Embed Size (px)
Citation preview

Survival Guide – FY1 – Part 2: Clinical 2017-18
Updated by Dr James Finnerty and Dr Tom MacDonagh (July 2017)
Contents INTRODUCTION ............................................................................................................................................... 2
USEFUL CONTACT DETAILS ............................................................................................................................... 3
USEFUL MEDICATIONS ..................................................................................................................................... 4
SEIZURES .......................................................................................................................................................... 5
MEDICAL EMERGENCY ..................................................................................................................................... 5
TRANSFUSION REACTION................................................................................................................................. 6
ANALPHYLAXIS ................................................................................................................................................ 8
AKI ................................................................................................................................................................... 9
ALCOHOL WITHDRAWAL................................................................................................................................ 11
DIABETIC KETOACIDOSIS AND SLIDING SCALE ................................................................................................ 15
HYPERKALAEMIA/HYPOKALAEMIA ................................................................................................................ 19
HYPERNATRAEMIA/HYPONATRAEMIA .......................................................................................................... 20
ELECTROLYTE REPLACEMENT TABLE .............................................................................................................. 21
END OF LIFE DRUGS ....................................................................................................................................... 22
TYPE 2 RESPIRATORY FAILURE ....................................................................................................................... 23
DELTEPARIN THERAPY ................................................................................................................................... 25
WARFARIN ..................................................................................................................................................... 27
ACUTE ABDOMINAL PAIN .............................................................................................................................. 28
ACUTE KIDNEY INJURY (AKI) .......................................................................................................................... 29
CARDIAC CHEST PAIN ..................................................................................................................................... 30
EXACERBATION OF COPD ............................................................................................................................... 31
NOF FRACTURE .............................................................................................................................................. 32
PNEUMONIA .................................................................................................................................................. 33
SEPSIS ............................................................................................................................................................ 34
STROKE .......................................................................................................................................................... 35
Introduction
Hello new FY1s!
This is a booklet we have put together with some pocket sized, useful points of reference
when first starting work, especially for on-call shifts.
Prescribing, being called to see sick patients, and being asked for advice in clinical situations
can be quite daunting at the beginning.
We have included information that we think we would have found helpful when we first
started, and hopefully this will give you just some quick hints and tips for some common
things you might encounter.
We have also included the hospital pathways that have been developed for some common
conditions, and which may help you with your initial assessment/management.
Don’t panic, good luck, and enjoy!
From the current FY1s (soon to be your FY2s!)

Useful contact details To bleep: Dial ‘50’ (you will hear two beeps) then the number you want to bleep (wait for another two beeps), then the number of the phone you are on (you will hear many beeps) Here is a list of some of the useful contacts you will need. It is not an exhaustive list. Other numbers including these can easily be found using the search section at the top of the Intranet homepage. If you cannot find a number, you can always go through switchboard by pressing “0”.
A&E X-ray 53400
Acute response team Bleep 600
Bereavement office 54417 / 53723
Blood Bank 53747/53746
Central X-ray 53657
Crash call 2222
CT & MRI 56619 (CT control room 53073)
Dietician 56777
Discharge team 55266
ECG Bleep 086 / 087
Echo 57735
Hospital security Bleep 728 / 5555
Medical staffing 53726
MHLT 55268 / 56841
Pathology 56950
Pharmacy 53784 / 54781
Pharmacy medicines information 53791
USS 56645
Vascular USS 56930

Useful medications
ANALGESICS ROUTE DOSE FREQ.
Buscopan PO/IV 10 – 20 Mg QDS
Co-Codamol (30/500) PO 1 – 2 Tabs QDS
Codeine Phosphate PO/IM 30 – 60 Mg QDS
Diclofenac PO/IM/PR 50 – 100 Mg TDS
Ibuprofen PO 200 – 400 Mg TDS
Morphine IV/PO 5 – 10 Mg STAT
Paracetamol PO/IV 500mg – 1g QDS
Tramadol PO 50 – 100 Mg QDS
GASTRIC REFLUX ROUTE DOSE FREQ.
Gaviscon PO 5 – 10 Ml TDS
Omeprazole PO 20 Mg OD
Ranitidine PO 150 Mg BD
LAXATIVES ROUTE DOSE FREQ.
Senna PO 15mg BD/TDS
Movicol PO 1-2 Sachets BD/TDS
Lactulose PO 15ml BD
Glycerine Suppository PR 4 gram (TT) STAT/PRN
Phosphate Enema PR T STAT/PRN
ANTI-EMETICS ROUTE DOSE FREQ
Cyclizine PO/IV/IM 50 Mg TDS
Domperidone PO 10 – 20 Mg QDS
Metoclopramide PO/IM/IV 10 Mg TDS
Ondansetron PO/IV/IM 8 Mg TDS
Prochlorperazine PO 10 – 20 Mg TDS
AGGITATION/AGGRESSION ROUTE DOSE
Diazepam PO 5-10mg

Seizures
MEDICAL EMERGENCY especially if lasting >5minutes
FIRST ASSESSMENT
ABCDE approach
AIRWAY – insert OP or NP airway, give o2
GLUCOSE – get BMs
Record timings (make sure someone does this if you
can’t)
Try to ensure patient is in safe environment – recovery
position etc
Patient Hx – known epileptic? Any evidence for cause in
notes (eg electrolytes, Alcohol dependence?)
IV access and bloods
IF >5 MINS
SENIOR help immediately
Give IV lorazepam 4mg IV over 2 mins or PR diazepam
10mg
Get advice re: phenytoin infusion - 15mg/kg IV at
50mg/min
Involve anaesthetics / ICU if not responsive to
treatments

Transfusion reaction
All Green
STOP the transfusion but leave connected. Re-check identity of the unit
with the patient, inform doctor. If all well, continue at reduced rate for the
next 30 minutes and then resume at prescribed rate. Continue to monitor
the patient carefully and be alert for other symptoms or signs of a
transfusion reaction. Anti-pyretics may be required.
1 or more Amber
STOP the transfusion but leave connected, request urgent clinical review,
re-check identity of the unit with the patient, give IV fluids. If symptoms
stable or improving over next 15 minutes consider restarting the unit.
Antihistamines and/or anti-pyretics may be required.
1 or more Red
STOP the transfusion and disconnect, request immediate clinical review, re-
check identity of the unit with the patient, give IV fluids, inform the
transfusion laboratory, contact the Consultant Haematologist.
NOTE: In all cases where a transfusion reaction is suspected and the transfusion is stopped and
disconnected, the implicated unit, complete with giving set, must be returned to the laboratory
for further investigation.
Follow your local transfusion policy and contact the transfusion laboratory for further instructions.

APPENDIX 1: TRANSFUSION REACTIONS - FOR GUIDANCE
Symptoms / Signs Mild Moderate Severe
Temperature
Temperature of >38oC
(Degrees Celsius) AND
rise of 1-2oC from
baseline temperature
Temperature of >39oC
OR a rise of >2oC from
baseline temperature
Sustained febrile
symptoms or any new,
unexplained pyrexia in
addition to clinical
signs
Rigors / shaking None Mild chills Obvious shaking/rigors
Pulse Minimal or no change
from baseline
Rise in heart rate from
baseline of 10 bpm or
more NOT associated
with bleeding
Rise in heart rate from
baseline of 20 bpm or
more NOT associated
with bleeding
Respirations Minimal or no change
from baseline
Rise in respiratory rate
from baseline of 10 or
more
Rise in respiratory rate
from baseline of 10 or
more accompanied by
dyspnoea/wheeze
Blood Pressure (Hypo
/ hypertension)
Minor or no change to
systolic or diastolic
pressure
Change in systolic or
diastolic pressure of
>30 mm/Hg NOT
associated with
bleeding
Change in systolic or
diastolic pressure of
>30 mm/Hg NOT
associated with
bleeding
Skin No change Facial flushing, rash
Urticaria, pruritis
Rash, urticaria and
Peri-orbital oedema
Conjunctivitis
Pain None
General discomfort or
myalgia
Pain at drip site
Acute pain in chest,
abdomen, back
Urine Clear
Normal output
Haematuria /
haemoglobinuria
Oliguria, Anuria
Bleeding No new bleeding Uncontrolled oozing
Nausea None Nausea or vomiting

Analphylaxis

AKI
This is a common condition that you will be expected to manage on a day-to-day basis. There is a hospital AKI pathway which is included in the pathways section of this booklet.
DEFINITION 1. Stage 1 - AKI stage 1 is a rise of >1.5x baseline creatinine level, or of >26umol/L within 48h, or a Urine output <0.5mg/kg/h for 6-12h.
2. Stage 2 - AKI stage 2 is a rise of >2x baseline creatinine or a urine output <0.5ml/kg/h for ≥12h
3. Stage 3 - AKI stage 3 is a rise of >3x baseline creatinine or
a rise of >1.5 to baseline to >354umol/L, a Urine output <0.3ml/kg/h for ≥24h or anuria for ≥12h
4. A laboratory comment will be attached to the report. This will include an AKI Stage e.g. STAGE (1or 2 or 3) ACUTE KIDNEY INJURY (AKI)
5. Please record the AKI stage in the case notes with the
creatinine value, and put in place a management plan
that is suitable for the severity of AKI.
COMMON CAUSES 1. Sepsis
2. Hypoperfusion
3. Medications
4. Obstruction
INVESTIGATIONS 1. Urinalysis, send msu
2. Fluid balance chart
3. May need a catheter to measure urine output
4. Input output chart
5. Bloods: U+E, FBC
6. ABG/ VBG looking for acidosis and hyperkalaemia
7. ECG (hyperkalaemia)
8. USS KUB (If you suspect obstruction)
INITIAL MANAGEMENT 1. Check the catheter isn’t blocked
2. Fluid challenge 500ml crystalloid stat, measure response
by urine output, bp
3. Treat underlying infection (remember to use renal dose
of tazocin and gentamicin)
4. Avoid nephrotoxic drugs
5. Treat hyperkalemia


Alcohol withdrawal
Complete the Audit C in admissions clerking, if score 8-12 inform alcohol liaison.
Look out for anxiety, fine tremor, sweating, vomiting, headache, insomnia,
tachycardia, hallucinations and fits.
They will advise you regarding
IV vitamins:
o pabrinex ( 2x (I +II), IV, TDS for 3-5 days)
oral vitamins:
o thiamine (100mg, PO, TDS)
o Folic acid (5mg, PO, OD)
Chlordiazepoxide:
o PRN chlordiazepoxide (10-30mg depending on patient needs) VS fixed dose
reducing regime of chlordiazepoxide (see tables below)
Can use PRN haloperidol or lorazepam **doses are different.
MONITOR:
patient’s vital signs
level of alertness
fluid intake
Watch out for wernickes encephalopathy, caused by thiamine deficiency
Symptoms can develop acutely or over a few days
Triad of confusion, cerebellar ataxia and ocular palsies.
Can be accompanied by apathy, drowsiness, disorientation and amnesia.
Can develop into a coma.

Table 1: Chlordiazepoxide reducing dose regimen under 65 or with severe withdrawal
Day (1) 30 30 30 30 = 120mg total
Day (2) 30 20 20 30 = 100mg total
Day (3) 20 20 20 20 = 80mg total
Day (4) 20 10 10 20 = 60mg total
Day (5) 10 10 10 10 = 40mg total
Day (6) 10 0 0 10 = 20mg total
Day (7) STOP
Consider PRN Chlordiazepoxide 20mg - 30mg for breakthrough AWS symptoms
Table 2: Chlordiazepoxide reducing dose regimen in patients over 65 or patients with significant co-morbidities
Day (1) 20 20 20 20 = 80mg total
Day (2) 20 10 10 20 = 60mg total
Day (3) 10 10 10 10 = 40mg total
Day (4) 10 5 5 10 = 30mg total
Day (5) 5 5 5 5 = 20mg total
Day (6) 5 0 0 5 = 10mg total
Day (7) STOP
Consider PRN Chlordiazepoxide 10mg - 20mg for breakthrough AWS symptoms.
NB Patients with Hepatic Impairment and Renal Impairment – Consideration should be given to the
use of benzodiazepines with shorter half lives and under caution. Start with smaller initial doses and
avoid use in severe hepatic impairment.



Diabetic ketoacidosis and sliding scale Definition
1. Capillary blood glucose above 11 mmol/L OR known case of Diabetes* 2. Capillary ketones above 3 mmol/L or significant urine ketones ++ or more 3. Venous pH less than 7.3 and / or venous bicarbonate less than 15 mmol/L
Summary of DKA Management
Time Fluid Insulin
0-60 min 0.9% sodium chloride 1000 mL/hour
(If systolic BP below 90mmHg then first start on 500
– 1000 mL of 0.9% sodium chloride solution over 10-
15 minutes and then as above)
1. A fixed rate intravenous
insulin infusion (FRIII)
(0.1unit/kg/hr based on
estimate of weight)
2. If patient normally takes long
acting insulin analogue
continue at usual dose and
time
60 min - 6
hour
0.9% sodium chloride 1L with potassium chloride over next 2 hours**
0.9% sodium chloride 1L with potassium chloride over next 2 hours**
0.9% sodium chloride 1L with potassium chloride over next 4 hours
Add 10% glucose 125mL/hr when blood glucose falls below 14mmol/L but continue on 0.9% sodium chloride infusion
Continue insulin as above
6 – 12
hour
0.9% sodium chloride 1L with potassium chloride over 4 hours**
0.9% sodium chloride 1L with potassium chloride over 6 hours**
Add 10% glucose 125ml/hr when blood glucose falls below 14 mmol/L but continue on 0.9% sodium chloride infusion
Continue insulin as above
12- 24
hour
Continue IV fluid replacement if not eating and drinking
If ketonaemia cleared but
patient is not eating and
drinking (unusual) move to a
variable rate IV insulin infusion
After 24 hour DKA should have resolved. Transfer to subcutaneous insulin if patient is eating and
drinking normally.
** KCL replacement

Potassium level in first 24 hours
(mmol/L)
Potassium replacement in
mmol/L of infusion solution(KCL)
> 5.5 nil
3.5 - 5.5 40 *
< 3.5 Additional KCL required, senior review
* Use ready-mixed 0.9% sodium chloride with potassium 40mmol/L
Resolution of DKA is confirmed by:
1. Capillary ketones less than 0.6 mmol/L and venous bicarbonate greater than
15mmol/L,
2. Venous pH over 7.3
Once DKA is resolved, change FRIII to Variable Rate Intravenous Insulin Infusion (VRIII) and 10%
Dextrose at 125mL/hr until patient is able to eat and drink.
(To make up VRIII, add 50 units Actrapid® (soluble insulin) made up to 50ml with 0.9% sodium
chloride solution in a 50ml syringe).
Restart patient’s usual insulin regime i.e. S/C injection of quick acting insulin (e.g. Novorapid®,
Humalog® or Apidra®) with their next meal or mixed insulin (e.g. Novomix30®) with either breakfast
or tea. Then stop VRIII and 10% Dextrose infusion 30-60 minutes after the administration of the
S/C insulin given in association with a meal.
Expectation: Patient should be eating and drinking and back on normal insulin regimen. If DKA not
resolved identify and treat the reasons for failure to respond. This situation is unusual and requires
senior and specialist input.
Action 1
Transfer to pre-existing
subcutaneous insulin regime
Convert to S/C insulin regime when biochemically stable (capillary
ketones less than 0.6 mmol/L, pH over 7.3) and patient able to eat
and drink.
Do not discontinue intravenous insulin infusion until 30-60 minutes
after subcutaneous insulin has been given.
Ensure referral has been made to Diabetes Specialist Nurses for
patient re-education to prevent subsequent admission with DKA.



Hyperkalaemia/Hypokalaemia Hyperkalaemia
K+ >5.6 is hyperkalaemic
K+ > 7.0 or >5.6 WITH ECG changes requires immediate treatment
ECG CHANGES Tall tented T waves
Flattened P waves
Widened QRS
Arrhythmias
INITIAL Mx ABCDE assessment
Ensure you have venous access
Review patient history (is this new? / explained by conditions or medications?)
Exclude life threatening causes: renal failure, tissue necrosis, acidosis
Stop any relevant medications (k+ sparing diuretics etc)
INVESTIGATIONS URGENT repeat U&Es
Blood gas for pH
ECG and consider cardiac monitoring if abnormal
ACUTE TREATMENT 10mls of 10% calcium gluconate IV over 2 minutes: to stablise cardiac activity (repeat ECG after this)
Salbutamol nebs 5mg : drive K into cells
Insulin-dextrose infusion : drive K into cells 10 units actrapid in 50mls of 50% glucose over 10 minutes
TREATMENT Calcium resonium 15g PO : removes excess K from body Onset of action is 2 - 12 hours
Also remember to make a senior aware and get help whenever you feel you aren’t managing Hypokalaemia K+ <3.0 is hypokalaemia K+ <2.5 or <3 WITH ECG CHANGES requires treatment.
ECG CHANGES Arrhythmias
Long PR interval
ST depression
TREATMENT Replacement of K+ - see table for doses

Hypernatraemia/Hyponatraemia
Sodium levels >145 or <135
Very common, especially hyponatraemia
IMPORTANT FEATURES Drowsiness
Decreased GCS or haemodynamic instability
Can cause SEIZURES
INVESTIGAIONS
Important to assess volume status – hypovolaemic, euvolaemic or overloaded?
Usually caused by: o fluid loss (diuretics, vomiting/diarrhoea) o or excess (Check what IV fluids are being given) e.g
diluted through excess fluid or hypernatraemic from too much 0.9% saline
Get repeat U&Es
MANAGEMENT
For HYPERNATRAEMIA o fluid replacement to correct Na+ slowly, dependent
on volaemic state
For HYPONATRAEMIA o treatment depends on volaemic status, get senior
advice if you are not sure
If for sodium replacement remember this should be done slowly.
Most patients will need daily bloods to monitor U&Es
Oxford handbooks (medicine and foundation programme) have helpful sections on this

Electrolyte replacement table
Appendix 2: Correction of Low Electrolytes
Electrolyte
Level Oral IV
Potassium 3.0 – 3.5 Sando K 1 tds
(12mmol/tablet)
20mmol KCL in 1 litre 0.9% NaCl over 8 hours
Potassium 2.5 – 2.9 Sando K 2 - 3 tds (12mmol/tablet)
40mmol KCL in 1 litre 0.9% NaCl over 8 hours
Potassium < 2.5 Sando K 3 – 4 tds (12mmol/tablet)
40mmol KCL in 1 litre 0.9% NaCl over 4 hours
RETEST before giving more as needed
Magnesium 0.51 – 0.70 Magnaspartate 1 sachet
BD (1 sachet 243mg =10mmols of Mg)
8mmol (2g) MgSO4 in 100ml 0.9% NaCl over 3 hours
Magnesium ≤ 0.50 Magnaspartate 1 sachet
BD (1 sachet 243mg =10mmols of Mg)
12mmol (3g) MgSO4 in 100ml 0.9% NaCl over 3 hours
Phosphate ≤ 0.80 Phosphate Sandoz
2 tds ( 16mmol each)
7.5ml/hr over 12 hours of phosphate polyfusor (9mmol)
NB: These are guidelines for initial doses to be given. Prior to further supplementation electrolytes should be checked, perhaps more than once per day if required. IV is always the preferred route for correction for patients with very low electrolyte levels or patients at high risk of RFS

End of life drugs

Type 2 Respiratory Failure
T2RF is hypoxia (o2 < 8) with hypercapnoea (CO2 >6)
Common condition among patients with COPD particularly but can occur in other
respiratory disease. Some COPD patients have chronic T2RF (and so pH will be normal) but
pH <7.35 IN ANY PATIENT (RESP ACIDOSIS) IS DANGEROUS AND REQUIRES IMMEDIATE
ACTION.
In ANY unwell patient with shortness of breath, be aware of:
Cyanosis
Drowsiness / reduced GCS / acute confusion
Unexplained increase in o2 requirement
Tachycardia
ASSESSMENT ABCDE approach
Especially look for signs of pneumothorax, DVT/PE and
cardiac failure
Establish if there is a history of respiratory disease
(especially hx of home oxygen use, previous T2RF and
previous ICU admissions)
INVESTIGATIONS Obtain an URGENT ABG
samples are usually sent to the lab on ice, in a medical
emergency there is a blood gas machine on AMU – ask
politely!
ECG
CXR
Bloods – FBC, U&Es, CRP
MANAGEMENT (if find T2RF on ABG)
Controlled o2 therapy is first line – reduce oxygen as
much as possible (e.g to 1L via nasal cannulae) aim for
sats between 88-92%
INVOLVE A SENIOR EARLY these patients can become
very unwell very quickly.
Consider need for Non Invasive Ventilation (bi-pap)
- this is a senior decision
Repeat ABGs 1 hour after any change to oxygen or NIV


Delteparin therapy Dalteparin Treatment Dose for Adults (Non-Pregnant) with Venous Thromboembolism
Body Weight (kg) Dalteparin Dose (units) Once a day
Subcutaneous (s.c) dose
Under 46 7,500
46 – 56 10,000
57 – 68 12,500
69 – 82 15,000
83 and over 18,000
The single daily subcutaneous dosage should NOT exceed 18,000 units

Dalteparin Dose is Dependent on the Patient’s Renal Function:
As Dalteparin is renally excreted, it must be used with caution in patients with reduced renal function
A renal function test should not delay initiation of the first dose but every effort must be made to base subsequent doses on the result
The Serum Creatinine level should not be used to estimate renal function
A Creatinine Clearance (Cr Cl) must be calculated o If the estimated CrCl is less than 30ml/min, then the prescriber must contact
the on-call Consultant Haematologist for advice
Monitoring anti-Xa levels may be required or the use of an alternative product such as unfractionated heparin
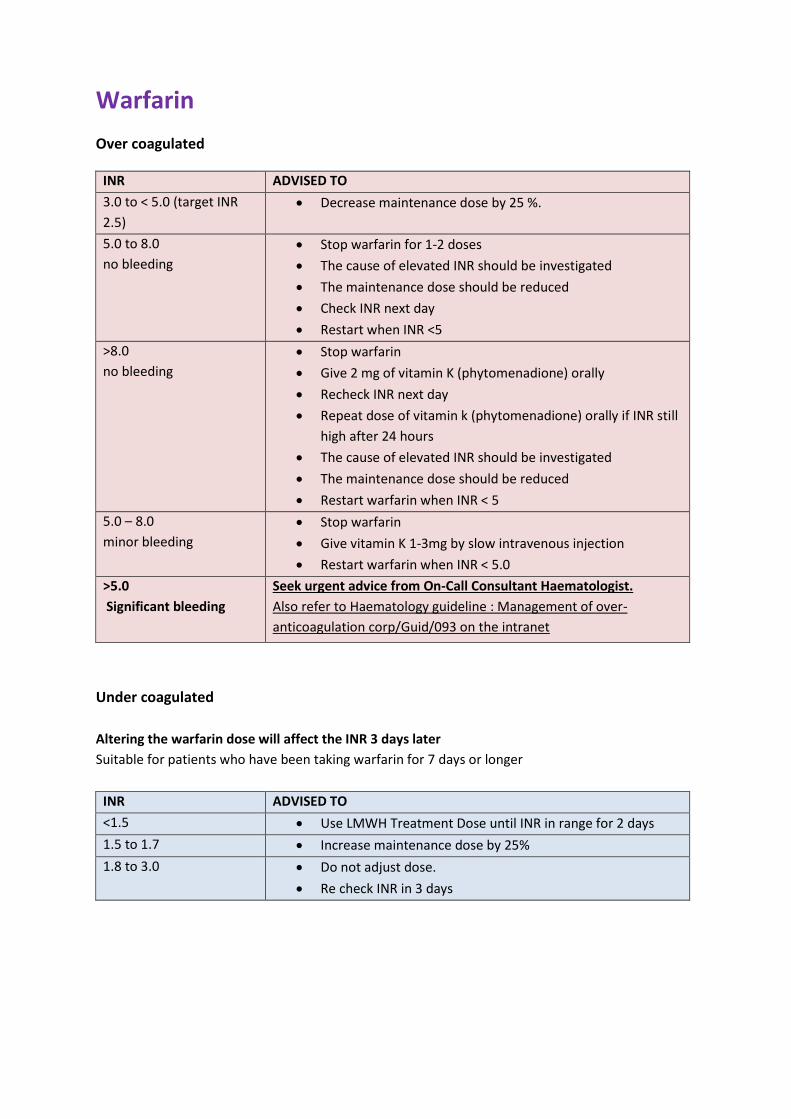
Warfarin
Over coagulated
INR ADVISED TO
3.0 to < 5.0 (target INR
2.5)
Decrease maintenance dose by 25 %.
5.0 to 8.0
no bleeding
Stop warfarin for 1-2 doses
The cause of elevated INR should be investigated
The maintenance dose should be reduced
Check INR next day
Restart when INR <5
>8.0
no bleeding
Stop warfarin
Give 2 mg of vitamin K (phytomenadione) orally
Recheck INR next day
Repeat dose of vitamin k (phytomenadione) orally if INR still
high after 24 hours
The cause of elevated INR should be investigated
The maintenance dose should be reduced
Restart warfarin when INR < 5
5.0 – 8.0
minor bleeding
Stop warfarin
Give vitamin K 1-3mg by slow intravenous injection
Restart warfarin when INR < 5.0
>5.0
Significant bleeding
Seek urgent advice from On-Call Consultant Haematologist.
Also refer to Haematology guideline : Management of over-
anticoagulation corp/Guid/093 on the intranet
Under coagulated
Altering the warfarin dose will affect the INR 3 days later
Suitable for patients who have been taking warfarin for 7 days or longer
INR ADVISED TO
<1.5 Use LMWH Treatment Dose until INR in range for 2 days
1.5 to 1.7 Increase maintenance dose by 25%
1.8 to 3.0 Do not adjust dose.
Re check INR in 3 days

Acute Abdominal Pain

Acute Kidney Injury (AKI)

Cardiac chest pain

Exacerbation of COPD

NOF fracture

Pneumonia

Sepsis

Stroke