Embed Size (px)
Citation preview
Survival and Predictors of Outcome in Patients WithAcute Leukemia Admitted to the Intensive Care Unit
Snehal G. Thakkar, MD1
Alex Z. Fu, PhD2
John W. Sweetenham, MD1
Zachariah A. Mciver, DO3
Sanjay R. Mohan, MD3
Giridharan Ramsingh, MD3
Anjali S. Advani, MD1
Ronald Sobecks, MD1
Lisa Rybicki, MS2
Matt Kalaycio, MD1
Mikkael A. Sekeres, MD, MS1
1 Department of Hematologic Oncology and BloodDisorders, Cleveland Clinic Taussig Cancer Cen-ter, Cleveland, Ohio.
2 Department of Quantitative Health Sciences,Cleveland Clinic Taussig Cancer Center, Cleve-land, Ohio.
3 Department of Internal Medicine, ClevelandClinic, Cleveland, Ohio.
BACKGROUND. Predictors of outcome and rates of successful discharge have not
been defined for patients with acute leukemia admitted to intensive care units
(ICUs) in the US.
METHODS. This is a retrospective analysis of 90 patients with acute leukemia (no
history of bone marrow transplant) admitted to an ICU from 2001–2004. The pri-
mary endpoints were improvement and subsequent discharge from the ICU, dis-
charge from the hospital, and 2-month survival after hospital discharge.
Secondary endpoints were 6- and 12-month survival. Univariate and multivariate
logistic regression analyses were performed to identify factors predicting out-
come.
RESULTS. The median age of patients was 54 years and 48 (53%) were male. The
most common reason for ICU transfer for all patients was respiratory compro-
mise. The majority of all patients (68%) were eventually placed on ventilator sup-
port and approximately half required pressors. During the ICU course, 29
patients (32%) improved and subsequently resumed aggressive leukemia manage-
ment, and 24 patients (27%) survived to be discharged from the hospital. The 2-,
6-, and 12-month overall survival was 24 (27%), 16 (18%), and 14 (16%), respec-
tively. Higher APACHE II score, use of pressors, undergoing bone marrow trans-
plantation preparative regimen, and adverse cytogenetics predicted worse
outcome. Newly diagnosed leukemia, type of leukemia, or age did not.
CONCLUSIONS. One of 4 patients with acute leukemia survived an ICU admission
to be discharged from the hospital and were alive 2 months later. A diagnosis of
acute leukemia should not disqualify patients from an ICU admission. Cancer
2008;112:2233–40. � 2008 American Cancer Society.
KEYWORDS: acute leukemia, intensive care unit admission, survival.
D espite advances (eg, growth factors, newer antibiotics) and
steady improvements in our understanding of acute leukemias,
the prognosis for many patients with acute leukemia remains poor,
particularly for older adults.1–6 Approximately 16,000 new cases of
acute leukemia will be diagnosed in the US in 2006.7 Estimates of 5-
year disease-free survival range from 25% to 40% in younger
patients and 5% to 15% in older adults. Treatment-related mortality
from remission induction therapy approaches 25% for certain sub-
groups.4,6,8–11 Patients with acute leukemia are also at high risk for
treatment-related morbidities, and these complications may necessi-
tate admission to an intensive care unit (ICU).12
Patients with acute leukemia historically have had poor out-
comes after admission to the ICU.13–16 Patients with cancer as a
whole are discouraged from admission to ICUs based on published
recommendations supporting the poor outcome of patients with
cancer, and on the belief that limited resources should be reserved
Address for reprints: Mikkael A. Sekeres, MD,MS, Hematologic Oncology and Blood Disorders,Cleveland Clinic Taussig Cancer Center, 9500Euclid Ave., Desk R35, Cleveland, OH 44195;Fax: (216) 636-0636; E-mail: [email protected]
Received October 9, 2007; revision receivedNovember 19, 2007; accepted November 27,2007.
ª 2008 American Cancer SocietyDOI 10.1002/cncr.23394Published online 17 March 2008 in Wiley InterScience (www.interscience.wiley.com).
2233

for patients with reversible medical conditions.17,18
Although predictors of outcome after an ICU stay for
the general population admitted to the ICU have
been published, these predictors have not been vali-
dated in patients with acute leukemia.19–21
The purpose of this study was to evaluate out-
comes and to determine predictors of outcome for
patients with acute leukemia admitted to the ICU.
MATERIALS AND METHODSThe Institutional Review Board at the Cleveland
Clinic initially approved this study in May 2005 and
an extension was approved in May 2006.
PatientsAll patients with a diagnosis of acute leukemia (acute
myeloid leukemia [AML] or acute lymphoblastic leu-
kemia [ALL] as defined by the World Health Organi-
zation) who had not received a bone marrow
transplantation (BMT) were enrolled if an ICU
admission at the Cleveland Clinic was part of the
hospital course.22 This included patients who were
newly diagnosed having not yet received chemother-
apy; patients undergoing or having just received
remission induction therapy; patients receiving or
having just received postremission therapy; patients
with recurring acute leukemia undergoing salvage
treatment; and patients beginning their preparative
regimens for BMT, but before stem cell infusions.
All patients with an AML diagnosis were treated
with an anthracycline- or anthracenedione-based
remission induction regimen. Postremission therapy
for younger patients (<55 years) consisted of at least
1 cycle of high-dose cytarabine (HiDAC), whereas for
older patients (�55 years) it included at least 1 cycle
of a low-dose cytarabine-based regimen. Patients
with ALL were treated with a vincristine/prednisone-
based remission induction regimen, followed by a
cytarabine-based intensification cycle, central nerv-
ous system prophylaxis that was either methotrexate
or radiation-based, and vincristine/prednisone-based
maintenance therapy. There were several BMT pre-
parative regimens, with the majority including busul-
fan and cyclophosphamide with or without
etoposide. Three of the preparative regimens also
included total body irradiation.
Description of the ICUApproximately 400 patients with acute leukemia are
admitted per year (approximately 130 with a new
acute leukemia diagnosis) to the Cleveland Clinic.
The medical ICU (MICU) is a closed 20-bed unit that
admits approximately 1400 patients per year. In addi-
tion, there are 5 other closed specialized units (surgical,
cardiothoracic, cardiac, heart failure, neurosurgical)
where overflow patients from the medical ICU can
be admitted.
The daytime MICU team consists of a senior
intensivist, 2 pulmonary/critical care fellows, and a
team of senior residents and interns. The nighttime
duties fall to a senior resident and intern who remain
in-house with pulmonary/critical care and leukemia
fellows available by phone. The nursing-staff-to-
patient ratio is 1:2. Patients with a leukemia diagno-
sis admitted to the ICU continue to be followed by
the primary leukemia service.
Data CollectionEvery patient with a diagnosis of acute leukemia
admitted directly to the ICU or to the leukemia ser-
vice between January, 2001 and February, 2005 was
identified. This list was then cross-referenced to the
MICU-tagged patient list available through the
Department of Pulmonary and Critical Care. This
was further corroborated by a documented substan-
tial increase in daily hospital charges, indicating
transfer from the leukemia floor to an intensive care
setting. A chart collection for those consecutive
patients admitted to the ICU was undertaken and
the written documentation in conjunction with the
electronic chart was the basis for the review. No
patients or families of patients were contacted.
Statistical AnalysisThe primary purpose of this study was to identify
prognostic factors for outcome. Successful outcomes
were defined as improvement in the ICU with subse-
quent ICU discharge and resumption of aggressive
leukemia management, 2-month, 6-month, and 1-
year survival measured from hospital admission
(Hospital Admission 5 Day 0). Patients were cen-
sored for death or ICU discharge to a palliative or
hospice setting. Each outcome assessed was meas-
ured against 10 prognostic variables. These variables
included age, white blood cell count (WBC) at hospi-
tal admission, lactate dehydrogenase (LDH) at admis-
sion, acute leukemia type, cytogenetics (AML, as
defined by CALGB; ALL, BCR/ABL translocation),
phase of treatment, hospital day of transfer to the
ICU, reason for transfer to the ICU, the use of press-
ors in the ICU, and APACHE II (Acute Physiology and
Chronic Health Evaluation) score.20,23 The APACHE II
score was calculated based on several factors, with
the total score predicting mortality (Table 1).21
To identify univariate correlates of outcome, a
logistic regression analysis was performed. A desired
outcome was defined as an odds ratio (OR) of greater
2234 CANCER May 15, 2008 / Volume 112 / Number 10

than 1. A similar logistic regression analysis was per-
formed to identify multivariate correlates of out-
come. There was a stepwise selection procedure for
the variables, which required a P < .20 for the vari-
able to enter the model, and then P < .05 for the
variable to retain itself within the model. A final
bootstrap analysis was performed to further support
the conclusions. The same multivariate logistic
regression was used to predict the survival outcomes
of patients with acute leukemia admitted to the ICU.
A decision model was developed for these patients
with pressor use, intubation, and length of ICU stay
information. The Cochran-Armitage trend test was
used to determine whether the percentage of death
in the ICU correlated with the predicted mortality
score (APACHE II, Table 1).
To better understand the impact of ICU care,
additional analyses were conducted comparing this
group of patients with a group of 1:1 age-matched
patients diagnosed with acute leukemia during the
same calendar years as the ICU patients, but who
were not admitted to the ICU. A logistical regression
was performed to compare the 2-, 6-, and 12-month
survival between these 2 groups after controlling for
baseline characteristics.
RESULTSPatient CharacteristicsNinety consecutive patients were identified as having
been admitted to the ICU and available for analysis.
The only leukemia patients excluded from analysis
were those patients who had already received the
stem cell infusion of their BMT regimen. Patient
characteristics are shown in Table 2. The median age
was 54 years and there was an approximate 1:1 ratio
of males to females. Seventy-four (82%) of the
reviewed patients had AML, 16 (18%) ALL. The distri-
bution of cytogenetic abnormalities was typical of
this population mix of younger and older adults: 74
(91%) of the AML patients had intermediate- or
poor-risk karyotypes, whereas 6 (38%) ALL patients
had a BCR-ABL translocation (the Philadelphia chro-
mosome).
Factors Associated With ICU AdmissionAdmission to the ICU was based on a comprehensive
review of the clinical scenario, including the wishes
of the patient. As criteria within the critical care liter-
ature defining set parameters for ICU admission of-
ten include no methodology, are not based on a
comprehensive literature review, or are based on an
author’s personal experience, and thus are not uni-
form, our institution does not follow set ICU admis-
sion criteria.24 Thus, the decision for ICU transfer
was based solely on the initial ICU consult. No
patient, however, was denied admission to the ICU
based on history of acute leukemia.
The most common reason for hospital admission
was fever or infection (Table 2). Twenty-seven (30%)
patients had a new diagnosis of acute leukemia and
were undergoing remission induction therapy.
Patients were transferred to the ICU a median of
8 days (range, 0–81) after hospital admission.
Forty patients (44%) were transferred to the ICU for
multiple reasons. Sixty-one required endotracheal
intubation with mechanical ventilatory support.
Approximately half (48%) required blood pressure
support with ionotropic therapies (pressors). The
median APACHE II score was 22 (range, 9–40) indi-
cating a predicted mortality of 40%.21
Outcome and Predictors of OutcomeTwenty-nine patients (32%) survived their ICU stay
to return to aggressive leukemia management,
whereas 24 patients (27%) survived to hospital dis-
charge. All but 6 patients were discharged to home.
Of the 6 patients not discharged to home, 5 were dis-
charged to a subacute nursing facility and 1 was dis-
charged to a regional community hospital near the
patient’s home. All 24 patients who survived to hos-
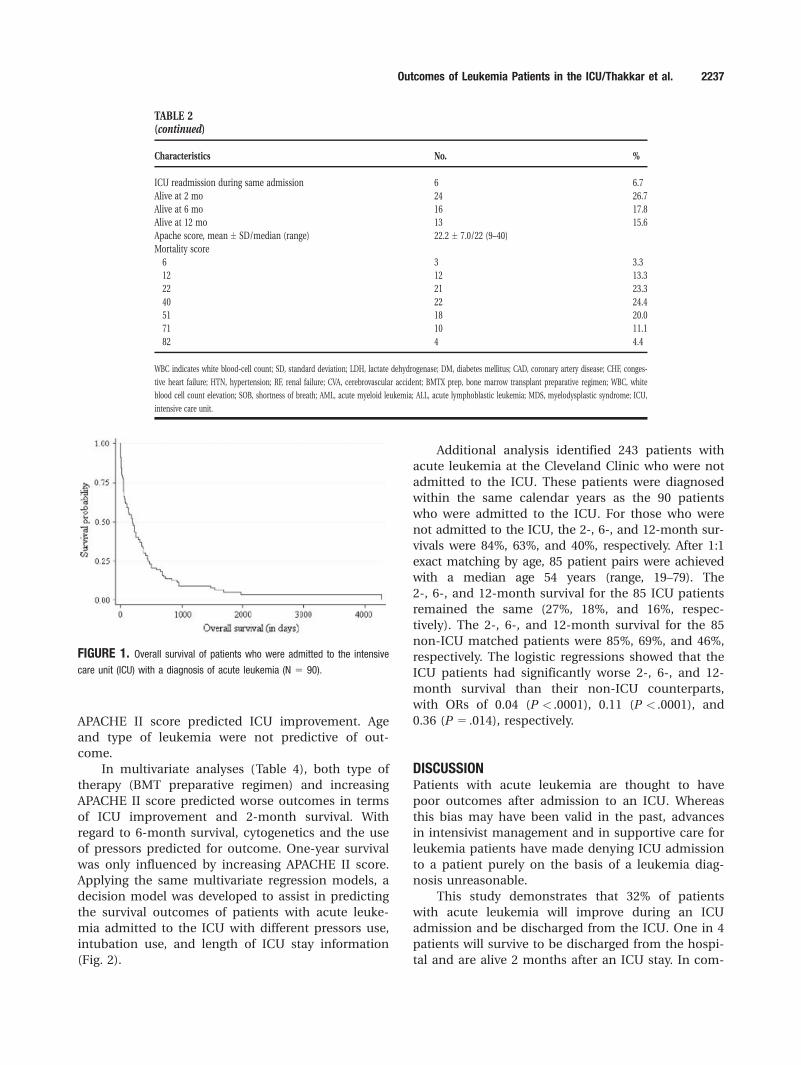
pital discharge were alive at 2 months. Six- and 12-
month survivals were 18% and 16%, respectively. Me-
dian survival for the entire population was 197 days
(Fig. 1). Patients with AML had a median survival of
199 days and those with ALL had a median survival
of 192 days. Of 11 patients with acute leukemia with
recurring disease, 7 (64%) died during their ICU stay.
Univariate analysis is shown in Table 3. The use
of pressors and a higher APACHE II score predicted
for shorter 2-, 6-, and 12-month survival. Only the
TABLE 1APACHE II Scoring System14
Apache II score* % Nonoperative mortality
0–4 4
5–9 6
10–14 12
15–19 22
20–24 40
25–29 51
30–34 71
�35 82
* The Acute Physiology Apache II Score is based on 14 variables (temperature, mean arterial pres-
sure, heart rate, respiratory rate, A-aPO2, PAO2, arterial pH, serum bicarbonate, serum sodium, serum
potassium, serum creatinine, hematocrit, white blood-cell count, Glasgow coma score). There is also
an Age Adjustment, Chronic Health Adjustment score.
Outcomes of Leukemia Patients in the ICU/Thakkar et al. 2235

TABLE 2Patient Characteristics
Characteristics No. %
Age, y, mean � SD/median (range) 52.6 � 12.3/54 (17–90)
Sex, men/women 48/42 53.3/46.7
Race
White 75 83.3
African American/other 13/2 14.4/2.2
Performance status, 0–1 to �2 67/23 74/26
WBC at admission
Mean � SD 36.5 � 67.3
Median (range) 7.8 (0.01–317.9)
LDH at admission, n 5 76
Mean � SD 618 � 749
Median (range) 305 (13–4624)
Growth factors used 19 21.1
Past medical history
DM 18 20.0
Cardiac, CAD/CHF/HTN 48 53.0
Other, RF/CVA/etc 47 52.2
None 38 42.2
Reason for hospital admissions
Fever or infection 32 35.6
New diagnosis 27 30.0
Relapse/BMTX prep 19 21.1
Other, incl WBC/SOB/etc 22 24.4
Diagnosis AML/ALL 74/16 82.2/17.8
If AML subtype n 5 74; M3/Non-M3 subtype 7/67 9.5/90.5
If AML, n 5 74
Cause unknown 50 67.6
MDS 20 27.0
Therapy 4 5.4
If ALL subtype n 5 16; Pre–B-cell/T-cell 13/3 81.3/18.7
If ALL
Philadelphia chromosome, n 5 16; Ph1/Ph2 6/6 37.5/37.5
Unknown 4 25.0
Cytogenetics
Good/Intermediate/Poor 7/36/38 8.6/44.4/46.9
Unknown 9 10.0
Type of treatment
Induction 27 30.0
BMT 19 21.1
Other 44 48.9
Days of transfer to ICU, mean � SD/median (range) 13.4 � 15.6/8 (0–81)
ICU admit chemotherapy, d. n 5 55, mean � SD/median (range) 15.8 � 13.2/14 (0–51)
Reason for transfer to ICU
Respiratory 57 63.3
Cardiovascular 12 13.3
Sepsis 51 56.7
Other 20 22.2
No. of reasons for transfer to ICU
0–1 50 55.5
2 37 41.1
3–4 3 3.4
Extubation (61 pts intubated) 25 41.0
ICU pressors 44 48.9
Length of ICU stay, d, n 5 89, mean � SD/median (range) 6.3 � 8.3/4 (1–60)
Outcome
Improved 29 32.2
Died in ICU/Died after transfer 51/10 56.7/11.1
(continued)
2236 CANCER May 15, 2008 / Volume 112 / Number 10
APACHE II score predicted ICU improvement. Age
and type of leukemia were not predictive of out-
come.
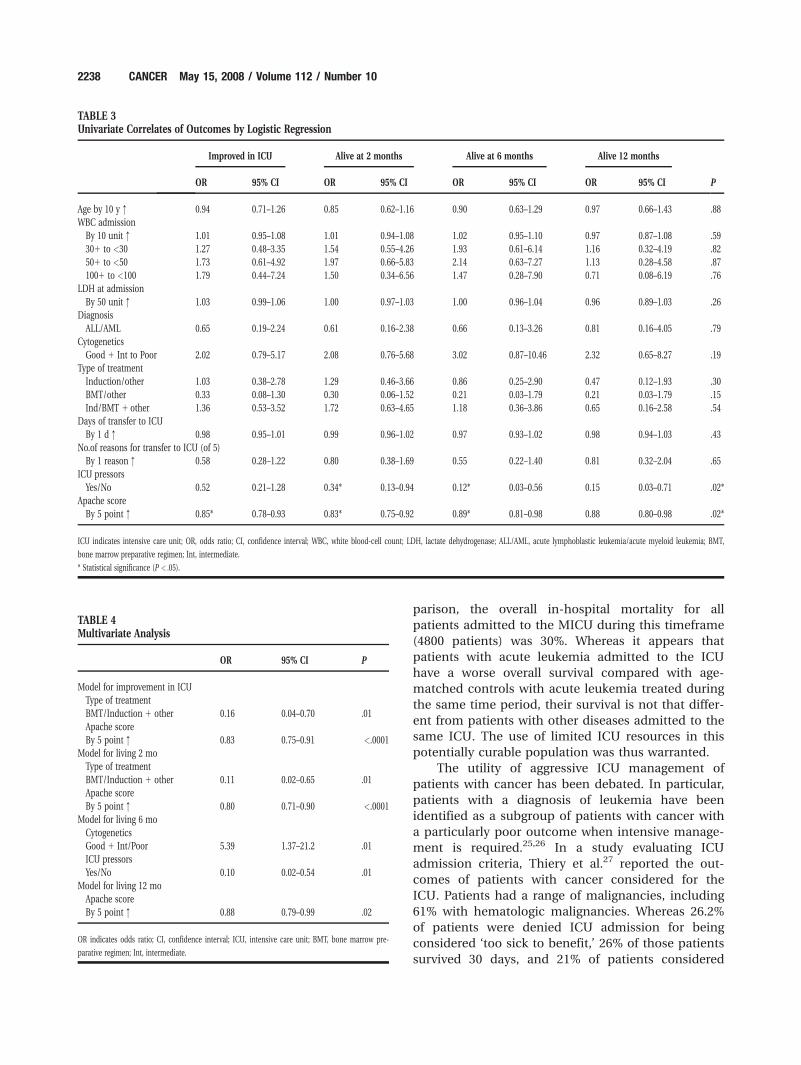
In multivariate analyses (Table 4), both type of
therapy (BMT preparative regimen) and increasing
APACHE II score predicted worse outcomes in terms
of ICU improvement and 2-month survival. With
regard to 6-month survival, cytogenetics and the use
of pressors predicted for outcome. One-year survival
was only influenced by increasing APACHE II score.
Applying the same multivariate regression models, a
decision model was developed to assist in predicting
the survival outcomes of patients with acute leuke-
mia admitted to the ICU with different pressors use,
intubation use, and length of ICU stay information
(Fig. 2).
Additional analysis identified 243 patients with
acute leukemia at the Cleveland Clinic who were not
admitted to the ICU. These patients were diagnosed
within the same calendar years as the 90 patients
who were admitted to the ICU. For those who were
not admitted to the ICU, the 2-, 6-, and 12-month sur-
vivals were 84%, 63%, and 40%, respectively. After 1:1
exact matching by age, 85 patient pairs were achieved
with a median age 54 years (range, 19–79). The
2-, 6-, and 12-month survival for the 85 ICU patients
remained the same (27%, 18%, and 16%, respec-
tively). The 2-, 6-, and 12-month survival for the 85
non-ICU matched patients were 85%, 69%, and 46%,
respectively. The logistic regressions showed that the
ICU patients had significantly worse 2-, 6-, and 12-
month survival than their non-ICU counterparts,
with ORs of 0.04 (P < .0001), 0.11 (P < .0001), and
0.36 (P 5 .014), respectively.
DISCUSSIONPatients with acute leukemia are thought to have
poor outcomes after admission to an ICU. Whereas
this bias may have been valid in the past, advances
in intensivist management and in supportive care for
leukemia patients have made denying ICU admission
to a patient purely on the basis of a leukemia diag-
nosis unreasonable.
This study demonstrates that 32% of patients
with acute leukemia will improve during an ICU
admission and be discharged from the ICU. One in 4
patients will survive to be discharged from the hospi-
tal and are alive 2 months after an ICU stay. In com-
TABLE 2(continued)
Characteristics No. %
ICU readmission during same admission 6 6.7
Alive at 2 mo 24 26.7
Alive at 6 mo 16 17.8
Alive at 12 mo 13 15.6
Apache score, mean � SD/median (range) 22.2 � 7.0/22 (9–40)
Mortality score
6 3 3.3
12 12 13.3
22 21 23.3
40 22 24.4
51 18 20.0
71 10 11.1
82 4 4.4
WBC indicates white blood-cell count; SD, standard deviation; LDH, lactate dehydrogenase; DM, diabetes mellitus; CAD, coronary artery disease; CHF, conges-
tive heart failure; HTN, hypertension; RF, renal failure; CVA, cerebrovascular accident; BMTX prep, bone marrow transplant preparative regimen; WBC, white
blood cell count elevation; SOB, shortness of breath; AML, acute myeloid leukemia; ALL, acute lymphoblastic leukemia; MDS, myelodysplastic syndrome; ICU,
intensive care unit.
FIGURE 1. Overall survival of patients who were admitted to the intensivecare unit (ICU) with a diagnosis of acute leukemia (N 5 90).
Outcomes of Leukemia Patients in the ICU/Thakkar et al. 2237
parison, the overall in-hospital mortality for all
patients admitted to the MICU during this timeframe
(4800 patients) was 30%. Whereas it appears that
patients with acute leukemia admitted to the ICU
have a worse overall survival compared with age-
matched controls with acute leukemia treated during
the same time period, their survival is not that differ-
ent from patients with other diseases admitted to the
same ICU. The use of limited ICU resources in this
potentially curable population was thus warranted.
The utility of aggressive ICU management of
patients with cancer has been debated. In particular,
patients with a diagnosis of leukemia have been
identified as a subgroup of patients with cancer with
a particularly poor outcome when intensive manage-
ment is required.25,26 In a study evaluating ICU
admission criteria, Thiery et al.27 reported the out-
comes of patients with cancer considered for the
ICU. Patients had a range of malignancies, including
61% with hematologic malignancies. Whereas 26.2%
of patients were denied ICU admission for being
considered ‘too sick to benefit,’ 26% of those patients
survived 30 days, and 21% of patients considered
TABLE 3Univariate Correlates of Outcomes by Logistic Regression
Improved in ICU Alive at 2 months Alive at 6 months Alive 12 months
POR 95% CI OR 95% CI OR 95% CI OR 95% CI
Age by 10 y : 0.94 0.71–1.26 0.85 0.62–1.16 0.90 0.63–1.29 0.97 0.66–1.43 .88
WBC admission
By 10 unit : 1.01 0.95–1.08 1.01 0.94–1.08 1.02 0.95–1.10 0.97 0.87–1.08 .59
301 to <30 1.27 0.48–3.35 1.54 0.55–4.26 1.93 0.61–6.14 1.16 0.32–4.19 .82
501 to <50 1.73 0.61–4.92 1.97 0.66–5.83 2.14 0.63–7.27 1.13 0.28–4.58 .87
1001 to <100 1.79 0.44–7.24 1.50 0.34–6.56 1.47 0.28–7.90 0.71 0.08–6.19 .76
LDH at admission
By 50 unit : 1.03 0.99–1.06 1.00 0.97–1.03 1.00 0.96–1.04 0.96 0.89–1.03 .26
Diagnosis
ALL/AML 0.65 0.19–2.24 0.61 0.16–2.38 0.66 0.13–3.26 0.81 0.16–4.05 .79
Cytogenetics
Good 1 Int to Poor 2.02 0.79–5.17 2.08 0.76–5.68 3.02 0.87–10.46 2.32 0.65–8.27 .19
Type of treatment
Induction/other 1.03 0.38–2.78 1.29 0.46–3.66 0.86 0.25–2.90 0.47 0.12–1.93 .30
BMT/other 0.33 0.08–1.30 0.30 0.06–1.52 0.21 0.03–1.79 0.21 0.03–1.79 .15
Ind/BMT 1 other 1.36 0.53–3.52 1.72 0.63–4.65 1.18 0.36–3.86 0.65 0.16–2.58 .54
Days of transfer to ICU
By 1 d : 0.98 0.95–1.01 0.99 0.96–1.02 0.97 0.93–1.02 0.98 0.94–1.03 .43
No.of reasons for transfer to ICU (of 5)
By 1 reason : 0.58 0.28–1.22 0.80 0.38–1.69 0.55 0.22–1.40 0.81 0.32–2.04 .65
ICU pressors
Yes/No 0.52 0.21–1.28 0.34* 0.13–0.94 0.12* 0.03–0.56 0.15 0.03–0.71 .02*
Apache score
By 5 point : 0.85* 0.78–0.93 0.83* 0.75–0.92 0.89* 0.81–0.98 0.88 0.80–0.98 .02*
ICU indicates intensive care unit; OR, odds ratio; CI, confidence interval; WBC, white blood-cell count; LDH, lactate dehydrogenase; ALL/AML, acute lymphoblastic leukemia/acute myeloid leukemia; BMT,
bone marrow preparative regimen; Int, intermediate.
* Statistical significance (P < .05).
TABLE 4Multivariate Analysis
OR 95% CI P
Model for improvement in ICU
Type of treatment
BMT/Induction 1 other 0.16 0.04–0.70 .01
Apache score
By 5 point : 0.83 0.75–0.91 <.0001
Model for living 2 mo
Type of treatment
BMT/Induction 1 other 0.11 0.02–0.65 .01
Apache score
By 5 point : 0.80 0.71–0.90 <.0001
Model for living 6 mo
Cytogenetics
Good 1 Int/Poor 5.39 1.37–21.2 .01
ICU pressors
Yes/No 0.10 0.02–0.54 .01
Model for living 12 mo
Apache score
By 5 point : 0.88 0.79–0.99 .02
OR indicates odds ratio; CI, confidence interval; ICU, intensive care unit; BMT, bone marrow pre-
parative regimen; Int, intermediate.
2238 CANCER May 15, 2008 / Volume 112 / Number 10
‘too well to benefit’ from an ICU admission died
within 30 days. It was concluded that enough inaccu-
racy existed in predicting ICU outcome that broader
admission criteria for patients with cancer being
considered for ICU admission should be considered.
Our study identified significant predictors of out-
come, including the treatment type and APACHE II
score (for earlier timepoints), and cytogenetics and
pressor use for 6- and 12-month survival. Those
patients who were being treated with a BMT prepara-
tive regimen had worse outcomes if they were
admitted to the ICU. This probably reflects the
increased intensity of the preparative regimen as
compared with typical induction therapy, and that
patients with acute leukemia who undergo a BMT
have already been exposed to multiple courses of
chemotherapy, and are more likely to be immuno-
suppressed and experience morbidities as a result.
This is the first study to validate the APACHE II
scoring system as a predictor of outcome in patients
with acute leukemia. This extends the finding that
the SAPS II has utility in this population.28 The use
of pressors in the ICU has already been correlated
with worse outcome in other reviews.29,30 Interest-
ingly, cytogenetic risk groups retained similar predic-
tive abilities in patients with acute leukemia
requiring an ICU stay, as they do in the acute leuke-
mia population as a whole.1,31 In these studies the 1-
year survival for those with poor-risk cytogenetics
was 40%, to almost 70% in those with good-risk cyto-
genetics. A similar dichotomy can be seen with our
ICU patients at 1 year between those with good-risk
cytogenetics (43% 1-year survival) and those with
poor risk (11% 1-year survival).
Other studies have also identified predictors of
outcome in patients with cancer admitted to the
ICU, including mechanical ventilation and older
age.32–35 Age was not a predictive factor in our study
and should not be used as an exclusion criterion for
ICU admission. That invasive mechanical ventilation
was not predictive reflects that most of our patients
required this modality, and thus it could not be ana-
lyzed separately.
On the basis of our results from the multivariate
analysis (Table 4) a decision model was developed to
assist in predicting the survival outcomes of patients
with acute leukemia admitted to the ICU (Fig. 2).
The differences between outcomes are useful both
clinically and statistically because of significant pre-
dictors form the multivariate analysis in Table 4. We
recognize that these survival estimates reflect our
single institution experience as well as only 90
patients, but it can serve as a template upon which
clinicians, patients, and families can discuss code
status as well as end-of-life decisions.
In conclusion, our review supports aggressive
ICU management of patients with acute leukemia.
Cytogenetics, APACHE II score, and the use of press-
ors predicted outcome. Mechanical ventilation,
increasing age, and WBC did not. It is reasonable to
expect almost 1 in 3 patients to improve after an
ICU admission to continue aggressive leukemia man-
agement and 1 in 4 to be alive 2 months after hospi-
tal discharge.
REFERENCES1. Byrd JC, Mrozek A, Dodge RK, et al. Pretreatment cytoge-
netic abnormalities are predictive of induction success, cu-
mulative incidence of relapse, and overall survival in adult
patients with de novo acute myeloid leukemia: results
from Cancer and Leukemia Group B (CALGB 8461). Blood.
2002;100:4325–4336.
FIGURE 2. Intensive care unit (ICU) outcomes decision model with the 2 months, 6 months, and 12 months chance of survival.
Outcomes of Leukemia Patients in the ICU/Thakkar et al. 2239

2. Baudard M, Beauchamp-Nicoud A, Delmer A, et al. Has
the prognosis of adult patients with acute myeloid leuke-
mia improved over years? A single institution experience of
784 consecutive patients over a 16-year period. Leukemia.
1999;13:1481–1490.
3. Pui CH, Evans WE. Treatment of acute lymphoblastic leu-
kemia. N Engl J Med. 2006;354:166–178.
4. Stone RM, Berg DT, George SL, et al. Granulocyte-macro-
phage colony-stimulating factor after initial chemotherapy
for elderly patients with primary acute myelogenous leuke-
mia. Cancer and Leukemia Group B. N Engl J Med.
1995;332:1671–167.
5. Goldstone AH, Burnett AK, Wheatley K, et al. Attempts to
improve treatment outcomes in acute myeloid leukemia
(AML) in older patients: the results of the United Kingdom
Medical Research Council AML11 trial. Blood. 2001;98:
1302–1311.
6. Larson RA, Dodge RK, Linker CA, et al. A randomized con-
trolled trial of filgrastim during remission induction and
consolidation chemotherapy for adults with acute lympho-
blastic leukemia: CALGB study 9111. Blood. 1998;92:1556–
1564.
7. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA
Cancer J Clin. 2006;56:106–130.
8. Sekeres MA, Stone RM, Zahrieh D, et al. Decision-making
and quality of life in older adults with acute myeloid leuke-
mia or advanced myelodysplastic syndrome. Leukemia.
2004;18:809–816.
9. Rowe JM, Neuberg D, Friedenberg W, et al. A phase 3 study
of 3 induction regimens and of priming with GM-CSF in
older adults with acute myeloid leukemia: a trial by the
Eastern Cooperative Oncology Group. Blood. 2004;103:479–
485.
10. Mayer RJ. Two steps forward in the treatment of colorectal
cancer. N Engl J Med. 2004;350:2406–248.
11. Hoelzer D, Thiel E, Loffler H, et al. Prognostic factors in a
multicenter study for treatment of acute lymphoblastic
leukemia in adults. Blood. 1988;71:123–131.
12. Darmon M, Thiery G, Ciroldi M, et al. Intensive care in
patients with newly diagnosed malignancies and a need
for cancer chemotherapy. Crit Care Med. 2005;33:2488–
2493.
13. Brunet F, Lanore JJ, Dhainaut JF, et al. Is intensive care jus-
tified for patients with haematological malignancies? Inten-
sive Care Med. 1990;16:291–297.
14. Carlon GC. Admitting patients with cancer to the intensive
care unit. Crit Care Clin. 1988;4:183–191.
15. Schuster D, Marion JM. Precedents for meaningful recovery
during treatment in a medical intensive care unit. Out-
come in patients with hematologic malignancy. Am J Med.
1983;75:402–408.
16. Rubenfeld GD, Crawford SW. Withdrawing life support
from mechanically ventilated recipients of bone marrow
transplants: a case for evidence-based guidelines. Ann
Intern Med. 1996;125:625–633.
17. Guidelines for intensive care unit admission, discharge,
and triage. Task Force of the American College of Critical
Care Medicine, Society of Critical Care Medicine. Crit Care
Med. 1999;27:633–638.
18. Consensus statement on the triage of critically ill patients.
Society of Critical Care Medicine Ethics Committee. JAMA.
1994;271:1200–1203.
19. Lemeshow S, Teres D, Klar J, et al. Mortality probability
models (MPM II) based on an international cohort of in-
tensive care unit patients. JAMA. 1993;270:2478–2486.
20. Knaus WA, Wagner DP, Draper EA, et al. The APACHE III
prognostic system. Risk prediction of hospital mortality
for critically ill hospitalized adults. Chest. 1991;100:1619–1636.
21. Knaus WA, Draper EA, Wagner DP, Zimmerman JE.
APACHE II: a severity of disease classification system. Crit
Care Med. 1985;13:818–829.
22. Jaffe ES, Harris NL, Diebold J, Muller-Hermelink HK. World
Health Organization classification of neoplastic diseases of
the hematopoietic and lymphoid tissues. A progress report.
Am J Clin Pathol. 1999;111(1 Suppl 1):S8–12.
23. Siro CA, Bastos PG, Knaus WA, Wagner DP. APACHE II
scores in the prediction of multiple organ failure syn-
drome. Arch Surg. 1991;126:528–529.
24. Giacomini M, Cook D, DeJean D, Shaw R, Gedge E. Deci-
sion tools for life support: a review and policy analysis.
Crit Care Med. 2006;34:864–870.
25. Tremblay LN, Hyland RH, Schouten BD, Hanley PJ. Sur-
vival of acute myelogenous leukemia patients requiring
intubation/ventilatory support. Clin Invest Med. 1995;18:
19–24.
26. Epner DE, White P, Krasnoff M, et al. Outcome of mechani-
cal ventilation for adults with hematologic malignancy.
J Investig Med. 1996;44:254–260.
27. Thiery G, Azoulay E, Darmon M, et al. Outcome of patients
with cancer considered for intensive care unit admission: a
hospital-wide prospective study. J Clin Oncol. 2005;23:
4406–4413.
28. Rabbat A, Chaoui D, Montani D, et al. Prognosis of patients
with acute myeloid leukaemia admitted to intensive care.
Br J Haematol. 2005;129:350–357.
29. Aggarwal A, Ong JP, Younossi ZM, et al. Predictors of mor-
tality and resource utilization in cirrhotic patients admitted
to the medical ICU. Chest. 2001;119:1489–1497.
30. Gildea TR, Cook WC, Nelson DR, et al. Predictors of long-
term mortality in patients with cirrhosis of the liver
admitted to a medical ICU. Chest. 2004;126:1598–1603.
31. Wetzler M, Dodge RK, Mrozek K, et al. Prospective karyo-
type analysis in adult acute lymphoblastic leukemia: the
cancer and leukemia Group B experience. Blood. 1999;93:
3983–3993.
32. Bellamy E, Oye RK. Admitting elderly patients to the ICU:
dilemmas and solutions. Geriatrics. 1987;42:61–63, 67–68.
33. Rabe C, Mey U, Paashaus M, et al. Outcome of patients
with acute myeloid leukemia and pulmonary infiltrates
requiring invasive mechanical ventilation-a retrospective
analysis. J Crit Care. 2004;19:29–35.
34. Azoulay E, Alberti C, Bornstain C, et al. Improved survival
in patients with cancer requiring mechanical ventilatory
support: impact of noninvasive mechanical ventilatory
support. Crit Care Med. 2001;29:519–525.
35. Schapira DV, Studnicki J, Bradham DD, Wolff P, Jarrett A.
Intensive care, survival, and expense of treating critically ill
patients with cancer. JAMA. 1993;269:783–786.
2240 CANCER May 15, 2008 / Volume 112 / Number 10