Embed Size (px)
Citation preview
Central European Journal of Medicine
* E-mail:[email protected]
Tako-Tsubo syndrome: A diagnostic challenge
1 Department of Neurology, University Hospital Center Zagreb, HR - 10000 Zagreb, Croatia
2 Department of Cardiology, Hospital for Medical Rehabilitation Krapinske Toplice, HR - 10000 Zagreb, Croatia
Darija Mahovic1, Nenad Lakusic2*, Valentina Slivnjak2
Letter to Editor
Received 8 November 2008; Accepted 12 February 2009
We have read with interest the article of Atanassova et al. [1] published in your respected Journal about electrocardiographic (ECG) changes during the acute phase of subarachnoid hemorrhage; which encouraged us to replay with regard to this subject.
Tako-Tsubo Syndrome (TTS), or stress cardiomyopathy, is an entity of unknown etiology and pathophysiology that manifests with sudden, severe chest pain and/or dyspnea. It is generally triggered by emotional or physical stress, and most instances are reported in postmenopausal women. ECG changes are similar to acute myocardial infarction with ST-elevation (STEMI); laboratory markers of myocardial lesion are usually mild to moderately high; and coronarography shows no significant pathomorphological changes in the coronary arteries. Ventriculography and echocardiography show reversible akinesis and ballooning of the left ventricle apex with reduced ejection fraction that normalizes within 2 to 4 weeks [2,3]. In this syndrome, the left ventricle of a patient takes the shape of an octopus trap [4].
The main trigger of the complex pathophysiological mechanism that instigates TTS is stress. High catecholamine plasma level as a result of stress-induced sympathetic hyperactivity affects the cardiomyocytes of the left ventricle by b adrenoreceptors, and a complex chain of intracellular second signals [5,6].
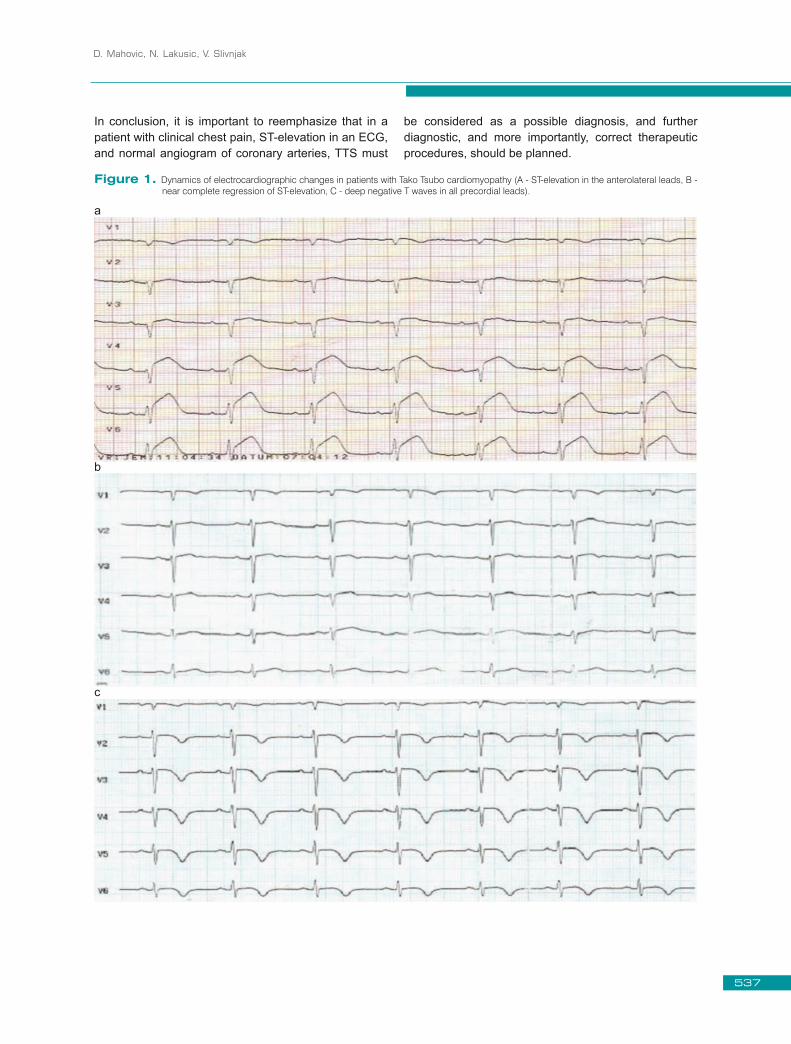
The main symptom of TTS is sudden, severe chest pain and/or dyspnea, but it can also manifest with cardiogenic shock, syncope, or malignant heart arrhythmia [3]. ECG changes are similar to acute myocardial infarction with ST-elevation, significant ST-segment elevation most often reported in precordial leads. ST-segment elevation usually persists for a few hours and then becomes isoelectric. After some time,
ECG shows a deep negative T wave, usually in all precordial leads, that can persist for a few months from the initial symptoms (Figure 1) [6,7]. For diagnosis of “real” TTS, some criteria must be applied. According to the Mayo Clinic, they are as follows: ECG changes similar to STEMI; absence of obstructive coronary artery disease; transient akinesis or dyskinesis of the left ventricle walls; absence of any kind of head trauma; intracranial bleeding; pheochromocytoma; and any other existing cardiomyopathy [4]. Presence of only some of the previously mentioned exclusion criteria is not sufficient to define “real” TTS, but rather a Tako-Tsubo–like cardiomyopathy (TTS-like). TTS-like cardiomyopathy is most often reported in subarachnoid hemorrhage after an aneurysm rupture [8]; it is also involved in any kind of central nervous system injury [9].
Recently, we had a case of TTS complicated by a secondary massive intracranial bleeding [7].
Tako-Tsubo is a rare syndrome [3,10] that in its overall clinical presentation simulates acute STEMI, and can be misdiagnosed as such. The importance is of this misdiagnosis is that the patient might be treated with extensive antithrombotic and/or anticoagulant therapy, which can then lead to severe, sometimes fatal, bleeding. TTS by itself does not require any specific treatment unless it develops into cardiogenic shock and/or malignant arrhythmia; it usually has a good prognosis. According to several reports, the in-hospital mortality rate is very low: about 1% [3]. There is an additional hazard accompanying misdiagnosis: if the patient with TTS comes to an institution where it is not possible to perform coronarography and cannot be transported to a tertiary PCI centre, that patient is a candidate for fibrinolytic therapy if contraindications are not present. This misapplied treatment can have a fatal outcome.
Cent. Eur. J. Med. • 4(4) • 2009 • 536-538DOI: 10.2478/s11536-009-0030-9
536
D. Mahovic, N. Lakusic, V. Slivnjak
In conclusion, it is important to reemphasize that in a patient with clinical chest pain, ST-elevation in an ECG, and normal angiogram of coronary arteries, TTS must
be considered as a possible diagnosis, and further diagnostic, and more importantly, correct therapeutic procedures, should be planned.
Figure 1. Dynamics of electrocardiographic changes in patients with Tako Tsubo cardiomyopathy (A - ST-elevation in the anterolateral leads, B - near complete regression of ST-elevation, C - deep negative T waves in all precordial leads).
a
c
b
537
Tako-Tsubo syndrome: A diagnostic challenge
References
[1] Atanassova P.A., Tokmakova M.P., Djurkova A.A., Naydenov V., Chalakova N.T., Dimitrov B.D., Abnormal ECG patterns during the acute phase of subarachnoid hemorrhage in patients without previous heart disease, Cent. Eur. J. Med., 2006, 1, 148-157
[2] Buchholz S., Rudan G., Tako-tsubo syndrome on the rise: a review of the current literature, Postgrad. Med. J., 2007, 83, 261- 264.
[3] Gianni M., Dentali F., Grandi A.M., Sumner G., Hiralal R., Lonn E., Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review, Eur. Heart. J., 2006, 27, 1523 – 1529
[4] Fricker J. Cardiologists search for the answer to the riddle of the octopus bottle, ESC Science News, www.escardio.org/vpo/News/Scientific/wcc-tako-tsubo-syndrome-feature
[5] Lyon A.R., Rees P.S.C., Prasad S., Poole-Wilson P.A., Harding S.E., Stress (Takotsubo) cardiomyopathy – a novel pathophysiological hypothesis to explain catecholamine – induced acute myocardial stunning, Nat. Clin. Pract. Cardiovasc. Med., 2008, 5, 22-9
[6] Stollberger C., Finsterer J., Schneider B., Transient left ventricular dysfunction (tako-tsubo phenomen): Findings and potential pathophysiological mechanisms, Can. J. Cardiol., 2006, 22, 1063-1068
[7] Slivnjak V., Lakusic N., Richter D., Cerovec D., Stress cardiomyopathy with ST-segment elevation of the anterolateral location complicated by a secondary massive intracranial bleeding, Int. J. Cardiol., 2008, Aug 14 [ahead of print]
[8] Lee V.H., Connolly H.M., Fulgham J.R., Manno E.M., Brown R.D. Jr., Wijdicks E.F., Tako-tsubo cardiomyopathy in aneurysmal subarachnoid hemorrhage: an underappreciated ventricular dysfunction, J. Neurosurg., 2006, 105, 264-270
[9] Ako J., Sudhir K., Farouque H.M., Honda Y., Fitzgerald P.J., Transient left ventricular dysfunction under severe stress: brain-heart relationship revisited, Am. J. Med., 2006, 119, 10-17
[10] Bybee K. A., Kara T., Prasad A., Lerman A., Barsness G.W., Wright R.S. et al., Systematic Review: Transient Left Ventricular Apical Ballooning: A Syndrome That Mimics ST-Segment Elevation Myocardial Infarction, Ann. Intern. Med., 2004, 141, 858-865Figure 1. Dynamics of electrocardiographic changes in patients with Tako-Tsubo cardiomyopathy (A - ST-elevation in the anterolateral leads, B - near complete regression of ST-elevation, C - deep negative T waves in all precordial leads)
538





























