more participants failed
multiple eligibility criteria.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 6. Summary of genetic mutations by treatment arm
Treatment Arm
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Gene(s) with adRP
Mutation
RHO 22 (50.0%) 19 (41.3%) 41 (45.6%)
PRPF311 5 (11.4%) 9 (19.6%) 14 (15.6%)
RP1 4 (9.1%) 9 (19.6%) 13 (14.4%)
PRPF8 3 (6.8%) 1 (2.2%) 4 (4.4%)
PRPH2 2 (4.5%) 2 (4.3%) 4 (4.4%)
NR2E3 0 (0%) 2 (4.3%) 2 (2.2%)
PRPF3 2 (4.5%) 0 (0%) 2 (2.2%)
RHO and PRPH2 2 (4.5%) 0 (0%) 2 (2.2%)
SNRNP200/ASCC3L1 2 (4.5%) 0 (0%) 2 (2.2%)
TOPORS 0 (0%) 2 (4.3%) 2 (2.2%)
IMPDH1 1 (2.3%) 0 (0%) 1 (1.1%)
KLHL7 1 (2.3%) 0 (0%) 1 (1.1%)
NR2E3 and TOPORS 0 (0%) 1 (2.2%) 1 (1.1%)
RHO and ROM1 0 (0%) 1 (2.2%) 1 (1.1%)
1 Two participants have two distinct PRPF31 mutations
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 7. Mean (SD) of visual field area by treatment arm at baseline
Placebo (N=44) VPA (N=46)
Mean (SD) OD OS OD OS
I4e Isopter (deg2) 929.1 (2014.59) 897.9 (1831.33) 1329.8 (2185.52) 1307.4 (2080.34)
III4e Isopter (deg2) 2823.8 (3741.81) 2804.8 (3635.20) 4519.9 (4488.80) 4353.5 (4372.51)
V4e Isopter (deg2) 4416.5 (4658.61) 4444.1 (4670.95) 6423.8 (4980.95) 6370.1 (4934.57)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
eTable 8. Adverse events by treatment arm
Treatment Arm
System Organ Class/
Preferred Term (MedDRA v19.0)
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Infections and infestations 24 (54.5%) 16 (34.8%) 40 (44.4%)
Nasopharyngitis 9 (20.5%) 3 (6.5%) 12 (13.3%)
Sinusitis 3 (6.8%) 7 (15.2%) 10 (11.1%)
Influenza 7 (15.9%) 1 (2.2%) 8 (8.9%)
Bronchitis 0 (0.0%) 3 (6.5%) 3 (3.3%)
Gastroenteritis viral 1 (2.3%) 1 (2.2%) 2 (2.2%)
Urinary tract infection 2 (4.5%) 0 (0.0%) 2 (2.2%)
Upper respiratory tract infection 1 (2.3%) 1 (2.2%) 2 (2.2%)
Tooth abscess 1 (2.3%) 1 (2.2%) 2 (2.2%)
Hordeolum 0 (0.0%) 1 (2.2%) 1 (1.1%)
Herpes zoster 1 (2.3%) 0 (0.0%) 1 (1.1%)
Fungal skin infection 0 (0.0%) 1 (2.2%) 1 (1.1%)
Eye infection 0 (0.0%) 1 (2.2%) 1 (1.1%)
Diarrhea infectious 0 (0.0%) 1 (2.2%) 1 (1.1%)
Conjunctivitis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Vulvovaginal candidiasis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Chronic sinusitis 1 (2.3%) 0 (0.0%) 1 (1.1%)
Tooth infection 1 (2.3%) 0 (0.0%) 1 (1.1%)
Staphylococcal skin infection 1 (2.3%) 0 (0.0%) 1 (1.1%)
Respiratory tract infection bacterial 1 (2.3%) 0 (0.0%) 1 (1.1%)
Pharyngitis streptococcal 1 (2.3%) 0 (0.0%) 1 (1.1%)
Oral herpes 1 (2.3%) 0 (0.0%) 1 (1.1%)
Nail infection 1 (2.3%) 0 (0.0%) 1 (1.1%)
Impetigo 0 (0.0%) 1 (2.2%) 1 (1.1%)
Gastrointestinal disorders 12 (27.3%) 24 (52.2%) 36 (40.0%)
Nausea 3 (6.8%) 8 (17.4%) 11 (12.2%)
Dyspepsia 0 (0.0%) 8 (17.4%) 8 (8.9%)
Diarrhea 1 (2.3%) 4 (8.7%) 5 (5.6%)
Abdominal pain upper 2 (4.5%) 3 (6.5%) 5 (5.6%)
Gastroesophageal reflux disease 0 (0.0%) 3 (6.5%) 3 (3.3%)
Flatulence 0 (0.0%) 2 (4.3%) 2 (2.2%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
Treatment Arm
System Organ Class/
Preferred Term (MedDRA v19.0)
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Dry mouth 2 (4.5%) 0 (0.0%) 2 (2.2%)
Constipation 1 (2.3%) 1 (2.2%) 2 (2.2%)
Diverticulum 0 (0.0%) 1 (2.2%) 1 (1.1%)
Abdominal pain 0 (0.0%) 1 (2.2%) 1 (1.1%)
Impaired gastric emptying 1 (2.3%) 0 (0.0%) 1 (1.1%)
Hemorrhoids 1 (2.3%) 0 (0.0%) 1 (1.1%)
Gastritis 1 (2.3%) 0 (0.0%) 1 (1.1%)
Frequent bowel movements 1 (2.3%) 0 (0.0%) 1 (1.1%)
Abdominal discomfort 0 (0.0%) 1 (2.2%) 1 (1.1%)
Food poisoning 0 (0.0%) 1 (2.2%) 1 (1.1%)
Eye disorders 17 (38.6%) 19 (41.3%) 36 (40.0%)
Vision blurred 5 (11.4%) 3 (6.5%) 8 (8.9%)
Vitreous floaters 2 (4.5%) 2 (4.3%) 4 (4.4%)
Cystoid macular edema 1 (2.3%) 3 (6.5%) 4 (4.4%)
Visual impairment 1 (2.3%) 2 (4.3%) 3 (3.3%)
Vitreous detachment 2 (4.5%) 0 (0.0%) 2 (2.2%)
Visual acuity reduced 0 (0.0%) 2 (4.3%) 2 (2.2%)
Posterior capsule opacification 2 (4.5%) 0 (0.0%) 2 (2.2%)
Photopsia 2 (4.5%) 0 (0.0%) 2 (2.2%)
Photophobia 1 (2.3%) 1 (2.2%) 2 (2.2%)
Macular fibrosis 1 (2.3%) 1 (2.2%) 2 (2.2%)
Conjunctival edema 0 (0.0%) 1 (2.2%) 1 (1.1%)
Conjunctival haemorrhagia 1 (2.3%) 0 (0.0%) 1 (1.1%)
Choroidal neovascularization 1 (2.3%) 0 (0.0%) 1 (1.1%)
Cataract subcapsular 1 (2.3%) 0 (0.0%) 1 (1.1%)
Cataract nuclear 1 (2.3%) 0 (0.0%) 1 (1.1%)
Blepharitis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Asthenopia 1 (2.3%) 0 (0.0%) 1 (1.1%)
Uveitis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Ulcerative keratitis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Retinal haemorrhagia 1 (2.3%) 0 (0.0%) 1 (1.1%)
Retinal exudates 0 (0.0%) 1 (2.2%) 1 (1.1%)
Metamorphopsia 1 (2.3%) 0 (0.0%) 1 (1.1%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
Treatment Arm
System Organ Class/
Preferred Term (MedDRA v19.0)
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Macular edema 1 (2.3%) 0 (0.0%) 1 (1.1%)
Altered visual depth perception 0 (0.0%) 1 (2.2%) 1 (1.1%)
Lens dislocation 1 (2.3%) 0 (0.0%) 1 (1.1%)
Iridocyclitis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Halo vision 1 (2.3%) 0 (0.0%) 1 (1.1%)
Eyelid edema 1 (2.3%) 0 (0.0%) 1 (1.1%)
Eye swelling 0 (0.0%) 1 (2.2%) 1 (1.1%)
Eye disorder 0 (0.0%) 1 (2.2%) 1 (1.1%)
Episcleritis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Diplopia 0 (0.0%) 1 (2.2%) 1 (1.1%)
Corneal irritation 1 (2.3%) 0 (0.0%) 1 (1.1%)
Accommodation disorder 0 (0.0%) 1 (2.2%) 1 (1.1%)
Conjunctivitis allergic 0 (0.0%) 1 (2.2%) 1 (1.1%)
Investigations 8 (18.2%) 22 (47.8%) 30 (33.3%)
Ammonia increased 1 (2.3%) 7 (15.2%) 8 (8.9%)
Alanine aminotransferase increased 2 (4.5%) 3 (6.5%) 5 (5.6%)
Aspartate aminotransferase increased 1 (2.3%) 3 (6.5%) 4 (4.4%)
Weight increased 0 (0.0%) 4 (8.7%) 4 (4.4%)
Hepatic enzyme increased 0 (0.0%) 3 (6.5%) 3 (3.3%)
Ammonia abnormal 2 (4.5%) 0 (0.0%) 2 (2.2%)
Prostatic specific antigen increased 0 (0.0%) 2 (4.3%) 2 (2.2%)
Lipase increased 1 (2.3%) 1 (2.2%) 2 (2.2%)
Blood glucose increased 0 (0.0%) 1 (2.2%) 1 (1.1%)
Blood glucose abnormal 0 (0.0%) 1 (2.2%) 1 (1.1%)
Blood alkaline phosphatase increased 1 (2.3%) 0 (0.0%) 1 (1.1%)
Amylase increased 0 (0.0%) 1 (2.2%) 1 (1.1%)
Weight decreased 1 (2.3%) 0 (0.0%) 1 (1.1%)
Vitamin A increased 0 (0.0%) 1 (2.2%) 1 (1.1%)
Prothrombin time prolonged 0 (0.0%) 1 (2.2%) 1 (1.1%)
Platelet count decreased 0 (0.0%) 1 (2.2%) 1 (1.1%)
Pancreatic enzymes increased 0 (0.0%) 1 (2.2%) 1 (1.1%)
Liver function test increased 0 (0.0%) 1 (2.2%) 1 (1.1%)
Gamma-glutamyltransferase increased 1 (2.3%) 0 (0.0%) 1 (1.1%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
Treatment Arm
System Organ Class/
Preferred Term (MedDRA v19.0)
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Blood triglycerides increased 0 (0.0%) 1 (2.2%) 1 (1.1%)
Alanine aminotransferase abnormal 0 (0.0%) 1 (2.2%) 1 (1.1%)
Blood lactate dehydrogenase increased 1 (2.3%) 0 (0.0%) 1 (1.1%)
Nervous system disorders 9 (20.5%) 18 (39.1%) 27 (30.0%)
Headache 4 (9.1%) 8 (17.4%) 12 (13.3%)
Dizziness 3 (6.8%) 2 (4.3%) 5 (5.6%)
Tremor 0 (0.0%) 3 (6.5%) 3 (3.3%)
Sciatica 2 (4.5%) 1 (2.2%) 3 (3.3%)
Dysgeusia 1 (2.3%) 1 (2.2%) 2 (2.2%)
Visual field defect 0 (0.0%) 2 (4.3%) 2 (2.2%)
Syncope 1 (2.3%) 1 (2.2%) 2 (2.2%)
Aphasia 0 (0.0%) 2 (4.3%) 2 (2.2%)
Nerve compression 1 (2.3%) 0 (0.0%) 1 (1.1%)
Migraine with aura 1 (2.3%) 0 (0.0%) 1 (1.1%)
Migraine 0 (0.0%) 1 (2.2%) 1 (1.1%)
Lethargy 0 (0.0%) 1 (2.2%) 1 (1.1%)
Hypoesthesia 0 (0.0%) 1 (2.2%) 1 (1.1%)
Somnolence 0 (0.0%) 1 (2.2%) 1 (1.1%)
Paraesthesia 0 (0.0%) 1 (2.2%) 1 (1.1%)
Musculoskeletal and connective tissue disorders 8 (18.2%) 11 (23.9%) 19 (21.1%)
Muscle spasms 1 (2.3%) 2 (4.3%) 3 (3.3%)
Exostosis 2 (4.5%) 1 (2.2%) 3 (3.3%)
Back pain 2 (4.5%) 1 (2.2%) 3 (3.3%)
Arthritis 1 (2.3%) 1 (2.2%) 2 (2.2%)
Osteoarthritis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Musculoskeletal stiffness 0 (0.0%) 1 (2.2%) 1 (1.1%)
Musculoskeletal discomfort 1 (2.3%) 0 (0.0%) 1 (1.1%)
Intervertebral disc protrusion 1 (2.3%) 0 (0.0%) 1 (1.1%)
Bone pain 0 (0.0%) 1 (2.2%) 1 (1.1%)
Tendonitis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Temporomandibular joint syndrome 0 (0.0%) 1 (2.2%) 1 (1.1%)
Spinal osteoarthritis 1 (2.3%) 0 (0.0%) 1 (1.1%)
Osteopenia 0 (0.0%) 1 (2.2%) 1 (1.1%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
Treatment Arm
System Organ Class/
Preferred Term (MedDRA v19.0)
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Injury, poisoning and procedural complications 12 (27.3%) 4 (8.7%) 16 (17.8%)
Ligament sprain 2 (4.5%) 0 (0.0%) 2 (2.2%)
Laceration 1 (2.3%) 1 (2.2%) 2 (2.2%)
Skin abrasion 2 (4.5%) 0 (0.0%) 2 (2.2%)
Ligament injury 1 (2.3%) 0 (0.0%) 1 (1.1%)
Humerus fracture 1 (2.3%) 0 (0.0%) 1 (1.1%)
Foreign body 1 (2.3%) 0 (0.0%) 1 (1.1%)
Foot fracture 1 (2.3%) 0 (0.0%) 1 (1.1%)
Eye injury 0 (0.0%) 1 (2.2%) 1 (1.1%)
Epicondylitis 1 (2.3%) 0 (0.0%) 1 (1.1%)
Wound 1 (2.3%) 0 (0.0%) 1 (1.1%)
Road traffic accident 0 (0.0%) 1 (2.2%) 1 (1.1%)
Procedural nausea 0 (0.0%) 1 (2.2%) 1 (1.1%)
Post-traumatic neck syndrome 0 (0.0%) 1 (2.2%) 1 (1.1%)
Post procedural constipation 0 (0.0%) 1 (2.2%) 1 (1.1%)
Muscle strain 1 (2.3%) 0 (0.0%) 1 (1.1%)
Muscle injury 1 (2.3%) 0 (0.0%) 1 (1.1%)
Corneal abrasion 1 (2.3%) 0 (0.0%) 1 (1.1%)
Limb injury 1 (2.3%) 0 (0.0%) 1 (1.1%)
Respiratory, thoracic and mediastinal disorders 4 (9.1%) 6 (13.0%) 10 (11.1%)
Respiratory tract congestion 1 (2.3%) 1 (2.2%) 2 (2.2%)
Dyspnea 1 (2.3%) 1 (2.2%) 2 (2.2%)
Cough 1 (2.3%) 1 (2.2%) 2 (2.2%)
Upper respiratory tract congestion 0 (0.0%) 1 (2.2%) 1 (1.1%)
Rhinorrhea 0 (0.0%) 1 (2.2%) 1 (1.1%)
Paranasal sinus discomfort 0 (0.0%) 1 (2.2%) 1 (1.1%)
Epistaxis 1 (2.3%) 0 (0.0%) 1 (1.1%)
General disorders and administration site
conditions
3 (6.8%) 6 (13.0%) 9 (10.0%)
Fatigue 3 (6.8%) 6 (13.0%) 9 (10.0%)
Chest pain 1 (2.3%) 0 (0.0%) 1 (1.1%)
Skin and subcutaneous tissue disorders 4 (9.1%) 4 (8.7%) 8 (8.9%)
Rash 1 (2.3%) 2 (4.3%) 3 (3.3%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
Treatment Arm
System Organ Class/
Preferred Term (MedDRA v19.0)
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Alopecia 2 (4.5%) 0 (0.0%) 2 (2.2%)
Photosensitivity reaction 1 (2.3%) 0 (0.0%) 1 (1.1%)
Hair texture abnormal 0 (0.0%) 1 (2.2%) 1 (1.1%)
Dermatitis allergic 0 (0.0%) 1 (2.2%) 1 (1.1%)
Psychiatric disorders 2 (4.5%) 4 (8.7%) 6 (6.7%)
Depression 1 (2.3%) 1 (2.2%) 2 (2.2%)
Mental fatigue 0 (0.0%) 1 (2.2%) 1 (1.1%)
Libido increased 1 (2.3%) 0 (0.0%) 1 (1.1%)
Insomnia 0 (0.0%) 1 (2.2%) 1 (1.1%)
Emotional disorder 0 (0.0%) 1 (2.2%) 1 (1.1%)
Depressed mood 1 (2.3%) 0 (0.0%) 1 (1.1%)
Abnormal dreams 0 (0.0%) 1 (2.2%) 1 (1.1%)
Metabolism and nutrition disorders 4 (9.1%) 2 (4.3%) 6 (6.7%)
Decreased appetite 1 (2.3%) 1 (2.2%) 2 (2.2%)
Hyperlipidemia 0 (0.0%) 1 (2.2%) 1 (1.1%)
Hypercholesterolemia 1 (2.3%) 0 (0.0%) 1 (1.1%)
Fluid retention 1 (2.3%) 0 (0.0%) 1 (1.1%)
Dehydration 1 (2.3%) 0 (0.0%) 1 (1.1%)
Immune system disorders 1 (2.3%) 4 (8.7%) 5 (5.6%)
Seasonal allergy 0 (0.0%) 2 (4.3%) 2 (2.2%)
Hypersensitivity 1 (2.3%) 1 (2.2%) 2 (2.2%)
Immunodeficiency common variable 0 (0.0%) 1 (2.2%) 1 (1.1%)
Vascular disorders 1 (2.3%) 2 (4.3%) 3 (3.3%)
Hypertension 1 (2.3%) 2 (4.3%) 3 (3.3%)
Surgical and medical procedures 2 (4.5%) 1 (2.2%) 3 (3.3%)
Vasectomy 1 (2.3%) 0 (0.0%) 1 (1.1%)
Hernia repair 1 (2.3%) 0 (0.0%) 1 (1.1%)
Endodontic procedure 0 (0.0%) 1 (2.2%) 1 (1.1%)
Renal and urinary disorders 0 (0.0%) 3 (6.5%) 3 (3.3%)
Nephrolithiasis 0 (0.0%) 2 (4.3%) 2 (2.2%)
Urine abnormality 0 (0.0%) 1 (2.2%) 1 (1.1%)
Cardiac disorders 2 (4.5%) 1 (2.2%) 3 (3.3%)
Palpitations 1 (2.3%) 1 (2.2%) 2 (2.2%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021

© 2018 American Medical Association. All rights reserved.
Treatment Arm
System Organ Class/
Preferred Term (MedDRA v19.0)
Placebo
(N=44)
VPA
(N=46)
Total
(N=90)
Atrial fibrillation 1 (2.3%) 0 (0.0%) 1 (1.1%)
Hepatobiliary disorders 1 (2.3%) 1 (2.2%) 2 (2.2%)
Gallbladder pain 1 (2.3%) 0 (0.0%) 1 (1.1%)
Cholelithiasis 0 (0.0%) 1 (2.2%) 1 (1.1%)
Ear and labyrinth disorders 0 (0.0%) 2 (4.3%) 2 (2.2%)
Vertigo 0 (0.0%) 1 (2.2%) 1 (1.1%)
Deafness bilateral 0 (0.0%) 1 (2.2%) 1 (1.1%)
Endocrine disorders 0 (0.0%) 1 (2.2%) 1 (1.1%)
Hypothyroidism 0 (0.0%) 1 (2.2%) 1 (1.1%)
Reproductive system and breast disorders 1 (2.3%) 0 (0.0%) 1 (1.1%)
Prostatitis 1 (2.3%) 0 (0.0%) 1 (1.1%)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 04/14/2021