Embed Size (px)
Citation preview

8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 1/8
Tetralogy of Fallot
Introduction:
Tetralogy of Fallot is a congenital heart defect. This type of heart defect changes the normal flow
of blood through the heart. It is the most common heart defect in children. The condition causes
mixing of oxygen-poor blood with the oxygen-rich blood being pumped out of the heart and into
the circulatory system of blood vessels.
It refers to a combination of abnormalities with four key features:
1)
P ulmonary stenosis: A narrowing of the right ventricular outflow tract and can occur
at the pulmonary valve (valvular stenosis) or just below the pulmonary valve(infundibular stenosis). Infundibular pulmonic stenosis is mostly caused by
overgrowth of the heart muscle wall (hypertrophy of the septoparietal trabeculae),
however the events leading to the formation of the overriding aorta are also believed
to be a cause. The pulmonic stenosis is the major cause of the malformations, with
the other associated malformations acting as compensatory mechanisms to the
pulmonic stenosis. The degree of stenosis varies between individuals with TOF, and
is the primary determinant of symptoms and severity. This malformation is
infrequently described as sub-pulmonary stenosis or subpulmonary obstruction .
2)
V entricular septal defect: A hole between the two bottom chambers (ventricles) of
the heart. The defect is centered on the most superior aspect of the ventricular septum
(the outlet septum), and in the majority of cases is single and large. In some cases
thickening of the septum (septal hypertrophy) can narrow the margins of the defect.
3)
³ Ov erriding´ aorta : An aortic valve with biventricular connection, that is, it is
situated above the ventricular septal defect and connected to both the right and the
left ventricle. The degree to which the aorta is attached to the right ventricle is
referred to as its degree of "override." The aortic root can be displaced toward the
front (anteriorly) or directly above the septal defect, but it is always abnormally
located to the right of the root of the pulmonary artery. The degree of override is
quite variable, with 5-95% of the valve being connected to the right ventricle.
4) Right v entricular hypertrophy : The right ventricle is more muscular than normal,
causing a characteristic boot-shaped (coeur-en-sabot) appearance as seen by chest X-
ray. Due to the misarrangement of the external ventricular septum, the rightventricular wall increases in size to deal with the increased obstruction to the right
outflow tract. This feature is now generally agreed to be a secondary anomaly, as the
level of hypertrophy generally increases with age

8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 2/8
C ause:
U nknown
Risk Factors:
y
A viral illness in the mother, such as rubella (German measles), during pregnancy
y
M aternal alcoholism
y
P oor nutrition
y
A mother older than 40
y
A parent with tetralogy of Fallot
y
B abies who are also born with Down syndrome or DiGeorge syndrome
y
Diabetes
S igns and S ymptoms:
y
A bluish coloration of the skin caused by blood low in oxygen (cyanosis)
y
S hortness of breath and rapid breathing, especially during feeding
y
L oss of consciousness (fainting)
y
C lubbing of fingers and toes ² an abnormal, rounded shape of the nail bed
y
P oor weight gain
y
Tiring easily during play
y
Irritability
y
A heart murmur
A natomy and P hysiology:
Heart De v elopment
The heart begins in the embryo from day 18 and is complete by day 56. A primitive straight
cardiac tube composed of an outer myocardium and an inner endocardium loops to form a
primitive atrium and ventricle, followed rapidly by a large truncus arteriosus. The tube doubles
over on itself during the second month of gestation to form two parallel pumping system, each
having two chambers and a great artery ( the truncus arteriosus). As a consequence of this
doubling, the heart begins to situate in the left side of the chest. An endocardial cushion develops
within the common chamber and is the first of the structures to divide the chambers of heart.
From the endocardial cushion, the mitral and tricuspid orifices develop. The large truncus
divides into the aorta and pulmonary arteries. Rotation of the truncus coils the
aortopulmonaryseptum and creates the normal spiral relationship between the aorta and
pulmonary artery. The truncus arteriosus is connected to the dorsal aorta by different times
during the formation of the heart and vessels. Abnormalities of the regression of the arch system

8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 3/8
in a number of sites can produce a wide variety of arch abnormalities. P artitioning of the heart is
accomplished by septa that form actively and passively. The major septa of the heart are formed
between the 27 th and 37 th days of development.
T he Normal Heart and How It Works
The normal heart is a strong, hard-working pump made of muscle tissue. It¶s about the size of a
person¶s fist.
The heart has four chambers. The upper two chambers are the atria, and the lower two are the
ventricles (Figure A). B lood is pumped through the chambers, aided by four heart valves. The
valves open and close to let the blood flow in only one direction.
The four heart valves are:
1.
the tricuspid valve, located between the right
atrium and the right ventricle;
2.
the pulmonary (pulmonic) valve, between the
right ventricle and the pulmonary artery;
3.
the mitral valve, between the left atrium and left
ventricle;
4. the aortic valve, between the left ventricle
and the aorta.
Each valve has a set of ³flaps´ (also called leaflets or cusps). The mitral valve normally has two
flaps; the others have three.
Dark bluish blood, low inoxygen, flows back to the heart
after circulating through the
body. It returns to the heart
through veins and enters the
right atrium. This chamber
empties blood through the
tricuspid valve ( B ) into the right
ventricle. The right ventricle
pumps the blood under low
pressure through the pulmonary
valve into the pulmonary artery.
From there the blood goes to the lungs where it gets fresh oxygen ( C ).
8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 4/8
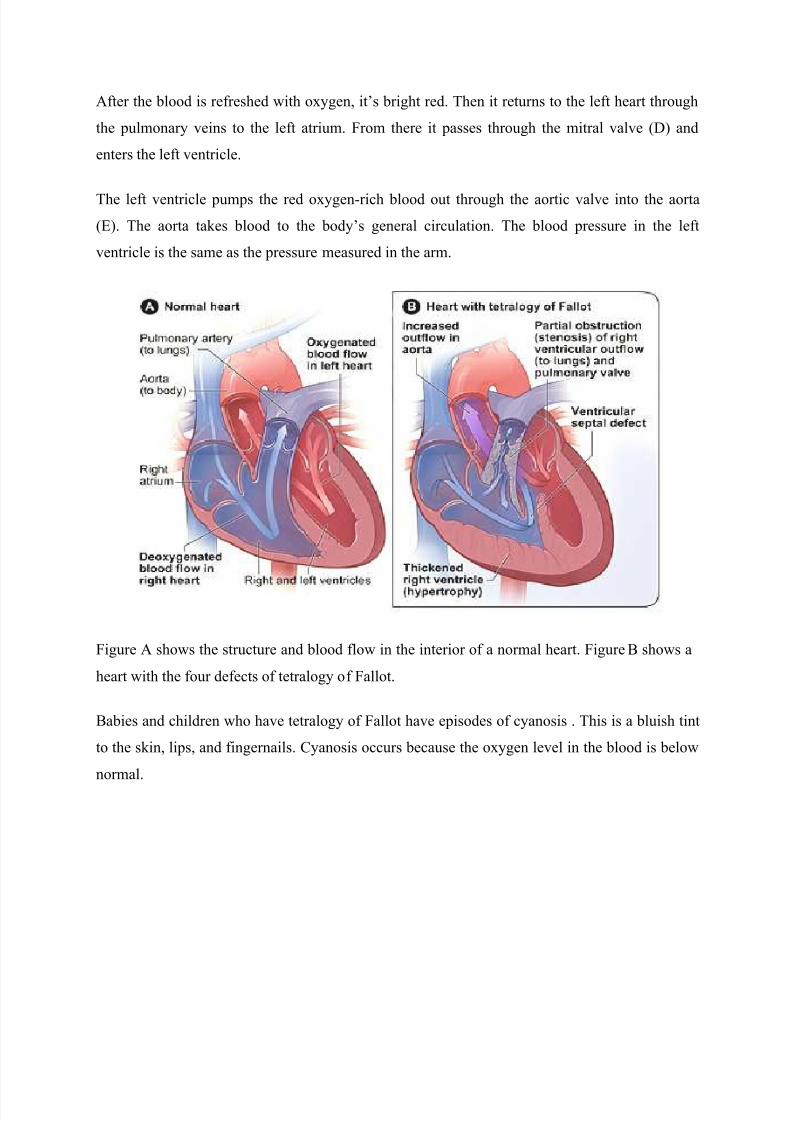
After the blood is refreshed with oxygen, it¶s bright red. Then it returns to the left heart through
the pulmonary veins to the left atrium. From there it passes through the mitral valve (D) and
enters the left ventricle.
The left ventricle pumps the red oxygen-rich blood out through the aortic valve into the aorta
(E). The aorta takes blood to the body¶s general circulation. The blood pressure in the left
ventricle is the same as the pressure measured in the arm.
Figure A shows the structure and blood flow in the interior of a normal heart. Figure B shows a
heart with the four defects of tetralogy of Fallot.
B abies and children who have tetralogy of Fallot have episodes of cyanosis . This is a bluish tint
to the skin, lips, and fingernails. C yanosis occurs because the oxygen level in the blood is below
normal.
8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 5/8
Diagnostic P rocedures:
Echocardiography
Echocardiography (echo) is a painless test that uses sound waves to create a moving picture of the heart. During the test, the sound waves (called ultrasound) bounce off the structures of the
heart. A computer converts the sound waves into pictures on a screen.
Echo allows the doctor to clearly see any problem with the way the heart is formed or the way
it's working.
Echo is an important test for diagnosing tetralogy of Fallot because it shows the four heart
defects and how the heart is responding to them. This test helps the cardiologist decide when torepair these defects and what type of surgery is needed.
EKG (Electrocardiogram)
An EKG is a simple, painless test that records the heart¶s electrical activity. The test shows how
fast the heart is beating and its rhythm (steady or irregular). It also records the strength and
timing of electrical signals as they pass through each part of the heart.
An EKG also can help the doctor determine whether the right ventricle is enlarged (ventricular
hypertrophy).
C hest X Ray
A chest x ray is a painless test that creates pictures of the structures in the chest, such as the heart
and lungs. This test can show whether the heart is enlarged or whether the lungs have extra blood
flow or extra fluid, a sign of heart failure.
P ulse Ox imetry
For this test, a small sensor is attached to a finger or toe (like an adhesive bandage). The sensor
gives an estimate of how much oxygen is in the blood.
C ardiac C atheterization
During cardiac catheterization a thin, flexible tube called a catheter is put into a vein in the arm,groin (upper thigh), or neck and threaded to the heart.
S pecial dye is injected through the catheter into a blood vessel or a chamber of the heart. The dye
allows the doctor to see the flow of blood through the heart and blood vessels on an x-ray image.

8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 6/8
The doctor also can use cardiac catheterization to measure the pressure and oxygen level inside
the heart chambers and blood vessels. This can help the doctor determine whether blood is
mixing between the two sides of the heart.
T reatment:
M edical:
y
administer oxygen(through face mask)
y
administer morphine sulfate(gen.beta bloacker), may be given orally to aid pulmonary
artery dilatation.
Morphine Sulfate (duramorph, astromorph, MS Contin)
D rug of choice for narcotic analgesia because of its reliable and predictable effects, safetyprofile, and easy of reversibility with naloxone
A dministered IV, may be dosed in number of ways and commonly titrated until desired effectobtained.
Metoprolol and Propranolol
Classification: Beta-Blockers
Used to treat tremors, angina, HPN, heart rhythm disorders, and other heart or circulatory conditions. It
also used to treat or prevent heart attack, and reduce the severity of migraine and headaches.
Phenylephrine
Classification- D econgestant
Brand names: A h-Chew D , Lusonal, Nasop, Neo-Syneprine
It works by constricting (shrinking ) blood vessels.
Constriction of blood vessels in the sinuse, nose, and chest allows drainage of these areas, which
decreass congestion. Constriction of blood vessels also affects blood pressure
S urgical:
y
B lalock- T aussig O peration
-T his is a palliative surgical repair. The physician will create a shunt between the
aorta and pulmonary artery.
-T emporary or P alliati v e S urgery
It was common in the past to do temporary surgery during infancy in babies who had tetralogy of
Fallot. This surgery improved blood flow to the lungs. A complete repair of the four defects was
done later in childhood.

8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 7/8
N ow, most babies who have tetralogy of Fallot have their defects fully repaired in infancy.
However, some babies are too weak or too small to have the full repair. They must have
temporary surgery first. This surgery improves oxygen levels in the blood. It also gives the baby
time to grow and get strong enough for the full repair.
In the temporary surgery, the surgeon places a tube called a shunt between a large artery
branching off the aorta and the pulmonary artery. One end of the shunt is sewn to the artery
branching off the aorta. The other end is sewn to the pulmonary artery.
The shunt creates an additional pathway for blood to travel to the lungs to get oxygen. The shunt
is removed when the baby's heart defects are fixed during the full repair.
y
C omplete Intracardiac Repair
S urgery to repair tetralogy of Fallot is done to improve blood flow to the lungs and to make sure
that oxygen-rich and oxygen-poor blood flows to the right places. The surgeon will:
y
W iden the narrowed pulmonary blood vessels. The pulmonary valve is widened or
replaced, and the passage from the right ventricle to the pulmonary artery is enlarged.
These procedures improve blood flow to the lungs. This allows the blood to get enough
oxygen to meet the body's needs.y
C lose the ventricular septal defect (V S D). A patch is used to cover the hole in the septum.
This patch stops oxygen-rich and oxygen-poor blood from mixing between the ventricles.
Fixing these two defects resolves problems caused by the other two defects. W hen the right
ventricle no longer has to work so hard to pump blood to the lungs, it will return to a normal
thickness. Fixing the V S D means that only oxygen-rich blood will flow out of the left ventricle
into the aorta.
The incision (cut) that the surgeon makes to reach the heart usually heals in about 6 weeks. The
surgeon or a hospital staff member will explain when it's okay to give your baby a bath, pick him
or her up under the arms, and take your baby for his or her regular shots (immunizations).
C omplications:
1.
C ongestive heart failure- may occur in newborn but is uncommon beyond infancy.
2.
C erebral vascular accident (due to thrombosis or severe hypoxia)

8/7/2019 Tetralogy of Fallot finale
http://slidepdf.com/reader/full/tetralogy-of-fallot-finale 8/8
P re v ention:
There is no known prevention for tetralogy of Fallot.
P re v alence Rate:
Tetralogy of Fallot is a rare, complex heart defect that occurs in about 5 out of every 10,000
babies. It affects boys and girls equally.
P rognosis:
S tudies of immediate and long-term follow-up in tetralogy of Fallot reveal excellent outcomes.
P atients born 30 years ago with tetralogy of Fallot have an 85% long-term rate of survival, and in
the absence of serious residue are able to lead normal lives as evidenced by the ability to carry
successful pregnancies for example [35-40]. C hronic issues that face the current population of
adults subsequent to their surgical repair include the hemodynamic manifestations of chronic
pulmonary regurgitation, recurrent or residual pulmonary stenosis, and ventricular arrhythmias.
The prognosis of patients born in the current era is expected to be substantially improved due to
advances in surgical and medical management that have occurred over the past couple of
decades. As for all patients with congenitally malformed hearts, the management of the patientwith Tetralogy of Fallot does not end at the time of complete repair. Follow-up by cardiologists
trained in congenital cardiac disease will remain a lifelong experience.