-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
1/13
Selected
InstructionalCourse Lectures
The American Academy of Orthopaedic Surgeons
PAU L TORNETTA II I
EDITOR , VOL. 61
COMMITTEE
PAU L TORNETTA II ICHAIR
K ENNETH A. EGOL
MARY I. O’CONNOR
MARK PAGNANO
R OBERT A. HART
EX -O FFICIO
DEMPSEY S. SPRINGFIELDDEPUTY EDITOR OF THE
JOURNAL OF BONE AND JOINT SURGERY
FOR INSTRUCTIONAL COURSE LECTURES
Printed with permission of the American Academy
of Orthopaedic Surgeons. This article, as well as other
lectures
presented at the Academy’s Annual Meeting, will be
available in February 2012 in Instructional Course
Lectures, Volume 61.The complete volume can be ordered online
at www.aaos.org,or by calling 800-626-6726 (8 A
. M .-5 P . M ., Central time).
1547
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
2/13
Surgical Techniques for Complex Proximal Tibial
Fractures
Jason A. Lowe, MD, Nirmal Tejwani, MD, Brad Yoo, MD, and Philip
Wolinsky, MD
An Instructional Course Lecture, American Academy of
Orthopaedic Surgeons
Traditional and Alternative Surgical
Approaches to the Tibial Plateau:
How to Select Them?
Any surgical approach for fracture fix-ation should facilitate
visualization of fracture fragments and allow the appli-cation
of optimal fixation devices andsoft-tissue repair. Treatment goals
ap-plied to tibial plateau fractures includeanatomic articular
surface reduction,restoration of the anatomic axis, andpreservation
of the menisci. The ap-
proach should not devitalize soft tissuesor cause further injury
to surrounding structures. An ideal surgical
dissectionencompasses these principles and per-mits early joint
motion.
The midline longitudinal incisionis the favored approach to the
knee joint,as this incision facilitates knee replace-ment if needed
in the future. Surgicalexposure for complex injuries (bicon-dylar
fractures) requiring dual fixationneeds large medial and lateral
flaps thatadd to soft-tissue complications. Other
surgical approaches allowing a moredirect approach to the
fracture to de-crease the risk of soft-tissue injury from
excessive retraction or periosteal strip-ping are available.
When one incisiondoes not adequately expose the fracture,it is
better to use a dual incision than asingle midline exposure1-3.
Anterolateral ApproachThe anterolateral approach is used
forthe most commonly seen tibial plateaufractures (Schatzker4 types
I, II, andIII). It is also used for the lateral part of a dual
incision approach needed for
internal fixation of a bicolumnar frac-ture. The incision is
centered onGerdy’s tubercle and is shaped as alazy S or a hockey
stick. The fascia iselevated off the tibial tubercle to exposethe
lateral tibial plateau. The kneecapsule is incised, and a
submeniscalarthrotomy allows visualization of thearticular surface
(Figs. 1 and 2). Inaddition to visualization of the
articularsurface, this approach allows repair of any meniscal
tears.
Medial ApproachThe medial approach is used for amedial
tibial plateau fracture (Schatzker
type IV) or as part of a dual approach tothe plateau. The
incision parallels theposteromedial border of the proximalpart of
the tibia. The pes anserinus iselevated, the fracture reduced,
andfixation implants are placed beneaththe pes anserinus. The pes
anserinusmay either be retracted (Fig. 3) orincised, with repair
after fracture fixa-tion. The medial meniscus cannot beelevated as
is possible with the lateralmeniscus; therefore, the limitation
of
this approach is the limited visualiza-tion of the articular
surface of themedial plateau. Also, access to the pos-terior
plateau is limited, but the medialapproach can be converted to a
postero-medial approach.
Anterior Approach with Tibial
Tubercle Osteotomy The advantage of the anterior
approachwith osteotomy of the tibial tubercle isthat the tibial
plateau and the intercon-dylar notch are completely exposed,
allowing reattachment or primary su-ture of the cruciate
ligaments5. Thisapproach is rarely used, and most
Disclosure: None of theauthors received paymentsor services,
eitherdirectlyor indirectly (i.e., via hisor herinstitution), froma
third party in support of any
aspect of this work. One or more of the authors, or his or her
institution, has had a financial relationship, in the thirty-six
months prior to submission of this
work, with an entity in thebiomedical arena that could be
perceivedto influence or have thepotential to influence what is
writtenin this work. No authorhas
had any other relationships, or has engaged in any other
activities, that could be perceived to influence or have the
potential to influence what is written in
this work. The complete Disclosures of Potential Conflicts
of Interest submitted by authors are always provided with the
online version of the article.
J Bone Joint Surg Am. 2011;93:1548-59
1548
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L F R A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
3/13
complex, bicondylar fractures are now treated with use of
dual incisions.
Posteromedial ApproachMedial tibial plateau fractures extend-ing
to the posterior aspect of the tibialplateau, posterior metaphyseal
frac-tures, or those that require a buttresson the posteromedial
cortex are bestfixed with use of the posteromedialapproach.
Fragment-specific fixation
of the medial plateau is recommendedover stabilization with a
laterally basedlocking construct6. To obtain optimal
fixation of bicondylar fractures, a dualplating technique is
recommended,with one plate fixing the medial frag-ment and one
fixing the lateral plateau.Medial plateau fractures may be me-dial
or posteromedial, with each re-quiring a plate to be, ideally,
placed atthe apex of the fracture (fragment-specific).
The patient can be positionedprone or supine7. An incision is
made
over the posteromedial aspect of theknee (Fig. 4). Dissection
between themedial head of the gastrocnemius mus-
cle and the semitendinosus muscleallows exposure of the
semimembra-nosus muscle, which is detached forbetter access to the
posterior aspect of the tibia. Visualization of the
articularsurface is limited, but, if necessary,visualization can be
improved with alongitudinal split in the medial collat-eral
ligament and capsule. Through thisincision, visualization of the
articularcartilage can aid in congruent jointreduction.
Posterior ApproachAn isolated posterior shear fracture,
aposterior cruciate ligament avulsionfracture with a large osseous
fragment,or a posterior fracture dislocation is best
exposed with a posterior approach8,9. A z-shaped incision
across the flexorcrease is used. The deep tissue planes arebetween
the medial head of the gas-trocnemius and the
semimembranosusmuscles or between the two heads of thegastrocnemius
muscle with protectionof the neurovascular structures. Themedial or
lateral head of the gastrocne-mius muscle may be partially
detached,if it is necessary to improve exposure,enable fracture
reduction, or insertfixation on the posterior rim.
Extended Lateral Approach withFibular Osteotomy The
Lobenhoffer approach is used toexpose fractures of the lateral
tibialplateau that extend posteriorly when thehead of the fibula
limits the exposure10,11.
The skin incision is made along the course of the peroneal
nerve, pos-terior to the fibular head. After dissec-tion, the
common peroneal nerve isprotected and an osteotomy of the fibulaat
the junction of the head and neck is
performed, leaving the proximal at-tachments intact. This allows
exposureof the tibial plateau from anterior toposterior.
Another way to approach theposterolateral plateau is without a
fibu-lar osteotomy 10. Absence of an osteot-omy makes it more
difficult to visualizethe tibial fracture at the level of
thefibular head; however, this approachis preferred as it avoids
the risk of anonunion at the fibular osteotomy site.
Fig. 1
Clinical photograph of a patient’sright knee withthelazy-S
incision used forinternalfixationof a lateral
proximal tibial fracture.
Fig. 2
Clinical photograph of a patient’s right knee with retention
sutures in the lateral meniscus (white
arrow) of a submeniscal arthrotomy.
1549
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
4/13
Medial Tibial Plateau ReductionA shearing force produces a
coronalplane fracture comprising approxi-mately 25% of the medial
articularsurface12. This fragment is seen on alateral radiograph,
but the full extent of articular involvement is best
appreci-ated on sagittal computed tomography (CT) images.
Since the medial collat-
eral ligament (MCL) prevents a sub-meniscal arthrotomy,
reduction of themedial joint line is often obtainedindirectly with
anatomic restoration of the medial cortex. If there is a
questionabout the accuracy of the reduction of the articular
surface of the medialplateau, a longitudinal incision is madein the
MCL, where the fracture enters
the medial aspect of the joint. Ana-tomic reduction is confirmed
by aligning the articular cartilage of eachfragment while the
cortex is reducedwith a well-placed Weber clamp per-pendicular to
the fracture. This white-white read of the medial plateauarticular
cartilage augments accuracy of reduction.
Medial Plateau FixationSurgical stabilization of isolated
me-dial plateau fractures (Schatzker typeIV) is accomplished with
an under-contoured, nonlocking, flexible plate(1/3 T-plate or
reconstruction plate)applied as a buttress. Fixation of themedial
plateau in Schatzker type-V and
VI fractures is more controversial.Stabilization can be
accomplished withlocking screws placed through a later-ally based
implant alone or stabilizedwith a medial plate as part of a
dualplating construct (medial and lateralplate)13-17. Biomechanical
and clinicaldata support both techniques. Al-though lateral-only
locked plates re-duce surgical time, blood loss, andlimit
soft-tissue stripping, a high rateof articular subsistence (26%)
has beenreported13-17. Displacement of the me-
dial fragment can result in knee in-stability, pain, and
posttraumaticosteoarthritis12. The authors, there-fore, recommend
fragment-specificfixation of the posteromedial and lat-eral plateau
through a two-incisionapproach for bicondylar tibial
plateaufractures. Fragment-specific fixation of the medial
plateau avoids inadequatepurchase of the posteromedial frag-ment
observed with lateral-only lock-ing screws6,16-18. The benefit of
addedfracture stability is offset by g reater
surgical time and higher postoperativeinfection rates. Current
reports havedemonstrated postoperative infectionrates of 8.4% with
dual plating com-pared with 1.6% with
lateral-only fixation13,14. In the absence of a pro-spective,
randomized, controlled trialcomparing these surgical approaches,the
need for anatomic reduction of the joint surface and adequate
stabiliza-tion of the medial plateau takesprecedence.
Fig. 3Clinical photograph of a patient’s left knee with a medial
incision (patient’s head is to the left). The
tendons of the pes anserinus (white arrow) are seen over the
clamp.
Fig. 4
Clinical photograph of a patient’s right knee. With the patient
in the prone position, the solid line
identifiesthe level of thekneejointwith thefemurto theleft.The
dashedline illustrates an incision for
a posterior-medial incision.
1550
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
5/13
Lateral Plateau Articular ReductionHigh-energy bicondylar tibial
fracturesare typically associated with articularsurface impaction
of the lateral plateau.Successful restoration of the lateralaspect
of the joint requires adequatevisualization and an array of
reduction
techniques. A submeniscal arthrotomy and a laterally based
femoral distractorimprove visualization of the articularsurface
when needed. A single Schanzpin is placed into the femoral
meta-physis, parallel to the joint line, and asecond Schanz pin is
placed in the tibia,distal to planned plate placement lo-cation19.
Care must be used withplacement of a lateral tibial pin so as tonot
injure the neurovascular struc-tures of the anterior
compartment20.Applying distraction opens the joint
and enhances visualization of the lat-eral plateau. Retraction
of the postero-lateral or anterolateral fragments(opening the door)
can allow evenmore v isualization.
Mobile articular pieces are re-duced with a dental pick or a
small (0.45to 0.62-mm) wire and are temporarily stabilized
with Kirschner wires. Im-pacted articular fragments must
bemobilized from surrounding cancellousbone before they can be
reduced. A 1/4
to 1/2 in (0.64 to 1.3-cm) osteotomeor bone tamp is used to
elevate 1.0 to1.5 cm of cancellous bone with the ar-ticular
segment. Once levered into po-sition, the fragment is stabilized
withKirschner wires. With the impactedsegment reduced and secured
with wirefixation, bone voids can be filled withgraft material and
the lateral segmentcan be reduced (closing the door). Themedial and
lateral plateaus can be re-duced and compressed with a
periartic-ular reduction clamp19.
The contained defect of a puredepression fracture cannot be
reducedwithout an osteotomy. If there is anincomplete fracture, the
articular seg-ment is accessed by completing the
fracture and reducing the articularfragment as described above.
If there isno cortical fracture, articular reductionis done with
one of two techniques. The
Fig. 5
Clinical intraoperative photograph of a patient’s left knee,
demonstrating incisions for minimally
invasive plate osteosynthesis.
Fig. 6
Anteroposterior radiograph of a knee
illustrating the inability of locking
screws to reduce the valgus malalign-
mentin the coronal plane. Asa result, a
valgus malunion, with the plate poorly
apposed to the tibia, is observed.
1551
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
6/13
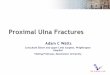
Fig. 7
Fig. 8
Fig. 7 Anteroposterior and lateral
radiographs of an extra-articular
proximal tibial fracture demon-
strating the most common defor-
mities (valgus and procurvatum)
observed in these fractures. Fig. 8
Anteroposterior radiographs
showing how a medial starting
site produces a valgus deformity
as the intramedullary device en-
ters the tibial diaphysis.
1552
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
7/13
anterior compartment is released fromthe metaphyseal flare for
both. Onetechnique is to use the DHS (DynamicHip Screw; Synthes,
Paoli, Pennsylvania)set and fluoroscopic visualization.
Theguidewire is directed from the lateraltibial metaphysis toward
the impactedsegment. The cortex is then opened withthe cannulated
11-mm reamer from theDHS system. Bone tamps are introducedand used
to tap the articular segmentinto place. The articular reduction
isconfirmed by direct visualizationthrough the submeniscal
arthrotomy.Alternatively, a lateral osteotomy ismade with drill
holes (2.0-mm drill-bit) in a diamond pattern, with thedrill holes
connected with use of a
0.25-in (0.64-cm) osteotome. Thearticular segment is reduced as
justdescribed. With either technique, thearticular fragments can be
supportedwith Kirschner wires and bone graftprior to definitive
fixation.
Lateral Plateau FixationSurgical stabilization of the
lateralplateau must maintain reduction andrigid fixation of the
articular segmentto a well-aligned tibial shaft. The jointsurface
is stabilized with multiple
parallel screws placed just beneaththe subchondral bone. These
rafting screws support the reduced articularsurface fragments
and can be the prox-imal screws of a 3.5-mm or a
4.5-mm,precontoured periarticular plate or withminifragment (2.4 or
2.7-mm) screws.Minifragment screws and plates arefavored for
articular comminutionwith fragments having minimal sub-chondral
bone or when the proximalscrews in the precontoured plate arenot
subchondral.
The articular segment is reducedto the shaft with traction (a
manual orfemoral distractor). First, the plate isfixed to the
proximal segment withbicortical screws (locked or
nonlocked)inserted parallel to the joint21. The plateis reduced to
the tibial shaft with abicortical screw or a so-called
whirlybirdpush-pull type of device. It is importantto ensure that
this does not malreducethe fracture in the coronal plane,
andlocking screws should not be placed in
the distal segment until the alignment iscorrect22.
Minimally Invasive Plate OsteosynthesisThe proximal
tibial anatomy and fracturepattern must be clearly understood
if precontoured plates are used with mini-mally invasive
techniques. The articularsurface is visualized with a small
arthrot-omy, and percutaneous techniques areused for screw
placement into the tibialshaft (Fig. 5). One must be careful
whenthis technique is used for plates longerthan eleven holes, as
the neurovascularbundles in the anterior and lateral com-partments
are at risk 12,23.
Locking ScrewsLocking screws increase construct ri-gidity, but
they should be placedbicortically 21,24. They are useful in
se-verely osteoporotic bone, substantialmetaphyseal-diaphyseal
comminution,
or short-segment periarticular and/orintra-articular fractures.
Malunion hasbeen a problem, and it is necessary topay meticulous
attention to fracturereduction before placement of
locking screws (Fig. 6)25.
Intramedullary Nailing of Proximal Tibial FracturesThe use
of an intramedullary nail forfracture stabilization is appealing.
Theinsertion point of an intramedullary nailis remote from the
fracture site, mini-mizing vascular disruption of the
fracturefragments, the implants are centrally located, and
tibial diaphyseal fractureshave a high rate of union and low rate
of complications. As a result, the use of
intramedullary nailing for tibial fractureshas expanded from
mid-shaft diaphysealfractures to proximal fractures26-32.
In-tramedullary nail fixation is technically more demanding
for proximal tibialfractures than for diaphyseal fractures.
Fig. 9
Lateral radiographs showing how an inferior starting site and
posterior nail trajectory produce a
procurvatum deformity of the proximal segment as the nail enters
the diaphysis.
1553
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
8/13
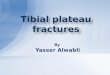
Fig. 10 Fig. 11
Fig. 12
Fig. 10 Anteroposterior radiograph demonstrating an
appropriate starting site, just medial to the lateral tibial
spineand inline with themechanicalaxis.Fig.11 Lateral
radiograph demonstrating a correctly selected starting
site and wire trajectory. The wire is just anterior to the
articularmargin anddirectedparallelto theanteriortibial
cortex. Fig. 12 Anteroposterior and lateral
radiographs
with a protection sleeve for a retropatellar tibial nail
centered at an appropriate starting site.
1554
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
9/13
Unlike intramedullary nailing of a di-aphyseal fracture,
placement of the in-tramedullary nail does not reduce aproximal
tibial fracture, and malreduc-tions of proximal tibial fractures
withintramedullary nail fixation are reportedto be as high as
84%27,33-36.
The typical deformity caused by intramedullary nailing of
proximal tibialfractures is valgus and apex anteriorangulation with
anterior translation of the proximal fragment (Fig. 7).
Thevalgus deformity is due to an imbalanceof muscle forces on the
proximal frag-ment and is accentuated when theinsertion point is
too medial or directedlaterally. The tip of the nail can abut
thelateral cortex causing the proximal
fragment to rotate into a valgus position(Fig. 8)34,35,37. The
apex anterior deformity results from a combination of the pull
of the patellar tendon34, a distal insertionsite, or a
posteriorly directed nail thatdeflects off the posterior tibial
cortex androtates the proximal fragment (Fig. 9).Nails with an
accentuated distal Herzog bend may translate the proximal
frag-ment anteriorly, described by Henley et al. as the wedge
effect38.
To prevent malalignment of proximal tibial fractures during
intra-
medullary nailing, one should properly place the starting
point; reduce thefracture prior to guidewire placement,reaming, and
nail insertion; and holdthe reduction until all of the
locking bolts have been inserted.
The Proper Starting Point Fluoroscopic imaging is used to
obtaingood anteroposterior and lateral C-armimages of the knee. The
starting pointon the anteroposterior radiograph is inline with the
medial border of the lateral
tibial spine (Fig. 10). The insertion siteon the lateral
radiograph is slightly anterior to the anterior margin of
thearticular surface. The guidewire and nailare inserted as
parallel to the anteriorcortex as possible (Fig. 11).
Fracture Reduction Techniques
Extended Leg PositionIt is critical to reduce the fracture
andmaintain the reduction during fracturefixation. The
intraoperative position of
the leg affects fracture reduction. Whenthe knee is maximally
flexed, whichfacilitates collinear insertion of the nail
with the anterior tibial cortex, the pull of the patellar
tendon increases the apex anterior deformity. When this
occurs, the
Fig. 13
Anteroposteriorand lateral radiographswith a proximal Schanz pin
for the AO distractor, appropriately
placed parallel to the articular surface (left) and posterior to
the nail path (right).
Fig. 14
Anteroposterior and lateral radiographs demonstrating an
appropriately placed distal Schanz pin
inserted parallel to the ankle joint and posterior to the nail
path.
1555
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
10/13
apex deformity can be limited by placing the
instrumentation in the leg withminimal knee flexion39. Originally,
semi-extended nailing was performed througha large medial
parapatellar incision;however, it can now be done with a
smallsuprapatellar incision. The instrumentsand nail are passed
through protectivesleeves, posterior to the patella to theproximal
part of the tibia (Fig. 12)16.Recent studies have suggested this
tech-nique can be used without injury to thepatella or femoral
articular cartilage, themenisci, or the anterior cruciate
liga-ment16,18,40. No outcomes data are avail-able for this
technique.
Use of a Femoral Distractor or an
External Fixation Frame A universal distractor or an
externalfixator can be used to obtain andmaintain fracture
reduction. With useof fluoroscopic imaging, a proximalSchanz pin is
inserted from the medialside of the proximal part of the
tibiaposterior to the planned intramedul-lary nail path (Fig. 13),
and a distalSchanz pin is placed medially in theposterior malleolus
(behind the nail) orat the level of the physeal scar (Fig. 14).The
pins should be inserted parallel
to the proximal and distal joint lines.Application of traction
through theframe until the pins are parallel typi-cally results in
adequate reduction34,41.
Temporary Plate FixationA small plate can be used as a
temporary reduction device29,42. The plate may beplaced on the
medial or lateral tibialborder, but the medial border is
bettersince the medial side of the fracture isoften less
comminuted. The medialincision is positioned posterior to the
posterior borders of the tibia so that if the incision
fails to heal, no bone will beexposed (Fig. 15). Minimal deep
dis-section is needed, and the plate is placedover intact
periosteum. Unicorticalscrews are used so the reamer and nailcan
pass. After insertion of the nail andall interlocking screws, the
plate may beremoved or the screws on the proximalside of the
fracture may be taken out.The plate then acts as a buttress
con-struct, preventing a deformity from
recurring while permitting relative mo-tion at the fracture
site.
Blocking ScrewsSo-called blocking or Poller screws canbe used
during intramedullary nailing of proximal tibial fractures.
They areplaced preemptively in an effort toprevent a deformity or
as a so-called
bailout after deformity has occurred.They are used to narrow the
canal, tocreate a path, or as an artificial cortex for the
nail to pass down28,33,43.
Blocking screws are inserted per-pendicular to the plane of the
deformity,on the concave side of the deformity,within the more
mobile fracture segment.For example, with a valgus deformity,
thescrew is placed from anterior to posterior,on the lateral side
of the instrument path,and in the proximal segment (Fig. 16).
The screw functions as a so-called artifi-cial cortex.
Blocking screws can also be usedfor an anterior malalignment.
Theblocking screw is placed slightly poste-rior to the midline,
from medial tolateral, in the proximal fragment (Fig.16). As a nail
is inserted, it contacts theblocking screw, extending the
proximal
fragment and decreasing the apex ante-rior deformity. The screw
should not beplaced in the midline since nail passagemay be blocked
by the screw.
Percutaneous ClampsThe orientation of a fracture line
may allow percutaneous placement of areduction clamp to obtain
and maintainthe reduction (Fig. 17). The use of clamps has not
been shown to increaseinfection rates44.
Fig. 15
Anteroposterior and lateral radiographs with a provisional
locking plate on the posteromedial tibial
cortex. Unicortical locking screws are used so as to not
obstruct insertion of reamers or the intra-
medullary implant.
1556
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
11/13
Implant SelectionIt is important to know the implants inorder to
ensure that at least two locking screws can be placed in the
proximalsegment. The distance from the end of the nail to the
locking bolts determineshow far proximal or distal fracture
linescan extend and still be stabilized by theintramedullary nail.
The number andorientation of the proximal and distalinterlocking
bolts vary by implant.Oblique bolts have demonstrated more
stability than transverse bolts in resist-ing coronal plane
deformity, but notaxial or torsional stability 38. The
com-bination of oblique and transverseinterlocking screws increases
constructstability 45,46. Intramedullary deviceswith a distal
Herzog bend may accen-tuate a sagittal plane deformity because,as
the Herzog bend contacts the pos-terior cortex, it can create a
so-calledwedge effect and translate the proximalsegment anteriorly
(Fig. 18)38.
Complications and Pitfalls
Knee pain, after intramedullary nailing of the tibia,
affects 60% to 70% of patients47-50. The anterior knee pain
isexacerbated by kneeling, squatting, stairclimbing, or
high-performance athleticactivities. Implant removal after
fractureunion has had inconsistent results withregard to relieving
anterior knee pain.There is no difference in the prevalenceof knee
pain when a transpatellar orparapatellar incision is used.
The prevalence of malunion hasbeen reported to be as high as
84%36.With use of the techniques described inthis article, malunion
rates have beenreduced to between 8% and 23%28,29,31.Strict
attention to surgical techniqueand the use of reduction aids
decreasethe prevalence of malreduction.
Infections and nonunions aremost commonly associated with
openand/or comminuted fractures29,31,36,42,51.Ultimate union rates
of 91% to 100%
have been reported, but the union ratefollowing primary fixation
is approxi-mately 77%28,29,36,42. Lindvall et al. re-ported a 100%
union rate for closedtibial fractures and a 23% rate of non-union
for open fractures stabilized withan intramedullary nail31.
Patient-specific contraindications tothe use of an
intramedullary nail includeopen physes, intramedullary canals
toonarrow to allow insertion of a nail, pre-existing canal
deformities, knee contrac-tures, and so-called blocking
hardwaresuch as an ipsilateral knee replacement orknee fusion.
Fracture-specific contraindi-cations to the use of an
intramedullary nailinclude substantial intra-articular
in-volvement, and short extra-articular seg-
ments that preclude placement of at leasttwo interlocking
screws6.
Nails Compared with Plates
A literature meta-analysis found a trendtoward an increased
prevalence of mal-union after intramedullary nailing compared
with plate and screw osteo-synthesis (p = 0.06), but a
lower infec-tion rate after intramedullary nailing (p <
0.05)52. Lindvall et al. also demon-strated a trend toward a higher
mal-union rate for intramedullary nailing
(p = 0.103), a threefold increased rate of hardware removal
after plate and screw fixation, and no difference in
implantfailure between these two techniques31.Both intramedullary
nails and plates canbe inserted with use of surgical tech-niques
that respect the local soft-tissuebiology. These techniques
optimizefracture-healing and contribute to ahigh rate of fracture
union for bothoperative procedures27,29,52,53.
Implant failure has been reportedfor both intramedullary nails
and
plates35,36,53. Early studies of intramedullary nails had
implant failure rates as high as25%, while only 2.6% of plates
failed36,53.Many early failures of intramedullary nailsinvolved
small-diameter locking bolts24.More recent literature has
demonstratedsimilar prevalences of implant failure
forintramedullary nails and plates2,28,31,34,54,55.
Overview
Extra-articular proximal tibial fractures aretechnically
demanding fractures to treat.
Fig. 16
Anteroposterior and lateral radiographsdemonstrating
properpositioning of blocking screwsto aid in
fracture reduction and strengthen the implant construct.
Anterior-posterior screws placed lateral to
the nail (whitelarge arrows) prevent valgusdeformation, and
medial-lateral screws placed posteriorto
the nail (white small arrows) prevent procurvatum.
1557
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
12/13
Fixation with an intramedullary nail re-quires a firm
understanding of the anat-omy of the proximal part of the tibia,
thefracture pattern, the deforming forces, andthe implant system.
The prevalence of malreduction can be reduced with use
of meticulous surgical technique, a correctnail insertion
site, and adjuvant reductionaids. The rates of postoperative
infectionand nonunion are related more to the
nature of the injury (open and com-minuted) than to the implant.
Patientsshould be educated on the occurrenceof postoperative
functional knee pain,
which seems to occur more commonly in younger, more active
patients.
Jason A. Lowe, MDUniversity of Alabama at Birmingham,510 20th
Street South, FOT 960,Birmingham, AL 35294
Nirmal Tejwani, MDNYU Orthopedic Surgery Associates,301 East
17th Street, Suite 1403,New York, NY 10003
Brad Yoo, MDPhilip Wolinsky, MDDepartment of Orthopaedic
Surgery,University of California Davis,4860 Y Street, Suite
1700,Sacramento, CA 95817
Printed with permission of the AmericanAcademy of Orthopaedic
Surgeons. This article,as well as other lectures presented at
theAcademy’s Annual Meeting, will be available
in February 2012 in Instructional CourseLectures, Volume 61. The
complete volumecan be ordered online at www.aaos.org, or
by calling 800-626-6726 (8 A.M.-5 P.M., Central
time).
References
1. Barei DP, Nork SE, Mills WJ, Coles CP, Henley
MB,Benirschke SK. Functional outcomes of severebicondylar tibial
plateau fractures treated with dualincisions and medial and lateral
plates. J Bone JointSurg Am. 2006;88:1713-21.
2. EgolKA, Tejwani NC,Capla EL,Wolinsky PL,Koval
KJ.Staged management of high-energy proximal tibia frac-
tures (OTA types 41): the results of a prospective,
stan-dardized protocol. J Orthop Trauma. 2005;19:448-56.
3. Georgiadis GM. Combined anterior and
posterior approaches for complex tibial plateau fractures.J
Bone Joint Surg Br. 1994;76:285-9.
4. Schatzker J, McBroom R, Bruce D. The tibialplateau
fracture. The Toronto experience 1968-
1975. Clin Orthop Relat Res. 1979;138:94-104.
5. Fernandez DL. Anterior approach to the knee
withosteotomy of the tibial tubercle for bicondylar
tibialfractures. J Bone Joint Surg Am. 1988;70:208-19.
6. Barei DP, O’Mara TJ, Taitsman LA, Dunbar RP,Nork SE.
Frequency and fracture morphology of the
Fig. 17 Fig. 18
Fig.17 Lateral intraoperative radiographwith a Weberclamp placed
percutaneouslyto holdthe reductionduring nailinsertion.Fig.18
Lateral intraoperative
radiograph with a well-positioned guidewire (parallel to the
anterior cortex) during reaming (left). Insertion of a nail with a
low Herzog bend (black arrow)
showing displacement of the proximal fragment as it contacts the
posterior cortex (right).
1558
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S
-
8/20/2019 Surgical Techniques for Complex Proximal Tibial
Fractures
13/13
posteromedial fragment in bicondylar tibial plateaufracture
patterns. J Orthop Trauma. 2008;22:176-82.
7. Weil YA, Gardner MJ, Boraiah S, Helfet DL, LorichDG.
Posteromedial supine approach for reduction andfixation of medial
and bicondylar tibial plateau frac-tures. J Orthop Trauma.
2008;22:357-62.
8. Fakler JK, Ryzewicz M, Hartshorn C, Morgan SJ,Stahel
PF, Smith WR. Optimizing the management of Mooretype I
postero-medial splitfracture dislocationsof the tibial head:
description of the Lobenhoffer approach. J Orthop Trauma.
2007;21:330-6.
9. Galla M, Lobenhoffer P. [The direct, dorsal ap-proach
to the treatment of unstable tibial postero-medial
fracture-dislocations]. Unfallchirurg. 2003;106:241-7. German.
10. Solomon LB, Stevenson AW, Baird RP, Pohl
AP.Posterolateral transfibular approach to tibial plateaufractures:
technique, results, and rationale. J OrthopTrauma.
2010;24:505-14.
11. Tao J,Hang DH, WangQG,GaoW, Zhu LB, WuXF,Gao KD. The
posterolateral shearing tibial plateaufracture: treatment and
results via a modified postero-lateral approach. Knee.
2008;15:473-9.
12. Higgins TF, Kemper D, Klatt J. Incidence and mor-
phologyof the posteromedial fragment in bicondylar tibialplateau
fractures. J Orthop Trauma. 2009;23:45-51.
13. Gosling T, Schandelmaier P, Muller M,Hankemeier S,
Wagner M, Krettek C. Single laterallocked screw plating of
bicondylar tibial plateaufractures. Clin Orthop Relat Res.
2005;439:207-14.
14. Gösling T, Schandelmaier P, Marti A, Hufner
T,Partenheimer A, Krettek C. Less invasive stabilizationof complex
tibial plateau fractures: a biomechanicalevaluation of a unilateral
locked screw plate anddouble plating. J Orthop Trauma.
2004;18:546-51.
15. Barei DP, Taitsman LA, Beingessner D, Dunbar RP,
Nork SE. Open diaphyseal long bone fractures: areduction method
using devitalized or extruded osse-ous fragments. J Orthop Trauma.
2007;21:574-8.
16. Eastman J, Tseng S, Lo E, Li CS, Yoo B, Lee
M.Retropatellar technique for intramedullary nailing
of proximal tibia fractures: a cadaveric assessment.
J Orthop Trauma. 2010;24:672-6.17. Higgins TF, Klatt J,
Bachus KN. Biomechanicalanalysis of bicondylar tibial plateau
fixation: how doeslateral locking plate fixation compare to dual
platefixation? J Orthop Trauma. 2007;21:301-6.
18. Eastman JG, Tseng SS, Lee MA, Yoo BJ. Theretropatellar
portal as an alternative site for tibial nailinsertion: a cadaveric
study. J Orthop Trauma. 2010;24:659-64.
19. Koval KJ, Sanders R, Borrelli J, Helfet D,DiPasquale
T, Mast JW. Indirect reduction and percu-taneous screw fixation of
displaced tibial plateaufractures. J Orthop Trauma.
1992;6:340-6.
20. Pichler W, Grechenig W, Tesch NP, Weinberg AM,Heidari
N, Clement H. The risk of iatrogenic injury tothe deep peroneal
nerve in minimally invasive osteo-synthesis of the tibia with the
less invasive stabilisa-tion system: a cadaver study. J Bone Joint
Surg Br.
2009;91:385-7.21. Dougherty PJ, Kim DG, Meisterling S,
Wybo C,YeniY. Biomechanicalcomparison of bicortical
versusunicortical screw placement of proximal tibia lockingplates:
a cadaveric model. J Orthop Trauma. 2008;22:399-403.
22. Oh JK, Sahu D, Hwang JH, Cho JW, Oh CW.Technical
pitfall while reducing the mismatch between
LCP PLT and upper end tibia in proximal tibia fractures.Arch
Orthop Trauma Surg. 2010;130:759-63.
23. Musahl V,Tarkin I, Kobbe P,TzioupisC, SiskaPA,Pape
HC. New trends and techniques in open reduc-tion and internal
fixation of fractures of the tibialplateau. J Bone Joint Surg Br.
2009;91:426-33.
24. Gautier E, Sommer C. Guidelines for the
clinicalapplication of the LCP. Injury. 2003;34Suppl 2:B63-76.
25. Marsh JL,Muehling V,Dirschl D,HurwitzS, BrownTD, Nepola J.
Tibial plafond fractures treated by articulated external
fixation: a randomized trial of postoperative motion versus
nonmotion. J OrthopTrauma. 2006;20:536-41.
26. Krettek C, Schandelmaier P, Tscherne H. Non-reamed
interlocking nailing of closed tibial fractureswith severe soft
tissue injury. Clin Orthop Relat Res.1995;315:34-47.
27. Bolhofner BR. Indirect reduction and compositefixation
of extraarticular proximal tibial fractures. ClinOrthop Relat Res.
1995;315:75-83.
28. Ricci WM, O’Boyle M, Borrelli J, Bellabarba C,Sanders
R. Fractures of the proximal third of the tibialshaft treated with
intramedullary nails and blockingscrews. J Orthop Trauma.
2001;15:264-70.
29. Nork SE, Barei DP, Schildhauer TA, Agel J, HoltSK,
Schrick JL, Sangeorzan BJ. Intramedullary nailingof proximal
quarter tibial fractures. J Orthop Trauma.2006;20:523-8.
30. Vidyadhara S, Sharath KR. Prospective study
of the clinico-radiological outcome of interlocked nailingin
proximal third tibial shaft fractures. Injury. 2006;37:536-42.
31. LindvallE, Sanders R, Dipasquale T, Herscovici
D,Haidukewych G, Sagi C. Intramedullary nailing versuspercutaneous
locked plating of extra-articular proximaltibial fractures:
comparison of 56 cases. J OrthopTrauma. 2009;23:485-92.
32. Nork SE, Schwartz AK, Agel J,Holt
SK,SchrickJL,Winquist RA. Intramedullary nailing of distal
meta-physeal tibial fractures. J Bone Joint Surg Am.
2005;87:1213-21.
33. Krettek C, Stephan C, Schandelmaier P,
Richter
M, Pape HC, Miclau T. The use of Poller screws asblocking screws
in stabilising tibial fractures treatedwith small diameter
intramedullary nails. J Bone JointSurg Br. 1999;81:963-8.
34. Buehler KC, Green J, Woll TS, Duwelius PJ. Atechnique
for intramedullary nailing of proximal thirdtibia fractures. J
Orthop Trauma. 1997;11:218-23.
35. Freedman EL, Johnson EE. Radiographic analy-sis of
tibial fracture malalignment following intra-medullary nailing.
Clin Orthop Relat Res. 1995;315:25-33.
36. Lang GJ, Cohen BE, Bosse MJ, Kellam JF.Proximal third
tibial shaft fractures. Should they benailed? Clin Orthop Relat
Res. 1995;315:64-74.
37. Weninger P, Tschabitscher M, Traxler H, Pfafl V,Hertz
H. Intramedullary nailing of proximal tibiafractures—an anatomical
study comparing three lat-eral starting points for nail insertion.
Injury. 2010;41:220-5.
38. Henley MB, Meier M, Tencer AF. Influences of some
design parameters on the biomechanics of theunreamed tibial
intramedullary nail. J Orthop Trauma.1993;7:311-9.
39. Tornetta P 3rd, Collins E. Semiextended positionof
intramedullary nailing of the proximal tibia. ClinOrthop Relat Res.
1996;328:185-9.
40. Gelbke MK, Coombs D, Powell S, DiPasquale
TG.Suprapatellar versus infra-patellar intramedullary nailinsertion
of the tibia: a cadaveric model for compar-ison of patellofemoral
contact pressures and forces.J Orthop Trauma. 2010;24:665-71.
41. Wysocki RW, Kapotas JS, Virkus WW. Intramed-ullary
nailing of proximal and distal one-third tibial
shaft fractures with intraoperative two-pin externalfixation. J
Trauma. 2009;66:1135-9.
42. DunbarRP, Nork SE,Barei DP,Mills
WJ.Provisionalplating of Type III open tibia fractures prior to
intramed-ullary nailing. J Orthop Trauma. 2005;19:412-4.
43. Shahulhameed A, Roberts CS, Ojike NI. Tech-nique for
precise placement of poller screws withintramedullary nailing of
metaphyseal fractures of thefemur and the tibia. Injury. 2010 May
18 [Epub aheadof print].
44. Tang P, Gates C, Hawes J, Vogt M, Prayson MJ.Does open
reduction increase the chance of infectionduring intramedullary
nailing of closed tibial shaftfractures? J Orthop Trauma.
2006;20:317-22.
45. Laflamme GY, Heimlich D, Stephen D, Kreder HJ,Whyne
CM. Proximal tibial fracture stability withintramedullary nail
fixation using oblique interlockingscrews. J Orthop Trauma.
2003;17:496-502.
46. Hansen M, Blum J, Mehler D, Hessmann MH,Rommens PM.
Double or triple interlocking whennailing proximal tibial
fractures? A biomechanicalinvestigation. Arch Orthop Trauma Surg.
2009;129:1715-9.
47. Court-Brown CM, Gustilo T, Shaw AD. Kneepain after
intramedullary tibial nailing: its incidence,etiology, and outcome.
J Orthop Trauma. 1997;11:103-5.
48. Keating JF, Orfaly R, O’Brien PJ. Knee pain
after tibial nailing. J Orthop Trauma. 1997;11:10-3.
49. Toivanen JA, Väistö O, Kannus P, Latvala K,Honkonen
SE, Järvinen MJ. Anterior knee pain after intramedullary
nailing of fractures of the tibial shaft. Aprospective, randomized
study comparing two differ-ent nail-insertion techniques. J Bone
Joint Surg Am.2002;84:580-5.
50. Karladani AH, Ericsson PA, Granhed H, Karlsson
L, Nyberg P. Tibial intramedullary nails—
should they be removed? A retrospective study of 71
patients.Acta Orthop. 2007;78:668-71.
51. Gaebler C, BergerU, Schandelmaier P,
Greitbauer M, Schauwecker HH, Applegate B, Zych G, Vécsei
V.Rates and odds ratios for complications in closed andopen tibial
fractures treated with unreamed, smalldiameter tibial nails: a
multicenter analysis of 467cases. J Orthop Trauma.
2001;15:415-23.
52. Bhandari M, Audige L, Ellis T, Hanson B;Evidence-Based
Orthopaedic Trauma Working Group.Operative treatment of
extra-articular proximal tibialfractures. J Orthop Trauma.
2003;17:591-5.
53. Cole PA, Zlowodzki M, Kregor PJ. Treatment
of proximal tibia fractures using the less invasive
stabi-lization system: surgical experience and early
clinicalresults in 77 fractures. J Orthop Trauma.
2004;18:528-35.
54. Stannard JP, Wilson TC, Volgas DA, Alonso JE.Theless
invasive stabilization system in the treatmentof complex fractures
of the tibial plateau: short-termresults. J Orthop Trauma.
2004;18:552-8.
55. Ricci WM, Rudzki JR, Borrelli J Jr. Treatment
of complex proximal tibia fractures with the less
invasiveskeletal stabilization system. J Orthop
Trauma.2004;18:521-7.
1559
T H E J O U R N A L O F B O N E & J O I
N T S U R G E R Y d J B J S . O RGVO L U M E 9
3 - A d NU M B E R 16 d A U G
U S T 1 7 , 2 0 1 1
S U R G I C A L T E C H N I Q U E S F O R C O M
P L E X
P R O X I M A L T I B I A L FR A C T U R E S