Embed Size (px)
Citation preview

The ‘Alberta Paradox’: The Regulation of The ‘Alberta Paradox’: The Regulation of Private Health Insurance in Comparative Private Health Insurance in Comparative Cross-Provincial PerspectiveCross-Provincial Perspective
Gerard W. BoychukGerard W. BoychukDepartment of Political ScienceDepartment of Political ScienceUniversity of WaterlooUniversity of Waterloo
Presented to the Institute for Advanced Policy Research, Presented to the Institute for Advanced Policy Research, University of CalgaryUniversity of CalgarySeptember 20September 20thth, 2006, 2006
The Paradox...The Paradox...
““Alberta is the testing ground of health care commercialization – Alberta is the testing ground of health care commercialization – and nose-thumbing at the and nose-thumbing at the Canada Health ActCanada Health Act – and its role as a – and its role as a national “Trojan Horse” in pushing privatization has yielded national “Trojan Horse” in pushing privatization has yielded impressive results elsewhere in the country...”impressive results elsewhere in the country...”
CUPECUPEInnovation Innovation
ExposedExposed, Oct.2004 , Oct.2004 "Alberta, of all the provinces in Canada, is the most hostile "Alberta, of all the provinces in Canada, is the most hostile
towards private clinics. We couldn't function in Alberta." towards private clinics. We couldn't function in Alberta." Dr. Brian DayDr. Brian Day
President Elect – CMAPresident Elect – CMAFounder, Cambie Founder, Cambie
Surgical ServicesSurgical Services Edmonton Edmonton Journal, Journal, 18 Sept.200518 Sept.2005
The Paradox...The Paradox...
political leadership in Alberta firmly committed political leadership in Alberta firmly committed to increasing private funding in health servicesto increasing private funding in health services
Alberta regulation of private funding/financing Alberta regulation of private funding/financing options is relatively stringentoptions is relatively stringent– more stringent that in several other Canadian more stringent that in several other Canadian
provincesprovinces– more stringent than required by more stringent than required by CHACHA
Why?Why?

The Answer...The Answer... relatively sophisticated political calculation based on a relatively sophisticated political calculation based on a
number of factors...number of factors...– electoral benefits are unclearelectoral benefits are unclear
public opinion in Alberta no more (and likely less) supportive than public opinion in Alberta no more (and likely less) supportive than public opinion in other provincespublic opinion in other provinces
– Alberta government has contributed to an emphasis federal-Alberta government has contributed to an emphasis federal-provincial aspects of reformprovincial aspects of reform
has undermined construction of a public consensus around reformshas undermined construction of a public consensus around reforms
– health care funding not as pressing a political problem as health care funding not as pressing a political problem as often made outoften made out
strong fiscal capacity make acceptance of the status quo a more strong fiscal capacity make acceptance of the status quo a more politically palatable optionpolitically palatable option
– Alberta government views health care reform as key Alberta government views health care reform as key ideological battlegroundideological battleground
reticent to experiment if success is not guaranteedreticent to experiment if success is not guaranteed
Stringency of Regulation (Private Stringency of Regulation (Private Provision/Funding/Insurance) in Alberta Provision/Funding/Insurance) in Alberta -- vis-a-vis -- vis-a-vis Canada Health ActCanada Health Act (CHA) (CHA) CHACHA
– universal availability of public health insurance (on uniform universal availability of public health insurance (on uniform terms and conditions) for all medically necessary hospital terms and conditions) for all medically necessary hospital and physician servicesand physician services
without financial barriers to accesswithout financial barriers to access– extra-billing on insured servicesextra-billing on insured services– user/facility fees on insured services (defined – Marleau, 1995)user/facility fees on insured services (defined – Marleau, 1995)
penaltiespenalties– non-discretionary penalties for extra-billing/user feesnon-discretionary penalties for extra-billing/user fees– discretionary penalties for other violations of five principlesdiscretionary penalties for other violations of five principles
– non-requirementsnon-requirements no legal probitions on private provision of servicesno legal probitions on private provision of services no legal prohibitions on private insuranceno legal prohibitions on private insurance no reference to the status of physicians – only the status of services no reference to the status of physicians – only the status of services
(insured vs. non-insured)(insured vs. non-insured)
Stringency of Regulation (Private Stringency of Regulation (Private Provision/Funding/Insurance) in Alberta Provision/Funding/Insurance) in Alberta -- vis-a-vis -- vis-a-vis Canada Health ActCanada Health Act (CHA) (CHA) limits on private income by opted-in physicianslimits on private income by opted-in physicians
prohibits opted-in physicians from billing individual patients at rates above prohibits opted-in physicians from billing individual patients at rates above those payable by the public insurance programthose payable by the public insurance program
limits on public income by non-participating physicianslimits on public income by non-participating physicians expressly prohibits reimbursement of residents who have paid fees for expressly prohibits reimbursement of residents who have paid fees for
services provided by a non-participating physician services provided by a non-participating physician
prohibitions on the private provision of servicesprohibitions on the private provision of services– prohibits private facilities providing emergency care requiring medically-prohibits private facilities providing emergency care requiring medically-
supervised stays of more than twelve hourssupervised stays of more than twelve hours– prohibits physicians from performing ‘major’ surgical services except in a public prohibits physicians from performing ‘major’ surgical services except in a public
hospitalhospital CHA only requires that facility fees be covered by public plan if physician CHA only requires that facility fees be covered by public plan if physician
fee is covered by public planfee is covered by public plan
bans third party insurance for services that are otherwise bans third party insurance for services that are otherwise publicly-fundedpublicly-funded
Alberta in Cross-Provincial Alberta in Cross-Provincial Comparative PerspectiveComparative Perspective
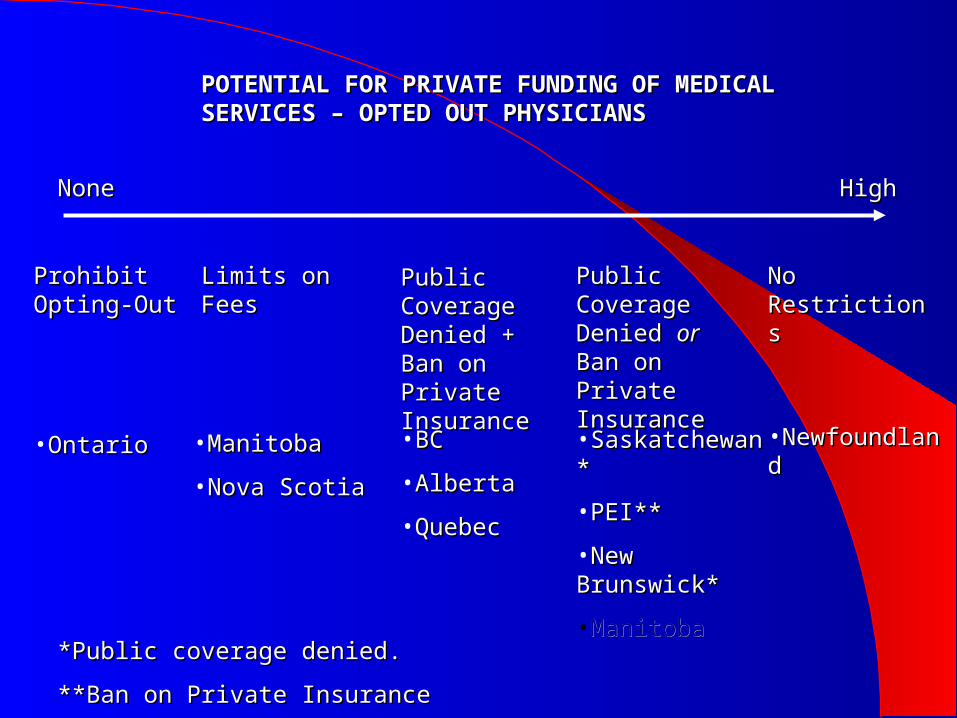
POTENTIAL FOR PRIVATE FUNDING OF MEDICAL POTENTIAL FOR PRIVATE FUNDING OF MEDICAL SERVICES – OPTED OUT PHYSICIANSSERVICES – OPTED OUT PHYSICIANS
NoneNone HighHigh
Prohibit Prohibit Opting-OutOpting-Out
Limits on FeesLimits on Fees Public Public Coverage Coverage Denied + Ban Denied + Ban on Private on Private InsuranceInsurance
Public Public Coverage Coverage Denied Denied oror Ban Ban on Private on Private InsuranceInsurance
No RestrictionsNo Restrictions
•OntarioOntario •ManitobaManitoba
•Nova ScotiaNova Scotia
•BCBC
•AlbertaAlberta
•QuebecQuebec
•Saskatchewan*Saskatchewan*
•PEI**PEI**
•New Brunswick*New Brunswick*
•ManitobaManitoba
•Newfoundland Newfoundland
*Public coverage denied.*Public coverage denied.
**Ban on Private Insurance**Ban on Private Insurance

POTENTIAL FOR PRIVATE FUNDING OF MEDICAL POTENTIAL FOR PRIVATE FUNDING OF MEDICAL SERVICES – OPTED-IN PHYSICIANSSERVICES – OPTED-IN PHYSICIANS
NoneNone HighHigh
Prohibit Direct Prohibit Direct Patient BillingPatient Billing
Ban Extra-Ban Extra-BillingBilling
Ban on Private Ban on Private InsuranceInsurance
Public Public Coverage Coverage DeniedDenied
No Restrictions No Restrictions (except no (except no direct billing of direct billing of public plan) public plan)
•SaskatchewanSaskatchewan
•ManitobaManitoba
•OntarioOntario
•QuebecQuebec
•Nova ScotiaNova Scotia
•NewfoundlandNewfoundland
•BCBC
•AlbertaAlberta
•SaskatchewanSaskatchewan
•ManitobaManitoba
•OntarioOntario
•QuebecQuebec
•Nova ScotiaNova Scotia
•NewfoundlandNewfoundland
•PEIPEI
•BCBC
•AlbertaAlberta
•ManitobaManitoba
•OntarioOntario
•QuebecQuebec
•New BrunswickNew Brunswick
•All other All other provincesprovinces
•Allowed by Allowed by CHA ?CHA ?

Alberta in Cross-Provincial Alberta in Cross-Provincial Comparative PerspectiveComparative Perspective maximum allowance for private funding (using maximum allowance for private funding (using
currently existing provincial practices)currently existing provincial practices)– non-participating phyisiciansnon-participating phyisicians
billing rates unrestrictedbilling rates unrestricted patient reimbursed (up to public rate schedule)patient reimbursed (up to public rate schedule) private insurance coverageprivate insurance coverage
– participating physiciansparticipating physicians direct patient billing at unrestricted ratesdirect patient billing at unrestricted rates private insurance coverageprivate insurance coverage no patient reimbursementno patient reimbursement

Alberta in Comparative PerspectiveAlberta in Comparative Perspective
the Australian model (e.g. Emery)the Australian model (e.g. Emery)– public subsidization of private insurance premiumspublic subsidization of private insurance premiums
waive public premiums for individuals who purchase private waive public premiums for individuals who purchase private insuranceinsurance
– coverage of physicians fee (non-participating, participating?) coverage of physicians fee (non-participating, participating?) outside of the plan (up to fixed %)outside of the plan (up to fixed %)
– facility fees in public facilities (up to fixed %) for ‘private’ facility fees in public facilities (up to fixed %) for ‘private’ patientspatients
allowable for services provided to private patients (corrollary of allowable for services provided to private patients (corrollary of Marleau stipulation)Marleau stipulation)
– non-participating physiciansnon-participating physicians• issue is granting hospital privileges to non-participating physiciansissue is granting hospital privileges to non-participating physicians
– participating physicians participating physicians • if physician fee is not publicly reimbursed (e.g. New Brunswick)if physician fee is not publicly reimbursed (e.g. New Brunswick)• if patient is publicly reimubursed for physician fee??if patient is publicly reimubursed for physician fee??

Alberta in Cross-Provincial Alberta in Cross-Provincial Comparative PerspectiveComparative Perspective maximum allowance for private funding (using maximum allowance for private funding (using
currently existing provincial practices)currently existing provincial practices)– non-participating phyisiciansnon-participating phyisicians
billing rates unrestrictedbilling rates unrestricted patient reimbursed (up to public rate schedule)patient reimbursed (up to public rate schedule) private insurance coverageprivate insurance coverage
– participating physiciansparticipating physicians direct patient billing at unrestricted ratesdirect patient billing at unrestricted rates private insurance coverageprivate insurance coverage no patient reimbursementno patient reimbursement

Alberta in Cross-Provincial Alberta in Cross-Provincial Comparative PerspectiveComparative Perspective maximum allowance for private funding (using maximum allowance for private funding (using
currently existing provincial practices)currently existing provincial practices)– non-participating phyisiciansnon-participating phyisicians
billing rates unrestrictedbilling rates unrestricted patient reimbursed (up to public rate schedule)patient reimbursed (up to public rate schedule) private insurance coverageprivate insurance coverage
– participating physiciansparticipating physicians direct patient billing at unrestricted ratesdirect patient billing at unrestricted rates private insurance coverageprivate insurance coverage patient reimbursed (up to public rate schedule)patient reimbursed (up to public rate schedule)
Alberta’s Proposed ReformsAlberta’s Proposed Reforms Mazankowski Report recommendations re: health care financingMazankowski Report recommendations re: health care financing
– ““Phyisicians should be able to work in public, private or not-for-proft systems Phyisicians should be able to work in public, private or not-for-proft systems and retain their privileges at public hospitals.” (51)and retain their privileges at public hospitals.” (51)
– private insuranceprivate insurance defined: “People would be able to choose to get both insured and non-insured health defined: “People would be able to choose to get both insured and non-insured health
service at a private facility. They could pay for these services directly or through some service at a private facility. They could pay for these services directly or through some form of private or supplementary insurance. The public system would continue to form of private or supplementary insurance. The public system would continue to provide the full range of insured health services.” (56)provide the full range of insured health services.” (56)
““...we do not recommend expanding private insurance for publicly funded services...” ...we do not recommend expanding private insurance for publicly funded services...” (56)(56)
““...this approach ...this approach would clearly contravenewould clearly contravene the Canada Health Act.” (56) the Canada Health Act.” (56)– MSA’sMSA’s
““...if people are are required to pay for some services once their medical savings ...if people are are required to pay for some services once their medical savings account is exhausted, this account is exhausted, this maymay contravene the Canada Health Act.” (58) contravene the Canada Health Act.” (58)
– variable premiumsvariable premiums variable based on income and health service usagevariable based on income and health service usage
– ““We believe our recommendations are consistent with the spirit and intent of the We believe our recommendations are consistent with the spirit and intent of the Canada Health Act.”Canada Health Act.”

Alberta’s Proposed ReformsAlberta’s Proposed Reforms
Health Policy FrameworkHealth Policy Framework, February 2006, February 2006– Directions 6-9 – relevant to issues of fundingDirections 6-9 – relevant to issues of funding
Direction 6: limiting publicly-funded health servicesDirection 6: limiting publicly-funded health services– excluding health services which are “discretionary, are not of excluding health services which are “discretionary, are not of
proven benefit, or are experimental in nature…”proven benefit, or are experimental in nature…”– and leaving those services to be financed either by patients and leaving those services to be financed either by patients
directly or through third-party insurancedirectly or through third-party insurance Direction 7: flexible funding optionsDirection 7: flexible funding options
– mentions co-payment, long-term care savings accounts, private mentions co-payment, long-term care savings accounts, private insuranceinsurance
• including non-emergency acute care (in addition to non-including non-emergency acute care (in addition to non-CHA services -- e.g prescription drugs, dental care)CHA services -- e.g prescription drugs, dental care)
• ““Alberta will closely examine...”Alberta will closely examine...”
Alberta’s Proposed ReformsAlberta’s Proposed Reforms
Health Policy FrameworkHealth Policy Framework, February 2006, February 2006– Directions 6-9 – relevant to issues of fundingDirections 6-9 – relevant to issues of funding
Direction 9: “paying for choice and access”Direction 9: “paying for choice and access”– shift away from requiring physicians who wish to bill privately to opt shift away from requiring physicians who wish to bill privately to opt
out for all servicesout for all services
• no violation of CHAno violation of CHA
• currently allowed in New Brunswick/PEIcurrently allowed in New Brunswick/PEI
– ““...allowing both public and private providers to offer enhanced services ...allowing both public and private providers to offer enhanced services and expedited acces to a limited range of ‘non-emergency’ services at and expedited acces to a limited range of ‘non-emergency’ services at an appropriate charge.”an appropriate charge.”
• CHA compliance – depends on implementationCHA compliance – depends on implementation
• phyisicians cannot bill public plan directly and bill patients an phyisicians cannot bill public plan directly and bill patients an additional chargeadditional charge
• facility fees cannot be charged if physician bills public plan facility fees cannot be charged if physician bills public plan directlydirectly
Alberta’s Proposed ReformsAlberta’s Proposed Reforms
Health Policy FrameworkHealth Policy Framework, February 2006, February 2006– Directions 6-9 – relevant to issues of fundingDirections 6-9 – relevant to issues of funding
Direction 6: limiting publicly-funded health servicesDirection 6: limiting publicly-funded health services– excluding health services which are “discretionary, are not of excluding health services which are “discretionary, are not of
proven benefit, or are experimental in nature…”proven benefit, or are experimental in nature…”– and leaving those services to be financed either by patients and leaving those services to be financed either by patients
directly or through third-party insurancedirectly or through third-party insurance Direction 7: flexible funding optionsDirection 7: flexible funding options
– mentions mentions co-paymentco-payment, long-term care savings accounts, private , long-term care savings accounts, private insuranceinsurance
• including including non-emergency acute carenon-emergency acute care (in addition to non- (in addition to non-CHA services -- e.g prescription drugs, dental care)CHA services -- e.g prescription drugs, dental care)
• ““Alberta will closely examine...”Alberta will closely examine...”
Alberta in Cross-Provincial Alberta in Cross-Provincial Comparative PerspectiveComparative PerspectiveMAIN POINTS...MAIN POINTS...
– there is a lot of room under the CHA to expand the there is a lot of room under the CHA to expand the potential for private funding and private insurance potential for private funding and private insurance of health servicesof health services
– enforcement of the CHA is a enforcement of the CHA is a politicalpolitical issue issue grey areas to be determined by federal interpretationgrey areas to be determined by federal interpretation
– enforcement more politically difficult where there are existing enforcement more politically difficult where there are existing provincial precedentsprovincial precedents
– enforcement more politically difficult in respect to existing enforcement more politically difficult in respect to existing practices than in respect to proposed reformspractices than in respect to proposed reforms
federal government retains right to amend the CHAfederal government retains right to amend the CHA

The Answer...The Answer... relatively sophisticated political calculation based on a relatively sophisticated political calculation based on a
number of factors...number of factors...– electoral benefits are unclearelectoral benefits are unclear
public opinion in Alberta no more (and likely less) supportive than public opinion in Alberta no more (and likely less) supportive than public opinion in other provincespublic opinion in other provinces
– Alberta government has contributed to an emphasis federal-Alberta government has contributed to an emphasis federal-provincial aspects of reformprovincial aspects of reform
has undermined construction of a public consensus around reformshas undermined construction of a public consensus around reforms
– health care funding not as pressing a political problem as health care funding not as pressing a political problem as often made outoften made out
strong fiscal capacity make acceptance of the status quo a more strong fiscal capacity make acceptance of the status quo a more politically palatable optionpolitically palatable option
– Alberta government views health care reform as key Alberta government views health care reform as key ideological battlegroundideological battleground
reticent to experiment if success is not guaranteedreticent to experiment if success is not guaranteed

Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial PerspectiveAlberta public opinion not more favourable Alberta public opinion not more favourable
to private funding/private insurance than to private funding/private insurance than other provinces (and probably less so)other provinces (and probably less so)
Compas, Pollara, Ipsos-Reid, EnvironicsCompas, Pollara, Ipsos-Reid, Environics
Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial Perspectivesupport for private payment for quicker support for private payment for quicker
service/service enhancementsservice/service enhancementssupport for private insurancesupport for private insurancesupport for different scenariossupport for different scenarios

Environics, National Issues Survey, June 2004.
0%
10%
20%
30%
40%
50%
60%
70%
Pe
rce
nt
(%)
BC Alberta SK MB Ontario Quebec Atlantic CDA
SUPPORT FOR 'RIGHT TO BUY PRIVATE CARE,' 2004

Pollara, Health Care in Canada Survey, 2005.
0%
10%
20%
30%
40%
50%
60%
Pe
rce
nt
(%)
BC/Terri Alberta MB/SK Ontario Quebec Atlantic CDA
SUPPORT FOR 'PAYING FOR QUICKER ACCESS' 2005

Pollara, Health Care in Canada Survey, 2005.
0%
10%
20%
30%
40%
50%
60%
Pe
rce
nt
(%)
BC/Terri Alberta MB/SK Ontario Quebec Atlantic CDA
INDIVIDUAL WILLINGNESS TO 'PAY FOR QUICKER ACCESS' 2005

0%
10%
20%
30%
40%
50%
60%
70%
Pe
rce
nt
Re
sp
on
din
g 'Y
es
' (%
)
BC/Terri Alberta MB/SK Ontario Quebec Atlantic CDA
SUPPORT FOR PAYING FOR SERVICE ENHANCEMENTS, 2005
Pollara, Health Care in Canada Survey, 2005.

Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial Perspectivesupport for private payment for quicker support for private payment for quicker
service/service enhancementsservice/service enhancementssupport for private insurancesupport for private insurancesupport for different scenariossupport for different scenarios
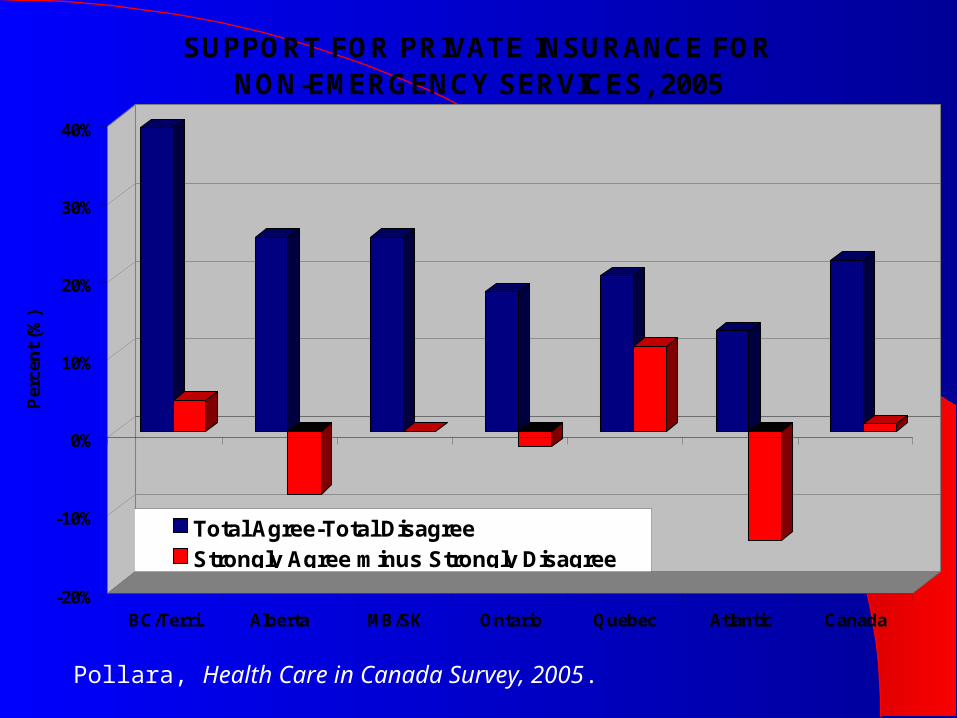
Pollara, Health Care in Canada Survey, 2005.
-20%
-10%
0%
10%
20%
30%
40%
Per
cen
t (%
)
BC/Terri. Alberta MB/SK Ontario Quebec Atlantic Canada
SUPPORT FOR PRIVATE INSURANCE FOR NON-EMERGENCY SERVICES, 2005
Total Agree-Total DisagreeStrongly Agree minus Strongly Disagree

Ipsos-Reid, CFNU, January 2006.
0
5
10
15
20
25
30
35
Per
cen
t (%
)
BC/Terri. Alberta MB/SK Ontario Quebec Atlantic Canada
PATIENT ALLOWED TO PAY/INSURE, 2005(When Timely Access Not Provided in Public System)
Disagree-AgreeDisagree Strongly-Agree Strongly
-10%
-5%
0%
5%
10%
15%
20%
25%
30%
35%
Per
cen
t (%
)
BC/Terri. Alberta MB/SK Ontario Quebec Atlantic Canada
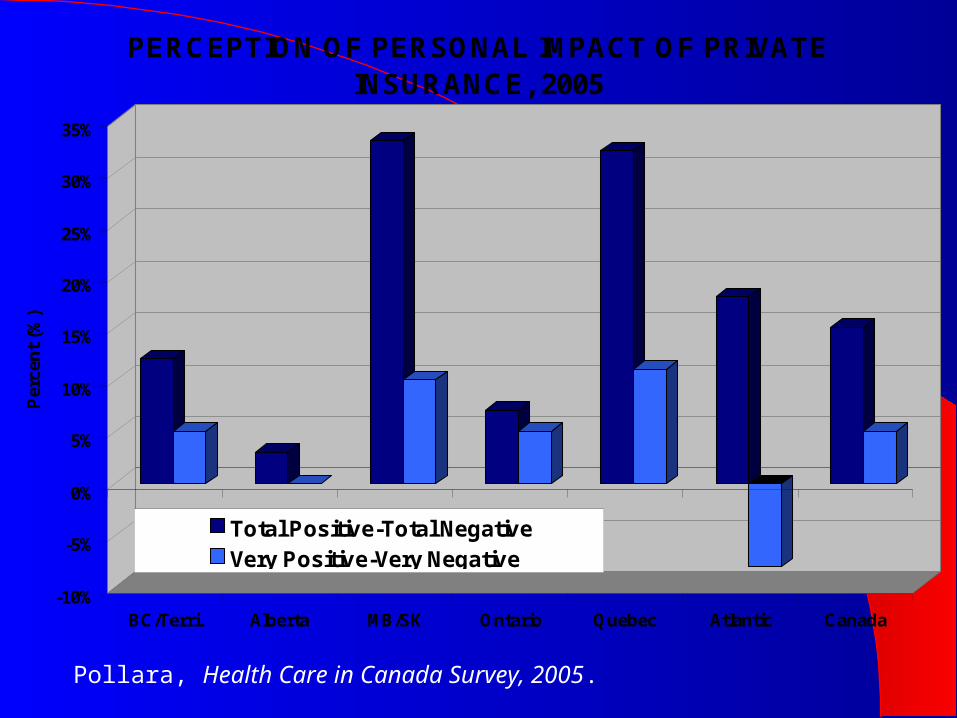
PERCEPTION OF PERSONAL IMPACT OF PRIVATE INSURANCE, 2005
Total Positive-Total NegativeVery Positive-Very Negative
Pollara, Health Care in Canada Survey, 2005.

Ipsos-Reid, CFNU, January 2006.
-20
-10
0
10
20
30
40
50
Per
cen
t (%
)
BC/Terri. Alberta MB/SK Ontario Quebec Atlantic Canada
IMPACT OF 'GREATER PRIVATE INVOLVEMENT', 2006 Would Improve Quality of Health Care Services
Net Improve Net Definitely Improve

Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial Perspectivesupport for private payment for quicker support for private payment for quicker
service/service enhancementsservice/service enhancementssupport for private insurancesupport for private insurancesupport for different scenariossupport for different scenarios
Ipsos-Reid, CFNU, January 2006.
-14
-12
-10
-8
-6
-4
-2
0
2
4
6
8
Per
cen
t (%
)
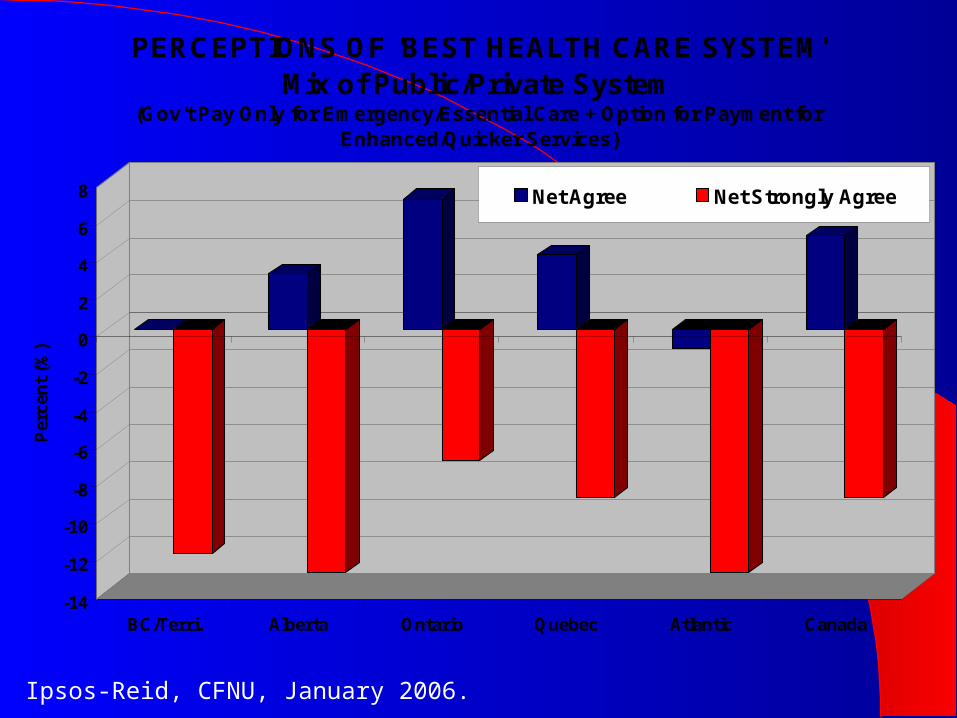
BC/Terri. Alberta Ontario Quebec Atlantic Canada
PERCEPTIONS OF 'BEST HEALTH CARE SYSTEM'Mix of Public/Private System
(Gov't Pay Only for Emergency/Essential Care + Option for Payment for Enhanced/Quicker Services)
Net Agree Net Strongly Agree

Ipsos-Reid, CMA, June 2006.
0
5
10
15
20
25
30
35
40
45
Per
cen
t (%
)
BC Alberta MB/SK Ontario Quebec Atlantic Canada
PREFERENCES FOR HEALTH CARE SCENARIOS, 2006Status Quo vs. Medicare + Parallel Private System
Status Quo
Medicare+Parallel Private
Net Status Quo
Ipsos-Reid, CMA, June 2006.
-20
-15
-10
-5
0
5
10
15
20
25
Per
cen
t (%
)
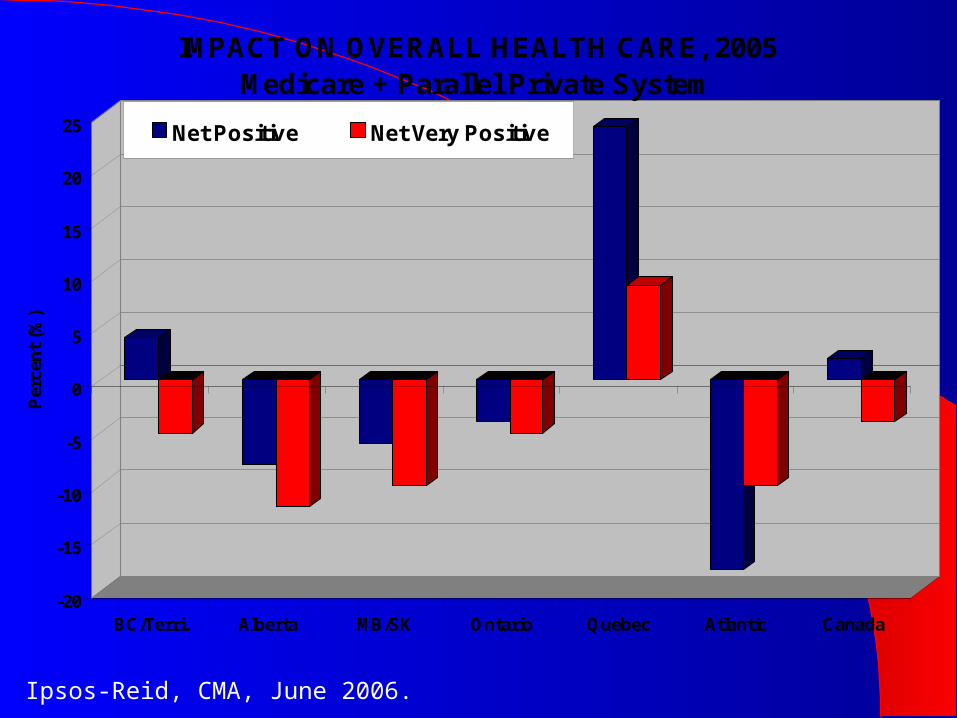
BC/Terri. Alberta MB/SK Ontario Quebec Atlantic Canada
IMPACT ON OVERALL HEALTH CARE, 2005Medicare + Parallel Private System
Net Positive Net Very Positive

Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial PerspectiveAlberta public opinion not more favourable Alberta public opinion not more favourable
to private funding/private insurance than to private funding/private insurance than other provinces (and probably less so) – other provinces (and probably less so) – WHY?WHY?
public perceptions of the quality of public health public perceptions of the quality of public health servicesservices
levels of spending on public health serviceslevels of spending on public health services government’s strategic approach to reformgovernment’s strategic approach to reform

Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial PerspectiveAlberta public opinion not more favourable Alberta public opinion not more favourable
to private funding/private insurance than to private funding/private insurance than other provinces (and probably less so) – other provinces (and probably less so) – WHY?WHY?
public perceptions of the quality of public health public perceptions of the quality of public health services and gov’t performance in health careservices and gov’t performance in health care
levels of spending on public health serviceslevels of spending on public health services government’s strategic approach to reformgovernment’s strategic approach to reform

Ipsos-Reid, Health Care System Report Card, August 2005.
0
10
20
30
40
50
60
Pe
rce
nt
(%)
BC Alberta SK/MB Ontario Quebec Atlantic Canada
Quality of Available Health Care Services, 2005(Graded A-F)
A
B
C
F
(A+B)-(C+F)

Ipsos-Reid, Health Care System Report Card, August 2005.
-50
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
Pe
rce
nt
(%)
BC Alberta SK/MB Ontario Quebec Atlantic Canada
GOV'T PERFORMANCE IN HEALTH CARE 2005, (Graded A-F)(A+B)-(C+F)
Provincial
Federal
Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial PerspectiveAlberta public opinion not more favourable Alberta public opinion not more favourable
to private funding/private insurance than to private funding/private insurance than other provinces (and probably less so) – other provinces (and probably less so) – WHY?WHY?
public perceptions of the quality of public health public perceptions of the quality of public health services and gov’t performance in health careservices and gov’t performance in health care
levels of spending on public health serviceslevels of spending on public health services government’s strategic approach to reformgovernment’s strategic approach to reform
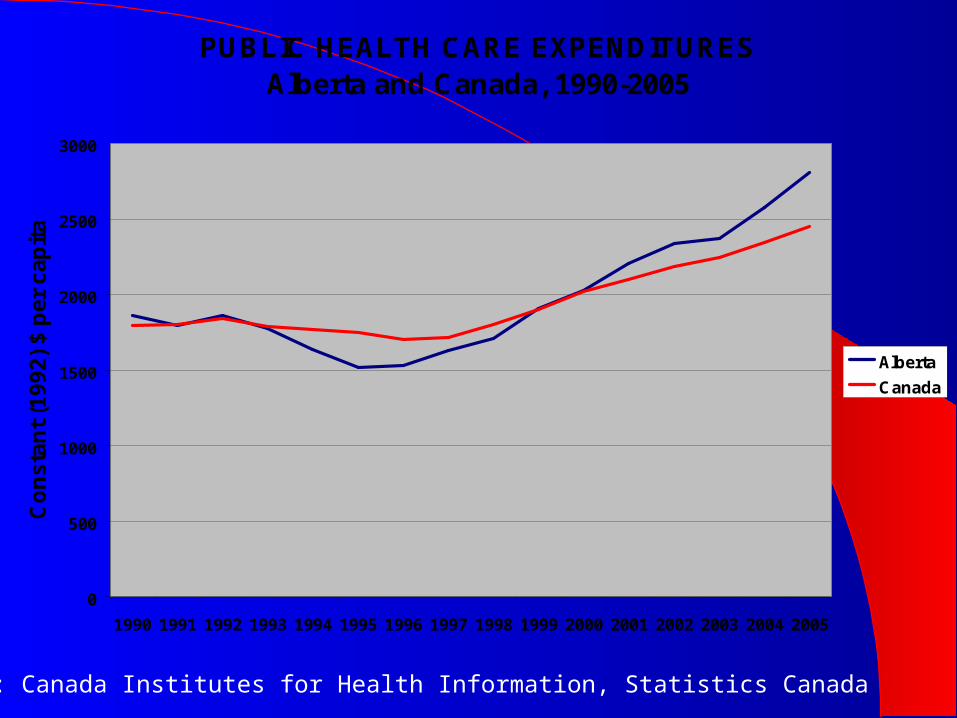
Source: Canada Institutes for Health Information, Statistics Canada
PUBLIC HEALTH CARE EXPENDITURESAlberta and Canada, 1990-2005
0
500
1000
1500
2000
2500
3000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Co
ns
tan
t (1
99
2)
$ p
er
ca
pit
a
Alberta
Canada

Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial PerspectiveAlberta public opinion not more favourable Alberta public opinion not more favourable
to private funding/private insurance than to private funding/private insurance than other provinces (and probably less so) – other provinces (and probably less so) – WHY?WHY?
public perceptions of the quality of public health public perceptions of the quality of public health servicesservices
levels of spending on public health serviceslevels of spending on public health services government’s strategic approach to reformgovernment’s strategic approach to reform
The Alberta Govt’s Strategic The Alberta Govt’s Strategic Approach to ReformApproach to Reform
““It is my preference that provincial/territorial Ministers It is my preference that provincial/territorial Ministers themselves be given an opportunity to interpret and apply the themselves be given an opportunity to interpret and apply the criteria of the criteria of the Canada Health ActCanada Health Act to their respective health care to their respective health care insurance plans.”insurance plans.”
Minister Jake EppMinister Jake EppNational Health and National Health and
Welfare CanadaWelfare Canada 19851985 ““There’s nothing that says you have to stay in the Canada Health There’s nothing that says you have to stay in the Canada Health
Act.”Act.”Premier Ralph KleinPremier Ralph Klein
June 2004June 2004 ““It may violate the Canada Health Act.”It may violate the Canada Health Act.”
Premier Ralph KleinPremier Ralph KleinMarch 2006 March 2006
(on Alberta health (on Alberta health reform proposals)reform proposals)

The Alberta Govt’s Strategic Approach to Reform, 2006 – The Alberta Govt’s Strategic Approach to Reform, 2006 – Perceptions that Reforms Violate CHAPerceptions that Reforms Violate CHA
““The Alberta government strongly supports these [CHA] principles and views them as The Alberta government strongly supports these [CHA] principles and views them as fundamental to the future evolution of the health system in this province.”fundamental to the future evolution of the health system in this province.”
Health Policy Framework 2006Health Policy Framework 2006 ““It may violate the Canada Health Act.”It may violate the Canada Health Act.”
Premier Ralph KleinPremier Ralph Kleinquoted in “Klein Willing quoted in “Klein Willing
to Defy Ottawa,”to Defy Ottawa,” Globe and Globe and Mail, 2 March Mail, 2 March 2006 2006
““The province's Health Minister, Iris Evans said...that she isn't sure whether the plan The province's Health Minister, Iris Evans said...that she isn't sure whether the plan would violate federal laws.”would violate federal laws.”
Globe and MailGlobe and Mail, 1 March 2006, 1 March 2006
Alberta Report characterized as “crossing the Rubicon of health care” and “breaching Alberta Report characterized as “crossing the Rubicon of health care” and “breaching the firewall” the firewall”
Don Martin, Don Martin, National PostNational Post, 2 March 2006, 2 March 2006 “…“…marks the beginning of the end of medicare as practiced today in Canada; the end marks the beginning of the end of medicare as practiced today in Canada; the end
of the Canada Health Act, at least as conventionally interpreted; the end of the of the Canada Health Act, at least as conventionally interpreted; the end of the world’s only fully publicly funded health-care delivery system; the end of the world’s only fully publicly funded health-care delivery system; the end of the guarantee that only need, and never wealth, will determine who gets served first.”guarantee that only need, and never wealth, will determine who gets served first.”
John Ibbotson, John Ibbotson, Globe and Globe and MailMail, 5 March, 2006, 5 March, 2006
““Mr. Klein...said those who opposed the province's plan had confused the public Mr. Klein...said those who opposed the province's plan had confused the public about what it would mean.”about what it would mean.”
Globe and MailGlobe and Mail, 21 April 2006, 21 April 2006
““The minister [Alberta Health Minister Iris Evans] said a The minister [Alberta Health Minister Iris Evans] said a Supreme Court of Canada ruling last spring opened the door to Supreme Court of Canada ruling last spring opened the door to broadening the use of private insurance for primary health-care broadening the use of private insurance for primary health-care treatments...”treatments...”
Calgary HeraldCalgary Herald, 14 Sept. 2005, 14 Sept. 2005
““It's impossible to know whether Evans is leading the charge for It's impossible to know whether Evans is leading the charge for a private, parallel health-care system, finally free of the a private, parallel health-care system, finally free of the constraints of the Canada Health Act, or for more modest constraints of the Canada Health Act, or for more modest reforms. […] Are we talking about a major realignment of reforms. […] Are we talking about a major realignment of services -- as if the Canada Health Act didn't exist -- where only services -- as if the Canada Health Act didn't exist -- where only public service is limited to expensive hospital treatment? Or public service is limited to expensive hospital treatment? Or some tinkering?”some tinkering?”
Sheila PrattSheila PrattEdmonton JournalEdmonton Journal, ,
25 Sept. 200525 Sept. 2005
The Alberta Govt’s Strategic Approach to Reform, 2006 – The Alberta Govt’s Strategic Approach to Reform, 2006 – Perceptions that Significant Reforms Perceptions that Significant Reforms MustMust Violate CHA Violate CHA

Ipsos-Reid, CFNU, January 2006.
-30
-20
-10
0
10
20
30
40
50
60
70
Pe
rce
nt
(%)
BC Alberta SK/MB Ontario Quebec Atlantic Canada
PREFERENCES FOR STRONG CHA ENFORCEMENT VS. GREATER PROVINCIAL LATITTUDE, 2006
Strong CHA EnforcementGreater Provincial LatitudeNet CHA Support

0
10
20
30
40
50
60
70
80
90
Per
cen
t (%
)
BC/Terri. Alberta MB/SK Ontario Quebec Atlantic Canada
SUPPORT FOR CONDITIONS ON ALL FEDERAL HEALTH TRANSFERS, 2005
Net Agree Net Strongly Agree
Ipsos-Reid, CFNU, January 2006.
The Paradox...The Paradox...
““Alberta is the testing ground of health care commercialization – Alberta is the testing ground of health care commercialization – and nose-thumbing at the and nose-thumbing at the Canada Health ActCanada Health Act – and its role as a – and its role as a national “Trojan Horse” in pushing privatization has yielded national “Trojan Horse” in pushing privatization has yielded impressive results elsewhere in the country...”impressive results elsewhere in the country...”
CUPECUPEInnovation Innovation
ExposedExposed, Oct.2004 , Oct.2004 "Alberta, of all the provinces in Canada, is the most hostile "Alberta, of all the provinces in Canada, is the most hostile
towards private clinics. We couldn't function in Alberta." towards private clinics. We couldn't function in Alberta." Dr. Brian DayDr. Brian Day
President Elect – CMAPresident Elect – CMAFounder, Cambie Founder, Cambie
Surgical ServicesSurgical Services Edmonton Edmonton Journal, Journal, 18 Sept.200518 Sept.2005

The Paradox...The Paradox...
““Alberta is the testing ground of health care commercialization – Alberta is the testing ground of health care commercialization – and nose-thumbing at the and nose-thumbing at the Canada Health ActCanada Health Act – and its role as a – and its role as a national “Trojan Horse” in pushing privatization has yielded national “Trojan Horse” in pushing privatization has yielded impressive results elsewhere in the country...”impressive results elsewhere in the country...”
CUPECUPEInnovation Innovation
ExposedExposed, Oct.2004, Oct.2004 "Alberta, of all the provinces in Canada, is the most hostile "Alberta, of all the provinces in Canada, is the most hostile
towards private clinics. We couldn't function in Alberta." towards private clinics. We couldn't function in Alberta." Dr. Brian DayDr. Brian Day
President Elect – CMAPresident Elect – CMAFounder, Cambie Founder, Cambie
Surgical ServicesSurgical Services Edmonton Edmonton Journal, Journal, 18 Sept.200518 Sept.2005

Alberta Public Opinion in Cross-Alberta Public Opinion in Cross-Provincial PerspectiveProvincial Perspective MAIN POINTS...MAIN POINTS...
– Alberta public opinion less favourably predispoed Alberta public opinion less favourably predispoed toward private funding/private insurance than is the toward private funding/private insurance than is the case generally in other provincescase generally in other provinces
– the Alberta government’s strategic approach to reform the Alberta government’s strategic approach to reform probably contributes significantly to this outcomeprobably contributes significantly to this outcome
undermines the political construction of a public consensus in undermines the political construction of a public consensus in favour of reformfavour of reform

The Answer...The Answer... relatively sophisticated political calculation based on a relatively sophisticated political calculation based on a
number of factors...number of factors...– electoral benefits are unclearelectoral benefits are unclear
public opinion in Alberta no more (and likely less) supportive than public opinion in Alberta no more (and likely less) supportive than public opinion in other provincespublic opinion in other provinces
– Alberta government has contributed to an emphasis on Alberta government has contributed to an emphasis on federal-provincial aspects of reformfederal-provincial aspects of reform
has undermined construction of a public consensus around reformshas undermined construction of a public consensus around reforms
– health care funding not as pressing a health care funding not as pressing a politicalpolitical problem as problem as often made outoften made out
strong fiscal capacity make acceptance of the status quo a more strong fiscal capacity make acceptance of the status quo a more politically palatable optionpolitically palatable option
– Alberta government views health care reform as key Alberta government views health care reform as key ideological battlegroundideological battleground
reticent to experiment if success is not guaranteedreticent to experiment if success is not guaranteed
The Alberta Govt’s Strategic The Alberta Govt’s Strategic Approach to ReformApproach to Reform WHY??WHY??
– recast provincial health reform as an issue relating to federal recast provincial health reform as an issue relating to federal intrusion into a field of provincial jurisdictionintrusion into a field of provincial jurisdiction
– rallying the baserallying the base not an appropriate strategy for a broader electoral appealnot an appropriate strategy for a broader electoral appeal
– blame avoidance for failing to undertake health care reforms blame avoidance for failing to undertake health care reforms which are not broadly politically popularwhich are not broadly politically popular
““Both Prime Minister Stephen Harper and federal Health Minister Both Prime Minister Stephen Harper and federal Health Minister Tony Clement had expressed concern in recent weeks that Alberta's Tony Clement had expressed concern in recent weeks that Alberta's proposed reforms, which Premier Ralph Klein had dubbed the Third proposed reforms, which Premier Ralph Klein had dubbed the Third Way, could violate the Canada Health Act -- something Ottawa could Way, could violate the Canada Health Act -- something Ottawa could address by withholding transfer payments. Mr. Klein took the federal address by withholding transfer payments. Mr. Klein took the federal government to task yesterday, saying it offered no alternatives.”government to task yesterday, saying it offered no alternatives.”
Globe & MailGlobe & Mail, , 21 April 200621 April 2006

The Answer...The Answer... relatively sophisticated political calculation based on a relatively sophisticated political calculation based on a
number of factors...number of factors...– electoral benefits are unclearelectoral benefits are unclear
public opinion in Alberta no more (and likely less) supportive than public opinion in Alberta no more (and likely less) supportive than public opinion in other provincespublic opinion in other provinces
– Alberta government has contributed to an emphasis federal-Alberta government has contributed to an emphasis federal-provincial aspects of reformprovincial aspects of reform
has undermined construction of a public consensus around reformshas undermined construction of a public consensus around reforms
– health care funding not as pressing a health care funding not as pressing a politicalpolitical problem as problem as often made outoften made out
strong fiscal capacity make acceptance of the status quo a more strong fiscal capacity make acceptance of the status quo a more politically palatable optionpolitically palatable option
– Alberta government views health care reform as key Alberta government views health care reform as key ideological battlegroundideological battleground
reticent to experiment if success is not guaranteedreticent to experiment if success is not guaranteed
Alberta Health ExpendituresAlberta Health Expenditures
““crowding out” argumentcrowding out” argument– ““Spending on health is crowing out other Spending on health is crowing out other
important areas like eduction, infrastructure, important areas like eduction, infrastructure, social services or security. If health spending social services or security. If health spending trends don’t change, by 2008 we could be trends don’t change, by 2008 we could be spending half of the province’s program budget spending half of the province’s program budget on health. We do not believe that is on health. We do not believe that is acceptable.”acceptable.”
Mazankowsi Report, 2001: 4Mazankowsi Report, 2001: 4

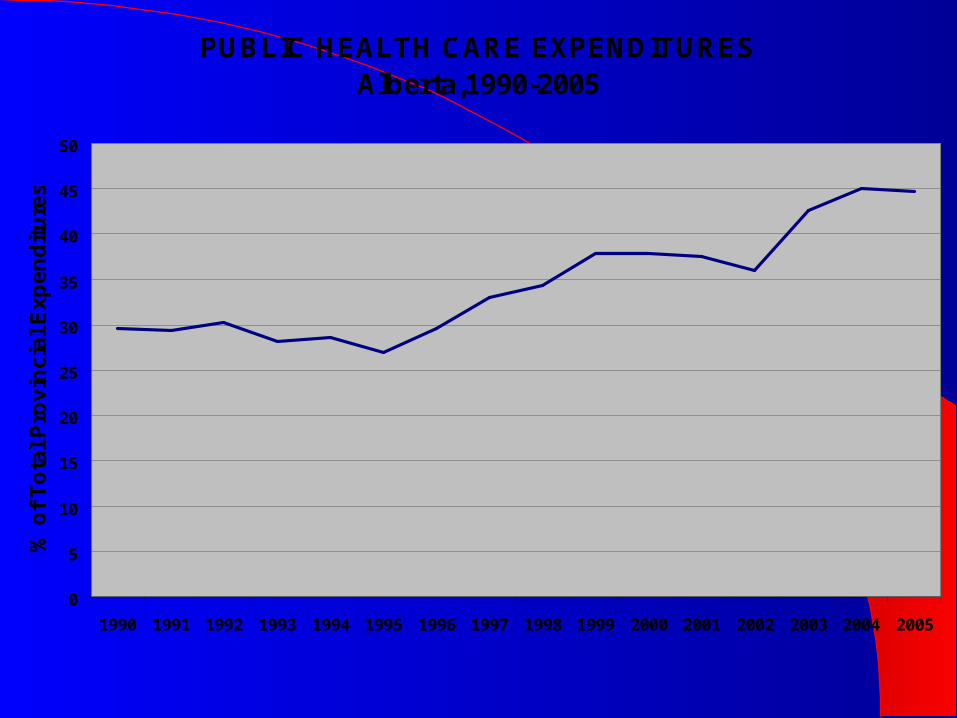
PUBLIC HEALTH CARE EXPENDITURESAlberta,1990-2005
0
5
10
15
20
25
30
35
40
45
50
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
% o
f T
ota
l P
rov
inc
ial
Ex
pe
nd
itu
res

Source: Canada Institutes for Health Information, Statistics Canada
PUBLIC HEALTH CARE EXPENDITURESAlberta and Canada, 1990-2005
0
500
1000
1500
2000
2500
3000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
Co
ns
tan
t (1
99
2)
$ p
er
ca
pit
a
Alberta
Canada


Source: Canada Institutes for Health Information, Statistics Canada
ALBERTA PROVINCIAL EXPENDITURESTotal Expenditures and Total Health Expenditures
0
5
10
15
20
25
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
% o
f G
DP
Health Expenditures
Total Expenditures
Total Revenue
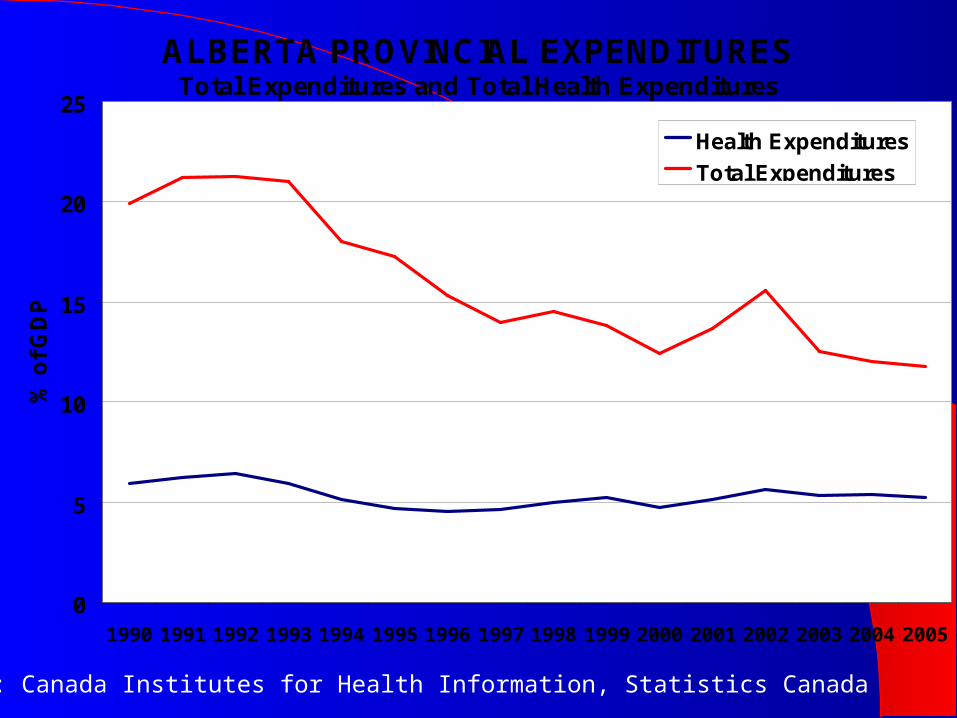
Source: Canada Institutes for Health Information, Statistics Canada
ALBERTA PROVINCIAL EXPENDITURESTotal Expenditures and Total Health Expenditures
0
5
10
15
20
25
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
% o
f G
DP
Health Expenditures
Total Expenditures

Source: Canada Institutes for Health Information, Statistics Canada
ALBERTA PROVINCIAL EXPENDITURESTotal Expenditures and Total Health Expenditures
0
5
10
15
20
25
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
% o
f G
DP
Health Expenditures
Total Expenditures
Total Revenue
PUBLIC HEALTH CARE EXPENDITURESAlberta,1990-2005
0
5
10
15
20
25
30
35
40
45
50
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
% o
f T
ota
l P
rov
inc
ial
Ex
pe
nd
itu
res

Alberta Health ExpendituresAlberta Health Expenditures
““crowding out” argumentcrowding out” argument– questionable logicquestionable logic
undue focus on health care expenditures (vs. tax undue focus on health care expenditures (vs. tax relief, debt reduction)relief, debt reduction)
– empirical evidence??empirical evidence??

Source: Canada Institutes for Health Information, Statistics Canada
Provincial Expenditures, 1990-2005Health and Education
0
500
1000
1500
2000
2500
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
Co
nst
ant
(199
2) $
per
cap
ita
Health
Total Education
E/S
PSE

Column B No Lag Column B Lagged Health Lagged
General Category
Specific Expenditure/Revenue Category
Annual % Increase
Rate of Change (Annual Increase)
Annual % Increase
Rate of Change (Annual Increase)
Annual % Increase
Rate of Change (Annual Increase)
Other Expenditure
Lag1 yr.
Lag2 yr.
Lag1 yr.
Lag2 yr.
Lag1 yr.
Lag2 yr.
Lag1 yr.
Lag2 yr.
Total Education 0.14 (0.02)
0.22 (0.05)
0.09 (0.01)
0.16 (0.03)
-0.03(-0.00)
0.14 (0.02)
-0.23(-0.05)
-0.32(-0.10)
-0.16(-0.03)
-0.27(-0.07)
Elementary/Secondary Education
-0.13 (-0.02)
0.15 (0.02)
-0.12 (-0.01)
0.13 (0.02)
-0.10(-0.01)
0.17 (0.03)
-0.43(-0.19)
-0.33 (0.11)
-0.24(-0.06)
-0.14(-0.02)
PSE 0.48 (0.23)
0.24 (0.06)
0.32 (0.10)
0.11 (0.01)
0.01 (0.00)
0.05 (0.00)
0.26 (0.07)
-0.14(-0.02)
0.03 (0.00)
-0.34(-0.11)
Debt Reduction 0.33 (0.11)
0.49 (0.24)
-0.13(-0.02)
-0.54(-0.29)
-0.10(-0.01)
-0.46(-0.21)
0.13 (0.02)
-0.66(-0.43)
0.43 (0.19)
-0.78(-0.62)
()=R()=R22
Correlation Between Health Expenditures and Other Expenditure, Alberta, Correlation Between Health Expenditures and Other Expenditure, Alberta, 1990-20051990-2005

Column B No Lag Column B Lagged Health Lagged
General Category
Specific Expenditure/Revenue Category
Annual % Increase
Rate of Change (Annual Increase)
Annual % Increase
Rate of Change (Annual Increase)
Annual % Increase
Rate of Change (Annual Increase)
Lag 1 yr.
Lag2 yr.
Lag1 yr.
Lag2 yr.
Lag1 yr.
Lag2 yr.
Lag1 yr.
Lag2 yr.
Revenue Own Source Revenue
0.20 (0.04)
0.21 (0.04)
-0.09(-0.01)
-0.09(-0.01)
-0.18(-0.03)
-0.21(-0.04)
0.09 (0.01)
-0.11(-0.01)
0.13 (0.02)
-0.08(-0.01)
Investment Income 0.38 (0.15)
0.36 (0.13)
0.00 (0.00)
-0.05(-0.00)
-0.24(-0.06)
-0.19(-0.04)
0.20 (0.04)
-0.10(-0.01)
0.19 (0.03)
-0.17(-0.03)
Income Tax -0.13(-0.02)
0.04 (0.00)
-0.21(-0.04)
-0.49(-0.24)
0.31 (0.09)
-0.09(-0.01)
-0.34(-0.12)
0.25 (0.06)
-0.20(-0.04)
0.24 (0.06)
Personal Income Tax
-0.23(-0.04)
-0.25(-0.06)
-0.23(-0.05)
-0.16(-0.02)
-0.01(-0.00)
0.39 (0.16)
0.07 (0.01)
0.45 (0.20)
0.07 (0.00)
0.40 (0.16)
Corporate Income Tax
0.07 (0.01)
0.24 (0.06)
0.06 (0.00)
-0.28(-0.08)
0.39 (0.15)
-0.45(-0.20)
-0.46(-0.21)
-0.21(-0.04)
-0.27(-0.07)
-0.18 (0.03)
()=R()=R22
Correlation Between Health Expenditures and Revenues, Alberta, 1990-2005Correlation Between Health Expenditures and Revenues, Alberta, 1990-2005
Alberta Health ExpendituresAlberta Health Expenditures
MAIN POINTS...MAIN POINTS...– ““crowding out”crowding out”
alternative interpretation – alternative interpretation – growthgrowth in provincial fiscal capacity has in provincial fiscal capacity has been shared between tax relief, debt reduction, and health carebeen shared between tax relief, debt reduction, and health care
– ““crowding out” hypothesis must have some empirical content crowding out” hypothesis must have some empirical content initial indicators -- does not appear to be the caseinitial indicators -- does not appear to be the case
– strong economic growth makes health funding status quo more strong economic growth makes health funding status quo more politically palatablepolitically palatable
it is politically easier to divided a growing pie than a shrinking oneit is politically easier to divided a growing pie than a shrinking one so long as budgets of other services are keeping pace with inflation so long as budgets of other services are keeping pace with inflation
and population growth, disproportionate growth in health care is not and population growth, disproportionate growth in health care is not politicallypolitically problematic problematic
The Answer...The Answer... relatively sophisticated political calculation based on a relatively sophisticated political calculation based on a
number of factors...number of factors...– electoral benefits are unclearelectoral benefits are unclear
public opinion in Alberta no more (and likely less) supportive than public opinion in Alberta no more (and likely less) supportive than public opinion in other provincespublic opinion in other provinces
– Alberta government has contributed to an emphasis federal-Alberta government has contributed to an emphasis federal-provincial aspects of reformprovincial aspects of reform
has undermined construction of a public consensus around reformshas undermined construction of a public consensus around reforms
– health care funding not as pressing a political problem as health care funding not as pressing a political problem as often made outoften made out
strong fiscal capacity make acceptance of the status quo a more strong fiscal capacity make acceptance of the status quo a more politically palatable optionpolitically palatable option
– Alberta government views health care reform as key Alberta government views health care reform as key ideological battlegroundideological battleground
reticent to experiment if success is not guaranteedreticent to experiment if success is not guaranteed
Health Care as Ideological Health Care as Ideological BattlegroundBattleground
highly directive approach to ‘opening up’ the health care system to highly directive approach to ‘opening up’ the health care system to private insuranceprivate insurance
RFIs/RFPsRFIs/RFPs actuarial reviewactuarial review proposal to approve a single private insurerproposal to approve a single private insurer
alternative viewalternative view– ““Some MLAs argued that Evans should simply announce a list of services Some MLAs argued that Evans should simply announce a list of services
that will be pay-for-priority and see which insurers come in to take up the that will be pay-for-priority and see which insurers come in to take up the challenge.”challenge.”
Edmonton Journal, Edmonton Journal, 14 September 14 September 2005 2005
– ““Alberta's tepid decision to keep on ‘studying’ the issue is the furthest Alberta's tepid decision to keep on ‘studying’ the issue is the furthest thing from anarchy. It's time to stop making excuses and loosen up the thing from anarchy. It's time to stop making excuses and loosen up the rules.”rules.”
Editorial, Editorial, Calgary HeraldCalgary Herald, 15 Sept. 2005, 15 Sept. 2005– these analyses ignore the perceived these analyses ignore the perceived politicalpolitical costs of failure costs of failure

ConclusionsConclusions
...the second ‘Third Option’?...the second ‘Third Option’?– Option #1 Status QuoOption #1 Status Quo– Option #2 Violation of Option #2 Violation of CHACHA– Option #3 Aggressive Redefinition of Public/Private Option #3 Aggressive Redefinition of Public/Private
Role in Health Funding within Role in Health Funding within CHACHA
ConclusionsConclusions
maximum redefinition allowed under CHAmaximum redefinition allowed under CHA– remove legal restrictions on private provision of privately funded remove legal restrictions on private provision of privately funded
servicesservices e.g. public monopoly of emergency services and major surgerye.g. public monopoly of emergency services and major surgery
– provide public subsidization of private insurance premiumsprovide public subsidization of private insurance premiums waive public premiums for individuals who purchase private insurancewaive public premiums for individuals who purchase private insurance
– provide coverage of physicians fee (non-participating, participating?) provide coverage of physicians fee (non-participating, participating?) outside of the plan (up to fixed %)outside of the plan (up to fixed %)
– facility fees in public facilities (up to fixed %) for ‘private’ patientsfacility fees in public facilities (up to fixed %) for ‘private’ patients allowable for services provided to private patientsallowable for services provided to private patients
– non-participating physiciansnon-participating physicians• grant hospital privileges to non-participating physiciansgrant hospital privileges to non-participating physicians
– participating physicians participating physicians • if physician fee is not publicly reimbursed (e.g. New Brunswick)if physician fee is not publicly reimbursed (e.g. New Brunswick)• if patient is publicly reimubursed for physician fee??if patient is publicly reimubursed for physician fee??

ConclusionsConclusions
political strategy political strategy make legislative changes and allow private make legislative changes and allow private
providers/insurers to react through the market (rather than providers/insurers to react through the market (rather than through government directed consultations)through government directed consultations)
emphasize that reforms are in keeping with emphasize that reforms are in keeping with CHACHA emphasize elements of reform already existing in other emphasize elements of reform already existing in other
provincesprovinces undertake reforms and allow federal government to undertake reforms and allow federal government to
challengechallenge– use dispute resolution mechanism to full extentuse dispute resolution mechanism to full extent– political pressure on federal government will be higher in the political pressure on federal government will be higher in the
case of existing (rather than hypothetical) practicescase of existing (rather than hypothetical) practices
ConclusionsConclusions
failure to achieve health financing reforms is not failure to achieve health financing reforms is not the result of external constraints (e.g. CHA) but the result of external constraints (e.g. CHA) but determined by domestic politicsdetermined by domestic politics
failure to achieve reform of health financing in failure to achieve reform of health financing in Alberta is not paradoxical – result of deliberate Alberta is not paradoxical – result of deliberate political calculationpolitical calculation– health reform in Alberta hs been the political health reform in Alberta hs been the political meansmeans
rather than the policy endsrather than the policy ends rather than allowing experimentation, federal-rather than allowing experimentation, federal-
provincial entaglement in health care has provincial entaglement in health care has contributed to sclerosis (through blame avoidance)contributed to sclerosis (through blame avoidance)