Embed Size (px)
Citation preview

[CANCER RESEARCH 41, 3275-3280, September 1981]0008-5472/81 /0041-OOOOS02.00
Testicular Cancer as a Model for a Curable Neoplasm: The Richard andHinda Rosenthal Foundation Award Lecture1
Lawrence H. Einhorn2
Department of Medicine, Indiana University Medical Center, and Veterans' Administration Hospital, Indianapolis, Indiana 46223
Abstract
The combination of platinum, vinblastine, and bleomycin wasfirst used at Indiana University in 1974. Thirty of 47 patients(64%) survived for 5 years, and 27 (57%) are currently diseasefree (NED) and cured of their neoplasm.
From 1976 to 1978, 78 consecutive patients were enteredon a random prospective study that indicated that equal therapeutic results could be achieved with a lower dosage (0.3mg/kg) of vinblastine. Fifty-two (67%) patients are continu
ously NED, and 57 (73%) are currently NED for 2 or moreyears.
Our third-generation study, done in conjunction with the
Southeastern Cancer Study Group, tested the hypothesis of
whether maintenance vinblastine was necessary to ensureoptimal cure rates in disseminated testicular cancer. Onehundred thirteen patients entered this maintenance study, andthe results demonstrated that cure in a far-advanced cancer
could be achieved with only 12 weeks of therapy (remissioninduction) because the relapse rate in such patients was only7%. The cure rate for patients presenting with locoregionaldisease (Stages A and B) should approach 100%.
Platinum, vinblastine, and bleomycin will regularly producea 70% complete remission rate, and a further 10% of patientswill be rendered NED with surgical resection of residual disease. The relapse rate with four courses of remission inductiontherapy in a large cooperative group study (Southeastern Cancer Study Group) was only 7%.
The high success rate in disseminated disease has allowedthe option of high cure rate in Stage B disease (positiveretroperitoneal nodes) with or without adjuvant chemotherapy.At Indiana University, 137 patients have been followed withStage A and B nonseminomatous testicular cancer from 1973to 1979 with a minimum follow-up of 2 years, and currently
135 are alive and well. Successful treatment strategies intesticular cancer have yielded a cure rate unparalleled incancer treatment.
Introduction and Background
Testicular cancer accounts for less than 1% of all causes ofmale cancer in the United States. There will be only approximately 5,000 new cases in 1981, compared to over 100,000new cases of lung cancer and colorectal cancer. Nevertheless,this tumor has become a landmark cancer among medicaloncologists because it represents the first disseminated carcinoma to enjoy a high cure rate with chemotherapy. Despite therelative rarity of germ cell tumors, it is the most commoncarcinoma in the 15- to 35-year age group (14), and again it is
an extremely important disease because of the potential lossof productive years of life.
In 1960, Li et al. (13) introduced the first major thrust ofchemotherapy in advanced testicular cancer with the combination of actinomycin D, chlorambucil, and methotrexate. Further actinomycin D-based chemotherapy programs confirmed
the 50% objective response rate in patients with disseminatedtesticular cancer (15). Later in the same decade, mithramycin(12) and vinblastine (21) were two other antineoplastic agentscapable of achieving similar therapeutic results. The mostimpressive factor of these early studies was not just the 50%response rate but that for the first time CR's3 were accom
plished, although in only 10 to 20% of these patients. It is also' Presented in part at the 1981 Meeting of the American Association for
Cancer Research in Washington, D. C. Supported in part by USPHS Grant M01RROO 750-06 and Southeast Cancer Study Group Grant CA-19657.
2 American Cancer Society Professor of Clinical Oncology.
Received May 20, 1981 ; accepted June 9, 1981.
3 The abbreviations used are: CR, complete remission; NED. disease free
(nonexistent disease); VB, vinblastine plus bleomycin; PVB, platinum plus vinblastine plus bleomycin; HCG, human chorionic gonadotropin; PR, partial remission; SECSG, Southeastern Cancer Study Group.
SEPTEMBER 1981 3275
on June 29, 2018. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

L. H. Einhorn
significant to note the outcome of CR in these patients; approximately one half of the patients who achieved CR's (5 to
10% of the total patient population) were cured of their neoplasms, whereas the other half of these patients relapsed andultimately died. Death was also inevitable in patients attainingless than a CR. It is interesting to note that those patients whorelapsed after a chemotherapy-induced CR invariably would doso within 2 years, and usually within 12 months, of initiation ofchemotherapy. In other words, unlike certain slow-growing
tumors such as breast cancer or prostate cancer, we do nothave to wait 5 years or longer to learn the ultimate fate of thesepatients. Germ cell tumors are rapidly proliferating neoplasmsthat do not remain dormant for long periods of time. Thus, if apatient is NED for 2 years after initiation of chemotherapy fordisseminated testicular cancer, the probability of cure isgreater than 99%. Today, with more modern, aggressivechemotherapy and more accurate definition of CR, a patientwho is NED for 1 year has a 99% chance for cure.
In the 1970's, several new important anticancer drugs were
introduced. Bleomycin, a Japanese antitumor antibiotic, wasdemonstrated to have definite activity in germinal neoplasms(2). Although this chemotherapeutic agent was not superior toolder drugs (actinomycin D, mithramycin, or vinblastine), it wasan ¡dealdrug for combination chemotherapy because of itslack of myelosuppression.
Samuels was the first to combine vinblastine and bleomycinsuccessfully, and this apparently synergistic two-drug regimen
represented a major advance. This apparent clinical synergismwas not observed in studies combining actinomycin, a drug aseffective as vinblastine in single-agent studies, and bleomycin.
A possible explanation for this synergism is that bleomycin, invitro, is most effective in killing Chinese hamster ovary cells inmitosis and that vinblastine produces an arrest in the mitoticphase of the cell cycle (1). Initial studies (VB-I) with VB used
vinblastine (0.4 to 0.6 mg/kg) plus bleomycin (15 mg/sq m)twice weekly. There were 17 of 51 (33%) CR's, with a relapse
rate of 23% (23). In 1973, Samuels switched from intermittent-to continuous-infusion bleomycin, and this VB-III program pro
duced a 57% CR rate (52 of 92 patients), with 41 patients(45%) remaining alive and NED (22). VB represented a majoradvance in the early 1970's in the treatment of disseminated
testicular cancer. Another major advance was discovery of theactivity of c/s-diamminedichloroplatinum in germinal neoplasms
(11 ). Platinum is the first heavy metal ever to be used successfully as an antineoplastic agent. This drug is also ideal forcombination chemotherapy because of its relative lack of myelosuppression.
With these historical data as a background, we began studiesin 1974 with PVB in disseminated testicular cancer.
Platinum Plus Vinblastine Plus Bleomycin
Our first-generation study with this three-drug combination
began in August 1974 and concluded in June 1976 (5). Thetherapy regimen for these 47 patients is shown in Table 1, withan initial "high" vinblastine dosage of 0.4 mg/kg, patternedafter Samuels' studies with VB. Most patients received three
courses of platinum; however, if a CR was not achieved, afourth course was administered. We were not able to discernany value in exceeding four courses of platinum because noneof those patients achieved a CR with a fifth or sixth course if
Table 1
Platinum + vinblastine + bleomycin
Platinum 20 mg/sq m ¡.v.for 5 days every 3 wk (3-4 courses)Vinblastine 0.2 mg/kg i.v. for 2 days every 3 wk (4 courses)Bleomycin 30 units i.v. push weekly for 12 mos.Vinblastine 0.3 mg/kg monthly for 20 mos. (maintenance)
Table 2
Results withPVBPatients
CRPRNED with PVB + surgeryNo. presently NED4733
(70)a
14(30)5(11)
27 (57)' Numbers in parentheses, percentage.
they failed to be NED with three to four courses. After completion of the 12 weeks of remission induction, maintenancetherapy was given with vinblastine (0.3 mg/kg) every 4 weeksfor a total of 2 years of chemotherapy.
Thirty-three of 47 évaluable patients (70%) achieved CR(defined as a complete disappearance of all clinical, radio-graphic, and biochemical evidence of disease, including normalwhole-lung tomograms, serum HCG, and a-fetoprotein done by
radioimmunoassay). The remaining 14 patients all achieved aPR. Clearly, a PR is not a laudable goal to strive for in thisyoung patient population, inasmuch as failure to eradicate alldisease dooms the patient to eventual progression of diseaseand death. However, five of these 14 patients had such significant cytoreduction with chemotherapy alone that they becamecandidates for surgical resection of residual localized disease.The therapeutic results are outlined in Table 2. All patientshave been followed for a minimum of 5 years. The 5-yearsurvival was 64% (30 of 47), and 27 patients (57%) arecurrently alive and cured of their cancer. We have seen onlyone episode of second cancer, and that was probably attributable to radiotherapy. This particular patient received 4500rads to a wide abdominal field for unresectable teratocarci-
noma, and he relapsed with disease in the abdomen and chestseveral months later. He achieved a CR with PVB for more than5 years but subsequently developed an angiosarcoma of thesmall bowel (in the irradiated field) and succumbed from widespread hepatic and pulmonary métastases.
We have not observed any late complications from PVB,except a high incidence of azoospermia due to impaired sper-
matogenesis from the effect of platinum on the remaining testis.There were no cases of progressive azotemia or pulmonaryfibrosis beyond remission induction therapy. Only six patientsrelapsed and, as was the case in the actinomycin D studiesfrom a decade earlier, late relapses were not seen. All relapsesoccurred within 1 year of initiation of chemotherapy with theexception of a single late relapse at 17 months.
The toxicity and prognostic variables have been describedin detail in our previous publications (5, 7). The most serioustoxic effect was related to the high dose of vinblastine because38% of these 47 patients developed granulocytopenic feversand 15% had documented sepsis. Although we were appropriately concerned about this toxicity and felt that it was necessary to try to mitigate the side effects shown in Table 3, wefelt that it was even more important to maintain the therapeuticresults, inasmuch as approximately 60% of these patients werecured. No treatment program with less toxicity was approach-
3276 CANCER RESEARCH VOL. 41
on June 29, 2018. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Testicular Cancer as Model for Curable Neoplasm
Table 3
PVB ±Adriamycin
Table 4
PVB ±Adriamycin and toxicity
R
AN-
Do-MI-
ZE
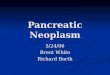
Platinum, 20 mg/sq. m for 5 days evry 3 wk (3-4 courses)Vinblastine. 0.4 mg/kg every 3 wkBleomycin, 30 units i.v. weekly for 12 wk
Platinum, 20 mg/sq m for 5 days every 3 wk (3-4 courses)Vinblasttine, 0.3 mg/kg very 3 wkBleomycin, 30 units i.v. weekly for 12 wk
Platinum, 20 mg/sq m for 5 days every 3 wk (3-4 courses)Vinblastine, 0.2 mg/kg every 3 wkBleomycin, 30 units i.v. weekly for 12 wkAdriamycin, 50 mg/sq m every 3 wk
After completion of 12 wk of bleomycin maintenance therapy on all three armsto be Vinblastine, 0.3 mg/kg monthly for 20 mos.
¡ngthis cure rate during this time period. The hematologicaltoxicity during remission induction was prominent but considerably less severe than that seen with remission inductionregimens used in adult myeloblastic leukemia. Intensive therapy in young patients with acute myeloblastic leukemia isunquestioned, although the ultimate cure rate in this disease isonly about 10%. Nevertheless, our concern to attempt to lessenthe hematological toxicity, if it would not lower the therapeuticindex, led to our second-generation study.
PVB ±Adriamycin
From June 1976 to June 1978, 78 consecutive patients wereentered in a three-armed random prospective study depictedin Table 3 (7). The main purpose of this study was to determineif we could reduce the toxicity but maintain the therapeuticsuccess of PVB by reducing the Vinblastine dosage from 0.4 to0.3 mg/kg. A third arm tested whether we could achieve evenhigher CR rates and long-term survival by adding a fourthactive drug, Adriamycin (17), to the PVB regimen. From 1974to 1976, when we were evaluating our initial PVB regimen, wetreated ten patients with far-advanced disease refractory toVinblastine and bleomycin (and frequently other chemothera-peutic agents) with platinum plus Adriamycin (6). This two-drug
regimen produced one CR and nine PRs in ten patients withfar-advanced refractory disease, and we felt that these results
were amply encouraging to warrant investigation of Adriamycinas first-line chemotherapy in combination with PVB.
Seventy-eight patients were entered in this study, and allpatients have been followed for over 3 years. The degree ofmyelosuppression for high-dose Vinblastine (0.4 mg/kg) wassimilar to that in our original PVB study. The 25% reduction inthe Vinblastine dosage resulted in the expected decrease inhematological toxicity (Table 4).
The therapeutic results are shown in Table 5. The overall CRrate (65%) and surgical resection rate for localized residualdisease (17%) were remarkably similar to our original PVBstudy. The therapeutic results are almost identical on the threeseparate induction arms; specifically, we could not demonstrate any therapeutic advantage for the more toxic Vinblastinedosage of 0.4 mg/kg. Multiple prognostic variables were analyzed between the two PVB arms, and no difference in favor ofthe reduced dose of Vinblastine could be ascertained (7). Onthe basis of the results of this random prospective study, weno longer use or recommend the higher dose (0.4 mg/kg) ofVinblastine in PVB studies.
PVB (Vinblastine. 0.3 mg/kg)PVB (Vinblastine, 0.4 mg/kg)PVB + AdriamycinGranulocytopenic
fevers4(15)"
9(35)6(24)Documented
sepsis0
3(12)1 (4)
Number's in parentheses, percentage.
Table 5
PVB ±Adriamycin results
PVB(Vinblastine,
0.4 rng/kg)PVB
(Vinblastine.0.3 mg/kg)
PVB +Adriamycin
TotalNo.
ofpatients26
272578CR1
7(65)"16(59)18(72)
51 (65)NEDafter
surgery6(23)
5(19)2
(8)
13(17)Re
lapses5(22)
2(9)3(15)
10(16)Contin
uouslyNED18(69)
17(63)1
7 (68)
52 (67)Pres
entlyNED20
(77)
19(70)18(72)
57 (73)
Numbers in parentheses, percentage.
The relapse rate in this study was 16%, with all ten relapsesoccurring within 1 year of initiation of platinum combinationchemotherapy. This has been a constant in all our PVB studies,and we feel that we have data to support the contention that a1-year NED survival with PVB in disseminated testicular cancerhas a 99% chance of remaining NED, and a 2-year NED
survival is tantamount to a cure.We have analyzed a variety of suspected prognostic vari
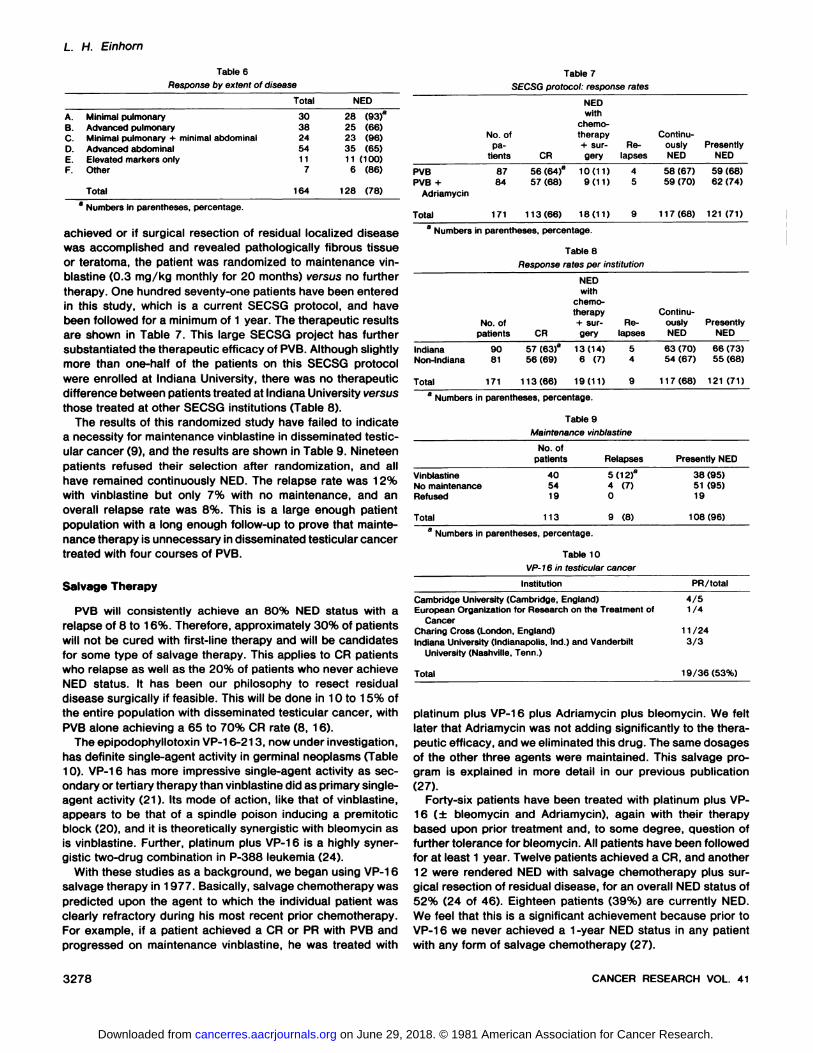
ables, and the only determinant to achieving CR was extent ofdisease. Table 6 delineates the important relationship of tumorvolume and ability to achieve NED status in the first 164patients treated with PVB (± Adriamycin) from 1974 through1978. Histology, prior treatment, age, and elevation of HCG,a-fetoprotein, or lactic dehydrogenase were not found to be
independent prognostic variables.Advanced pulmonary métastaseswere defined (Table 6) as
pulmonary métastasesgreater than 2 cm in diameter or greaterthan five métastases per lung. Advanced abdominal diseasemeant palpable abdominal mass and/or hepatic métastases.This is far from an ideal classification system; e.g., the overwhelming majority of patients with a large palpable abdominalmass (Stage B3 disease) as their only area of metastatic spreadwill be cured with PVB and surgical resection of the residualpost-PVB abnormality on abdominal computer-assisted tomog
raphy scan. However, the cure rate for patients with massivepulmonary métastasesand advanced abdominal disease is lessthan 50%.
Maintenance Therapy
The role of maintenance therapy in disseminated testicularcancer has never been established. It is quite possible that, ina disease where remission induction therapy is so effective andCR can be defined so accurately, maintenance therapy may beunnecessary. To test this hypothesis, we started our "third-generation" study in June 1978. All patients received induction
therapy with either PVB (0.3 mg/kg) or PVB plus Adriamycin(the bottom two arms of Table 3). To ensure uniformity, allpatients received four courses of platinum. If a CR was
SEPTEMBER 1981 3277
on June 29, 2018. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
L. H. Einhorn
Table 6
flesponse by extent of diseaseTable 7
SECSG protocol: response rates
A.BCD.E.F.MinimalpulmonaryAdvancedpulmonaryMinimal
pulmonary + minimalabdominalAdvancedabdominalElevated
markersonlyOtherTotalTotal30382454117164NED28
(93)"25
(66)23<96)35(65)11(100)6
(86)128
(78)8 Numbers in parentheses, percentage.
achieved or if surgical resection of residual localized diseasewas accomplished and revealed pathologically fibrous tissueor teratoma, the patient was randomized to maintenance vin-
blastine (0.3 mg/kg monthly for 20 months) versus no furthertherapy. One hundred seventy-one patients have been entered
in this study, which is a current SECSG protocol, and havebeen followed for a minimum of 1 year. The therapeutic resultsare shown in Table 7. This large SECSG project has furthersubstantiated the therapeutic efficacy of PVB. Although slightlymore than one-half of the patients on this SECSG protocol
were enrolled at Indiana University, there was no therapeuticdifference between patients treated at Indiana University versusthose treated at other SECSG institutions (Table 8).
The results of this randomized study have failed to indicatea necessity for maintenance vinblastine in disseminated testic-
ular cancer (9), and the results are shown in Table 9. Nineteenpatients refused their selection after randomization, and allhave remained continuously NED. The relapse rate was 12%with vinblastine but only 7% with no maintenance, and anoverall relapse rate was 8%. This is a large enough patientpopulation with a long enough follow-up to prove that mainte
nance therapy is unnecessary in disseminated testicular cancertreated with four courses of PVB.
Salvage Therapy
PVB will consistently achieve an 80% NED status with arelapse of 8 to 16%. Therefore, approximately 30% of patientswill not be cured with first-line therapy and will be candidates
for some type of salvage therapy. This applies to CR patientswho relapse as well as the 20% of patients who never achieveNED status. It has been our philosophy to resect residualdisease surgically if feasible. This will be done in 10 to 15% ofthe entire population with disseminated testicular cancer, withPVB alone achieving a 65 to 70% CR rate (8, 16).
The epipodophyllotoxin VP-16-213, now under investigation,has definite single-agent activity in germinal neoplasms (Table10). VP-16 has more impressive single-agent activity as secondary or tertiary therapy than vinblastine did as primary single-
agent activity (21). Its mode of action, like that of vinblastine,appears to be that of a spindle poison inducing a premitoticblock (20), and it is theoretically synergistic with bleomycin asis vinblastine. Further, platinum plus VP-16 is a highly synergistic two-drug combination in P-388 leukemia (24).
With these studies as a background, we began using VP-16
salvage therapy in 1977. Basically, salvage chemotherapy waspredicted upon the agent to which the individual patient wasclearly refractory during his most recent prior chemotherapy.For example, if a patient achieved a CR or PR with PVB andprogressed on maintenance vinblastine, he was treated with
PVBPVB+AdriamycinTotalNo.
ofpa
tients8784171CR56(64)"57
(68)113(66)NED
withchemotherapy+
surgery10(11)9(11)18(11)Relapses459Continu
ouslyNED58
(67)59(70)1
17 (68)PresentlyNED59
(68)62(74)121
(71)" Numbers in parentheses, percentage.
Table 8
Response rates per institution
IndianaNon-IndianaTotalNo.
ofpatients9081171CR57
(63)a56
(69)1
13 (66)NEDwith
chemotherapy+
surgery13(14)6
(7)19(11)Re
lapses549ContinuouslyNED63
(70)54(67)1
17 (68)PresentlyNED66
(73)55(68)121
(71)a Numbers in parentheses, percentage.
Table 9
Maintenance vinblastine
VinblastineNomaintenanceRefusedTotalNo.
ofpatients405419113Relapses5
(12)a4
(7)09
(8)Presently
NED38
(95)51(95)19108(96)
Numbers in parentheses, percentage.
Table 10VP- 76 in testicular cancer
Institution PR/total
Cambridge University (Cambridge, England) 4/5European Organization for Research on the Treatment of 1/4
CancerCharing Cross (London, England) 11/24Indiana University (Indianapolis, Ind.) and Vanderbilt 3/3
University (Nashville, Tenn.)
Total 19/36(53%)
platinum plus VP-16 plus Adriamycin plus bleomycin. We felt
later that Adriamycin was not adding significantly to the therapeutic efficacy, and we eliminated this drug. The same dosagesof the other three agents were maintained. This salvage program is explained in more detail in our previous publication(27).
Forty-six patients have been treated with platinum plus VP-16 (± bleomycin and Adriamycin), again with their therapybased upon prior treatment and, to some degree, question offurther tolerance for bleomycin. All patients have been followedfor at least 1 year. Twelve patients achieved a CR, and another12 were rendered NED with salvage chemotherapy plus surgical resection of residual disease, for an overall NED status of52% (24 of 46). Eighteen patients (39%) are currently NED.We feel that this is a significant achievement because prior toVP-16 we never achieved a 1-year NED status in any patient
with any form of salvage chemotherapy (27).
3278 CANCER RESEARCH VOL. 41
on June 29, 2018. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Testicular Cancer as Model for Curable Neoplasm
Adjuvant Therapy
Adjuvant therapy appears attractive in patients with Stage B(positive nodes at the time of retroperitoneal lymphadenec-
tomy) disease because the surgical cure rate is only 50 to 60%(4). Clearly, adjuvant PVB would greatly reduce, if not eliminate, the probability of relapse in such patients. It is our belief,however, that a similar 100% cure rate can be attained inStage B disease without adjuvant therapy. The majority ofsurgical relapses occurs during the first postoperative year,with occasional relapses during the second year and onlyanecdotal recurrences subsequently. PVB will have a 98 to100% CR rate in patients with minimal metastatic disease (5,7, 9), and we have the capability to ensure that if a patientrelapses after lymphadenectomy he will do so with minimalrather than massive disease. Postoperatively, we recommendmonthly chest X-rays, HCG, and a-fetoprotein determinations
as well as a routine physical examination for the first postoperative year. The same studies are recommended every othermonth during the second year and then every 6 to 12 monthsthereafter.
Sixty-three patients with Stage A disease (negative lymphad-
enectomies) have been followed for 2 or more years. Fivepatients (8%) relapsed postoperatively, but all were cured withPVB with the postoperative follow-up mentioned above (Table
11).From 1973 to 1976, 30 consecutive patients were treated
with adjuvant actinomycin D. The relapse rate (47%) wassimilar to the expected relapse rate with no adjuvant therapy.Again all relapses were treated with PVB, however, and allachieved CR. One patient relapsed after PVB and died. From1976 to 1979, most patients with Stage B disease were fol-
Table 11
StageANo.
of patientsRelapsesPresently NED635
(8)"
63 (100)
Numbers in parentheses, percentage.
Table 12
Stage B
No. of patients Relapses Presently NED
ActinomycinDNoadjuvantpvr"30311314(47)"12(40)029
(97)30(97)13
Numbers in parentheses, percentage.' Two courses of adjuvant PVB postoperatively.
lowed expectantly with no adjuvant therapy. Twelve of 31 suchpatients relapsed, but all were subsequently cured with PVB.One postoperative patient died of unrelated causes 6 monthsafter surgery.
Despite one set of data indicating a cure rate of almost 100%without aggressive adjuvant therapy, we felt that it was important to answer this significant research question. As a pilotstudy for the proposed intergroup adjuvant study, we entered13 patients with Stage B2 disease (grossly positive nodes) andgave them two courses of PVB. All 13 remain continuouslyNED for 2 or more years. The results of these studies for StageA and B patients are shown in Tables 11 and 12.
At the present time, we participate in the national intergroupadjuvant study for patients with Stage B disease. This studyrandomizes patients to two courses of adjuvant platinum combination chemotherapy versus observation as outlined abovewith use of chemotherapy only if the patient relapses postoperatively. There have been no relapses with adjuvant platinumcombination chemotherapy, but it is expected that, if there isa difference in overall survival for patients receiving twocourses of platinum combination chemotherapy as prophylaxisversus observation, it will be a small difference requiring a well-
designed randomized study to answer.Thus, overall, at Indiana University, 137 patients have been
followed with Stages A and B nonseminomatous testicularcancer from 1973 to 1979 with a minimum follow-up of 2 years.Overall, 135 of 137 patients are alive and well. The integrationof orchiectomy and lymphadenectomy with PVB chemotherapy, when indicated, has yielded a cure rate unparalleled incancer treatment.
Conclusion
Data have been presented indicating that the cure rate forStage A and B nonseminomatous testicular cancer shouldapproach 100%. Data have also been presented for patientswith Stage C disease, indicating a 70% cure rate with PVB in296 patients with disseminated disease (5, 7, 9). The conceptsof PVB therapy have been used at several other medicalcenters in this country (3,10), cooperative groups (26), Canada(19), and Europe (18, 25). The results of these other PVBstudies are illustrated in Table 13. There is a marked uniformityworldwide with PVB in disseminated testicular cancer.
There is no question today about the curability of disseminated testicular cancer. In the 1960s and early 1970s, curativechemotherapy was predominantly limited to the hematological
Table 13
PVB at other institutions
AuthorRamseyOliverStoterBoslGarnickTortiEinhornTotalRef.19182531026gInstitutionsUniversity
ofManitobaSt.Bartholomews(London)NetherlandsUniversity
ofMinnesota(Minneapolis,Minn.)Sidney
Farber CancerInstitute(Boston,Mass.)NCOG"SECSGCNo.14207128255881297CR10(71)a10(50)41
(58)23
(82)1
5(60)46
(79)57
(70)202
(68)NED
+surgery1
(7)2(10)5
(7)8(32)7
(9)23
(8)Presently
NED1
1(78)9(45)43(61)23
(82)23(92)42
(72)54(67)205
(69)" Numbers in parentheses, percentage.6 NCOG, Northern California Oncology Group.c Non-Indiana University Patients.
SEPTEMBER 1981 3279
on June 29, 2018. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

L. H. Einhorn
cancers. Testicular cancer is a solid tumor, and treatment of itrequired merely finding an apparently synergistic two-drug
regimen (vinblastine and bleomycin) and combining it withplatinum (then a drug under investigation), which had shown ahigh level of activity in refractory germinal neoplasms. I feelstrongly that the success rate in testicular cancer will beduplicated in the future in other chemosensitive tumors suchas small-cell lung cancer and ovarian cancer. These two dis
eases are at a historical point very similar to that for testicularcancer a decade ago; it is hoped that appropriate combinationregimens will be devised with current and future drugs for thesetumors and that they will make a similar quantum jump forwardin curative therapy.
References
1. Barranco, S. C., and Humphrey. R. M. The effects of bleomycin on survivaland cell progression in Chinese hamster cells in vitro. Cancer Res.. 3Õ:1218-1223. 1971.
2. Blum, R. H.. Carter, S., and Agre. K. A clinical review of bleomycin—a newantineoplastic agent. Cancer (Phila.), 31: 903-914, 1973.
3. Bosl. G. J., Lange, P. H., Fraley. E. E., Nochomovity, L. E., Rosai, J.,Vogelzang, N.. Johnson, K.. Goldman. A., and Kennedy, B. J. Vinblastine,bleomycin, and c/s-diamminedichloroplatinum in the treatment of advancedtesticular carcinoma. Am J. Med., 68. 492-496, 1980.
4. Donohue, J. P., Perez, J. M., and Einhorn, L. H. Improved management ofnon-seminomatous testis tumors. J. Urol., 121: 425-428, 1979.
5. Einhorn, L. H., and Donohue, J. c/s-Diamminedichloroplatinum, vinblastineand bleomycin combination chemotherapy in disseminated testicular cancer.Ann. Intern. Med., 87: 293-298, 1977.
6. Einhorn, L. H., and Williams, S. D. Combination chemotherapy with c/s-diamminedichloroplatinum and Adriamycin in testicular cancer refractory tovinblastine and bleomycin. Cancer Treat. Rep.. 62. 1351-1353, 1978.
7. Einhorn, L. H., and Williams, S. D. Chemotherapy of disseminated testicularcancer. Cancer (Phila.), 46: 1339-1344, 1980.
8. Einhorn, L. H.. Williams, S. D., Mandelbaum. I., and Donohue. J. P. Surgicalresection in disseminated testicular cancer following chemotherapeutic cy-
toreduction. Cancer (Phila.). in press, 1981.9. Einhorn, L. H., Williams. S. D., Turner, S., Trôner, M., and Greco. F. A. The
role of maintenance therapy in disseminated testicular cancer: a Southeastern Cancer Study Group (SECSG) protocol. Proc. Am. Assoc. Cancer Res.,22:474, 1981.
10. Garnick. M. B., Cannellos, G. P., Richie, J. P., and Stark, J. J. Sequentialcombination chemotherapy and surgery for disseminated testicular cancer:c/s-dichlorodiammineplatinum (II), vinblastine and bleomycin remission-induction therapy followed by cyclophosphamide and Adriamycin. Cancer
Treat. Rep., 63. 1681-1686, 1979.11. Higby. D. J., Wallace. H. J., Albert, D. J., and Holland, J. F. Diaminodichlo-
roplatinum: a phase I study showing responses in testicular and other solidtumors. Cancer (Phila.), 33: 1219-1225, 1974.
12. Kennedy. B. J. Mithramycin therapy in advanced testicular neoplasms.Cancer (Phila.). 26: 755-766, 1970.
13. Li, M. C., Whitmore, W. F., Golbey, R., andGrabstad, H. Effects of combineddrug therapy on metastatic cancer of the testis. J. Am. Med. Assoc., »74:145-153, 1960.
14. MacKay, E. N., and Sellers. A. H. A statistical review of malignant testiculartumors based on the experience of the Ontario Cancer Foundation Clinics,1938-1961. Can. Med. Assoc. J., 94: 889-899, 1966.
15. MacKenzie, A. R. Chemotherapy of metastatic testis cancer—results in 154patients. Cancer (Phila.), 19: 1369-1376, 1966.
16. Mandelbaum, I., Williams, S. D., and Einhorn, L. H. Aggressive surgicalmanagement of testicular carcinoma metastatic to lungs and mediastinum.Ann. Thorac. Surg., 30: 224-229, 1980.
17. Monfardini. S.. Bajetta, E., Musumeci, R., and Bonadonna, G. Clinical useof Adriamycin in advanced testicular cancer. J. Urol., 108: 293-296, 1972.
18. Oliver, R. T D., Rohatiner, A. A., Wrigley, P. F. M., and Malpas, J. S.Chemotherapy of metastatic testicular tumors. Br. J. Urol.. 52:34-37, 1980.
19. Ramsey, E. W., Bowmen, D. M., and Weinerman. B. The management ofdisseminated testicular cancer. Br. J. Urol.. 52: 45-49, 1980.
20. Rozencweig, M., Vontloff, D. D., Henney, J. E.. and Muggia, F. M. VM 26and VP-16-213: a comparative analysis. Cancer (Phila.), 40: 334-342.1977.
21. Samuels, M. L., and Howe, C. D. Vinblastine in the management of testicularcancer. Cancer (Phila.), 25: 1009-1017, 1970.
22. Samuels, M. L., Lanzotti, V. J., Boyle, L. E., Holoye, P. Y., and Johnson, D.E. An update of the Velban-bleomycin program in testicular neoplasia witha note on c/s-dichlorodiammineplatinum. In: D. E. Johnson and M. Samuels,(eds ), Cancer of the Genitourinary Tract, pp. 159-172. New York: RavenPress. 1979.
23. Samuels, M. L., Lanzotti, V. J., Holoye, P. Y., Boyle, L. E., Smith, T. L., andJohnson, D. E. Combination chemotherapy in germinal cell tumors. CancerTreat. Rev.. 3: 185-204, 1976.
24. Schabel. F. M., Trader. M. W., Laster, W. R., Corbett, T. H., and Griswold,D. P. C/s-dichlorodiammineplatinum II: combination chemotherapy andcross-resistance studies with tumors of mice. Cancer Treat. Rep.. 63:1459-1473, 1979.
25. Stoter, G., Sleijfer, D. T., Vendrik, C. P. J., Koops, H. S.. Struyvenburg, A..Oosterom, A. T., Brouwers, T. M., and Pinedo, H. M. Combination chemotherapy with c/s-diammine-dichloro-platinum, vinblastine, and bleomycin inadvanced testicular non-seminoma. Lancet, ): 941-945, 1979.
26. Torti, F. M., Krikorian. J., Daniels, J., Master, D.. Cumes, D., Spaulding, J.,Blane, C., Chak, L., Yu, K. P., Hannigan, J., and Carter, S. K. Platinum,vinblastine, and bleomycin induction without maintenance therapy in testicular carcinoma. Proc. Am. Assoc. Cancer Res., 22: 473, 1981.
27. Williams, S. D.. Einhorn, L. H.. Greco, F. A., Oldham, R., and Fletcher, R.VP-16-213 salvage therapy for refractory germinal neoplasms. Cancer(Phila.), 46: 2154-2158. 1980.
3280 CANCER RESEARCH VOL. 41
on June 29, 2018. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1981;41:3275-3280. Cancer Res Lawrence H. Einhorn Richard and Hinda Rosenthal Foundation Award LectureTesticular Cancer as a Model for a Curable Neoplasm: The
Updated version
http://cancerres.aacrjournals.org/content/41/9_Part_1/3275
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/41/9_Part_1/3275To request permission to re-use all or part of this article, use this link
on June 29, 2018. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from






![Isolated Testicular Tuberculosis Mimicking Testicular ... involvement, but testicular involvement is an unusual clinical condition [3]. In this report, a case with isolated testicular](https://img.pdfslide.net/doc/110x75/5f3d57bf74280d66ef795ba2/isolated-testicular-tuberculosis-mimicking-testicular-involvement-but-testicular.jpg)