Embed Size (px)
Citation preview

Take II: Factors Related to Recruitment and Retention of Primary Care Physicians at Community Health
Centers post MA Health Care Reform:Results from 2008 and 2013Statewide Physician Surveys
APHA Annual MeetingNew Orleans, LANovember, 2014
Judith A. Savageau, MPHUMass Medical School

Presenter Disclosure
No members of the project team have any relationships to disclose
2

Project Team
• MA League of Community Health Centers (MLCHC)
– Joan Pernice, Leslie Bailey
• MassAHEC Network, UMass Medical School (UMMS)
– Linda Cragin
• UMMS Department of Family Medicine & Community Health
– Warren Ferguson
• UMMS Center for Health Policy and Research (CHPR)
– Judy Savageau, Laura Sefton
3

Background and Significance
Health care reform, in Massachusetts and nationally, has increased the number of patients utilizing public or private health insurance to seek care.
•Newly-insured patients are expected to continue to seek care in Community Health Centers (CHCs), which act as medical homes for underserved or uninsured populations , offering a range of, and easy access to, high-quality coordinated services in one setting.
•Existing and predicted shortages of primary care providers (PCPs) in an environment of rising need will reduce access for vulnerable populations.
4

Background and Significance
Training and preparing medical students and residents to be PCPs skilled in providing culturally-appropriate care to underserved populations has never been more important.
•CHCs find it challenging to recruit and retain physicians, leading to staff shortages.
•Primary care training in a CHC prepares students and residents to work with vulnerable populations, increasing the likelihood of practicing in a CHC setting.
•Insights into the values of the current CHC PCP workforce can guide educational priorities.
5

Study Objectives
• In 2008, UMMS, MassAHEC, and MLCHC surveyed CHC PCPs to:
– characterize the workforce;
– identify factors related to preparedness, recruitment and retention; and
– correlate satisfaction with organizational improvement efforts.
• Survey repeated in 2013 to determine the impact of Massachusetts health care reform.
6

Methods
• Sample frame: 2013 list from MLCHC members (N=677 providers with email addresses)
• Mailing intended to survey primary care physicians only (excluded: residents, PAs, NPs and specialists)
• Emailed link with URL to SurveyMonkey web-based survey to all providers with…
– 2 email reminders to physicians
– final follow-up reminder to CHC Medical Directors from the MLCHC
7

Methods
• 30-item survey:– Physician demographics and practice characteristics– Medical education and residency training– Past and current participation in loan repayment programs– Preparedness to practice in a CHC– Factors related to the process of selecting a CHC practice setting– Satisfaction with current practice arrangement– Retention strategies within the CHC– Future practice plans
• New questions added to baseline (2008) survey, e.g.:– integrated care– multidisciplinary team-based care– language competencies
8

Methods
• Data analysis: SAS V9.13; univariate, bivariate and multivariate statistics computed
• Factor analyses used to create domain scores• for example… compensation/benefits pkg/CMEs;
opportunities to do QI/administration/project leadership; and patient diversity/CHC mission
9

Results – Response Rates
• Response rate in 2008: 58% (294/505)• Responses received from providers at 46 CHCs• Response rates per CHC ranged from 29% - 100%
• Response rate in 2013: 48% (301 of 629 usable surveys)• Responses received from providers at 44 CHCs• Response rates per CHC ranged from 8% - 100%
10

Demographic and Practice Characteristics
11
Table 1. Frequency, percent distributions and descriptive statistics of study sample sociodemographic and practice characteristics; N=301, 2013.
Study Sample*
n (%)
Sociodemographic Characteristics
Gender
Male
Female
106 (38.3%)
171 (61.7%)
Age group
Under 40 years
40-49 years
50-59 years
60+ years
Range
Mean (SD)
78 (30.4%)
79 (30.7%)
59 (23.0%)
41 (16.0%)
30-79 years
46.9 (10.8)
Years in practice
Less than 10 years
Less than 5 years
5-9 years
10+ years
Range
Mean (SD)
103 (39.0%)
[58; 22.0%]
[45; 17.0%]
131 (61.0%)
<1-51 years
14.9 (11.1)
Race
White
Non-White
Decline to state
193 (70.2%)
61 (22.2%)
21 (7.6%)
Ethnicity
Not Hispanic or Latino
Hispanic or Latino
Decline to state
230 (83.3%)
27 (9.8%)
19 (6.9%)
Number of non-English languages spoken in clinical practice
0
1
2
3+
80 (26.6%)
148 (49.2%)
48 (15.9%)
25 (8.3%)

Demographic and Practice Characteristics
12
Practice Characteristics
CHC Region of Massachusetts
Boston
Northeast
Southeast
Cape/Islands
Central
West
165 (54.8%)
61 (20.3%)
19 (6.3%)
11 (3.7%)
28 (9.3%)
17 (5.6%)
Specialty
Family Medicine
Internal Medicine
Pediatrics (including Med-Peds)
OB/GYN
121 (40.9%)
99 (33.4%)
67 (22.6%)
9 (3.0%)
Year of hire at current CHC
< 5 years ago
5+ years ago
< 10 years ago
10+ years ago
< 20 years ago
20+ years ago
104 (35.9%)
186 (64.1%)
168 (57.9%)
122 (42.1%)
245 (84.5%)
45 (15.5%)
Current employment status
Part-time at this CHC (< 25 hrs/wk)
Full-time at this CHC (25+ hrs/wk)
91 (30.6%)
206 (69.4%)
Visa/Loan repayment program participation
None
1 current/former participants
2+ current/former participants
161 (53.5%)
114 (37.9%)
26 (8.6%)

Provider / Practice Characteristics
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
In 2013, MD ages ranged from 30-79 yrs (Mean: 47 yrs).Older PCPs were significantly more likely to be: working PT, non-FM MDs, white, and at their current CHC more than 10 yrs. Age was not significantly associated with provider gender.
13

Provider / Practice Characteristics
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
In 2013, one-half of respondents speak 1 additional non-English language, and 24% speak 2+ non-English languages. PCPs in 2013 were significantly more likely to speak additional non-English languages compared to respondents in 2008.
14
****p<.001

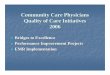
Provider / Practice Characteristics
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301
In 2013, 86% of MDs with foreign language skills reported speaking Spanish fluently enough to conduct a new patient history and physical exam with a patient compared to 76% in 2008.
None 27%
Spanish 63%
Portuguese 9%
French 6%
Hindi 5%
Haitian Creole 5%
Arabic 4% Cape Verdean 4% Vietnamese 3% Chinese 2% Urdu 2%
Russian 2%
Gujarati, Khmer, Korean <1%
• MDs in the < 40 yrs and 50-59 yrs age groups were more likely to report speaking 1 additional non-English language. However, providers 40-49 yrs were significantly more likely to report speaking 2+ additional non-English language.
• Female providers were more likely to speak 1 additional language while male providers reported speaking 2+ additional languages.
• White providers were more likely to speak 1 additional language while non-white providers were significantly more likely to report speaking 2+ languages.
• Hispanic providers were significantly more likely to report speaking 1 additional non-English language.
15

Preparedness Following Residency Training
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
Compared to 2008, PCPs responding in 2013 rated themselves as being significantly more prepared to practice in a CHC, work with underserved populations, and work with MassHealth insurance.
16
**p<.05

Factors Related to Recruitment
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
Of comparable questions asked in both 2008 and 2013, only ‘I needed to serve out a loan/visa obligation’ was significantly different (higher) in 2013 among factors important to PCPs in their initial considerations of working in a CHC.
17
****p<.001

Interviewing Factors Important in Hiring
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
Compared to 2008, PCPs were significantly more likely to rate ‘meeting professional needs’, ‘understanding community of pts to be served’ and ‘acceptance of loan/visa program’ as important in the interviewing process. However, touring the CHC’s local community/neighborhood was significantly less important to PCPs in 2013.
18
*p<.10; **p<.05; ***p<.01

Factors Important to Joining CHC
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
Among the many differences between 2008 and 2013, the most significant increases in importance of factors related to joining their current CHC were ‘benefits package’, ‘continuing medical education benefits’, and ‘total compensation’.
19
*p<.10; **p<.01; ***p<.001

Satisfaction with Current Practice Arrangement
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
Similar to factors important in joining their current CHC, PCPs in 2013 were significantly more satisfied with many factors compared to 2008; key among them were ‘benefits package’, ‘CME benefits’, ‘total compensation’, and ‘opportunities to participate in research’.
20
*p<.10; **p<.05; ***p<.01; ****p<.001

Retention Factors Identified as Important
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
Many factors were deemed ‘important’ by MDs – some increasing in importance from 2008 to 2013 and some decreasing in importance. Among those of significance in increased importance was: ‘support staff or other operational support’. Of significance in decreased importance was ‘addition or increase in mid-level providers’. ‘pension plan availability’, and ‘flex-time/job sharing’.
21

Provider Retention in Five Years
Source: Statewide Surveys of PCPs in MA CHCs: October, 2013; N=301 and May, 2008; N=294
There were few differences in planning for the next 5 years between the 2 study cohorts. Only intent to retire was significantly higher in 2013 compared to the 2008 group of MDs.
22

Multivariate Models Predicting Likelihood of Continuing to Practice in a CHC in Next 5 Years
Multivariate (mixed-method) regression models run for:
•All participants
•All participants, excluding those most likely to retire in next 5 years
•All participants, excluding those most likely to retire in next 5 years and 60+ years of age
•Participants in current practice < 10 years vs 10+ years
•Participants in current practice 10+ years, excluding those 60+ years of age
•Participants in Boston-based vs non Boston-based CHCs23

Multivariate Models Predicting Likelihood of Continuing to Practice in a CHC in Next 5 Years
24
Mixed model regression results assessing factors important to PCPs remaining in a CHC clinical setting in the next 5 years – Total Population, N=301, 2013. Independent variables Beta estimate (SE) p value
Age group
< 40 years
40-49 years
50-59 years
60+ years
2.3014 (.7781)
1.8884 (.5944)
2.2513 (.5926)
Referent group
.0035
.0017
.0002
Years out of residency training
< 10 years
10+ years
-1.5249 (.5852)
Referent group
.0098
Speak additional Non-English languages in practice
0 additional languages spoken
1+ additional languages spoken
-0.7955 (.4065)
Referent group
.0531
Research and teaching opportunities as an important factor when first considering CHC practice (lower score = greater importance)
-0.2340 (.0848) .0069
Compensation as an important factor when making decision to join CHC (lower score = greater importance)
0.1784 (.0719) .0139
Satisfaction with CHC model of care and morale of colleagues at current CHC practice (lower score = greater satisfaction)
-0.1612 (.0768) .0375
Satisfaction with recognition and mentoring at CHC practice (lower score = greater satisfaction)
-0.1459 (.0508) .0045

Multivariate Models Predicting Likelihood of Continuing to Practice in a CHC in Next 5 Years
Overall, physicians who were more likely to report intent to remain in a CHC environment were more likely to:•be younger;•be in practice for 10+ years;•speak at least one non-English language;•report greater importance for research and teaching opportunities when first considering the CHC as a practice setting;•report less importance regarding compensation when making the decision to join their current CHC;•report increased satisfaction with the CHC model of care and the morale of their colleagues; and•report increased satisfaction with recognition of their professional development, clinical practice goals, and overall work (plus having a mentor and receiving regular feedback).
25

Limitations
• Self-reported information; potential under- or over-reporting of perceptions of preparedness for practice, importance of recruitment strategies, satisfaction with current practice, anticipated changes in practice, etc.
• ~ 50% response rate; limited data to assess non-response bias
• One state: MA; may not be generalizable
26

Discussion
• When asked, in an open-ended fashion, whether there were any additional comments the PCP would like to share with use about recruitment and/or retention issues, the many comments (n=70) received were grouped into several categories:
Administration Compensation and Benefits
Workload Loan repayment
Mission CHC structure and systems
Support staff Resources
Lifestyle Professional development
Morale Residency training27

Discussion – Provider Quotes Regarding Recruitment/Retention
• [PREPARATION] “I think exposure to primary care and CHC settings need to start earlier in a person's medical career. We need more exposure to CHC settings for medical students and residents, more participation for residents with QI projects at CHC and exposure to medical home/team-based care initiatives - so students and residents can see how rewarding, challenging and exciting it is to practice primary care at a CHC. Students and residents see so easily how exciting the hospital is and we need to infuse the same experience at CHCs.”
28

Discussion – Provider Quotes Regarding Recruitment/Retention
• [RECRUITMENT] “I fulfilled a four-year NHSC scholarship obligation at a CHC in [another state]. That experience nearly burned me out and I left for private practice... I am now once again working at a CHC because I believe in the mission and I desire to work with the underserved. My current practice is a much saner place - the workload is more reasonable and I'm working part-time and creating my own work-life balance. I still haven't decided if I'll remain here...my next move may very well be to leave medicine entirely.”
29

Discussion – Provider Quotes Regarding Recruitment/Retention
• [RETENTION] “After working 20 years for the same CHC, I think there are many dedicated, extremely bright and talented physicians and compensation and lack of good support make retention an ongoing difficult problem. I think that if compensation cannot be better, then efforts should be made to make support better so that a choice to work in a CHC can offer good support and the perk of a good work/home life balance.”
30

Conclusions
Outcomes from 2008 and 2013 indicate opportunities to better prepare medical students and residents for careers in CHCs and recruit, retain and replace this vital and aging workforce.
•Exposure to CHCs during and throughout training fosters social commitment.
•Physician success, i.e. their retention, is dependent upon a competent, interprofessional clinical support team.
•A menu of options – teaching, policy and procedure development, research, etc. also contributes to retention.
31

Commitment is Not Enough
While commitment to underserved populations served by CHCs is strong, equally important is:
• maintaining a work/life balance;
• professional development in light of new models of interprofessional care; and
• addressing compensation.
To attract and maintain younger physicians as older physicians retire will be challenging as overall fewer young physicians are choosing primary care.
32

Impact of MA Healthcare Reform
• In a state with a media-purported large supply of primary care physicians, health reform has come to demonstrate a clear imbalance of primary care access.
• As the main provider of the medical home for Massachusetts underserved and uninsured individuals, CHCs are at the forefront of health reform implementation; its success or failure is partly dependent upon CHCs’ ability to meet the rising need for health services for the newly insured.
• The recruitment and retention of primary care physicians has never been more important!
33

And in closing…
“For me, the most important things are that the board is over half patients and also the mission, and flexibility of schedule and work type. Over the years, I have been privileged to have had the opportunity to do clinical work, then administrative and teaching work as well, and now am back to mostly clinical work. What a place! All sorts of things to do, and a lot of sensitivity to the life needs of the clinicians as well.”
34

Contact Information
For more information, please contact either:Judy Savageau, [email protected](774) 442-6535
Linda Cragin, [email protected].(508) 856-4303
35