Embed Size (px)
Citation preview
All Rights Reserved, Duke Medicine 2011
Surgery versus stereotactic body radiation therapy in medically operable NSCLC
David H Harpole Jr, MD Professor of Surgery
Associate Professor in Pathology Vice Chief, Division of Surgical Services
Duke University School of Medicine Durham, North Carolina

90 year old female, 40 pack-year former smoker CAD with drug-eluting stents (clopidogrel bisulfate) 4 cm right upper lobe lung mass PET SUVmax 3.4, Otherwise (-) PFDs FEV1 75%; DLCO 70% ECOG 0-1

• • • •
–

All Rights Reserved, Duke Medicine 2011
Surgery versus stereotactic body radiation therapy in medically operable NSCLC
David H Harpole Jr, MD Professor of Surgery
Associate Professor in Pathology Vice Chief, Division of Surgical Services
Duke University School of Medicine Durham, North Carolina
All Rights Reserved, Duke Medicine 2011
Disclosure
No relevant conflicts of interest to disclose

All Rights Reserved, Duke Medicine 2011
Stereotactic Body Radiotherapy
• Multiple radiation beams focused on a single tumor
• Doses are usually 5-10 times traditional daily radiation doses

All Rights Reserved, Duke Medicine 2011
Stereotactic Radiosurgery
• Treated tumor control 85-95%
7

All Rights Reserved, Duke Medicine 2011
Study n Dose (Fractionation) Survival (year)
Local Failure (year)
Nagata (Japan) 45 48 Gy (12 Gy×4) 83%- T1 (5) 72%-T2 (5)
5%-T1 (5) 0%-T2 (5)
Bauman (Sweden) 57 45 Gy (15 Gy×3) 60% (3) 8% (3)
Fakiris (Indiana) 70 60-66 Gy(20–22 Gy×3) 43% (3) 12% (3)
Ricardi (Italy) 62 45 Gy (15 Gy×3) 57% (3) 12 (3)
Bral (Belgium) 40 60 Gy (20 Gy×3)* 60 Gy (15 Gy×4)†
52% (2) 16% (2)
Hoyer (Denmark) 40 45 Gy (15 Gy×3) 47% (2) 15% (2)
Timmerman (RTOG) 55 54 Gy (18 Gy×3)º 56% (3) 2% (3)
SBRT for early stage NSCLC: Retrospective Single Institution Series

All Rights Reserved, Duke Medicine 2011
SBRT Toxicity: SBRT for early stage NSCLC: Pulmonary Toxicity
9 Bongers E et al. Radiotherapy and Oncology 2013;109:95-99

All Rights Reserved, Duke Medicine 2011
SBRT Toxicity:Centrally Located Tumors
• Grade 5=6 – PNA x 4 – Pericardial effusion – Hemoptysis
• Grade 3-4: – Decline in PFTs – Pleural Effusion – Apnea – PNA – Skin reaction
Timmerman R et al. JCO 2006;24:4833-4839

All Rights Reserved, Duke Medicine 2011 Timmerman R et al. JCO 2006;24:4833-4839
©2006 by American Society of Clinical Oncology
SBRT Toxicity: Centrally Located Tumors

All Rights Reserved, Duke Medicine 2011
Primary Endpoint: 1 year rate of > Grade 3 definitely, possibly, or probably treatment related toxicity Secondary: 1 year primary tumor control rate, 1 year OS and DFS, FDG PET changes
Correlative biomarker for toxicity and control
SBRT: What is the Optimal Dose Schema? RTOG 0915: Randomized Phase II

All Rights Reserved, Duke Medicine 2011 Grills I S et al. JCO 2010;28:928-935
©2010 by American Society of Clinical Oncology
Surgical Resection vs SBRT for High Risk Operable Early Stage NSCLC

All Rights Reserved, Duke Medicine 2011 Grills I S et al. JCO 2010;28:928-935
©2010 by American Society of Clinical Oncology
Surgical Resection vs SBRT for High Risk Operable Early Stage NSCLC
All Rights Reserved, Duke Medicine 2011
• JCOG 0403: – 3 year PFS: 55% – 3 year OS: 76%
• RTOG 0618: – Accrual completed – Data maturing
15
SBRT for Medically Operable Early Stage NSCLC
All Rights Reserved, Duke Medicine 2011
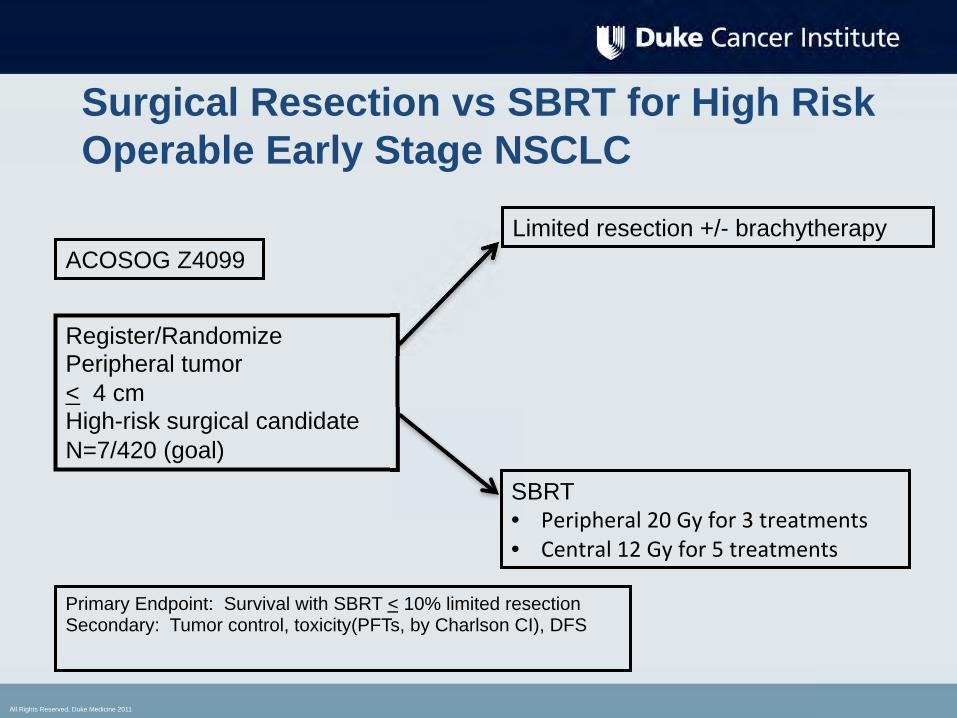
Surgical Resection vs SBRT for High Risk Operable Early Stage NSCLC
Register/Randomize Peripheral tumor < 4 cm High-risk surgical candidate N=7/420 (goal)
Limited resection +/- brachytherapy
SBRT • •
ACOSOG Z4099
Primary Endpoint: Survival with SBRT < 10% limited resection Secondary: Tumor control, toxicity(PFTs, by Charlson CI), DFS

All Rights Reserved, Duke Medicine 2011
Surgical Resection vs SBRT for Operable Early Stage NSCLC: ROSEL
SBRT 18 Gy x 3
Primary Endpoint: Local and Regional Control, Treatment Costs, QOL Secondary:Total Costs, Quality Adjusted Life Years, Overall Survival

All Rights Reserved, Duke Medicine 2011
Surgical Resection vs SBRT for Operable Early Stage NSCLC: VALOR
SBRT: BED > 100 Central 5-8 doses
Primary Endpoint: 5 year OS • 25 Federal hospitals • Resources being allocated at end of 2014

All Rights Reserved, Duke Medicine 2011
Ablative Radiotherapy (SBRT) • Ablative Radiotherapy results in high rates of treated
tumor control and survival • Toxicity profile varies between central and peripheral
tumor locations • Randomized comparisons ongoing:
– Surgery: • High risk operable patients • Medically operable patients
– Conventional Radiotherapy • Patterns of Progression have changed
– Distant progression most common
19

• – – – – – –

• –
• • •





























