Embed Size (px)
Citation preview
http://ajs.sagepub.com/
MedicineThe American Journal of Sports
http://ajs.sagepub.com/content/35/11/1940The online version of this article can be found at:
DOI: 10.1177/0363546507304175
2007 35: 1940 originally published online July 16, 2007Am J Sports MedNobuyasu Ochiai, James P. Tasto, Seiji Ohtori, Norimasa Takahashi, Hideshige Moriya and David Amiel
Nerve Regeneration After Radiofrequency Application
Published by:
http://www.sagepublications.com
On behalf of:
American Orthopaedic Society for Sports Medicine
can be found at:The American Journal of Sports MedicineAdditional services and information for
http://ajs.sagepub.com/cgi/alertsEmail Alerts:
http://ajs.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
at UNIV CALIFORNIA SAN DIEGO on January 10, 2010ajs.sagepub.comDownloaded from

1940
Chronic tendinopathy, like medial and lateral epicondylitisand patellar and Achilles tendinopathy, is a well-knownpainful orthopaedic disease. The characteristic pathologiccharacteristics of all these tendinosis conditions are linkedto microrupture of the tendon,4,5 granulation tissue,9 anddegenerative changes.13,15 Nonsteroidal anti-inflammatorymedication, physical therapy, steroid injections, and
orthoses are symptomatic treatment for these and variousother orthopaedic conditions, while arthroscopic or opensurgery is reserved for patients with insufficient responseto less invasive procedures.
Neovessels and accompanying free nerve endings havebeen observed in tendinosis tissue using Protein GeneProduct 9.5 immunohistochemistry.2 Furthermore, the ten-don insertion, which is supplied with substance P (SP) andcalcitonin gene-related peptide (CGRP) innervation, hasbeen implicated in the origins of tennis elbow.11 The ratmodel of Achilles tendinosis showed an increased number ofnerve filaments and increased immunoreactivity for SP andCGRP.12 Neuropeptides SP and CGRP are not only involvedin transmitting nociceptive information to the spinal cord, butalso in peripheral effects, including microvascular leakageand local edema formation.21 Pathological nerve ingrowthmay have been involved in the origin of tendinosis.11 On the
Nerve Regeneration After RadiofrequencyApplicationNobuyasu Ochiai,* MD, PhD, James P. Tasto,† MD, Seiji Ohtori,‡ MD, PhD,Norimasa Takahashi,‡ MD, PhD, Hideshige Moriya,‡ MD, PhD, and David Amiel,*§ PhDFrom the *Department of Orthopedic Surgery, University of California San Diego,La Jolla, California, †San Diego Sports Medicine & Orthopedic Center, San Diego, California,and the ‡Department of Orthopedic Surgery, Graduate School of Medicine,Chiba University, Chiba, Japan
Background: Many patients with chronic tendinosis have experienced early pain relief after application of bipolar radiofrequencytreatment. It is hypothesized that the mechanism of action may be the acute degeneration and/or ablation of sensory nerve fibers.
Hypothesis: After ablation or degeneration by bipolar radiofrequency, nerve fibers will have the ability to regenerate with time.
Study Design: Controlled laboratory study.
Methods: Eighteen Sprague-Dawley rats were used in this study. These rats were divided into 3 groups (30, 60, and 90 daysafter bipolar radiofrequency). These rats were treated with 2 points of bipolar radiofrequency applications to the left hindpawswith the Topaz microdebrider device. Right hindpaws were used as the contralateral control. Tissues were processed for neuralclass III β-tubulin or calcitonin gene-related peptide immunohistochemistry by using the free-floating avidin biotin complex tech-nique. The numbers of neural class III β-tubulin–immunoreactive and calcitonin gene-related peptide-immunoreactive nervefibers in the epidermis were counted and compared with those in the contralateral control.
Results: Although the numbers of nerve fibers demonstrated by both the antibodies of neural class III β-tubulin and calcitoningene-related peptide were significantly decreased (P < .0001) until 60 days after bipolar radiofrequency treatment, regenerationof the epidermal nerve fibers occurred 90 days after treatment.
Conclusion: Bipolar radiofrequency treatment induced degeneration of sensory nerve fibers immediately after treatment, but by90 days posttreatment, there was evidence of complete regeneration.
Clinical Relevance: Early degeneration followed by later regeneration of nerve fibers after bipolar radiofrequency treatment mayexplain long-term postoperative pain relief after microtenotomy for tendinosis.
Keywords: bipolar radiofrequency; chronic tendinosis; microtenotomy; pain relief
§Address correspondence to David Amiel, PhD, Department ofOrthopedic Surgery, Connective Tissue Biochemistry, 9500 Gilman Drive,Department 0630, La Jolla, CA 92093-0630 (e-mail: [email protected]).
One or more of the authors has declared a potential conflict of interest:Drs Tasto and Amiel are members of the Medical and Scientific AdvisoryBoard for ArthroCare Corp.
The American Journal of Sports Medicine, Vol. 35, No. 11DOI: 10.1177/0363546507304175© 2007 American Orthopaedic Society for Sports Medicine
at UNIV CALIFORNIA SAN DIEGO on January 10, 2010ajs.sagepub.comDownloaded from

Vol. 35, No. 11, 2007 Nerve Regeneration After Radiofrequency Application 1941
other hand, CGRP is important for formation of new vesselsduring wound healing.10 Furthermore, CGRP is vasoactive innormal rabbit medial collateral ligaments, suggesting that itmay participate in the maintenance of ligament homeostasisand the promotion of soft tissue healing.7
Recently extracorporeal shock wave therapy (ESWT)17 andbipolar radiofrequency (bRF) microtenotomy20 have been usedfor the treatment of chronic tendinosis. Clinically, the majorityof patients with chronic lateral epicondylitis received at leastsome pain relief within the first 7 to 10 days, and it lasted atleast 2 years after bRF microtenotomy. The pathomechanismof pain relief after ESWT14 and bRF microtenotomy18 isthought to be acute degeneration of epidermal nerve fibers inthe early period. A previous study showed that bRF treatmentinduced acute degeneration or ablation of the sensory nervefibers for at least 2 weeks.18 Although regeneration of the epi-dermal nerve fibers was observed 2 weeks after ESWT,14
regeneration after bRF is still unknown.We hypothesized thatmicrotenotomy with bRF-induced degeneration of the nervefibers would be followed by regeneration. Regeneration ofnerve fibers would be necessary to resume normal tendon con-dition that leads to long-term effect by bRF, similar to theprocess of wound healing.10 The purpose of this study was toevaluate the regeneration potential of peripheral nerve fibersafter bRF application using a rat model.
MATERIALS AND METHODS
Following Institutional Animal Care and Use Committeeand our institution’s Animal Subjects Committee approval,we used 18 male Sprague-Dawley rats (weight, 250-300 g)divided into 3 groups (30, 60, and 90 days after bRF). Theywere anesthetized with isofluorane (VEDCO Inc, StJoseph, Mo) and sodium pentobarbital (Abbott Labs,Chicago, Ill) and treated aseptically throughout bRF appli-cations. Two separate points of bRF were equally applied (ata distance of 1-3 mm from each other for 500 ms) to the mid-dle 2 footpads of the left hindpaw of the 18 rats. The TOPAZMicrodebrider device (ArthroCare, Sunnyvale, Calif) con-nected to a System 2000 generator at a setting of 4 V-RMS(voltage-root metered squared) was used to perform the bRFapplication. In this process, bRF energy is used to excite theelectrolytes in normal saline, and the energized particleshave sufficient energy to break molecular bonds, ablatingsoft tissue at low temperatures (40°-70°C). After treatment,the rats were allowed activity as tolerated.
Rats treated by bRF after 30 (n = 6), 60 (n = 6), and 90 days(n = 6) were anesthetized with ketamine (80 mg/kg intraperi-toneal) and isofluorane and perfused transcardially with 0.9%saline, followed by 500 mL 4% paraformaldehyde in a phos-phate buffer (0.1 1M, pH 7.4). The footpads of both rat hind-paws were resected (left for study group, right for thecontralateral control group). After being stored in 0.01 Mphosphate buffered saline (PBS) containing 20% sucrosefor 20 hours at 4°C, the specimens were sectioned at a 30-µm thickness on a cryostat. Twenty sections were collectedin PBS. Half of them were processed for neural class III β-tubulin (TUJ-1) for immunochemistry, and the other halfwere processed for CGRP immunohistochemistry1 by using
the free-floating avidin biotin complex (ABC) technique.They were incubated for 20 hours at 4°C with mouse anti-body for TUJ-1 (1:500; Convance, Berkeley, Calif) or rabbitantibody for CGRP (1:500; ImmunoStar Inc, Hudson, Wis)diluted with a blocking solution in 0.01 M PBS containing0.3% Triton X-100, 5% skim milk (Becton, Dickinson andCompany, Sparks, Md), and 0.05% bovine serum albumin(Sigma-Aldrich, St Louis, Mo). After thorough washing, sec-tions were incubated for 90 minutes in an Alexa Fluor 488labeled goat anti-mouse IgG (1:100; Molecular Probes,Eugene, Ore) or Alexa Fluor 488 labeled anti-rabbit IgG(1:100; Molecular Probes). The sections were then viewedwith fluorescent light microscopy by 1 observer in our labo-ratory (N.O.), who was blinded to the experimental groupand time period of each sample, and nerve fibers that passedthrough the basement membrane of the epidermis werecounted. Branching occurred within the epidermis, butthese additional branches were not counted. The numbersof TUJ1-immunoreactive (IR) and CGRP-IR fibers werecounted for each section per 16.3 × 10-1 mm2 of epidermisin a footpad. After counting all sections in all time periods,the numbers of TUJ1-IR and CGRP-IR fibers in the 10 sec-tions of each rat were summed and then averaged in eachgroup.
Statistical analysis of results was performed usingStatView 5.0 (Statsoft, Tokorozawa, Japan). Results werepresented as mean ± standard deviation (SD) in each group.The mean numbers of nerve fibers between the bRF studygroups were matched with their respective contralateralcontrol group and were analyzed using a paired t test.
The mean numbers of nerve fibers between the bRFstudy group on day 30, day 60, and day 90 were comparedusing a nonpaired Student t test. Significance was definedas P < .05.
RESULTS
Although the RF-treated footpad had a dimple on the sur-face just after bRF application, no macroscopic differencewas detected between the bRF foot and the contralateralcontrol foot at 30, 60, and 90 days after bRF. The rats wereobserved ambulating with a normal gait immediately afterthe bRF applications.
Figure 1A shows the nerve fibers in the epidermis of thefootpad (the area in which the bRF was applied), withimmunoreactivity of the TUJ-1 in the contralateral controlsample. The contralateral control epidermis is richly inner-vated by TUJ1-IR nerve fibers.
After bRF application, nerve fibers were rarely seen inthe epidermis at day 30 (Figure 1B) and day 60 (Figure1C). There was a significant difference between the con-tralateral control and bRF group in the numbers of TUJ1-IR–stained nerve fibers (mean number of nerve fibers ±SD) at day 30 (172.9 ± 20.4 vs 91.6 ± 20.5, P < .0001) andat day 60 (169.9 ± 15.2 vs 119.1 ± 20.5, P < .0001). Therewas no significant difference between the contralateralcontrol and bRF group in the numbers of TUJ1-IR–stainednerve fibers at day 90 (169.2 ± 20.5 vs 164.7 ± 24.0, P =.6557) (Figure 1D; Figure 2).
at UNIV CALIFORNIA SAN DIEGO on January 10, 2010ajs.sagepub.comDownloaded from
1942 Ochiai et al The American Journal of Sports Medicine
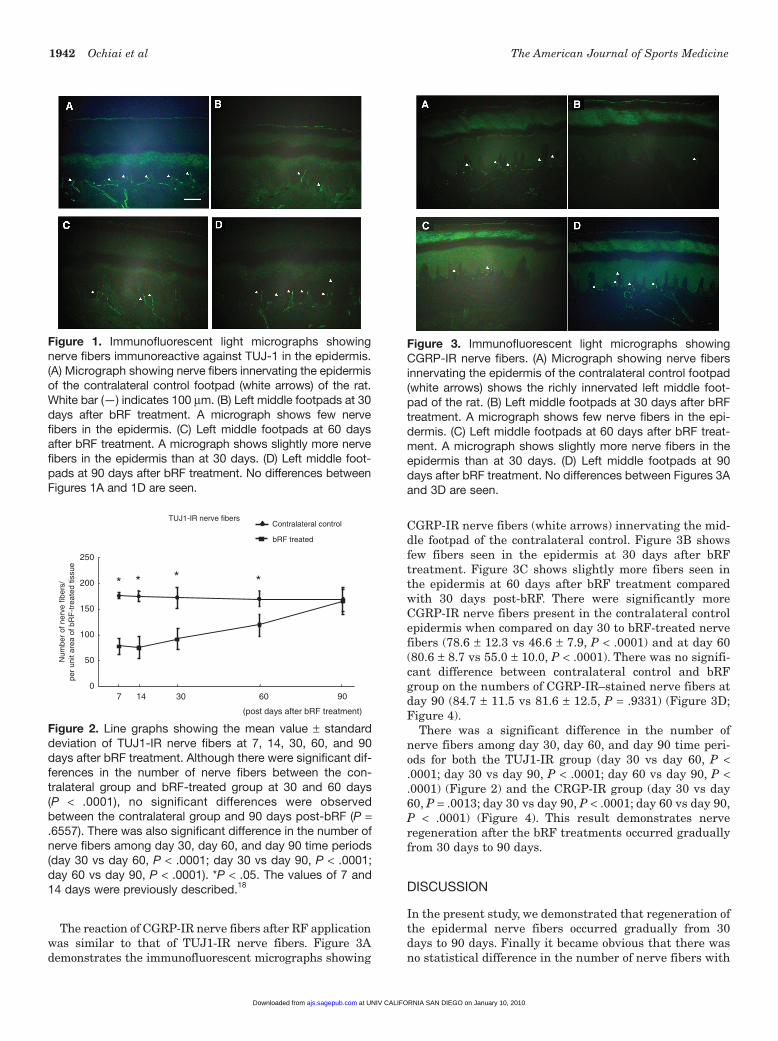
The reaction of CGRP-IR nerve fibers after RF applicationwas similar to that of TUJ1-IR nerve fibers. Figure 3Ademonstrates the immunofluorescent micrographs showing
CGRP-IR nerve fibers (white arrows) innervating the mid-dle footpad of the contralateral control. Figure 3B showsfew fibers seen in the epidermis at 30 days after bRFtreatment. Figure 3C shows slightly more fibers seen inthe epidermis at 60 days after bRF treatment comparedwith 30 days post-bRF. There were significantly moreCGRP-IR nerve fibers present in the contralateral controlepidermis when compared on day 30 to bRF-treated nervefibers (78.6 ± 12.3 vs 46.6 ± 7.9, P < .0001) and at day 60(80.6 ± 8.7 vs 55.0 ± 10.0, P < .0001). There was no signifi-cant difference between contralateral control and bRFgroup on the numbers of CGRP-IR–stained nerve fibers atday 90 (84.7 ± 11.5 vs 81.6 ± 12.5, P = .9331) (Figure 3D;Figure 4).
There was a significant difference in the number ofnerve fibers among day 30, day 60, and day 90 time peri-ods for both the TUJ1-IR group (day 30 vs day 60, P <.0001; day 30 vs day 90, P < .0001; day 60 vs day 90, P <.0001) (Figure 2) and the CRGP-IR group (day 30 vs day60, P = .0013; day 30 vs day 90, P < .0001; day 60 vs day 90,P < .0001) (Figure 4). This result demonstrates nerveregeneration after the bRF treatments occurred graduallyfrom 30 days to 90 days.
DISCUSSION
In the present study, we demonstrated that regeneration ofthe epidermal nerve fibers occurred gradually from 30days to 90 days. Finally it became obvious that there wasno statistical difference in the number of nerve fibers with
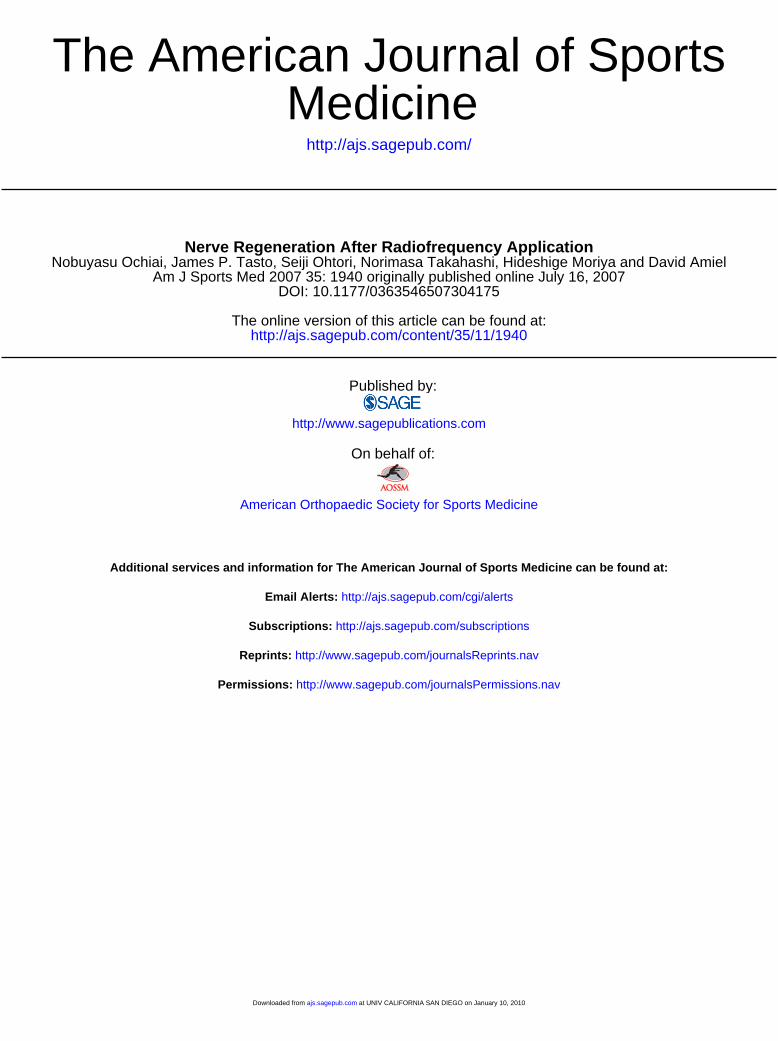
Figure 1. Immunofluorescent light micrographs showingnerve fibers immunoreactive against TUJ-1 in the epidermis.(A) Micrograph showing nerve fibers innervating the epidermisof the contralateral control footpad (white arrows) of the rat.White bar (—) indicates 100 µm. (B) Left middle footpads at 30days after bRF treatment. A micrograph shows few nervefibers in the epidermis. (C) Left middle footpads at 60 daysafter bRF treatment. A micrograph shows slightly more nervefibers in the epidermis than at 30 days. (D) Left middle foot-pads at 90 days after bRF treatment. No differences betweenFigures 1A and 1D are seen.
Figure 2. Line graphs showing the mean value ± standarddeviation of TUJ1-IR nerve fibers at 7, 14, 30, 60, and 90days after bRF treatment. Although there were significant dif-ferences in the number of nerve fibers between the con-tralateral group and bRF-treated group at 30 and 60 days(P < .0001), no significant differences were observedbetween the contralateral group and 90 days post-bRF (P =.6557). There was also significant difference in the number ofnerve fibers among day 30, day 60, and day 90 time periods(day 30 vs day 60, P < .0001; day 30 vs day 90, P < .0001;day 60 vs day 90, P < .0001). *P < .05. The values of 7 and14 days were previously described.18
Contralateral control
bRF treated
Num
ber
of n
erve
fibe
rs/
per
unit
area
of b
RF
-tre
ated
tiss
ue
TUJ1-IR nerve fibers
0
50
100
150
200
250
7 14 30 60 90
(post days after bRF treatment)
* * * *
Figure 3. Immunofluorescent light micrographs showingCGRP-IR nerve fibers. (A) Micrograph showing nerve fibersinnervating the epidermis of the contralateral control footpad(white arrows) shows the richly innervated left middle foot-pad of the rat. (B) Left middle footpads at 30 days after bRFtreatment. A micrograph shows few nerve fibers in the epi-dermis. (C) Left middle footpads at 60 days after bRF treat-ment. A micrograph shows slightly more nerve fibers in theepidermis than at 30 days. (D) Left middle footpads at 90days after bRF treatment. No differences between Figures 3Aand 3D are seen.
at UNIV CALIFORNIA SAN DIEGO on January 10, 2010ajs.sagepub.comDownloaded from
Vol. 35, No. 11, 2007 Nerve Regeneration After Radiofrequency Application 1943
the contralateral control groups. Regeneration of TUJ1-IRand CGRP-IR nerve fibers seemed to be similar to each other.
Neovascularity has been proposed to be one of the fac-tors in the origin of tendinosis. Hypovascularity inducesnot only necrosis and fibrillation in the tendon1 but alsoinduces the rupture of the tendon. Lack of vascularity com-promises the nutrition required by tendon cells, making itmore difficult for those cells to synthesize extracellularmatrix necessary for repair and remodeling for fatigue-damaged tendon.20 Regarding the effect of bRF, histologicevidence of neovessel formation and an increase in angio-genic markers demonstrated that bRF microtenotomy canincrease tissue vascularity when properly applied to ten-dons, leading to healing of the tendon.20 Although theresults revealed macroscopic and microscopic changes inthe early term, bRF-treated tendons resumed a normalappearance by 90 days.20
Neural class III β-tubulin antibody, which recognizesclass III β-tubulin exclusively, reveals the axons and theirterminations, as well as significant injury-related alter-ations.8 In this study, we demonstrated that bRF applica-tions significantly decrease the number of TUJ1-IR nervefibers by 60 days, which gradually increase by 90 days.This increase after decrease in numbers of nerve fibers wasalso found after ESWT to the rat skin but resumed rapidlyat 2 weeks.14
Calcitonin gene-related peptide has previously beenreported also to promote angiogenesis and tissue regener-ation,3,6,10 partly by stimulating proliferation of endothelialcells and fibroblasts.3,10 The effect of CGRP on endothelialcells has a potential effect in angiogenesis, including for-mation of new vessels in wound healing.10 The increase in
immunoreactivity for CGRP-IR nerve fibers may result inchanging the hypovascularity condition such as occurs intendinosis to be healed with the increase responses of thevascularity. Although this study did not clarify the confu-sion in the literature about the vascularity,2,16 we demon-strated that the CGRP-IR nerve fibers regenerate by 90days and resumed normal appearance. We postulated thatthe regeneration of the CGRP-IR nerve fibers accompaniedby the increase of vascularity is important for the healingprocess in tendinosis that may in turn be partially causedby hypovascularity.
Clinically, the majority of patients with chronic lateral epi-condylitis received at least some pain relief within the first 7to 10 days that lasted at least 2 years after bRF microteno-tomy.19 Although degeneration of sensory nerve fibers wouldlead to early pain relief,18 our study explained that the nervefibers regenerated, along with the healing process, and withpotential of no return of the pathological condition.
One of the limitations of this study is using rat skin insteadof pathological tendon. There are no suitable animal modelsfor assessing effectiveness of bRF treatment of tendinosis. Weanalyzed the abundant nerve fibers in the rat sole for aresponse to bRF. Extracorporeal shock wave therapy studyhas already showed the validity of using this model.14 Weassume that the effects of bRF would be the same for normalepidermal nerves and the pathologic nerves found in tendi-nosis. The long-lasting effectiveness of bRF in clinical cases19
would correlate with the regeneration of the nerve fibers thesame as in the contralateral control. Further study is neces-sary to determine the effects of bRF on pathological condi-tions and to confirm the expected same mechanism.
We concluded that bRF treatment induced degenerationand regeneration of the nerve fibers in the rat sole. Theseresults may explain the rapid pain relief as well as one ofthe healing responses after bRF treatment in tendinosis.
ACKNOWLEDGMENT
The authors gratefully acknowledge support from ArthroCareCorp.
REFERENCES
1. Ahmed IM, Lagopoulos M, McConnell P, Soames RW, Sefton GK.Blood supply of the Achilles tendon. J Orthop Res. 1998;16:591-596.
2. Alfredson H, Ohberg L, Forsgren S. Is vasculoneural ingrowth thecause of pain in chronic Achilles tendinosis? An investigation usingultrasonography and colour Doppler, immunohistochemistry, anddiagnostic injections. Knee Surg Sports Traumatol Arthrosc. 2003;11:334-338.
3. Brain SD. Sensory neuropeptides: their role in inflammation andwound healing. Immunopharmacology. 1997;37:133-152.
4. Coonrad RW, Hooper WR. Tennis elbow: its course, natural history,conservative, and surgical management. J Bone Joint Surg Am. 1973;55:1177-1182.
5. Cyriax JH. The pathology and treatment of tennis elbow. J Bone JointSurg. 1936;18:921-940.
6. Engin C. Effects of calcitonin gene-related peptide on wound con-traction in denervated and normal rat skin: a preliminary report. PlastReconstr Surg. 1998;101:1887-1890.
7. Ferrell WR, McDougall JJ, Bray RC. Spatial heterogeneity in the effectsof calcitonin gene-related peptide (CGRP) on the microvasculature
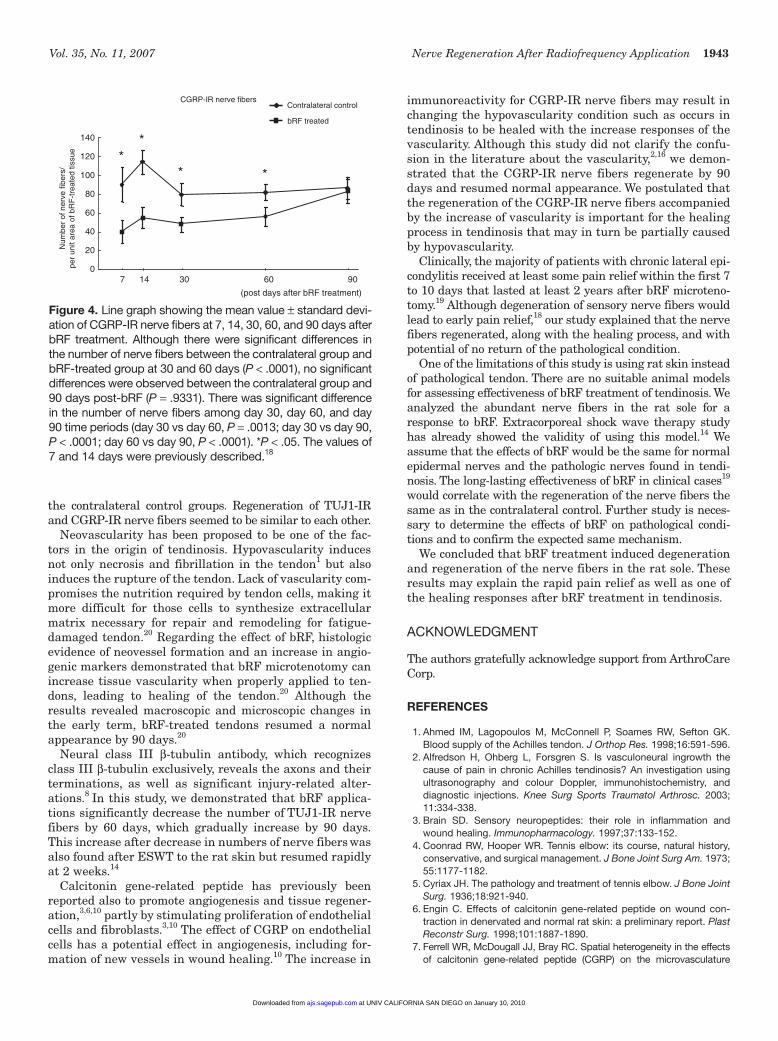
Figure 4. Line graph showing the mean value ± standard devi-ation of CGRP-IR nerve fibers at 7, 14, 30, 60, and 90 days afterbRF treatment. Although there were significant differences inthe number of nerve fibers between the contralateral group andbRF-treated group at 30 and 60 days (P < .0001), no significantdifferences were observed between the contralateral group and90 days post-bRF (P = .9331). There was significant differencein the number of nerve fibers among day 30, day 60, and day90 time periods (day 30 vs day 60, P = .0013; day 30 vs day 90,P < .0001; day 60 vs day 90, P < .0001). *P < .05. The values of7 and 14 days were previously described.18
**
(post days after bRF treatment)
CGRP-IR nerve fibers
20
40
60
80
100
120
140
7 14 30 60 900
Contralateral control
bRF treated
**
Num
ber
of n
erve
fibe
rs/
per
unit
area
of b
RF
-tre
ated
tiss
ue
at UNIV CALIFORNIA SAN DIEGO on January 10, 2010ajs.sagepub.comDownloaded from

1944 Ochiai et al The American Journal of Sports Medicine
of ligaments in the rabbit knee joint. Br J Pharmacol. 1997;121:1397-1405.
8. Geisert EE Jr, Frankfurter A. The neuronal response to injury as visu-alized by immunostaining of class III β-tubulin in the rat. NeurosciLett. 1989;102:137-141.
9. Goldie I. Epicondylitis lateralis humeri (epicondylalgia or tennis elbow):a pathogenetical study. Acta Chir Scand Suppl. 1964;339:1-119.
10. Haegerstrand A, Dalsgaard CJ, Jonzon B, Larsson O, Nilsson J.Calcitonin gene-related peptide stimulates proliferation of humanendothelial cells. Proc Natl Acad Sci USA. 1990;87:3299-3303.
11. Ljung BO, Forsgren S, Friden J. Substance P and calcitonin gene-related peptide expression at the extensor carpi radialis brevis mus-cle origin: implications for the etiology of tennis elbow. J Orthop Res.1999;17:554-559.
12. Messner K, Wei Y, Andersson B, Gillquist J, Rasanen T. Rat model ofAchilles tendon disorder. A pilot study. Cells Tissues Organs.1999;165:30-39.
13. Nirschl RP. Elbow tendinosis/tennis elbow. Clin Sports Med. 1992;11;851-870.
14. Ohtori S, Inoue G, Mannoji C, et al. Shock wave application to rat skininduces degeneration and reinnervation of sensory nerve fibers.Neurosci Lett. 2001;315:57-60.
15. Regan W, Wold LE, Coonrad R, Morrey BF. Microscopic histopathol-ogy of chronic refractory lateral epicondylitis. Am J Sports Med.1992;20:746-749.
16. Schneeberger AG, Masquelet AC. Arterial vascularization of the prox-imal extensor carpi radialis brevis tendon. Clin Orthop Relat Res.2002;398:239-244.
17. Sems A, Dimeff R, Iannotti JP. Extracorporeal shock wave therapy inthe treatment of chronic tendinopathies. J Am Acad Orthop Surg.2006;14:195-204.
18. Takahashi N, Tasto JP, Ritter M, et al. Pain relief through an antinoci-ceptive effect after radiofrequency application. Am J Sports Med.2007;35:805-810.
19. Tasto JP, Cummings J, Medlock V, Hardesty R, Amiel D. Microtenotomyusing a radiofrequency probe to treat lateral epicondylitis. Arthroscopy.2005;21:851-860.
20. Tasto JP, Cummings J, Medlock V, Harwood F, Hardesty R, Amiel D.The tendon treatment center: new horizons in the treatment of tendi-nosis. Arthroscopy. 2003;19(Suppl 1):213-223.
21. Willis WD Jr, Coggeshall RE. Chemical anatomy of dorsal root gan-glion cells. In: Sensory Mechanisms of the Spinal Cord. PrimaryAfferent Neurons and the Spinal Dorsal Horn. 3rd ed. Vol 1. New York,NY: Kluwer Academic/Plenum Publishers; 2004:103-154.
at UNIV CALIFORNIA SAN DIEGO on January 10, 2010ajs.sagepub.comDownloaded from