Embed Size (px)
Citation preview

The additional value of gait analysis in the identification of specific physical therapy treatment goals for ambulant
children with spastic Cerebral Palsy
Inge Franki
Jos De Cat
Chris Van den Broeck
Guy Molenaers
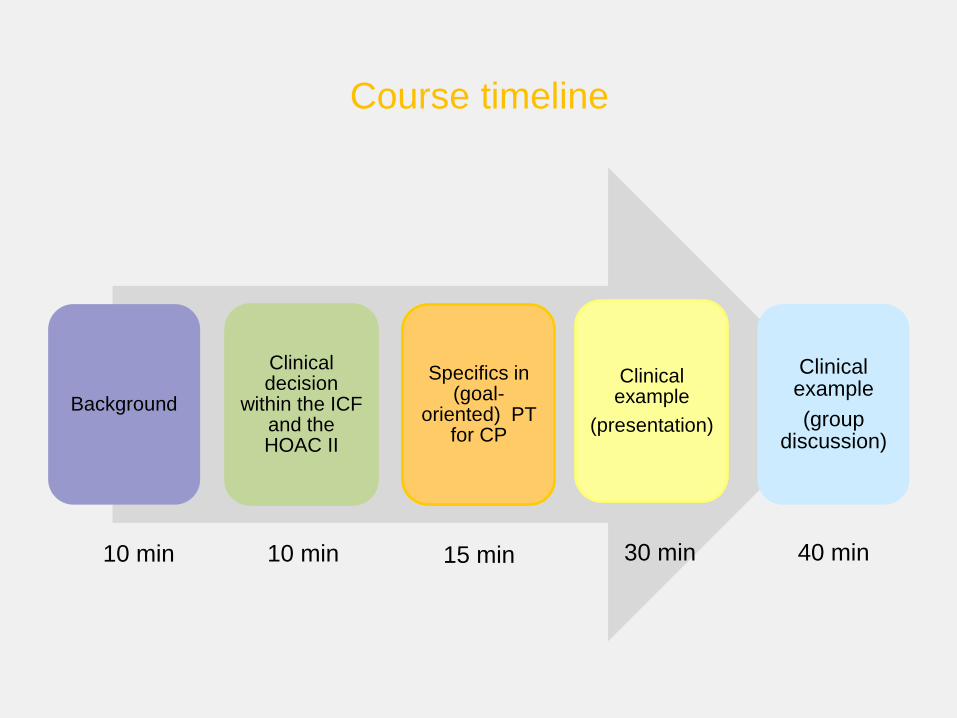
Course timeline
Background
Clinical decision
within the ICF and the HOAC II
Specifics in (goal-
oriented) PT for CP
Clinical example
(presentation)
Clinical example
(group discussion)
10 min 10 min 15 min 30 min 40 min
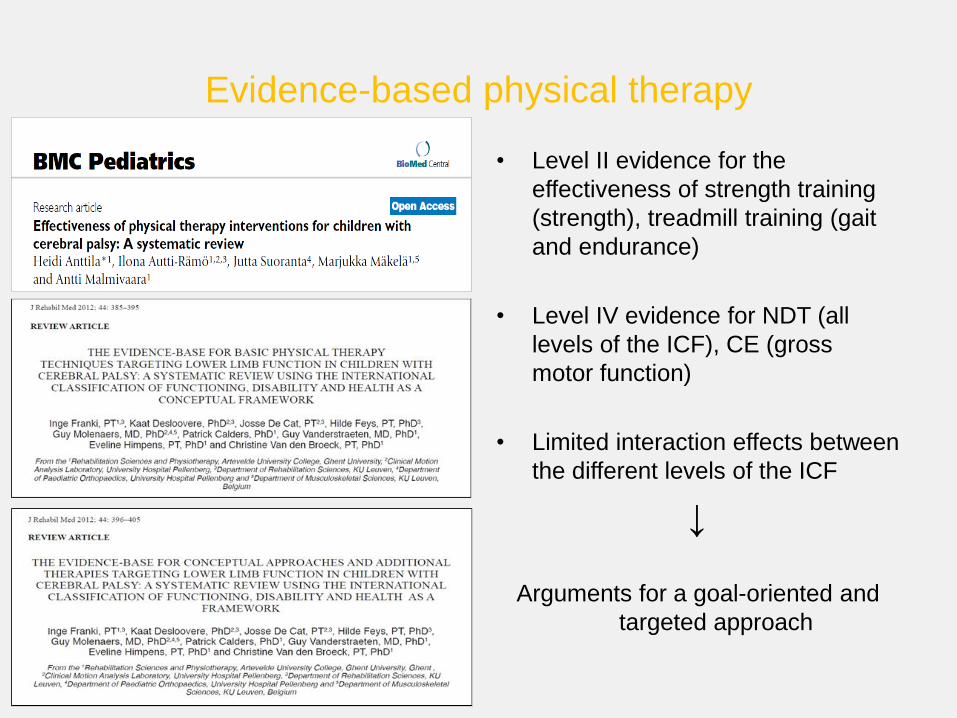
Evidence-based physical therapy
• Level II evidence for the
effectiveness of strength training
(strength), treadmill training (gait
and endurance)
• Level IV evidence for NDT (all
levels of the ICF), CE (gross
motor function)
• Limited interaction effects between
the different levels of the ICF
↓
Arguments for a goal-oriented and
targeted approach
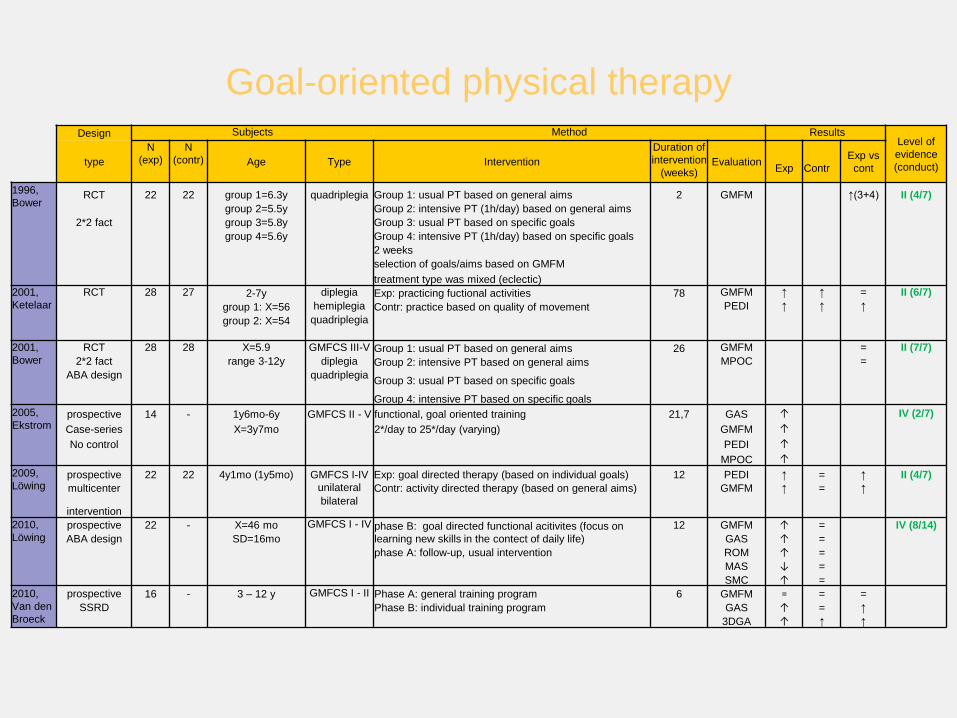
Goal-oriented physical therapy Design Subjects Method Results
Level of
evidence
(conduct)
type
N
(exp)
N
(contr) Age Type Intervention
Duration of
intervention
(weeks) Evaluation
Exp
Contr
Exp vs
cont
1996,
Bower
RCT 22 22 group 1=6.3y quadriplegia Group 1: usual PT based on general aims 2 GMFM ↑(3+4) II (4/7)
group 2=5.5y Group 2: intensive PT (1h/day) based on general aims
2*2 fact group 3=5.8y Group 3: usual PT based on specific goals
group 4=5.6y Group 4: intensive PT (1h/day) based on specific goals
2 weeks
selection of goals/aims based on GMFM
treatment type was mixed (eclectic)
2001,
Ketelaar
RCT 28 27 2-7y diplegia Exp: practicing fuctional activities 78 GMFM ↑ ↑ = II (6/7)
group 1: X=56 hemiplegia Contr: practice based on quality of movement PEDI ↑ ↑ ↑
group 2: X=54 quadriplegia
2001,
Bower
RCT 28 28 X=5.9 GMFCS III-V Group 1: usual PT based on general aims 26 GMFM = II (7/7)
2*2 fact range 3-12y diplegia Group 2: intensive PT based on general aims MPOC =
ABA design quadriplegia Group 3: usual PT based on specific goals
Group 4: intensive PT based on specific goals
2005,
Ekstrom prospective 14 - 1y6mo-6y GMFCS II - V functional, goal oriented training 21,7 GAS ↑ IV (2/7)
Case-series X=3y7mo 2*/day to 25*/day (varying) GMFM ↑
No control PEDI ↑
MPOC ↑
2009,
Löwing
prospective 22 22 4y1mo (1y5mo) GMFCS I-IV Exp: goal directed therapy (based on individual goals) 12 PEDI ↑ = ↑ II (4/7)
multicenter unilateral Contr: activity directed therapy (based on general aims) GMFM ↑ = ↑
intervention bilateral
2010,
Löwing prospective 22 - X=46 mo GMFCS I - IV phase B: goal directed functional acitivites (focus on
learning new skills in the contect of daily life)
12 GMFM ↑ = IV (8/14)
ABA design SD=16mo GAS ↑ =
phase A: follow-up, usual intervention ROM ↑ =
MAS ↓ =
SMC ↑ =
2010,
Van den
Broeck
prospective 16 - 3 – 12 y GMFCS I - II Phase A: general training program 6 GMFM = = =
SSRD Phase B: individual training program GAS ↑ = ↑
3DGA ↑ ↑ ↑
Advantages of a goal-oriented approach
• More specific: focus on main problems – one cannot work on all
problems at the same time
• Faces heterogeneous clinical problems
• Availability of many different physical therapy techniques
- promotes choosing specific techniques accordingly
Problems and difficulties
• Many different applications and definitions for treatment goals
• Lack of a clear structure to define individual goals
↓
Which way to choose?
Back to basics!
• International Classification of Functioning, Disability and Health
• Hypothesis-Oriented Algorithm for Clinicians II (HOAC II)
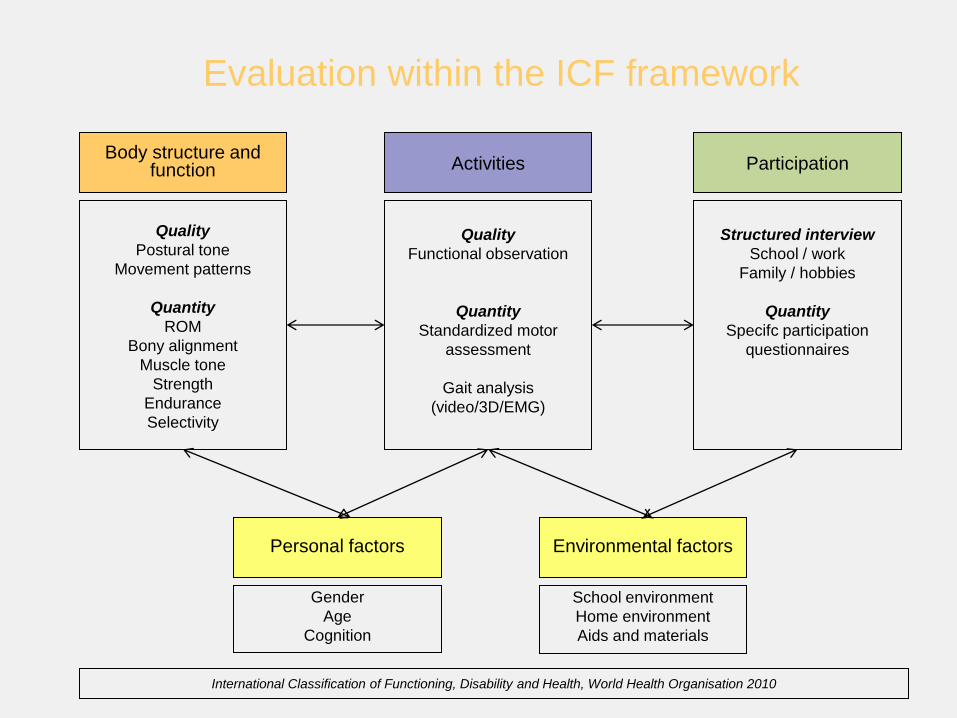
Quality
Postural tone
Movement patterns
Quantity
ROM
Bony alignment
Muscle tone
Strength
Endurance
Selectivity
Quality
Functional observation
Quantity
Standardized motor
assessment
Gait analysis
(video/3D/EMG)
Structured interview
School / work
Family / hobbies
Quantity
Specifc participation
questionnaires
Evaluation within the ICF framework
Body structure and function Activities Participation
International Classification of Functioning, Disability and Health, World Health Organisation 2010
Personal factors Environmental factors
Gender
Age
Cognition
School environment
Home environment
Aids and materials
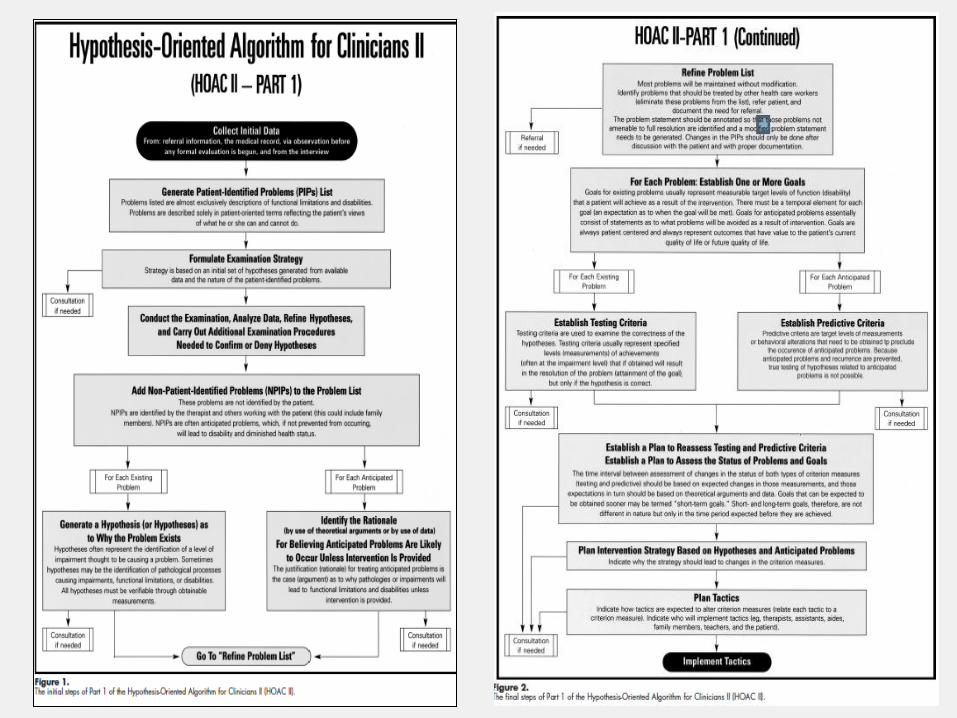
HOAC –II
• Specifically developped for clinicians
• Algorithm defining a clinical reasoning process starting from initial referral,
planning examination strategy to implementing tactics
• Hypothesis-oriented
• Very long, complicated
The Hypothesis-Oriented Algorithm for Clinicians II (HOAC II): A guide for patient management. Rothstein et al. 2003
Strengths and limitations
HOAC
• Structure for clinical reasoning
• Strategy-oriented
• No structure for assessment
• Complex
• Hypothesis oriented – risk of
bias/errors
ICF
• No direct structure for clinical
reasoning
• Good structure for assessment
• Not directly strategy-oriented
• Simple
• Straight-forward

Background Clinical decision
within the ICF and the HOAC II
Specifics in (goal-
oriented) PT for CP
Clinical example
(presentation)
Clinical example
(group discussion)

3DGA Clinical
examination
GMFM
(66 or 88)
Problems
ROM
Strength
Spasticity
Selectivity
Problems
Time-and
distance
parameters
Kinematics
Kinetics
EMG
Problems
Lying
Rolling
Sitting
Crawling
Kneeling
Standing
Walking
Running
Jumping
CAPE
Problems
Home
School
Environment
Body function
and structure Activities Participation
Non-patient identified problems Patient identified problems
Personal and
environmental
factors
Background
information and
parent/child
assessment
Positive and
negative factors
Personal
Environment
Refined
problem list to
main
problems
One or more
goals per
problem
Generate a hypothesis as to why the problem exists Identify the rationale
Definition of main problem(s)
Underlying, common factor(s) that can explain the problems at all levels of the
ICF, explain the globality of the child , the causes of the child’s difficulties.
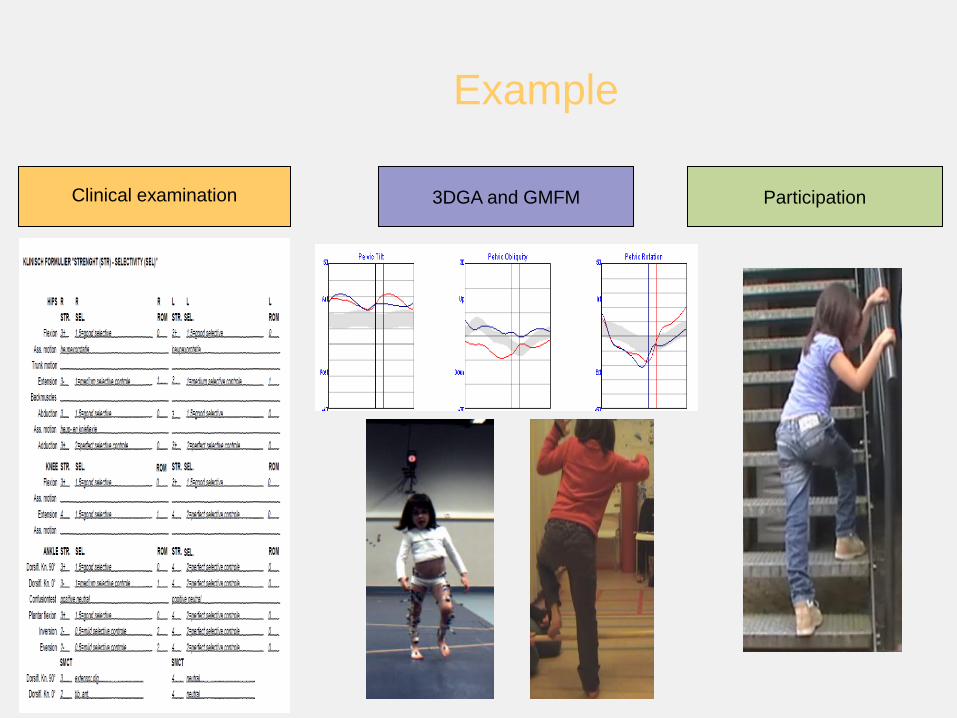
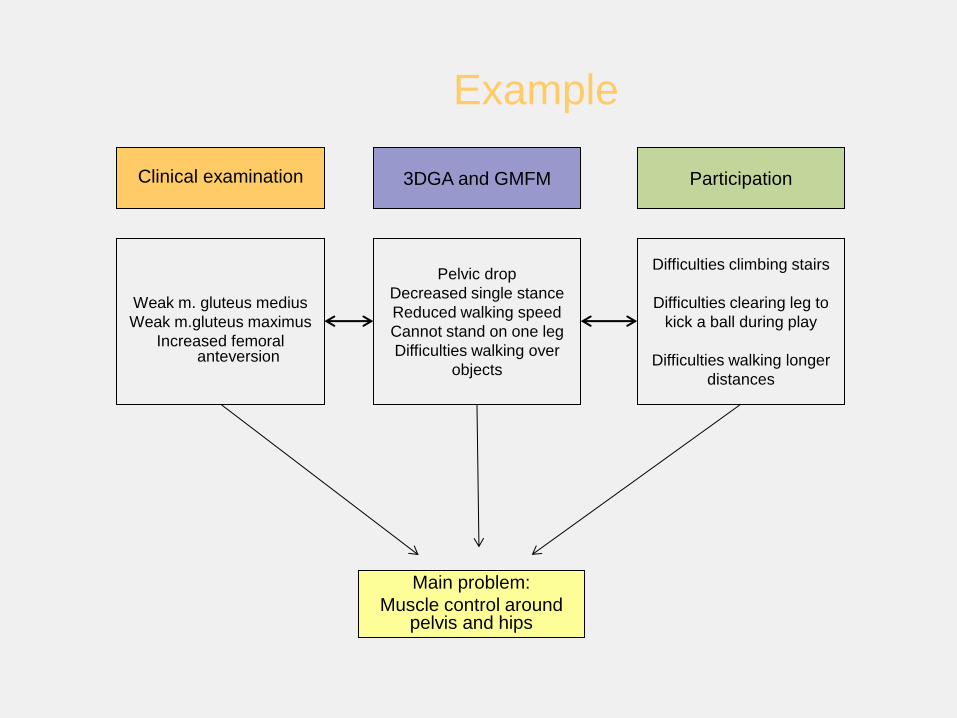
Example
Clinical examination 3DGA and GMFM Participation
Example
Weak m. gluteus medius
Weak m.gluteus maximus
Increased femoral anteversion
Pelvic drop
Decreased single stance
Reduced walking speed
Cannot stand on one leg
Difficulties walking over
objects
Difficulties climbing stairs
Difficulties clearing leg to
kick a ball during play
Difficulties walking longer
distances
Clinical examination 3DGA and GMFM Participation
Main problem:
Muscle control around pelvis and hips
Clinical examination 3DGA and GMFM Participation
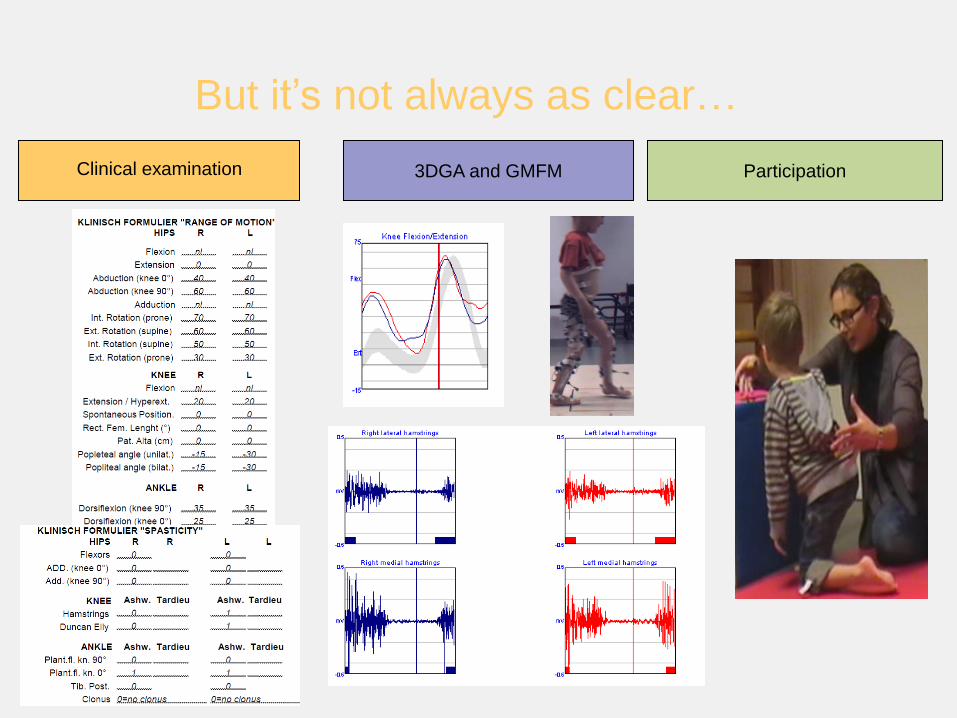
But it’s not always as clear…
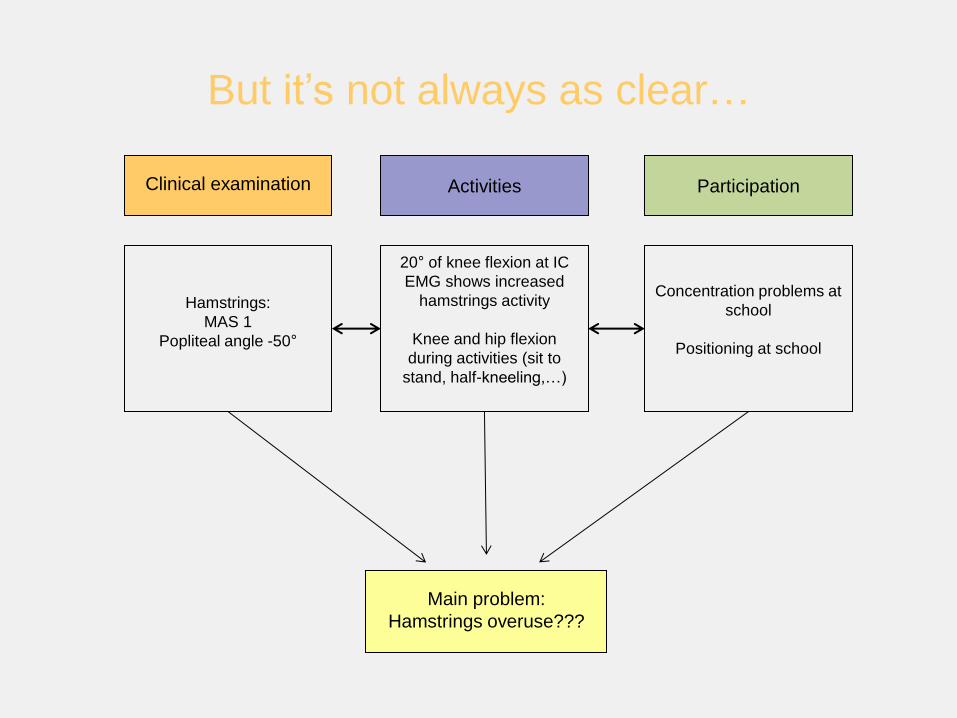
But it’s not always as clear…
Hamstrings:
MAS 1
Popliteal angle -50°
20° of knee flexion at IC
EMG shows increased
hamstrings activity
Knee and hip flexion
during activities (sit to
stand, half-kneeling,…)
Concentration problems at
school
Positioning at school
Clinical examination Activities Participation
Main problem:
Hamstrings overuse???
Background
Clinical decision within the
ICF and the HOAC II
Specifics in (goal-oriented) PT for
CP
Clinical example
(presentation)
Clinical example
(group discussion)
Training principles
1. Knowledge of typical walking
2. Use of basic training principles
(load, repetition, frequency)
Typical walking and goal setting
• Stability in stance
• Sufficient foot clearance during
swing
• Appropriate swing phase pre-
positioning of the foot
• Adequate step length
• Energy conservation
• Specific muscle training (open/closed
loop, concentric, eccentric or isometric)
• Train muscles in specific ‘range of
motion’
• Train muscle at specific contraction
velocity
• Train for specific combination of muscle
activity (coordination)
The identification and treatment of gait problems in Cerebral
Palsy. J Gage, Mac Keith Press, London 2009

Problems in therapeutic planning
• Results of clinical exam (static)
• Dynamic ‘range of motion’ in gait
• Stability
• Underlying weakness (kinetic data)
• Primary and secondary motor patterns
• Gait velocity – control of velocity
• Fixed and dynamic problems
Individual ‘goal setting’ for physiotherapy

Steps to take
Body structure and function Activities Participation
Positioning
Stretching
Orthosis
Analytical muscle work
Strengthening specific
muscle groups
Functional, active gait
training
Integration into
function
Transfer into activities
of daily life
Automatisation

Background
Clinical decision within the
ICF and the HOAC II
Specifics in (goal-
oriented) PT for CP
Clinical example
(presentation)
Clinical example
(group discussion)

Conclusion
• Using gait analysis information can be very useful in the definition of specific
goals in ambulant children with CP
• It is necessary to understand the principles of muscle work during gait in
order to work specifically and targeted
• Effects of individually-defined therapy programs should be evaluted on long
term






























