Embed Size (px)
Citation preview

Technical Handbook for the Integration of Cytoreductive
Surgery and Perioperative Intraperitoneal Chemotherapy
into the Surgical Management of Gastrointestinal and
Gynecologic Malignancy
4th Edition
Paul H. Sugarbaker, MD, FACS, FRCS
Contents I. Background and rationale
II. Quantitative prognostic indicators III. Peritonectomy IV. Sugarbaker retractor V. Heater circulator apparatus
VI. Heated intraoperative intraperitoneal chemotherapy VII. Early postoperative intraperitoneal chemotherapy
VIII. Clinical pathway for postoperative care IX. Results of treatment X. Current indications for cytoreductive surgery plus perioperative intraperitoneal
chemotherapy XI. Conclusions
XII. Appendix
Foundation for Applied Research in Gastrointestinal Oncology
December 5, 2005

2
Technical Handbook for the Integration of Cytoreductive
Surgery and Perioperative Intraperitoneal Chemotherapy
into the Surgical Management of Gastrointestinal and
Gynecologic Malignancy
Paul H. Sugarbaker, MD, FACS, FRCS

3
by
Paul H. Sugarbaker, MD, FACS, FRCS Washington Cancer Institute
106 Irving Street, NW, Suite 3900 Washington, DC 20010
All rights reserved. Reproduction in whole or in part by any means without permission of the author
is prohibited.
French, Italian, Turkish, Chinese, Polish, Russian, Portuguese, Spanish, Hungarian translations are available
Printed in the United States of America
by The Ludann Company
Grand Rapids, Michigan
Supported by the Foundation for
Applied Research in Gastrointestinal
Oncology – FARGO, and the Washington
Cancer Institute.

4
INTRODUCTION
Most cancers that occur within the abdomen or pelvis will disseminate by three different routes. These are: hematogenous metastases, lymphatic metastases, and implants on peritoneal surfaces. In a substantial number of patients, disease progression that is isolated to the resection site or to peritoneal surfaces may occur. If this is true, elimination of peritoneal surface spread will have an impact on the survival of these cancer patients in whom a prominent cause of death is peritoneal carcinomatosis or sarcomatosis. Prior to the use of a combined treatment using cytoreductive surgery plus intraperitoneal chemotherapy, these conditions were uniformly fatal, eventually resulting in intestinal obstruction over the course of months or years. Occasionally, patients with minimally aggressive malignancies such as peritoneal mesothelioma or pseudomyxoma peritonei survived long-term, but all end results reporting shows a fatal outcome with progression of intraabdominal cancer.
We have devised techniques that allow the administration of intraperitoneal
chemotherapy as an integrated part of a surgical procedure for cancer. This approach involves two conceptual changes in chemotherapy administration. Both the route and timing of chemotherapy administration are changed. The intraperitoneal route assures a high concentration of anticancer therapy at the peritoneal surfaces. The perioperative timing has several advantages. With heated intraoperative intraperitoneal chemotherapy (HIIC), hyperthermia can be used to enhance cytotoxicity and improve drug penetration. Also, the surgeon will manually manipulate the peritoneal surfaces to uniformly distribute heat and drugs thereby improving response and reducing complications. With early postoperative intraperitoneal chemotherapy (EPIC) the abdominal lavage occurs before wound healing causes adhesions and utilizes a large volume of fluid and gravity distribution to contact a majority of the peritoneal surface and irrigate away any old blood or fibrinous debris. The chemotherapy administration is performed after cytoreductive surgery so that all of the malignancy, except microscopic residual disease or tiny nodules on small bowel surfaces, is removed surgically before the chemotherapy treatments. This means that the limited penetration of chemotherapy, approximately 1 mm into tissues, may eradicate all tumor cells. Finally, the chemotherapy will be used prior to the construction of any anastomoses, which means that suture line recurrences should also be eliminated.
This manual is written to describe for the physician and nurse methods for treatment and
prevention of peritoneal carcinomatosis, mesothelioma and sarcomatosis currently in use at the Washington Cancer Institute.

5
Intraperitoneal Chemotherapy for Gastrointestinal Cancer
Four distinct time periods have been identified for the use of chemotherapy in gastrointestinal cancer. The timing for instillation of an intraperitoneal chemotherapy solution most commonly utilized is perioperative. If the treatment is used intraoperatively moderate hyperthermia is generally applied along with heat-augmented chemotherapy solutions such as cisplatin, doxorubicin, mitomycin C or oxaliplatin. In this book hyperthermic intraoperative intraperitoneal chemotherapy will be abbreviated as HIIC.
The other perioperative intraperitoneal chemotherapy shown to be effective is early
postoperative intraperitoneal chemotherapy. In this book early postoperative intraperitoneal chemotherapy is abbreviated as EPIC. This chemotherapy treatment involves a large volume of solution instilled into the peritoneal cavity for 23 hours. Usually the instillations are continued for 5 or 7 days until wound healing will begin to cause the adherence of bowel loops to themselves and other intraperitoneal structures. HIIC and/or EPIC have been shown to be effective in the treatment of established peritoneal carcinomatosis after cytoreductive surgery (1,2). Also one or both of the perioperative treatments have been successfully added to primary cancer resection to eliminate microscopic residual disease disseminated as a result of full thickness invasion of the bowel wall or from surgical trauma (3). Less frequently HIIC and EPIC are used in an effort to palliate gross intraabdominal progression of gastrointestinal cancer. If intestinal dysfunction is present or likely to occur in the near future debulking surgery with bowel resection may be necessary. In some patients with debilitating ascites, only greater omentectomy may be indicated. Usually both HIIC and EPIC are used because gross disease remains after the surgical effort.
Long-term intraperitoneal chemotherapy is used to prolong the regional (peritoneal surface) effects of selected drugs. Its benefit has been demonstrated most definitively in ovarian cancer. Some precautions regarding the logistics of long-term intraperitoneal chemotherapy are necessary. Long-term access to the peritoneal cavity will require repeated paracentesis or an intraperitoneal port. Repeated paracentesis has been associated with bowel perforation which may become especially hazardous after repeated chemotherapy instillations or with the progression of peritoneal surface cancer. An intraperitoneal port has been associated with infection, with pain upon instillation, and with a progressive increase in non-uniform drug distribution. Both repeated paracentesis and an intraperitoneal port are more problematic after extensive peritonectomy. Currently, long-term intraperitoneal chemotherapy is unusual after extensive parietal peritonectomy.
Recently, perioperative use of the laparoscope in patients with primary gastrointestinal cancer has made possible the identification and biopsy of peritoneal carcinomatosis. Consequently intraperitoneal chemotherapy can be selectively used to downstage the extent of peritoneal surface disease prior to definitive surgery. Because no prior surgery has caused adhesions, distribution of chemotherapy solution in a large volume of fluid should be adequate. In order to downstage not only carcinomatosis but also the primary cancer, systemic chemotherapy in addition to intraperitoneal chemotherapy is used. This neoadjuvant intraperitoneal and systemic chemotherapy is referred to as NIPS chemotherapy. Similar doses of drugs are given intraperitoneally as are used systemically.

6
I. Background and rationale Intraperitoneal chemotherapy gives high response rates within the abdomen because the
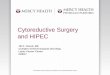
peritoneal space to plasma barrier provides dose intensive therapy (1). Figure 1 shows that large molecular weight substances such as mitomycin C are confined to the abdominal cavity for long time periods (2). This means that the exposure of peritoneal surfaces to pharmacologically active molecules can be increased considerably by giving the drugs via the intraperitoneal as opposed to intravenous route.
Figure 1. Large molecular weight compounds when instilled into the peritoneal cavity are sequestered at that site for long periods. The physiologic barrier to the release of intraperitoneal drugs is called the peritoneal space to plasma barrier. In this experiment, 15 mg of mitomycin C was infused into the peritoneal cavity as rapidly as possible. Intraperitoneal, intravenous, portal venous and urine mitomycin C concentrations were determined by HPLC assay. (From Sugarbaker PH, Graves T, DeBruijn EA, Cunliffe WJ, Mullins RE, Hull WE, Oliff L, Schlag P: Rationale for Early Postoperative Intraperitoneal Chemotherapy (EPIC) in patients with advanced gastrointestinal cancer. Cancer Res 50:5790-5794, 1990)

7
For the chemotherapy agents used to treat peritoneal carcinomatosis or peritoneal mesothelioma, the area under the curve (AUC) ratios of intraperitoneal to intravenous exposure are favorable. Table 1 presents the molecular weight and AUC IP/IV for the drugs in routine clinical use in patients with peritoneal seeding (4). In our studies, these include 5-fluorouracil, mitomycin C, doxorubicin, cisplatin, oxaliplatin, and paclitaxel.
TABLE 1. Area under the curve ratios of peritoneal surface exposure to systemic exposure for drugs used to treat intraabdominal cancer.
Drug Molecular Weight Area Under the Curve Ratio5-Fluorouracil 130 250 Mitomycin C 334 75 Doxorubicin 544 500
Cisplatin 300 20 Oxaliplatin 397 16 Paclitaxel 854 1000
Sugarbaker and colleagues have advanced the tumor cell entrapment hypothesis to
explain the high incidence of peritoneal dissemination in patients who undergo the surgical treatment of intraabdominal adenocarcinoma (2). This theory relates the high incidence of tumor implantation to one or more of the following mechanisms:
a. free intraperitoneal tumor emboli as a result of full thickness invasion of the bowel wall by
cancer; b. leakage of malignant cells from transected lymphatic channels; c. dissemination of malignant cells from trauma as a result of dissection at a narrow margin; d. blood clots that remain in the abdomen or pelvis that contain viable cancer cells; e. fibrin entrapment of intraabdominal tumor emboli on traumatized peritoneal surfaces; f. tumor promotion of these entrapped cells through growth factors involved in the wound
healing process.

8
In order to interrupt progression of tumor cells on abdominal and pelvic surfaces, the peritoneal cavity is flooded with chemotherapy in a large volume of fluid prior to surgery (NIPS), during surgery (HIIC), and in the postoperative period (EPIC). In many cases systemic chemotherapy is used simultaneously. These strategies may be used to treat peritoneal surface malignancy or to prevent it in groups at high risk. In this approach to peritoneal surface malignancy, the traditional route (intraperitoneal vs. intravenous) and timing (perioperative vs. postoperative) of chemotherapy delivery is changed. Non-perioperative intraperitoneal chemotherapy, often used in the past, and given over long time periods is reserved for management of debilitating malignant ascites.
This new approach to the surgical treatment of intraabdominal malignancy begins in the
operating room after a complete resection of a primary cancer or after the cytoreduction of peritoneal carcinomatosis, or mesothelioma. The intraoperative chemotherapy is performed prior to construction of suture lines. A proper placement of tubes, drains and temperature probes is needed prior to initiation of heated intraoperative intraperitoneal chemotherapy. Before abdominal closure, the temperature probes are removed, but the tubes and drains remain to deliver early postoperative intraperitoneal chemotherapy and assist in postoperative removal of excess peritoneal fluid.
In the operating room, heated intraperitoneal chemotherapy is used. Heat is part of the
optimizing process and is used to bring as much dose intensity to the abdominal and pelvic surfaces as is possible. Hyperthermia with intraperitoneal chemotherapy has several advantages. First, heat by itself has greater toxicity for cancerous tissue than for normal tissue. This effect on cancer tissue increases as the vascularity of the malignancy decreases. Second, hyperthermia increases the penetration of chemotherapy into tissues. As tissues soften in response to heat, the elevated interstitial pressure of a tumor mass decreases allowing improved drug penetration. Third, and probably most important, heat increases the cytotoxicity of selected intraperitoneal chemotherapy agents. Systemic chemotherapy with heat-augmented drugs may target small peritoneal surface cancer nodules if administered with hyperthermic intraperitoneal solutions. This enhancement occurs only at the interface of heat and body tissue, at the peritoneal surface. The benefits of heat and the intraoperative timing of intraperitoneal chemotherapy are listed in Table 2.

9
The large volume of chemotherapy solution required to administer heated intraoperative intraperitoneal chemotherapy removes tissue debris and blood products from the abdominal cavity to minimize fibrin entrapment of cancer cells. The chemotherapy not only directly destroys tumor cells, but it also eliminates viable platelets, neutrophils and monocytes from the peritoneal cavity. This diminishes the promotion of tumor growth associated with the wound healing process.
Tumor cells that remain viable in the abdominal cavity after cytoreductive surgery and
heated intraoperative intraperitoneal chemotherapy can be further treated by pharmacologic concentrations of intraperitoneal chemotherapy instilled on postoperative days 1 through 4 or 1 through 5. The timely use of intraperitoneal chemotherapy in the operating room or in the early postoperative period eliminates tumor cells from the abdomen before they are fixed within scar tissue that results from wound healing. Cell cycle-specific drugs such as 5-fluorouracil or paclitaxel are usually administered as early postoperative intraperitoneal chemotherapy.
TABLE 2. Benefits of intraperitoneal hyperthermia and of intraoperative timing of
intraperitoneal and systemic chemotherapy. • Heat increases drug penetration into tissue. • Heat increases the cytotoxicity of selected chemotherapy agents. • Heat has anti-tumor effects by itself. • Heat at the peritoneal surface causes increased cytotoxicity of systemic chemotherapy to
small cancer nodules. • Intraoperative chemotherapy allows manual distribution of drug and heat uniformly
to all surfaces of the abdomen and pelvis. • Renal toxicities of chemotherapy can be avoided by careful monitoring of urine output
during chemotherapy perfusion. • Nausea and vomiting are avoided because the patient is under general anesthesia. • The time that elapses during the heated perfusion allows a normalization of many
functional parameters (temperature, blood clotting, hemodynamics, etc.).

10
Figure 2. CT cut through the mid-abdomen in a patient with pseudomyxoma peritonei. The
mucinous tumor is extensive but the surface of the small bowel remains isolated from the mucinous tumor. This radiologic picture is referred to as compartmentalization. The patient had a complete cytoreduction and remains disease-free.

11
Figure 3. CT cut through the mid-abdomen in a patient with peritoneal mucinous carcinoma
of appendiceal origin. The bowel and its mesentery are coated by mucinous tumor nodules greater than 5 cm. The radiologic anatomy of the small bowel loops and its mesentery are distorted indicating segmental narrowing of the bowel. This patient has less than 5% likelihood of a complete cytoreduction.

12
II. Quantitative Prognostic Indicators in Peritoneal Surface Malignancy Predicting outcome by preoperative CT of the chest, abdomen and pelvis
CT is an inaccurate test by which to quantitate peritoneal carcinomatosis from non-invasive adenocarcinoma (5). The malignant tissue progresses on the peritoneal surfaces and its shape conforms to the normal contours of the abdominal and pelvic structures. This is quite different from the metastatic processes in liver or lung which progress as 3-dimensional tumor nodules. A second flaw in using CT for peritoneal surface may occur from inadequate patient preparation with oral contrast resulting in the imaging of non-opacified bowel loops.
The CT has been of greater help in locating and quantifying mucinous adenocarcinoma
within the peritoneal cavity (6). These tumors produce a copious colloid material that is readily distinguished by shape and by density from normal structures. Using two distinctive radiological criteria, those patients with resectable mucinous peritoneal carcinomatosis can be selected from those with non-resectable malignancy. This spares patients who are unlikely to benefit from cytoreductive surgery from unnecessary procedures. The two radiological criteria for patients with mucinous adenocarcinoma found to be most useful are: 1) segmental obstruction of small bowel, and 2) presence of tumor more than 5 cm in greatest dimension on the small bowel surface or directly adjacent to small bowel mesentery. These criteria reflect radiologically the biology of the mucinous adenocarcinoma. The obstructed segments of small bowel signal an invasive character of malignancy that is unlikely to be cytoreduced completely. Masses of mucinous cancer on small bowel and small bowel mesentery indicates that the disease is no longer redistributed. Usually, this indicates that small bowel surfaces will have residual disease after cytoreduction, for the intestinal surface is difficult to peritonectomize (see Figures 2 and 3).
The two radiologic criteria for patients with peritoneal mesothelioma found to be most
useful are extensive tumor in the epigastric region and generalized involvement of the small bowel. These radiologic findings indicate that an adequate cytoreduction is not likely to be possible. In order to quantitate the CT findings with small bowel and its mesentery, an interpretative CT classification has been described (7).

13
As shown in Table 3, characteristic interpretative CT findings of the small bowel and its mesentery are categorized into four classes. Class 0 CT showed no ascites in the region of the small bowel. The jejunal and ileal vessels appeared as round and curvilinear densities within the mesenteric fat. Class I CT scans showed free intraperitoneal fluid only. The mesentery was stranded and stratified as the fluid accumulation outlined the small bowel mesentery. The small bowel vessels are easily identified within the mesenteric fat (Figure 4). Class II CT showed tumor involvement of the small bowel and/or its mesentery. The peritoneal surface was thickened and enhanced due to the presence of nodules (usually half-spherical bodies) or plaques (flat implants whose diameter was greater than thickness). There may be an increased amount of ascites fluid and the mesentery may appear to be stellate or pleated. The small bowell mesenteric vessels were still identifiable (Figure 5). Class III CT showed increased solid tumor involvement and adjacent small bowel loops are matted together in some cuts. The configuration of the small bowel and its mesentery was distorted and thickened. Segmental small bowel obstruction may be present and intraperitoneal fluid may be loculated. The small bowel mesenteric vessels were difficult to define on some cuts due to obliteration of mesenteric fat (Figure 6) .
In predicting the likelihood of adequate cytoreduction in peritoneal mesothelioma
interpretative CT classification of the small bowel has been shown useful. A second criteria by which to predict adequate cytoreduction is large volume tumor involvement of the epigastric regions. If there is extensive disease infiltrating the lesser omentum, adequate cytoreduction is not usually possible (Figure 7).

14
Figure 4. Class I CT interpretative findings in peritoneal mesothelioma. CT shows free intraperitoneal fluid only. The mesentery becomes stranded and stratified as the fluid accumulation outlines the small bowel mesentery. Normal small bowel vasculature is identified within the mesenteric fat.

15
Figure 5. Class II interpretative findings in peritoneal mesothelioma. CT shows tumor
layering out on the small bowel mesentery. The peritoneal lining is thickened and enhanced due to the presence of tumor nodules or plaques. There may be an increased amount of ascitic fluid; the small bowel loops and mesentery remain separated. The small bowel mesenteric vessels are still identifiable.

16
Figure 6. Class III interpretative findings in peritoneal mesothelioma. CT shows increased
solid tumor involvement with adjacent bowel loops matted together. The configuration of the small bowel and its mesentery is distorted and thickened. Intraperitoneal fluid may be loculated. The small bowel mesenteric vessels are difficult to define due to the obliteration of mesenteric fat.

17
Figure 7. Patient with large volume peritoneal mesothelioma who has extensive tumor
within the epigastric region. The subpyloric space is filled by tumor indicating that the lesser curvature of the stomach cannot be cleared of tumor. A suboptimal cytoreduction occurred in this patient.

18
Table 3. Intepretative CT classification of small bowel and its mesentery in patients
with peritoneal mesothelioma.
Class Presence of ascites
Small bowel and mesentery involvement
Loss of mesenteric vessel clarity CT scan interpretation
0 No No No Normal appearance
I Yes No No Ascites only
II Yes Thickening, enhancing No Solid tumor present
III Yes Nodular thickening Segmental obstruction Yes Loss of normal architecture
Prior Surgical Score A second quantitative prognostic indicator useful in patients with peritoneal surface malignancy is the extent of prior surgical intervention. We have proposed a scoring system of the prior surgical interventions referred to as the prior surgical score (PSS). It estimates the extent of surgery by quantitating surgical dissection within nine abdominopelvic regions (Figure 8). If the prior surgical score is 3 (PSS-3), at least 5 of the 9 abdominopelvic regions (AR 0-8) have been dissected without the use of intraoperative or early postoperative intraperitoneal chemotherapy (Table 4). For the PSS-2, 2 to 5 abdominopelvic regions had been dissected. For PSS-1, only one region had been dissected. These patients had exploratory surgery but no major organ or tissue dissection. For PSS-0, patients had biopsy only. This may have been by laparoscopy, by CT-guided biopsy, or by paracentesis with cytology. The number of abdominopelvic regions is, by convention, additive for all prior surgical procedures. In this regard PSS is a composite of all prior surgeries.

19
Figure 8. Summation of the regions in which surgical dissection occurred determines the
prior surgical score

20
Table 4. Assessment of prior surgical score (PSS).
PSS-0 (none) Biopsy only
PSS-1 (minimal) Exploratory laparotomy, 1 region
PSS-2 (moderate) Exploratory laparotomy with resections, 2-5 regions
PSS-3 (heavy) Extensive prior cytoreduction, >5 regions
Peritoneal Cancer Index
Patients with peritoneal seeding from invasive adenocarcinomas are selectively treated at this point in time according to the Peritoneal Cancer Index (8). This is a clinical summary of both lesion size and distribution of peritoneal surface malignancy (Figure 9). It should be used in the decision making process as the abdomen is explored. To arrive at a score, the size of intraperitoneal nodules must be assessed. The lesion size (LS) score should be used. LS-0 means that no malignant deposits are visualized. LS-1 signifies that tumor nodules less than 0.5 cm in greatest dimension are present. The number of nodules is not scored, only the size of the largest nodules. LS-2 signifies tumor nodules between 0.5 and 5.0 cm present. LS-3 signifies tumor nodules greater than 5.0 cm in any dimension present. If there is a confluence of tumor nodules (layering), the lesion size is scored as 3.
In order to assess the distribution of peritoneal surface disease, the abdominopelvic
regions are utilized. For each of these 13 regions, a lesion size score is determined. The summation of the lesion size score in each of the 13 abdominopelvic regions is the Peritoneal Cancer Index for that patient. A maximal score is 39 (13x3).
There are some caveats in the use of the Peritoneal Cancer Index. First, diseases such as
pseudomyxoma peritonei, grade I sarcoma and cystic peritoneal mesothelioma are noninvasive. In these situations, the status of the abdomen and pelvis after cytoreduction may have no relationship to the status at the time of abdominal exploration. In other words, even though the surgeon may find an abdomen with a Peritoneal Cancer Index of 39, it can be converted to an index of 0 by cytoreduction. In these noninvasive peritoneal surface malignancies, the prognosis will only be related to the completeness of cytoreduction and not to the Peritoneal Cancer Index.

21
Figure 9. Peritoneal Cancer Index is used to estimate the likelihood of complete cytoreduction in patients with invasive peritoneal surface malignancy. The score is a summation of cancer implant lesion size (scored 0 to 3) present in the 13 abdominopelvic regions. (From Esquivel J, Sugarbaker PH: Elective surgery in recurrent colon cancer with peritoneal seeding: When to and when not to proceed. (Editorial) Cancer Therapeutics 1:321-325, 1998).

22
A second caveat for the Peritoneal Cancer Index is invasive cancer at CRUCIAL ANATOMIC SITES. For example, unresectable cancer on the common bile duct will cause a poor prognosis despite a low Peritoneal Cancer Index. Cancer implants at numerous sites on the small bowel surface will confer a poor prognosis. Lymph node metastases within groups unrelated to the primary cancer represent lymphatic dissemination from peritoneal surface cancer (metastases from metastases) and a poor prognosis. Cancer at crucial anatomic sites becomes a systemic disease equivalent in assessing prognosis and will override a favorable score with the Peritoneal Cancer Index.
The score of the Peritoneal Cancer Index compatible with benefit using combined treatment will vary with the type of peritoneal surface malignancy treated. Berthet, et al in a study of sarcomatosis found an index of < 13 associated with a 74% five-year survival; an index of > 13 was associated with an 11% five-year survival (9). For colon cancer with carcinomatosis, Sugarbaker reported a Peritoneal Cancer Index of < 10 associated with a 50% five-year survival; an index of 11-20 was associated with a 20% five-year survival; and an index of > 20 was associated with a 0% five-year survival (10).
Completeness of cytoreduction score
The final assessment to be used to assess prognosis with peritoneal surface malignancy is the completeness of cytoreduction (CC) score. This information is of less value to the surgeon in planning treatments than the abdominopelvic CT, prior surgical score, and the Peritoneal Cancer Index because the CC score is not available until after the cytoreduction is complete. If during exploration it becomes obvious that cytoreduction will not be complete, the surgeon may decide that a palliative debulking that will provide symptomatic relief is appropriate and discontinue plans for a potentially curative cytoreduction. In both noninvasive and invasive peritoneal surface malignancy, the completeness of cytoreduction score is thought to be the principle prognostic indicator.

23
For gastrointestinal cancer, the completeness of cytoreduction score has been defined as follows: A CC-0 score indicates that no visible peritoneal carcinomatosis remains after cytoreduction. A CC-1 score indicates that tumor nodules persisting after cytoreduction are less than 2.5 mm. This is a nodule size thought to be penetrable by intracavitary chemotherapy. A CC-2 score indicates tumor nodules between 2.5 mm and 2.5 cm. A CC-3 score indicates tumor nodules greater than 2.5 cm or a confluence of unresected tumor nodules at any site within the abdomen or pelvis (Figure 10). In high-grade malignancy, complete cytoreduction may require a CC-0 score. In less invasive malignancy such as pseudomyxoma peritonei, a complete cytoreduction may include CC-0 and CC-1 cytoreduction.
Figure 10. Completeness of cytoreduction score CC-0 to CC-3. A complete cytoreduction for
a noninvasive malignancy such as pseudomyxoma peritonei includes CC-0 and CC-1 resection. For invasive cancer such as colorectal or gastric carcinomatosis, only CC-O resection is considered complete cytoreduction.

24
In summary, cytoreductive surgery using peritonectomy and visceral resections is combined with perioperative intraperitoneal and systemic chemotherapy as a planned surgical event. The surgery is to reduce the tumor volume to microscopic disease or tiny tumor implants; then the intraperitoneal and systemic chemotherapy with hyperthermia is used to eradicate the residual disease. Attempts at treatment of peritoneal surface disease when quantitative prognostic indicators suggest a poor outcome is to be avoided. Although large volume noninvasive malignancy can be successfully treated, only patients with small volume high-grade peritoneal surface cancer should be electively treated with curative intent using cytoreductive surgery and intraperitoneal chemotherapy. Patients with microscopic residual peritoneal seeding with limited distribution on peritoneal surfaces following cytoreduction should be expected to benefit and are candidates for this comprehensive management strategy.

25
III. Cytoreductive surgery for peritoneal surface malignancy – peritonectomy procedures
Not all six of these peritonectomy procedures will be required in all patients. The
peritoneal surfaces are stripped of tumor only where there is visible disease. The surgeon's goal with the cytoreduction is to remove as much tumor as is possible (11). The smaller the cancer volume that remains for chemotherapy treatments, the better the results will be.
Position and incision
The patient is placed in a supine position with the gluteal folds advanced to the break in the operating table in order to provide full access to the perineum during the surgical procedure (Figure 11). This modified lithotomy position is achieved with the legs extended in St. Mark's leg holders (AMSCO, Erie, PA). The weight of the legs must be directed to the bottom of the feet by positioning the footrests so that minimal weight is borne by the calf muscle.
All surfaces of the St. Mark's stirrups are protected by egg crate foam padding. The thighs and legs are surrounded by alternating pressure devices (SCB Compression Boots, Kendall Co., Boston, MA). These should be operative prior to the induction of anesthesia for maximal protection against venothrombosis. A hyperthermia blanket is placed over the chest. arms and head of the patient (Bair Hugger Upper Body Cover, Augustine Medical, Eden Prairie, MN), and also beneath the torso (Cincinnati Sub-Zero, Cincinnati, OH).
Abdominal skin preparation is from mid-chest to mid-thigh. The external genitalia are prepared in the male, and in the female, a vaginal preparation is also used. The Foley catheter is inserted after the skin preparation so that this catheter can be accessed as part of the sterile field during the surgical procedure. A large bore silastic nasogastric tube is placed within the stomach and its position confirmed at the time of abdominal exploration (Argyle Silastic Salem Sump Tube, Sherwood Medical, St. Louis, MO).

26
Figure 11. Position and incision for peritonectomy procedures. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

27
Total anterior parietal peritonectomy After the linea alba has been divided a single entry into the peritoneal cavity in the upper portion of the incision (peritoneal window) allows the surgeon to assess the requirement for a complete parietal peritonectomy (Figure 12). If cancer nodules are palpated on the parietal peritoneum, a decision regarding a complete parietal peritonectomy should occur (12). Except for the small defect in the peritoneum required for this peritoneal exploration, the remainder of the peritoneum is maintained intact. Adair clamps are placed on the skin in order to provide broad traction along the complete extent of the point for tissue transection. The dissecting tool is the ball tip and smoke evacuation is used continuously. After the initial 10 cm of peritonectomy the self-retaining retraction system is steadily advanced along the anterior abdominal wall. This optimizes the broad traction at the point of dissection of the peritoneum from its underlying tissues. It is most adherent directly overlying the transversus muscle. In some instances, dissection from inferior to superior aspects of the abdominal wall facilitates clearing in the mid-abdomen. The dissection blends in with the right and left subphrenic peritonectomy superiorly and with the complete pelvic peritonectomy inferiorly. As the dissection proceeds beyond the peritoneum overlying the paracolic sulcus the dissection becomes more rapid with the loose connections of the peritoneum at this anatomic site.

28
Figure 12. Total anterior parietal peritonectomy. (From De Lima Vazquez V, Sugarbaker PH: Total anterior parietal peritonectomy. J Surg Oncol 83:261-263, 2003)

29
Abdominal exposure, greater omentectomy, and splenectomy
As the abdomen is opened from xiphoid to pubis, the xiphoid is excised using electrosurgical dissection (13). Generous abdominal exposure is achieved through the use of a Thompson Self-Retaining Retractor (Thompson Surgical Instruments, Inc., Traverse City, Ml). The standard electrosurgical tool used to dissect tumor on peritoneal surfaces from the normal tissues is a 3 mm ball-tip (Valleylab, Boulder, CO). The ball-tip hand piece is placed at the interface of tumor and normal tissues. The focal point for further dissection is placed on strong traction. The electrosurgical generator is used on pure cut at high voltage. The ball-tip electrode is used for dissecting on visceral surfaces including stomach, small bowel, and colon. When more generalized tumor destruction is required, for example on the liver surface, the ball-tip will cause more rapid tumor destruction if used in the “hockey stick” configuration.
Using ball-tip electrosurgery on pure cut creates a large volume of plume because of the
electroevaporation of tissue. In order to maintain visualization of the operative field and to preserve a smoke-free atmosphere in the operating theater, a smoke filtration unit is utilized (Buffalo, Buffalo, NY). The vacuum tube tip is maintained two to three inches from the field of dissection whenever electrosurgery is in use.
In order to free the mid-abdomen of a large volume of tumor, a complete greater
omentectomy is performed. The greater omentum is elevated and then separated from the transverse colon using ball-tip electrosurgery (Figure 13). This dissection continues beneath the peritoneum that covers the transverse mesocolon, in order to expose the anterior surface of the pancreas. All branches of the gastroepiploic vessels on the greater curvature of the stomach are clamped, ligated, and divided. Also, the short gastric vessels are ligated and divided. With traction on the spleen, the anterior fascia of the pancreas is elevated from the gland using ball-tip electrosurgery. This freely exposes the splenic artery and vein at the tail of the pancreas. These vessels are ligated in continuity and proximally suture ligated. The specimen of greater omentum and spleen is often free at this point for submission to pathology. In some patients, the spleen is adherent by tumor to the undersurface of the left hemidiaphragm; when this occurs the left upper quadrant peritonectomy must be completed before the specimen is released.

30
Figure 13. Abdominal exposure, greater omentectomy, and splenectomy. (From Sugarbaker
PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

31
Left upper quadrant peritonectomy
In order to begin exposure of the left upper quadrant, the portion of the peritoneum which constitutes the edge of the abdominal incision is stripped away from the posterior rectus sheath (Figure 14). To secure this peritoneal layer, Kelly clamps are placed on it at 10 cm intervals. This allows traction to be achieved on the tumor specimen throughout the left upper quadrant.
The left upper quadrant peritonectomy involves the stripping of all tumor tissue from
beneath the left hemidiaphragm to expose diaphragmatic muscle, left adrenal gland, distal portion of the pancreas, and the cephalad one-half of the perirenal fat. In order to achieve full exposure of the left upper quadrant, peritoneum at the splenic flexure is released from the left abdominal gutter and moved medially by dividing tissue along Toldt's line.
Stripping of tumor tissue from beneath the left hemidiaphragm is accomplished with ball-
tip electrosurgery and not by blunt dissection. Numerous blood vessels between the diaphragm muscle and its peritoneal surface must be electrocoagulated before their transection or unnecessary bleeding will occur. Tissues are transected using ball-tip electrosurgery on pure cut, but all blood vessels are electrocoagulated prior to their division.
Figure 14. Peritoneal stripping from beneath the left hemidiaphragm. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

32
Left upper quadrant peritonectomy completed
When the left upper quadrant peritonectomy is completed the stomach may be reflected medially. Numerous ligated branches of the gastroepiploic vessels are evident. The left adrenal gland, pancreas, and left Gerota's fascia are completely exposed, as is the anterior peritoneal surface of the transverse mesocolon. With all the upper abdominal peritonectomy procedures, the surgeon must carefully avoid the major branches of the left gastric artery and coronary vein in order to preserve the sole remaining vascular supply to the stomach (Figure 15).
Figure 15. Left upper quadrant peritonectomy completed. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

33
Right upper quadrant peritonectomy
Peritoneum is stripped away from the right posterior rectus sheath to begin the peritonectomy in the right upper quadrant of the abdomen (Figure 16). Kelly clamps are placed on the specimen and strong traction is used to elevate the hemidiaphragm into the operative field. Again, ball-tip electrosurgery on pure cut is used to divide tissue planes. Coagulation current is used to seal blood vessels as they are encountered.
Figure 16. Peritoneal stripping from beneath the right hemidiaphragm. (From Sugarbaker
PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

34
Dissection beneath tumor through Glisson's capsule
The stripping of tumor from the muscular surface of the diaphragm continues until the bare area of the liver is encountered (Figure 17). At this point, tumor on the anterior surface of the liver is electroevaporated until the liver surface is visualized. With electrosurgical dissection, one lifts tumor off the dome of the liver moving through or beneath Glisson's capsule. Hemostasis is achieved as the dissection proceeds using generous coagulation electrosurgery. Isolated patches of tumor on the liver surface are electroevaporated with the distal 2 cm of the ball-tip bent and stripped of insulation (hockey stick configuration). Ball-tip electrosurgery is also utilized to extirpate tumor in and around the umbilical fissure of the liver.
Figure 17. Dissection beneath tumor through Glisson's capsule. (From Sugarbaker PH:
Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

35
Removal of tumor from beneath the right hemidiaphragm, from right subhepatic space, and from the surface of the liver
Tumor from beneath the right hemidiaphragm, from the right subhepatic space, and from the surface of the liver forms an envelope as it is removed en-bloc (Figure 18). The dissection is greatly simplified if the tumor specimen can be maintained intact. The dissection continues laterally on the right to encounter the perirenal fat covering the right kidney. Also, the right adrenal gland is visualized and avoided as tumor is stripped out of Morrison's pouch (right subhepatic space). Care is taken not to traumatize the vena cava or to disrupt caudate lobe veins that pass between the vena cava and segment 1 of the liver.
Figure 18. Removal of tumor from beneath the right hemidiaphragm, from right subhepatic
space, and from the surface of the liver. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

36
Completed right upper quadrant peritonectomy
With strong traction on the right costal margin and medial displacement of the liver, one can visualize the completed right upper quadrant peritonectomy. The anterior branch of the phrenic artery and vein are seen and have been preserved (Figure 19). The right hepatic vein and the vena cava below have been exposed. The right adrenal gland and Gerota's fascia covering the right kidney constitutes the base of the dissection. Not infrequently, tumor will be densely adherent to the tendinous mid-portion of the left or right hemidiaphragm. If this occurs, the fibrous tissue infiltrated by tumor must be resected. This usually requires a generous elliptical excision of a portion of the hemidiaphragm. The defect in the diaphragm is left open until the intraperitoneal chemotherapy is complete. Then it is closed with interrupted sutures and rarely causes respiratory problems postoperatively. Implantation of tumor cells into the pleural space must be avoided by treating the pleural space along with the peritoneal cavity with heated intraoperative intraperitoneal chemotherapy.
Figure 19. Completed right upper quadrant peritonectomy. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

37
Cholecystectomy with stripping of the hepatoduodenal ligament
The gallbladder is removed in a routine fashion from its fundus toward the cystic artery and cystic duct (Figure 20). Blunt dissection of the base of the gallbladder away from the common duct and right hepatic artery distinguishes these structures from the surrounding tumor and fatty tissue. These structures are ligated and divided.
To strip the peritoneum from the anterior aspect of the hepatoduodenal ligament, its
peritoneal reflection to the liver surface is released (14). Special care is taken not to injure the left hepatic artery, which is usually the most superficial of the portal structures. The peritoneum is firmly grasped using a Russian forceps and peeled away from the common bile duct and hepatic artery. The gallbladder with hepatoduodenal peritoneum is divided from the superior aspect of the first portion of the duodenum to release the specimen.
Figure 20. Cholecystectomy with stripping of the hepatoduodenal ligament. (From
Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

38
Circumferential resection of the hepatogastric ligament and lesser omentum by digital dissection
The triangular ligament of the left lobe of the liver was resected in performing the left
subphrenic peritonectomy. This completed the left lateral segment of the liver is retracted left to right to expose the hepatogastric ligament in its entirety. A circumferential release of this ligament from the fissure between liver segments 2, 3 and 1, and from the arcade of right gastric artery to left gastric artery along the lesser curvature of the stomach, is required (Figure 21). After electrosurgically dividing the peritoneum on the lesser curvature of the stomach, digital dissection with extreme pressure from the surgeon’s thumb and index finger separates lesser omental fat and tumor from the vascular arcade. As much of the anterior vagus nerve is spared as is possible. The tumor and fatty tissue surrounding the right and left gastric arteries are split away from the vascular arcade. In this manner the specimen is centralized over the major branches of the left gastric artery. With strong traction on the specimen, the lesser omentum is released from the left gastric artery and vein.
If an accessory left hepatic artery off the left gastric artery is present it is resected with
the lesser omentum specimen. This is done in preparation for resection of the peritoneal surfaces below this structure.
Figure 21. Circumferential resection of the hepatogastric ligament and lesser omentum by
digital dissection. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

39
Figure 22. Limits of the lesser omentectomy with stripping of the omental bursa. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)
Limits of the lesser omentectomy with stripping of the floor of the omental bursa A Dever retractor or the assistant’s fingertips beneath the left caudate lobe are positioned
to expose the entire floor of the omental bursa (Figure 22 and Figure 23). Electroevaporation of tumor from the caudate process of the left caudate lobe of the liver may be necessary to achieve this exposure. Ball-tip electrosurgery is used to cautiously divide the peritoneal reflection of liver onto the left side of the subhepatic vena cava. After the peritoneum is divided Russian forceps assist in a blunt stripping of the peritoneum from the superior recess of the omental bursa, from the crus of the right hemidiaphragm, and from beneath the portal vein. Electroevaporation of tumor from the shelf of liver parenchyma beneath the portal vein and joining right and left aspects of the caudate lobe may be required. Care is taken while stripping the floor of the omental bursa to stay superficial to the right phrenic artery. Figure 24 shows the complete cholecystectomy, lesser omentectomy and stripping of the omental bursa.

40
Figure 23. Stripping of the omental bursa. The retractor is beneath the caudate process of the
liver. The dotted line shows the peritoneal incision required to strip the floor of the omental bursa. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

41
Figure 24. Cholecystectomy, lesser omentectomy and stripping of the omental bursa
completed. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

42
Figure 25. Initiation of the pelvic peritonectomy by defining the limits of the dissection.

43
Pelvic peritonectomy with resection of the rectosigmoid colon
To initiate the pelvic dissection, the peritoneum is stripped from the posterior surface of the lower abdominal incision, exposing the rectus muscle (Figure 25). The muscular surface of the bladder is seen as ball-tip electrosurgery strips tumor-bearing peritoneum and pre-peritoneal fat from this structure. The urachus must be divided and used as a point for traction for this dissection. Round ligaments are divided as they enter the internal inguinal ring on both the right and left in the female patient (Figure 26).
The peritoneal incision around the pelvis is completed superiorly by stripping peritoneum posteriorly up to the duodenum and the Treitz ligament. Right and left ureters are identified and preserved. In females, the right and left ovarian veins are ligated and divided at the level of the lower pole of the kidney. A linear stapler is used to divide the colon at the junction of sigmoid and descending colon. The vascular supply of the distal portion of the bowel is traced back to its origin on the aorta. The inferior mesenteric artery is ligated and divided. This allows one to pack all of the viscera, including the proximal sigmoid colon, into the upper abdomen.
Figure 26. Pelvic peritonectomy. (From Sugarbaker PH: Peritonectomy procedures. Surg
Oncol Clin N Am 12:703-727, 2003)

44
Hysterectomy and transection of the rectum beneath the peritoneal reflection
Ball-tip electrosurgery is used to dissect deep to the mesorectum (Figure 27). One works in a centripetal fashion to free up the entire pelvis. An extraperitoneal suture ligation of the uterine arteries occurs just above the ureter and close to the base of the bladder. In females, the bladder is gently moved off from the cervix and the vagina is entered. The vaginal cuff anterior and posterior to the cervix is divided using ball-tip electrosurgery and the perirectal fat inferior to the posterior vaginal wall is encountered. Ball-tip electrosurgery is used to divide the perirectal fat beneath the peritoneal reflection. This ensures that all tumor which occupies the cul-de-sac is removed intact with the specimen. The mid-portion of the rectal musculature is skeletonized using ball-tip electrosurgery. A roticulator stapler (Autosuture Inc., Norwalk, CT) is used to close the rectal stump. Vaginal closure and colorectal anastomosis
Interrupted absorbable sutures are used to close the vaginal cuff and prevent leakage of fluid during intraperitoneal perfusion (Figure 28). A monofilament suture in a purse string fashion is used to secure the stapler anvil in the proximal sigmoid colon. A circular stapling device is passed into the rectum and the trochar used to penetrate the middle of the rectal staple line. The body of the circular stapler and anvil are mated and the stapler fired to complete the low colorectal anastomosis (Intraluminal Stapler 33, Ethicon, Cincinnati, OH). This anastomosis is performed after the heated intraoperative intraperitoneal chemotherapy is completed.

45
Figure 27. Resection of rectosigmoid colon beneath the peritoneal reflection. (From
Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

46
Figure 28. Complete pelvic stripping and rectosigmoid resection. (From Sugarbaker PH:
Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

47
An absolute requirement of a complication-free, low colorectal anastomosis is an absence of tension on the suture line. Adequate mobilization of the entire left colon with preservation of its blood supply is necessary. To accomplish this requires several steps.
The branches of the inferior mesenteric artery (superior hemorrhoidal, sigmoid and left
colic) are ligated as they arise from this vascular trunk. This converts the Y-configuration of these vessels to a V-configuration. This allows for great stretching of the left colic mesentery with a preservation of adequate blood supply to the distal colon (Figure 29). Then the inferior mesenteric artery is ligated and then suture ligated on the aorta. The inferior mesenteric vein is divided as it courses around the duodenum. The mesentery of the transverse colon and splenic flexure are completely elevated from the perirenal fat. Taking care to avoid the left ureter, one divides the left colon mesentery from all of its retroperitoneal attachments. These maneuvers will allow the junction of sigmoid and descending colon to reach to the low rectum for a tension-free anastomosis.
In order to ensure a safe colorectal anastomosis, one examines the proximal and distal
tissue rings for their completeness. One insufflates air under pressure into the rectum with a water-filled pelvis to check for staple closure and an air-tight anastomosis: One observes that the distal colonic segment follows the concavity of the sacrum showing that there is no tension on the stapled anastomosis. A rectal examination is performed to check for staple-line bleeding at the anastomosis.

48
Figure 29. Preservation of the intermediate vasculature to the distal colon by converting the Y-configuration of the sigmoidal vessels to a V-configuration. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

49
Total gastrectomy and reconstruction
In some patients, a total gastrectomy will be needed to clear the left upper quadrant of mucinous tumor.
To perform the gastrectomy, the esophagus is closed with a linear stapler (Ethicon TA30,
Cincinnati, OH) and then transected. The duodenum is transected just distal to the pylorus with a linear stapler. The left gastric artery and vein are ligated and suture ligated. Final attachments of the stomach to celiac lymph nodes and to the superior portion of the head of the pancreas are divided using ball-tipped electrosurgery. Great care is taken not to traumatize the anterior surface of the pancreas.
To reconstruct the gastrointestinal tract after gastrectomy that is part of a complete
cytoreduction, a duodenal exclusion operation is performed (15). This protects the esophagojejunal anastomosis. Approximately 20 cm below the ligament of Treitz, a portion of jejunum is transected with a linear stapler and brought in a retrocolic fashion up to the esophagus. The esophageal staple line is removed and a purse string suture is used to secure the anvil of a circular stapler in the distal esophagus (Ethicon ILS29, Cincinnati, OH). The staple line closing the proximal jejunum is removed and the stapler is passed approximately 5 cm into the jejunum and then the spear is passed through the jejunal wall. It is mated with the anvil within the esophagus, and the staple line is completed. The proximal jejunum is stapled off, and then the staple line inverted with interrupted sutures. All of these suture lines are performed after the heated intraoperative intraperitoneal chemotherapy has been completed.

50
The portion of jejunum proximal to the linear staple line is now brought out in the left upper quadrant as an end ostomy in order to divert all bile and digestive enzymes from the gastrointestinal tract. This diverting jejunostomy is closed between 3 and 6 months postoperatively as part of a second-look procedure (Figure 30).
Figure 30. In patients who require gastrectomy in addition to extensive cytoreduction, a high
diverting jejunostomy is performed. This ostomy is closed in approximately six months with a second-look surgery. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

51
Tubes and drains required for heated intraoperative and early postoperative intraperitoneal chemotherapy
Closed suction drains are placed in the dependant portion of the abdomen. This includes the right subhepatic space, the left subdiaphragmatic space and the pelvis (Figure 31).
Figure 31. Tubes and drains required for heated intraoperative and early postoperative
intraperitoneal chemotherapy. (From Sugarbaker PH: Peritonectomy procedures. Surg Oncol Clin N Am 12:703-727, 2003)

52
A Tenckhoff catheter (Quinton Curled Peritoneal Catheter, Quinton, Inc., Seattle, WA) is placed through the abdominal wall in order to administer heated intraoperative intraperitoneal chemotherapy. All transabdominal drains and tubes are secured in a watertight fashion with a purse string suture at the skin. If subphrenic peritonectomy was performed, right angle thoracostomy tubes (Deknatel, Floral Park, NY) are inserted in order to prevent fluid accumulation in the chest as a result of intraperitoneal chemotherapy and diaphragm stripping.
IV. Heated Intraoperative Intraperitoneal Chemotherapy (HIIC) using the Sugarbaker
Retractor
In order to optimize the delivery of heated intraoperative intraperitoneal chemotherapy, a new containment instrument has been developed. The instrument is positioned over the top of a midline abdominal incision. All components are covered by a disposable drape with a hole placed centrally to allow access of the surgeon’s double-gloved hand and arm into the open abdomen and pelvis.
The instrument is composed of two hinged bars (21 inches), two stabilization plates (19 x
9½ inches), and a lid (14 inch diameter). To assemble the instrument the hinged bars are secured one on either side of the operating table at the upper and lower aspects of the midline abdominal incision approximately six inches above the skin of the anterior abdominal wall (Thompson Surgical Instruments, Traverse City, MI). The two stainless steel stabilization plates are securely attached using plastic bands. Eight pairs of holes near the inner edge of the large central defect of the stabilization plates allow placement of eight monofilament sutures in the skin edges (Figure 32). The elevation of the edges of the abdominal incision temporarily converts the abdomen and pelvis into a reservoir for the chemotherapy solution. The abdominal and pelvic space will now accommodate two to four liters of fluid.

53
Figure 32. Sugarbaker retractor. Hinged bars are used to stabilize stainless steel plates approximately 6 inches above the anterior abdominal wall. Sutures suspend the skin edges to make a reservoir of the peritoneal space.

54
A single inflow and four outflow tubes are placed through the lateral aspect of the abdominal wall for hyperthermic peritoneal irrigation. The inflow catheter is secured to a temperature probe within the mid-abdomen. During the hyperthermic chemotherapy irrigation the inflow catheter is placed beneath the right hemidiaphragm. After the skin edges are elevated by monofilament suture, a lid, also made of stainless steel, closes off the space above the peritoneal cavity except for an access site. An impermeable disposable drape covers the entire operative field with a cruciate cut in its central portion to open the access site. The surgeon’s double-gloved arm is placed through the access site to continuously mix the heated chemotherapy solution (Figure 33). If desired to further seal off the open abdomen, the access site may be secured to the surgeon’s arm by hand assist laparoscopy equipment. If the access site is not sealed a smoke evacuator (Buffalo, Buffalo, NY) is used to create a laminar flow of air from the access site to charcoal filtration.
Figure 33. Sugarbaker retractor in place to facilitate the delivery of heated intraoperative
intraperitoneal chemotherapy.

55
V. Heater-circulator apparatus
Hyperthermic intraoperative intraperitoneal chemotherapy is administered by a continuous closed-circuit apparatus (Figure 34). There is a single inflow pump with dual inflow catheters continuously irrigating the right upper quadrant and the pelvis. There are four outflow catheter also connected to an outflow pump. The temperature is monitored at both of the inflow catheters and at a remote site within the abdomen and pelvis.
Figure 34. Diagram of the hyperthermic intraoperative intraperitoneal chemotherapy
apparatus.

56
VI. Heated intraoperative intraperitoneal chemotherapy
After the cytoreductive surgery is complete, the Tenckhoff catheter and closed suction drains are placed through the abdominal wall and made watertight with a purse string suture at the skin. Temperature probes are secured to the skin edge. Using a monofilament suture, the skin edges are elevated on the Sugarbaker retractor (Thompson Surgical Instruments, Traverse City, MI). During the 90 minutes of perfusion, all the anatomic structures within the peritoneal cavity are uniformly exposed to heat and to chemotherapy. The surgeon vigorously manipulates all viscera to keep adherence of peritoneal surfaces to a minimum. A roller pump forces the chemotherapy solution into the abdomen through the Tenckhoff catheter and pulls it out through the drains. A heat exchanger keeps the fluid being infused at 44-46°C so that the intraperitoneal fluid is maintained at 41-43°C. The smoke evacuator is used to pull air from beneath the plastic cover through activated charcoal preventing any possible contamination of air in the operating room by chemotherapy aerosols.
The standardized orders for heated intraoperative intraperitoneal chemotherapy are given
in Table 5.
Selection of the optimal intraoperative chemotherapy agent for an individual patient There are four different regimens that have been extensively tested at the Washington
Cancer Institute and are in routine use. Treatment plan A utilizes intraperitoneal mitomycin C, intraperitoneal doxorubicin, intravenous 5-fluorouracil and intravenous leucovorin. In minimally aggressive mucinous appendiceal tumors with a complete cytoreduction intraperitoneal doxorubicin is usually withheld. Also for adjuvant treatment of primary colorectal cancer the doxorubicin is withheld. With mucinous adenocarcinoma or intestinal type carcinomatosis all four drugs are used intraoperatively and four days of early postoperative intraperitoneal 5-fluorouracil also. The early postoperative 5-fluorouracil is usually withheld if the patient has failed prior intravenous treatment with this drug.
Treatment plan B is used for adjuvant treatment or for established peritoneal surface
disease from gastric cancer, ovarian cancer, mesothelioma and sarcoma. For poor prognosis gastric cancer, ovarian cancer and peritoneal mesothelioma early postoperative intraperitoneal paclitaxel is added to the intraperitoneal chemotherapy used intraoperatively.
Treatment plan C is used with early postoperative intraperitoneal 5-fluorouracil
postoperative days 1-4 for peritoneal seeding from appendiceal or colorectal adenocarcinoma in patients having no prior oxaliplatin treatment. Treatment plan D is used for carcinomatosis patients who have incomplete cytoreduction.
After the intraoperative perfusion is complete, the abdomen is suctioned dry of fluid,
reopened, and reconstructive surgery is performed. It should be emphasized that no anastomoses are constructed until after the intraoperative chemotherapy perfusion is complete.

57
TABLE 5. Standardized Orders for Heated Intraoperative Intraperitoneal Chemotherapy. A. For pseudomyxoma peritonei, adenocarcinoma from appendiceal, colonic, and rectal cancer 1. Add mitomycin C ________ mg to 2 liters of 1.5% dextrose peritoneal dialysis solution. 2. Add doxorubicin ________ mg to the same 2 liters of 1.5% dextrose peritoneal dialysis solution. 3. Dose of mitomycin C and for doxorubicin is 15 mg/m2 for each chemotherapy agent. 4. Use 33% dose reduction for heavy prior chemotherapy, marginal renal function, age greater than
60, extensive intraoperative trauma to small bowel surfaces, or prior radiotherapy. 5. Add ________ mg 5-fluorouracil (400 mg/m2) and leucovorin _________ mg (20 mg/m2) to
separate bags of 250 ml normal saline. Begin IV infusion of both drugs simultaneously with IP chemotherapy infusion.
6. Send the above to operating room _______ at _______ o'clock for 90-minute irrigation. B. For gastric and ovarian cancer, mesothelioma and sarcoma 1. Add cisplatin ________ mg to 1 liter of 1.5% dextrose peritoneal dialysis solution. Dose of
cisplatin 50 mg/m2. 2. Add doxorubicin ________ mg to same 1 liter of 1.5% dextrose peritoneal dialysis solution. Dose
of doxorubicin 15 mg/m2. 3. Use 33% dose reduction for heavy prior chemotherapy, marginal renal function, age greater than
60, extensive intraoperative trauma to small bowel surfaces, or prior radiotherapy. 4. Add ________ mg 5-fluorouracil (400 mg/m2) and leucovorin _________ mg (20 mg/m2) to
separate bags of 250 ml normal saline. Begin IV infusion of both drugs simultaneously with IP chemotherapy infusion.
5. Send the above to operating room _______ at _______ o'clock for 90-minute irrigation. C. Oxaliplatin and Intravenous 5-Fluorouracil and Leucovorin Orders
1. Add oxaliplatin ________ mg (130 mg/m2) to 2 liters 5% dextrose and water for intraperitoneal
administration. 2. Add ________ mg 5-fluorouracil (400 mg/m2) and leucovorin ________ mg (20 mg/m2) to
separate bags of 250 ml normal saline. Begin IV infusion of both drugs simultaneously with IP chemotherapy infusion.
3. Send the above to operating room _______ at _______ o'clock for 60-minute irrigation.
D. Melphalan Orders 1. Add Melphalan _________ mg (50-70 mg/m2) to 2 liters of 1.5% dextrose peritoneal dialysis
solution. 2. Send the above to operating room _______ at _______ o'clock for 60-minute irrigation.

58
VII. Early postoperative intraperitoneal chemotherapy Intraperitoneal chemotherapy following adequate cytoreduction in patients with appendiceal, colonic, rectal, or other gastrointestinal adenocarcinomas has utilized early postoperative intraperitoneal 5-fluorouracil. In patients with ovarian cancer heavily pretreated by paclitaxel, intraperitoneal 5-fluorouracil is indicated.
The standardized orders for early postoperative administration of intraperitoneal 5-fluorouracil are shown in Table 6.
TABLE 6. Early postoperative intraperitoneal chemotherapy with 5-fluorouracil. 5-fluorouracil (postoperative days 1-4 or 1-5) 1. 5-FU __________ mg (600 mg/m2 x __________ m2) (maximum dose: 1400 mg), and 50 meq
sodium bicarbonate in __________cc 1.5% dextrose peritoneal dialysis solution via intraperitoneal catheter on _________________. Last dose _________.
2. Infuse as rapidly as possible via Tenckhoff catheter. Dwell for 23 hours and drain for one hour
prior to next instillation. 3. Continue to drain abdominal cavity after last dose until Tenckhoff catheter is removed. 4. During initial 6 hours after chemotherapy infusion, patient's bed should be kept flat. The patient
should be on the right side during infusion. Turn at ½-hour post infusion onto the left side and continue to change sides at ½-hour intervals for 6 hours.
5. Monitor with pulse oximeter during the first 6 hours of intraperitoneal chemotherapy.

59
Intraperitoneal chemotherapy following adequate cytoreduction in patients with ovarian cancer, gastric cancer and peritoneal mesothelioma is now with paclitaxel in 6% hetastarch carrier solution. The standardized orders are shown in Table 7.
TABLE 7. Early postoperative intraperitoneal chemotherapy with paclitaxel. Paclitaxel (postoperative days 1-5) 1. Paclitaxel __________ mg (20-40 mg/m2 x __________ m2) (maximum dose: 80
mg) in __________cc 6% Hetastarch (B. Braun, Irvine, CA) via IP catheter on _________________. Last dose _________.
2. Infuse as rapidly as possible via Tenckhoff catheter. Dwell for 23 hours. Drain from
Tenckhoff x 15 minutes before draining all catheters for one hour prior to next instillation.
3. Use 1 liter 6% Hetastarch for body surface 1 - 2 m2, 1.5 liters for body surface > 2.0
m2. 4. Continue to drain abdominal cavity after last dose until Tenckhoff catheter is
removed. 5. During initial 6 hours after chemotherapy infusion, patient's bed should be kept flat.
The patient should be on the right side during infusion. Turn at ½-hour post infusion onto the left side and continue to change sides at ½-hour intervals for 6 hours.
6. Monitor with pulse oximeter during the first 6 hours of intraperitoneal chemotherapy

60
VIII. Clinical pathway for postoperative care The theory supporting a clinical pathway for management of patients following cytoreductive surgery and perioperative intraperitoneal chemotherapy has its major focus on complete bowel rest for 10-20 days postoperatively. The time required for the ileus to resolve depends on the patient’s condition preoperatively, the extent of the peritonectomy, and the intensity of the perioperative intraperitoneal chemotherapy. Patients who had extensive prior surgery and require time consuming lysis of adhesions will have a longer ileus. Patients who have been treated with extensive prior chemotherapy and whose wound healing has been impaired will have a prolonged ileus. Also, the extent of peritonectomy, especially the anterior parietal peritonectomy will prolong ileus. A requirement for complete bowel rest is nasogastric suctioning using a silicone Salem sump nasogastric tube (Sherwood Medical, St. Louis, MO). A large bore, no. 18 French gauge tube is used and its position within the body of the stomach is confirmed during the operative procedure. It is meticulously maintained by the nursing staff on low wall suction (approximately 30 mm/Hg). The patient is allowed ice chips ad lib in order to clear the tube within the stomach. A second requirement for complete bowel rest is total parenteral nutrition. This is given through the two-lumen intrajugular central venous line (Arrow International, Reading, PA) for approximately the first 7 postoperative days. Then the patient has a 5 French dual-lumen percutaneous intravenous central catheter (PICC line) inserted through the brachial vein under ultrasound control (Bard, Salt Lake City, UT). A biopatch is maintained at the skin exit site (Johnson and Johnson, Somerville, NJ). This PICC line is maintained and parenteral feeding continued until the patient is able to take a full complement of calories postoperatively. It is not unusual for patients to go home from the hospital still on some maintenance parenteral feeding. Multiple fluids accumulate in both the pleural and abdominal spaces postoperatively. Bilateral chest tubes are placed to be removed at postoperative days 7-14. They are never removed until the EPIC is complete.

61
Six Jackson-Pratt drains are placed (Figure 31). Two are in the pelvis next to the low colorectal anastomosis, one is beneath the right and left hemidiaphragm. A fifth drain is placed from the anterior abdominal wall down through the lesser curvature of the stomach and along the superior border of the pancreas. The sixth Jackson-Pratt drain is placed within the subcutaneous space. These drains are removed if the fluid is clear and if the volume is less than 30 cc/day. Otherwise, these closed-suction drains are left in place sometimes for three to four weeks postoperatively. The chest tubes are positioned using a “U stitch” so that they can be removed even after a tract has been established without creating a Pneumothorax. For thromboembolic prophylaxis patients are placed in venous compression stockings (Kendall, Tyco Healthcare Group, Mansfield, MA) before anesthesia is induced. These are maintained throughout the hospitalization while the patient is in bed. After the dilutional coagulopathy from cytoreductive surgery has cleared and at approximately day 7, subcutaneous heparin 5000 units twice a day is initiated. Patients are maintained under full monitoring in a surgical intensive care unit for approximately 24 hours. They are generally not extubated until major hemodynamic shifts have resolved. A majority of patients are extubated the morning following the cytoreductive surgery. Very often, the first cycle of early postoperative intraperitoneal chemotherapy is given prior to extubation.

62
IX. Results of treatment of peritoneal surface malignancy
The disease-free survival of all patients with peritoneal surface malignancy treated over the last 20 years is presented in Table 8.
Table 8. Results of treatment of peritoneal surface malignancy with cytoreductive surgery and perioperative intraperitoneal chemotherapy.
Disease State No. Patients 3-Year SurvivalAppendix cancer with carcinomatosis and pseudomyxoma peritonei syndrome after complete cytoreduction 800 83%
Primary and recurrent colon or rectal cancer with carcinomatosis and complete cytoreduction 150 41%
Peritoneal mesothelioma 100 50% Recurrent abdominopelvic sarcoma with sarcomatosis following complete cytoreduction 50 43%
Advanced primary and recurrent ovarian cancer 28 50% Symptomatic malignant ascites 16 0%

63
X. Current indications for cytoreductive surgery plus perioperative intraperitoneal chemotherapy
Currently, there are three groups of patients that may have the indications for perioperative intraperitoneal chemotherapy: Prevention of carcinomatosis or sarcomatosis after resection of primary disease, management of established peritoneal surface dissemination of gastrointestinal or gynecologic malignancy or peritoneal mesothelioma and management of debilitating malignant ascites.
A major role for intraperitoneal chemotherapy is the prevention of subsequent peritoneal carcinomatosis or sarcomatosis. It should be used in all patients who are at high risk for disease progression or peritoneal surfaces. Virtually every patient who has a free intraabdominal perforation of gastrointestinal cancer through the malignancy itself subsequently develops peritoneal carcinomatosis. Patients with primary cancer adherent to the adjacent organs or structures (T4 lesions) are at great risk for peritoneal carcinomatosis. The same is true for patients with positive peritoneal cytology. Not infrequently, patients who are undergoing the resection of a large intraabdominal tumor will have a tumor spill. This may be extremely common with advanced primary or recurrent rectal malignancy and recurrent colonic cancer. It may occur almost routinely in resections of advanced gastric cancer. If there is a tumor spill, then in order to prevent subsequent development of peritoneal carcinomatosis or sarcomatosis, intraperitoneal chemotherapy is necessary. The reports of Yu and colleagues (Taegu, Korea) show benefit in stage III and resectable stage IV gastric cancer patients (3). Also, all patients with positive pre-resection or post-resection peritoneal cytology should be treated. For colorectal cancer patient at high risk for subsequent carcinomatosis progression, include those with perforated cancers, obstructing cancers, cancers adherent to adjacent organs or structures, cancers (especially large rectal tumors) with positive margins or intraoperative tumor disruption, and cancers with positive peritoneal cytology. The same indications would apply to small bowel adenocarcinoma.
Primary retroperitoneal visceral sarcoma patients need treatment if there are positive
margins of resection, piecemeal resection, or sarcoma disruption occurring with resection. Intraperitoneal chemotherapy is an important treatment option for recurrent ovarian
malignancy. In patients with recurrent ovarian cancer who have failed systemic chemotherapy, cytoreduction is followed by intraperitoneal chemotherapy.
A final indication for intraperitoneal chemotherapy is debilitating malignant ascites. This
is one of the few instances when intraperitoneal chemotherapy is not always combined with cytoreductive surgery.

64
Table 9 presents the current indications for the use of intraperitoneal chemotherapy to treat peritoneal carcinomatosis or sarcomatosis or to prevent the progression of microscopic residual disease in high risk groups. Adenocarcinoma or sarcoma of low malignant potential may arise from many different intraabdominal sites and seed the abdominal or pelvic cavity extensively. Most of these noninvasive malignancies can be eradicated from the abdomen. Cytoreductive surgery followed by intraperitoneal chemotherapy should be considered the standard therapy for patients with pseudomyxoma peritonei syndrome and peritoneal mesothelioma. TABLE 9. Current indications for cytoreductive surgery and perioperative intraperitoneal chemotherapy.
1. Large volume of noninvasive peritoneal carcinomatosis or sarcomatosis. 2. Peritoneal mesothelioma. 3. Low volume peritoneal seeding from invasive cancer. 4. Perforated gastrointestinal cancers. 5. Cancer adherent to adjacent organs or structures. 6. Gastrointestinal cancer with positive peritoneal cytology. 7. Gastrointestinal cancer with ovarian involvement. 8. Positive margins or tumor spill intraoperatively (especially large rectal cancers). 9. Systemic chemotherapy for recurrent ovarian cancer after a long disease-free interval. 10. Palliation of patients with malignant ascites.
XI. Conclusions
Changes in the use of chemotherapy in patients with peritoneal carcinomatosis and sarcomatosis have been presented along with early favorable results of treatment. A change in the ROUTE of drug administration has occurred. Chemotherapy is given intraperitoneally, or by combined intraperitoneal and intravenous routes. Also, a change in TIMING has occurred so that chemotherapy delivery begins in the operating room and may continue for the first five postoperative days. In selecting patients with high-grade cancer for treatment, the Peritoneal Cancer Index is of crucial importance. Only patients who have a complete cytoreduction are likely to respond with long-term survival and the Peritoneal Cancer Index provides a reliable way to select these patients. The treatment of large volume/low-grade tumors following complete cytoreduction has shown beneficial results especially in the pseudomyxoma peritonei syndrome. Aggressive treatment of a large volume of high grade intraabdominal cancer is unlikely to produce long-term benefits, and is often the cause of excessive morbidity and mortality.

65
SELECTED REFERENCES 1. Jacquet P, Vidal-Jove J, Zhu BW, Sugarbaker PH: Peritoneal carcinomatosis from intra-
abdominal malignancy: Natural history and new prospects for management. Acta Belgica Chirurgica 94:191-197, 1994.
2. Sugarbaker PH, Graves T, DeBruijn EA, Cunliffe WJ, Mullins RE, Hull WE, Oliff L, Schlag
P: Rationale for early postoperative intraperitoneal chemotherapy (EPIC) in patients with advanced gastrointestinal cancer. Cancer Res 50:5790-5794, 1990.
3. Yu W, Whang I, Averbach A, Chang D, Sugarbaker PH: Prospective randomized trial of early
postoperative intraperitoneal chemotherapy as an adjuvant to resectable gastric cancer. Ann Surg 223(3):347-357, 1998.
4. Sugarbaker PH, Mora JT, Carmignani P, Stuart OA, Yoo D: Update on chemotherapeutic
agents utilized for perioperative intraperitoneal chemotherapy. Oncologist 10(2):112-122, 2005.
5. Jacquet P, Jelinek JS, Steves MA, Sugarbaker PH: Evaluation of computer tomography in
patients with peritoneal carcinomatosis. Cancer 72(5):1631-1636, 1993. 6. Jacquet P, Jelinek JS, Chang D, Koslowe P, Sugarbaker PH: Abdominal CT scan in the
selection of patients with mucinous peritoneal carcinomatosis for cytoreductive surgery. J Am College Surg 181:530-538, 1995.
7. Yan TD, Haveric N, Carmignani P, Chang D, Sugarbaker PH: Abdominal computed
tomography scans in the selection of patients with malignant peritoneal mesothelioma for comprehensive treatment with cytoreductive surgery and perioperative intraperitoneal chemotherapy. Cancer 15:839-849, 2005.
8. Esquivel J, Sugarbaker PH: Elective surgery in recurrent colon cancer with peritoneal
seeding: When to and when not to proceed. (Editorial). Cancer Therapeutics 1:321-325, 1998.
9. Berthet B, Sugarbaker TA, Chang D, Sugarbaker PH: Quantitative methodologies for
selection of patients with recurrent abdominopelvic sarcoma for treatment. Eur J Cancer 35(3):413-419, 1999.
10. Sugarbaker PH: Successful management of microscopic residual disease in large bowel
cancer. Cancer Chemother Pharmacol 43(Suppl):S15-S25, 1999. 11. Sugarbaker PH: Peritonectomy procedures. Ann Surg 221:29-42, 1995. 12. De Lima Vazquez V, Sugarbaker PH: Total anterior parietal peritonectomy. J Surg Oncol
83(4):261-263, 2003.

66
13. De Lima Vazquez V, Sugarbaker PH: Xiphoidectomy. Gastric Cancer 6:127-129, 2003. 14. De Lima Vazquez V, Sugarbaker PH: Cholecystectomy, lesser omentectomy and stripping of
the omental bursa, a peritonectomy procedure. J Surg Oncol 84:45-49, 2003. 15. Sugarbaker PH: Cytoreduction including total gastrectomy for pseudomyxoma peritonei. Br
J Surg 89(2):208-212, 2002.

67
XII. Appendix