Embed Size (px)
Citation preview

©2014 MFMER | slide-1
TB and the Eye
Wendy M. Smith, M.D. Assistant Professor of Ophthalmology
Mayo Clinic, Rochester, MN USA

©2014 MFMER | slide-2
Disclosure
• No financial disclosures

©2014 MFMER | slide-3
TB and the Eye
Outline
• Introduction
• Ocular TB manifestations
• Case Examples
• Diagnosis
• Treatment
Objectives
• Identify the variety of manifestations of ocular tuberculosis
• Describe the challenges associated with diagnosing ocular tuberculosis

©2014 MFMER | slide-4
Pre-test Questions
• True or False: Mycobacterium tuberculosis is usually isolated from ocular specimens in cases of suspected TB uveitis.
• True or False: The presence of M. tuberculosis DNA is evidence of active infection.
• True or False: TB uveitis is only treated with anti-TB drugs.

©2014 MFMER | slide-5
Tuberculosis = Mycobacterium tuberculosis
• Worldwide distribution
• ~1/3 latently infected
• Incidence >9 million active TB cases/yr
• Special populations
• People living in or immigrating from endemic regions
• Immunocompromised people (HIV, elderly, diabetics, those on immunosuppressive medications)

©2014 MFMER | slide-6
TB and the Eye
• Ocular disease is rare
• May affect any ocular tissue
• Direct invasion, hematogenous dissemination
• Hypersensitivity reaction to bacillus infection outside the eye
Mittal R et al. Ophthalmology. 2013 May; 120(5): 1103.e1-4

©2014 MFMER | slide-7
Ocular TB Epidemiology
• Varies worldwide
• U.S. 1.4% of those with primarily pulm TB
• Spain: 18% of randomly selected patients with culture-proven TB
• Italy: 20% of newly diagnosed TB cases (only 5% with ocular symptoms)
• Subgroups of TB (reviewed in Cutrufello et al. 2010)
• tubercular meningitis (16.2%), tubercular lymphadenopathy (23.2%), pediatric tubercular meningitis (~70%)

©2014 MFMER | slide-8
Ocular TB
• Tuberculosis of the conjunctiva and eyelids
• Tuberculous chancre and gumma of eyelids atypical chalazion
• Mucopurulent conjunctivitis with regional lymphadenopathy
• Chronic blepharitis
• Interstitial keratitis
• Phlyctenular conjunctivitis
Mittal R et al. Ophthalmology. 2013 May; 120(5): 1103.e1-4
Babu RB et al. Am J Ophthalmol. 2006
Sep;142(3):413-8.

©2014 MFMER | slide-9
Ocular TB
• Scleritis (most often anterior necrotizing or non-necrotizing, less often posterior)
• Orbital or adnexal disease Biswas J et al. Ocul Immunol
Inflamm. 2012 Feb;20(1):49-52.
Madge SN et al. Orbit. 2008;27(4):267-77.

©2014 MFMER | slide-10
Intraocular TB
• Tuberculoma
• Granulomatous uveitis
• Granulomatous choroiditis
• Retinal vasculitis
• Retinal or vitreous hemorrhages (Eales disease)
• Papilledema
• Optic neuritis, neuroretinitis

©2014 MFMER | slide-11
Most common presentations of ocular TB
• Demirci et al: review of 92 published case reports
• Choroidal mass +/-inflammatory signs (34%)
• Choroiditis/chorioretinitis (27%)
• Vitritis (24%)
• Iridocyclitis/anterior chamber reaction (13%)
• Panuveitis (11%)

©2014 MFMER | slide-12
TB Uveitis
• Uveitis = inflammation of the uveal tract (iris, ciliary body, retina/choroid)
• Uveitis attributed to TB:
• Once considered the most common cause of uveitis (up to 40% of granulomatous uveitis)
• Now relatively rare:
• US ~1%, China 4%, Italy 6%, Japan 7%, India up to 10%, Saudi Arabia 16%

©2014 MFMER | slide-13
IUSG Classification of Uveitis
• Anterior uveitis
• iris and pars plicata (CB)
• Intermediate uveitis
• pars plana and vitreous
• Posterior uveitis
• retina + choroid
• Panuveitis
“front”
“back”

©2014 MFMER | slide-14
ANTERIOR UVEITIS Granulomatous or Non-granulomatous
Keratic
precipitates
Posterior
synechia
Iris nodule
Rathinam SR, Lalitha P. Eye 2007 May;21(5):667-8.

©2014 MFMER | slide-15
http://www.reviewofophthalmology.com/content/d/retinal_insider/i/1206/c/22740/
http://www.eyecalcs.com/DWAN/pages/v5/ch033/016f.html
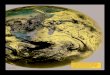
Choroidal tubercle with miliary TB
Choroidal
Tuberculoma

©2014 MFMER | slide-16 Bansal R et al. Ophthalmology. 2012 Nov;119(11):2334-42.
Serpiginous-like Choroiditis

©2014 MFMER | slide-17
M Ishaq, A H Feroze, M Shahid, M A Baig, S
S Ameen, S H Feroze and R A Chishti. Eye 2007
Sandeep Saxena http://www.ejournalofophthalmology.com/ejo/ejo21.html
Eales Disease
Idiopathic peripheral
perivasculitis
proliferative vascular
retinopathy,
recurrent vitreous
hemorrhages, and
tractional retinal
detachment
Young, otherwise
healthy men, 20-40 yrs
India, PPD+
TB identified by PCR
on aqueous, vitreous,
ERM

©2014 MFMER | slide-18
Case: 28 yo M from Kenya, in US x 8 yrs
• 2 months earlier: clouding in peripheral vision
• Then, black spot in vision, not a floater
• A week ago: awoke with red, painful eye
• In college, PPD rxn left scar on his arm
• 2009: PPD 25mm
• 2013: nml CXR

©2014 MFMER | slide-19
38 sec
1 min
5 min VA cc: 20/50 OU, Ta 10, 9
K OU: inferior subepithelial
opacification, neovascularization,
pigmented KPs, endothelial debris
AC OU: 3+ cell, 1+ flare
Vit OU: 2+ cell, 1+ haze, veils

©2014 MFMER | slide-20
5 min
58 sec • CRP 14.5
• Quantiferon positive
• ANA low positive 1.1
• wnl/neg: CBC (except low MCV), diff, Cr, UA, ESR, ACE, lysozyme, dsDNA, RF, CCP, toxoplasma IgG/M, Lyme abs, HepB/C, Syphilis IgG, HIV
• 28 yo M from Kenya
• Bilateral panuveitis
• Keratitis
• Anterior uveitis
• Vitritis
• Posterior uveitis/choroiditis

©2014 MFMER | slide-21
Chest CT
• Calcified granuloma in the superior segment of the left lower lobe
• Scattered tiny indeterminant pulmonary nodules with an upper lung predominance
• These may all represent old granulomas, and are consistent with the diagnosis of prior TB lung infection, but can be seen with other granulomatous processes

©2014 MFMER | slide-22
Presumed TB Uveitis • ID consult:
• requested AC tap neg acid fast smear and culture
• Quadruple drug tx (ethambutol, isoniazid, pyrazinamide, rifampin for 6 months
• Oral prednisone taper
• One month after finishing prednisone and anti-TB meds, no active uveitis

©2014 MFMER | slide-23
Case: 45 yo F from Pakistan, U.S. x 11 yr Sudden onset of “wavy lines” in vision
Aunt had tuberculosis, but no
direct exposure
Yearly PPD for work (teacher)
Chest x-ray: normal
Quantiferon: indeterminate,
but she was on systemic
immunosuppression

©2014 MFMER | slide-24
35 sec
5 min
42 sec
5 min

©2014 MFMER | slide-25
Serpiginous vs Serpiginous-like Choroiditis
Differences from Classic Serpiginous:
• From TB endemic region
• More likely unilateral
• Multifocal lesions involve posterior pole, mid-periphery,
periphery and spare juxtapapillary region (unlike
classic serpig)
• Inflammation in anterior chamber & vitreous
• Inflammation stops in response to anti-TB meds

©2014 MFMER | slide-26
Diagnosis of Ocular TB
Clinical context + clinical findings
• immigration from or travel to TB endemic region
• exposure to active TB
• healthcare worker
• worker or resident of nursing home or prison
• Immunocompromised (HIV+, iatrogenic, chronic disease)
• Homeless, elderly

©2014 MFMER | slide-27
Diagnostic Testing
• Assessments for other uveitis etiologies including HIV
• Chest imaging (x-ray, CT, PET/CT)
• TST/PPD
• False negative in 20-30% active TB
• Low positive predictive value in non-endemic areas
• Interferon-gamma release assay
• In vitro test using M tb antigens to stimulate release of IFNg from peripheral blood cells
• Biopsy, Smear, Culture, PCR

©2014 MFMER | slide-28
Challenges in Ocular TB Diagnosis
• Limited specimen
• aqueous – 150-200 uL
• Morbidity of obtaining specimen
• Vitrectomy
• Chorioretinal biopsy
• Low DNA yield, and presence of DNA not necessarily indicative of active disease
• Inflammation might be response to extraocular infection (no organism in the eye)
Van der Lelij A, Rothova A. Br J Ophthalmol.
1997 Nov;81(11):976-9.

©2014 MFMER | slide-29
Ocular TB - Treatment
• Report to local health department
• Coordinate care with infectious diseases specialist
• Confirmed and Presumed Ocular TB
• Both: quadruple drug tx x 6-12 mo
• Longer if increased risk of relapse (cavitary pulm disease, sputum cx + after 2 months)
• Concurrent corticosteroids
• Therapy efficacy: 40-70%
• Enucleation rate up to 30%

©2014 MFMER | slide-30
Delayed diagnosis/treatment: Sight- and/or life-threatening consequences
Patel et al. JAMA Ophth 2013:
• Midwestern U.S. cohort of 14 patients
• Average delay from ocular disease onset to uveitis referral: 755.3 days
• Non-Hispanic white race, posterior uveitis
• Vision loss associated with diagnosis after 500 days, age >50 yrs
Kesen MR. Arch Ophthalmol. 2009 Aug;127(8):1079-80.
Corneoscleral perforation
Choroiditis affecting macula, optic nerve
Choroidal neovascular membrane
Endophthalmitis

©2014 MFMER | slide-31
Post-test Questions
• True or False: Mycobacterium tuberculosis is usually isolated from ocular specimens in cases of suspected TB uveitis.
• True or False: The presence of M. tuberculosis DNA is evidence of active infection.
• True or False: TB uveitis is only treated with anti-TB drugs.

©2014 MFMER | slide-32
References 1. Alvarez GG, Roth VR, Hodge W. Ocular tuberculosis: diagnostic and treatment challenges. Int J
Infect Dis. 2009 Jul;13(4):432-5. 2. Babu RB, Sudharshan S, Kumarasamy N, Therese L, Biswas J. Ocular tuberculosis in acquired
immunodeficiency syndrome. Am J Ophthalmol. 2006 Sep;142(3):413-8. 3. Bansal R, Gupta A, Gupta V, Dogra MR, Sharma A, Bambery P. Tubercular serpiginous-like
choroiditis presenting as multifocal serpiginoid choroiditis. Ophthalmology. 2012 Nov;119(11):2334-42. 4. Biswas J, Aparna AC, Annamalai R, Vaijayanthi K, Bagyalakshmi R. Tuberculous scleritis in a patient
with rheumatoid arthritis. Ocul Immunol Inflamm. 2012 Feb;20(1):49-52. 5. Bodaghi B, LeHoang P. Ocular tuberculosis. Curr Opin Ophthalmol. 2000 Dec;11(6):443-8. 6. Cutrufello NJ, Karakousis PC, Fishler J, Albini TA. Intraocular tuberculosis. Ocul Immunol Inflamm.
2010 Aug;18(4):281-91. 7. Gupta A, Bansal R, Gupta V, Sharma A, Bambery P. Ocular signs predictive of tubercular uveitis. Am
J Ophthalmol. 2010 Apr;149(4):562-70. 8. Ishaq M, Feroze AH, Shahid M, Baig MA, Ameen SS, Feroze SH, Chishti RA. Intravitreal steroids
may facilitate treatment of Eales' disease (idiopathic retinal vasculitis): an interventional case series. Eye (Lond). 2007 Nov;21(11):1403-5.
9. Kesen MR, Edward DP, Rao NA, Sugar J, Tessler HH, Goldstein DA. Atypical infectious nodular scleritis. Arch Ophthalmol. 2009 Aug;127(8):1079-80.
10. Madge SN, Prabhakaran VC, Shome D, Kim U, Honavar S, Selva D. Orbital tuberculosis: a review of the literature. Orbit. 2008;27(4):267-77.
11. Mittal R, Tripathy D, Sharma S, Balne PK. Tuberculosis of eyelid presenting as a chalazion. Ophthalmology. 2013 May;120(5):1103.e1-4.
12. Nazari Khanamiri H, Rao NA. Serpiginous choroiditis and infectious multifocal serpiginoid choroiditis. Surv Ophthalmol. 2013 May-Jun;58(3):203-32.
13. Patel SS, Saraiya NV, Tessler HH, Goldstein DA. Mycobacterial ocular inflammation: delay in diagnosis and other factors impacting morbidity. JAMA Ophthalmol. 2013 Jun;131(6):752-8.
14. Rathinam SR, Lalitha P. Paradoxical worsening of ocular tuberculosis in HIV patients after antiretroviral therapy. Eye (Lond). 2007 May;21(5):667-8.
15. Sheu SJ, Shyu JS, Chen LM, Chen YY, Chirn SC, Wang JS. Ocular manifestations of tuberculosis. Ophthalmology. 2001 Sep;108(9):1580-5.
16. Van der Lelij A, Rothova A. Diagnostic anterior chamber paracentesis in uveitis: a safe procedure? Br J Ophthalmol. 1997 Nov;81(11):976-9.

©2014 MFMER | slide-33
Thank you!