Embed Size (px)
DESCRIPTION
Surveillance and screening for new neoplasms in adult survivors of childhood cancer A report from the Childhood Cancer Survivor Study (CCSS). Paul Nathan MD, MSc The Hospital for Sick Children Toronto, Canada. Background The childhood cancer survivor population. - PowerPoint PPT Presentation
Citation preview

Surveillance and screening for new neoplasms in adult survivors of childhood cancer
A report from the Childhood Cancer Survivor Study (CCSS)
Paul Nathan MD, MScThe Hospital for Sick ChildrenToronto, Canada

• 5-year cancer survival in children ~80%
• Over 325,000 childhood cancer survivors alive in United States
• Over 40% of survivors will develop a severe or life threatening late effect of therapy
BackgroundThe childhood cancer survivor population

• 30-year cumulative incidence of SMN = 9.3%
• 30-year cumulative incidence of non-melanoma skin cancer = 6.9%
• Leading cause of death in 20+ year survivors
• Standardized incidence ratio = 9.0
• Standardized mortality ratio = 15.2
Meadows et al. JCO, 2009; Mertens et al. JNCI, 2008
SMN in the CCSS cohort
Second malignant neoplasms (SMN) in childhood cancer survivors

1. To assess adherence to published cancer surveillance guidelines by survivors at high risk for breast, colorectal or skin cancer as a result of their therapy
2. To compare non-high risk survivors’ adherence to national screening guidelines for breast, colorectal and cervical cancer with the general population
Study Aims

• Retrospective cohort study
• 26 centers: USA and Canada
• Diagnosis 1970-1986
• < 21 years at diagnosis
• Alive at 5 years
• Selected malignancies
Childhood Cancer Survivor Study

Coordinating Center
Contributing Institutions
Resource Center
Participating Centers

Study participants

Eligiblen=20,602
Eligiblen=20,602
Contactedn=17,567
Contactedn=17,567
Participants in Baseline Surveyn=14,370
Participants in Baseline Surveyn=14,370
Participants in Follow-up 2000n=10,388
Participants in Follow-up 2000n=10,388
Participants in Follow-up 2003n=9,308
Participants in Follow-up 2003n=9,308
Eligible for Current Analysisn=8,318
Eligible for Current Analysisn=8,318
Lost to Follow-upn=3,035Lost to Follow-upn=3,035
Declined Participationn=3,197Declined Participationn=3,197
Deceased Casesn=1,541Deceased Casesn=1,541
Exclusions n=990 Developed SMN (n=960) Race/ethnicity unknown (n=29) Other (n=1)
Exclusions n=990 Developed SMN (n=960) Race/ethnicity unknown (n=29) Other (n=1)

Survivors (8,318)
Population control (8,318)*
Gender (male) 51.9%
Race (White, non-Hispanic) 88.7%
Mean age at diagnosis (SD), years 7.8 (5.7) -
Mean age at interview (SD), years 31.2 (7.3) 32.7 (10.6)
Cancer center visit in last 2 years 12.5% -
*Matched 1:1 by age, gender, race/ethnicity from 2003 National Health Interview Survey
Demographics of Study Population

Leukemia35%
CNS tumor13%Hodgkin's
lymphoma10%
Wilms' tumor10%
Neuroblastoma7%
Soft tissue sarcoma
9%
Bone cancer8%
Non-Hodgkin's lymphoma
8%
Cancer Diagnosis in 8,318 Survivors

Specific Aim 1
Adherence to published cancer surveillance guidelines by survivors at high risk for breast, colorectal or skin cancer


Risk Definitions and Recommended Surveillance
COLORECTAL BREAST SKIN
HIGH-RISK
>30 Gy to abdomen, pelvis or spine
N=794
Female, >20 Gy to breast
N=521
Any radiation therapy
N=4,833
RECOMMENDEDSURVEILLANCE
Colonoscopy every 5 years starting at age 35
Annual mammogram starting at later of 8 years after radiation or age 25
Annual dermatologic exam of irradiated areas

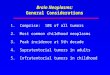
Compliance with Recommended Surveillance Tests
11.5%
46.3%
26.7%
0%
20%
40%
60%
80%
100%
Colorectalcancer
Breast cancer Skin cancer
High-risk group
% c
om
ply
ing
wit
h g
uid
elin
es

Predictors of AdherenceMultivariable Logistic Regression Models
Covariates
• Sex
• Race/ethnicity
• Age at diagnosis and interview
• Employment, education, insurance
• Chronic disease, mental health, physical
impairment, concern about future health
• Survivor or doctor has cancer treatment summary
• Medical care in last 2 years, care at a cancer center

Significant Predictors of AdherenceMultivariable Logistic Regression Models
• ColonoscopyOlder age at interview RR=1.08 (1.00-1.17)
• MammogramOlder age at interview RR=1.09 (1.04-1.13)
Care at cancer center RR=1.70 (1.04-2.76)
• Skin examNon-white RR=0.63 (0.42-0.95)
Care at cancer center RR=1.55 (1.22-1.96)
Survivor has treatment summary RR=1.30 (1.07-1.58)

Specific Aim 2
Comparison of “non-high risk” survivors vs. general population on adherence to national screening guidelines for breast, colorectal and cervical cancer

US Preventive Services Task Force Cancer Screening Recommendations
• Breast Screening mammography every 1-2 years for women aged 40 and older
• ColorectalColonoscopy at intervals of 10 years between ages of 50-75 years*
• CervixPap smear beginning within 3 years of onset of sexual activity or age 21 (whichever comes first) and screening at least every 3 years
* OR annual fecal occult blood testing OR sigmoidoscopy every 5 years combined with fecal occult blood testing every 3 years

US Preventive Services Task Force Cancer Screening Recommendations
Breast Colon CervixRR=1.29 RR=0.97 RR=1.17
95% CI, 1.12-1.48 95% CI, 0.31-3.00 95% CI, 1.14-1.20
P<0.001 P=0.95 P=<0.001
Co
mp
lian
ce w
ith s
cre
enin
g
Survivor Gen. Pop. Survivor Gen. Pop. Survivor Gen. Pop.

Significant Predictors of AdherenceMultivariable Logistic Regression Models
• Breast None
• ColonToo few survivors over 50 years to analyse in
detail
Emerging evidence of increased GI malignancies in survivor cohort
• CervixOnly being “married or living as married”
predicted PAP smear compliance (RR 1.17, 1.03-1.34)

Conclusions (1)Adherence to Guidelines for Cancer Survivors
• Rates of colonoscopy, mammography and skin exams in high-risk patients are very low.
• Care at a cancer center modestly increases surveillance for breast and skin cancer.
• Patients and their physicians need to be educated about recommended surveillance.

Conclusions (2)Adherence to National Screening Guidelines Survivors
• Cancer survivors are more likely to undergo mammograms and PAP smears than general population.
• BUT: Compliance rates are very low for colonoscopy and only moderate for mammography.
• Health care providers must take opportunity to promote early cancer detection strategies in survivors.

Study Considerations
1. Self-report data
2. CCSS cohort is a select group – study may overestimate care received
3. Cohort 1970-1986
4. Did not assess all screening/surveillance modalities (e.g. breast MRI, fecal occult blood)

Co-Investigators
• Kevin Oeffinger, Memorial Sloan-Kettering Cancer Center • Kirsten Ness, St. Jude Children’s Research Hospital • Martin Mahoney, Roswell Park Cancer Institute • Zhenghong Li, St. Jude Children’s Research Hospital
• Melissa Hudson, St. Jude Children’s Research Hospital • Jennifer Ford, Memorial Sloan-Kettering Cancer Center • Wendy Landier, City of Hope • Greg Armstrong, St. Jude Children’s Research Hospital • Tara Henderson, University of Chicago • Leslie Robison, St. Jude Children’s Research Hospital

CCSS Institutions
• University of Minnesota• Denver Children’s Hospital• Children’s Hospital of Pittsburgh• Stanford University• Dana-Farber Cancer Institute• Children’s National Medical Center• M.D. Anderson Cancer Center• Memorial Sloan-Kettering Cancer
Center• Texas Children’s Hospital• University of California, San
Francisco• Seattle Children’s Hospital• Toronto Hospital for Sick Children• Children’s Medical Center of Dallas• Children’s Hospital of Columbus• Emory University
• St. Jude Children’s Research Hospital • Roswell Park Cancer Center• Mayo Clinic• Children’s Health Care Minneapolis• Children’s Hospital of Philadelphia• St. Louis Children’s Hospital• Children’s Hospital of Los Angeles• UCLA Medical Center• Miller Children’s Hospital Long Beach• Children’s Hospital of Orange County• Riley Hospital for Children – Indiana
Univ.• UAB/Children’s Hospital of Alabama• University of Michigan – Mott Children’s • Fred Hutchinson Cancer Research
Center

A Resource for Research
• The Childhood Cancer Survivor Study is an NCI-funded resource to promote and facilitate research among long-term survivors of cancer diagnosed during childhood and adolescence.
• Investigators interested in potential uses of this resource are encouraged to visit:
www.stjude.org/ccss