Embed Size (px)
Citation preview
The Art of the Possible Using CPCSSN Data for Primary Care Research
Family Medicine ForumNov 16, 2012
Karim Keshavjee - EMR Consultant & Research Data ArchitectKen Martin - Information and Technology Manager

Outline• Introduction to CPCSSN• CPCSSN Data Holdings• A Tour of CPCSSN Data Tables• Current Research Projects at CPCSSN• The Art of the Possible• How to use CPCSSN data for your research• Goodies for Today

329 physicians in 8 provinces using 10 EMRs
10 PC-PBRNs• British Columbia - BCPCReN (Wolf ) • Alberta - SaPCReN, Calgary (Med Access, Wolf) - AFRPN, Edmonton (Med Access)
• Manitoba - MaPCReN, Winnipeg (Jonoke)
• Ontario - DELPHI, London (Healthscreen, Optimed, OSCAR - NorTReN, Toronto (Nightingale, xwave, Practice Solutions) - CSPC, Kingston (P&P, OSCAR, xwave)
• Quebec - Q-Net, Montréal (Da Vinci, Purkinje)
• Nova Scotia / New Brunswick - MarNet, Halifax (Nightingale, Purkinje)
• Newfoundland - APBRN, St. John’s (Wolf , Nightingale)

CPCSSN population
CPCSSN PopulationData Extracted on all patients in the practice, including children Studying patients with the following chronic diseases
• Chronic Obstructive Lung Disease • Depression• Diabetes• Hypertension• Osteoarthritis
Chronic Neurological Disease• Dementia• Epilepsy• Parkinson's Disease

Data Holdings Q2 2012
5

6Database Schema - ERD

7
Data Cleaning/Recoding• We clean and recode the following fields
• Billing, Encounter and Problem List Diagnoses (ICD9)• Medications (ATC)• Lab results (LOINC)• Referrals (SNOMED CT)• Physical signs (Wt, Ht, BP, unit conversion, calculate
BMI)• Vaccines (ATC)• Risk factors (smoking, alcohol, diet --Text)

8Patient Demographics
} < 5%
} < 5%
368,000 Records368,000 Records

9
Provider Information

10
Billing
6.8 Million Records6.8 Million Records
Dates of EncounterDates of Encounter
Original diagnosis sent for billing
Original diagnosis sent for billing
Text from Code Recoded by CPCSSN
Text from Code Recoded by CPCSSN
Original Diagnosis Code sent for billing
Original Diagnosis Code sent for billing
Recoded by CPCSSNRecoded by CPCSSN

11
Research Discussion• Useful for case finding• Useful for understanding deficiencies of using
billing information for clinical research
• There is some inconsistency in use of billing codes across the country
• CPCSSN recodes all billing diagnosis codes to a standard version

12
Encounters
5.1 Million Records5.1 Million Records
Dates of EncounterDates of Encounter
Data inconsistent across the Country
Data inconsistent across the Country
CPCSSN Cleaning Not StartedCPCSSN Cleaning Not Started
Active area of CleaningE.g., Office Visit, Phone, E-mail etc
Active area of CleaningE.g., Office Visit, Phone, E-mail etc

13
Research Discussion• Can we segment patients by pattern of visits?• Does pattern of visits predict other things?
– Control of disease– Frequency of prescriptions– Multiple comorbidities
• Does visit type affect quality of care?
• Reason for Encounter is poorly captured in most EMRs

Problem List Diagnoses
14
Original Diagnosis Written by UserE.g. DMT2
Original Diagnosis Written by UserE.g. DMT2
Recoded by CPCSSNE.g., Diabetes Mellitus, Type 2
Recoded by CPCSSNE.g., Diabetes Mellitus, Type 2
} Not well populated
1.8 Million Records1.8 Million Records
Active = Problem ListInactive = Past Medical History
Active = Problem ListInactive = Past Medical History
Problem List Diagnoses
15
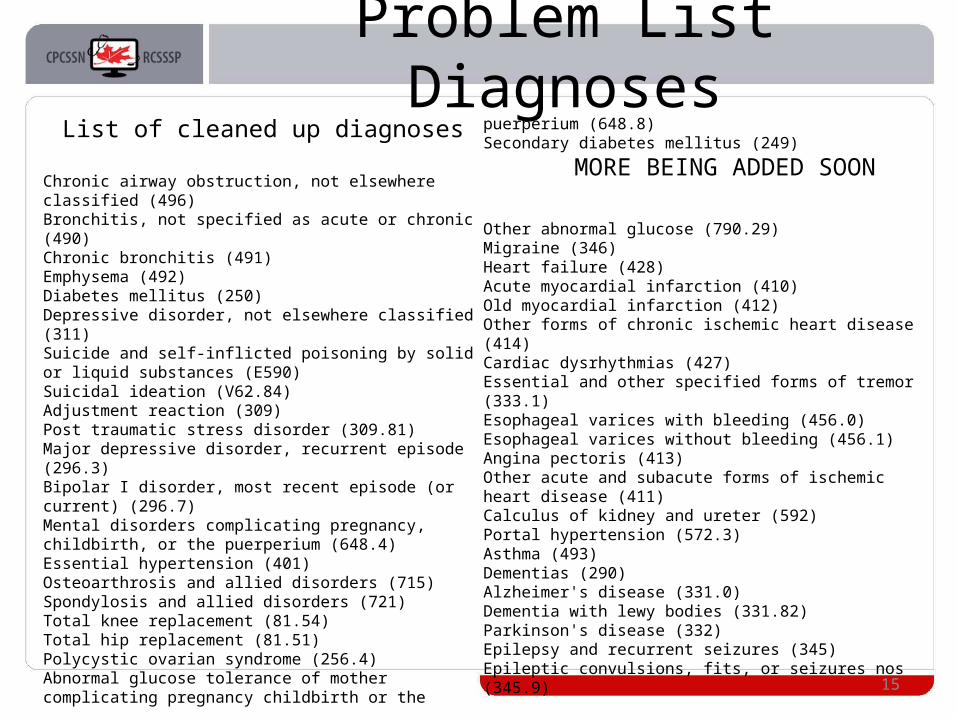
List of cleaned up diagnoses
Chronic airway obstruction, not elsewhere classified (496)Bronchitis, not specified as acute or chronic (490)Chronic bronchitis (491)Emphysema (492)Diabetes mellitus (250)Depressive disorder, not elsewhere classified (311)Suicide and self-inflicted poisoning by solid or liquid substances (E590)Suicidal ideation (V62.84) Adjustment reaction (309)Post traumatic stress disorder (309.81)Major depressive disorder, recurrent episode (296.3)Bipolar I disorder, most recent episode (or current) (296.7)Mental disorders complicating pregnancy, childbirth, or the puerperium (648.4)Essential hypertension (401)Osteoarthrosis and allied disorders (715)Spondylosis and allied disorders (721)Total knee replacement (81.54)Total hip replacement (81.51)Polycystic ovarian syndrome (256.4)Abnormal glucose tolerance of mother complicating pregnancy childbirth or the puerperium (648.8)Secondary diabetes mellitus (249)
MORE BEING ADDED SOON
Other abnormal glucose (790.29)Migraine (346)Heart failure (428)Acute myocardial infarction (410)Old myocardial infarction (412)Other forms of chronic ischemic heart disease (414)Cardiac dysrhythmias (427)Essential and other specified forms of tremor (333.1)Esophageal varices with bleeding (456.0)Esophageal varices without bleeding (456.1)Angina pectoris (413)Other acute and subacute forms of ischemic heart disease (411)Calculus of kidney and ureter (592)Portal hypertension (572.3)Asthma (493)Dementias (290)Alzheimer's disease (331.0)Dementia with lewy bodies (331.82)Parkinson's disease (332)Epilepsy and recurrent seizures (345)Epileptic convulsions, fits, or seizures nos (345.9)

16
Research Discussion• Sensitivity and specificity of problem list
diagnoses not currently known, so cannot determine incidence and prevalence of disease from problem list alone
• Need to develop case finding criteria for diseases (includes diagnosis, meds, labs, etc)
• Need to identify sensitivity and specificity of having a diagnosis in the problem list
• Currently in the process of validating 8 case finding criteria across the country

17
Vital Signs
Name of exam (e.g., sBP)Name of exam (e.g., sBP)
Cleaned up result(e.g, lbs -> kg, inch -> cm)
Cleaned up result(e.g, lbs -> kg, inch -> cm)
5 Million Records5 Million Records
Cleaned up unit of measure(e.g., unit is kg, but result was lb)
Cleaned up unit of measure(e.g., unit is kg, but result was lb)

18
Research Discussion• Currently have access to
– sBP/dBP– Ht– Wt– BMI– Waist circum

19
Allergies
Name of allergenName of allergen
Cleaned up nameCleaned up name
155K Records155K Records
Data will be coded as ATCData will be coded as ATC

20
Research Discussion• Not yet cleaned, but will soon clean it• Focus of cleaning will be on medication
allergies– All other allergies will be retained as original text
• Useful when assessing why patients are not receiving medications for a particular disease

21
Risk Factors
Name of Risk Factor (e.g., smoking)Name of Risk Factor (e.g., smoking)
Cleaned up version of Risk Factors.Cleaned up version of Risk Factors.
588K Records588K Records
Working on cleaning up Current Exposures & Cumulative Exposures
Working on cleaning up Current Exposures & Cumulative Exposures

22
Research Discussion• Risk factors are actively being cleaned
• Getting the status of the risk factor (i.e., smoker/non-smoker) is difficult, but easier than
• Current levels of exposure (e.g., # of cig/day)• Cumulative exposure (e.g., pack years)• Alcohol use is also being cleaned up
23
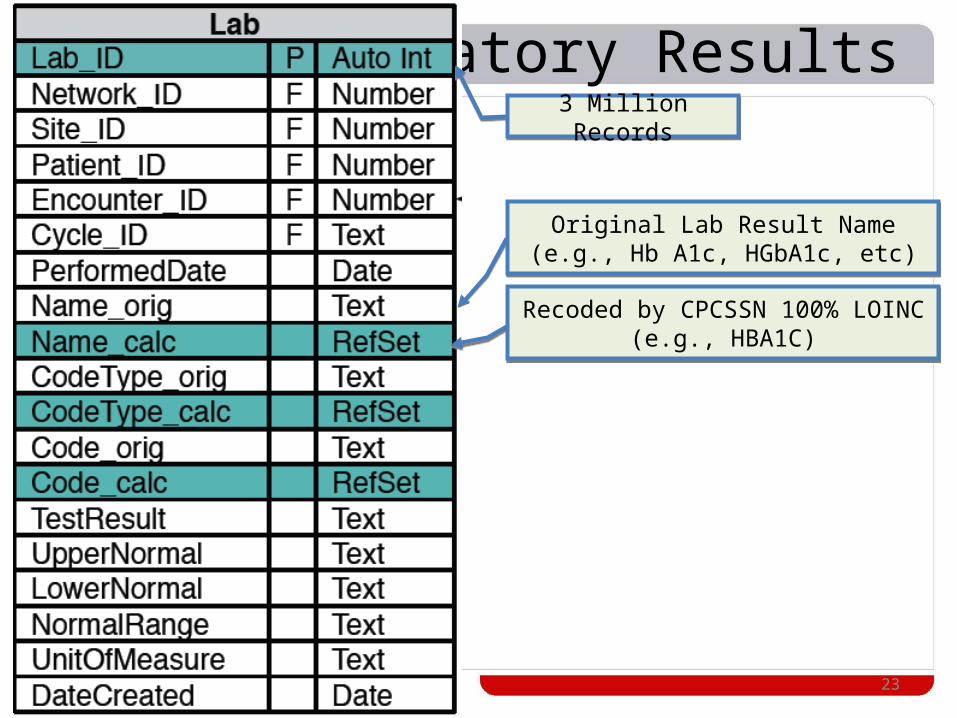
Laboratory Results
Original Lab Result Name(e.g., Hb A1c, HGbA1c, etc)Original Lab Result Name
(e.g., Hb A1c, HGbA1c, etc)
Recoded by CPCSSN 100% LOINC(e.g., HBA1C)
Recoded by CPCSSN 100% LOINC(e.g., HBA1C)
3 Million Records3 Million Records
24
Research Discussion• Currently only capturing the following
• One site does not capture labs yet
HDLTRIGLYCERIDESLDLTOTAL CHOLESTEROLFASTING GLUCOSEHBA1CURINE ALBUMIN CREATININE RATIOMICROALBUMINGLUCOSE TOLERANCE

25
Encounter Diagnoses
Original Diagnosis Recorded in Encounter(e.g., axniety)
Original Diagnosis Recorded in Encounter(e.g., axniety)
83% Recoded by CPCSSN(Anxiety ICD-9 300)
83% Recoded by CPCSSN(Anxiety ICD-9 300)
6.3 Million Records6.3 Million Records
63% Originally coded by Doctor63% Originally coded by Doctor

26
Research Discussion• Not all EMRs capture Encounter Diagnoses in a
structured manner
• This table is not ready for prime time across all sites, but may be useful for projects where data from just a few sites is acceptable

Medications
27
What the doctor orderedE.g., HCTZ 25 mg bid
What the doctor orderedE.g., HCTZ 25 mg bid
91% Recoded by CPCSSNE.g., Hydrochlorthiazide
91% Recoded by CPCSSNE.g., Hydrochlorthiazide
56% Coded as DIN56% Coded as DIN
Strength 56%Dose 70%
Unit of Measure 84%Frequency 95%Duration 52%
Dispensed 86%
Strength 56%Dose 70%
Unit of Measure 84%Frequency 95%Duration 52%
Dispensed 86%
72% Coded by doctor (DIN + other)72% Coded by doctor (DIN + other)
91% Coded by CPCSSN (ATC)91% Coded by CPCSSN (ATC)
4.9 Million Records4.9 Million Records
}

28
Research Discussion• Medication name data is relatively clean• Medications coded as ATC
– Allows easy grouping by class
• Don’t have daily dose and months supply for many records –working on clean up

29
Referrals
Original Text of ReferralOriginal Text of Referral
80% Recoded by CPCSSNSNOMED-CT
80% Recoded by CPCSSNSNOMED-CT
600 K Records600 K Records
30
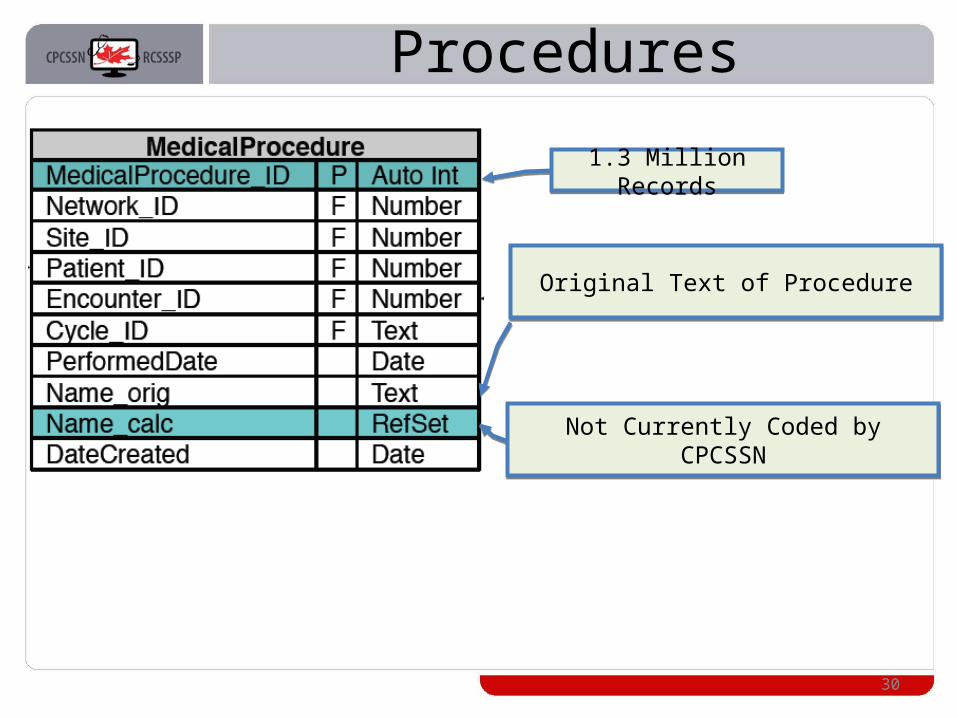
Procedures
Original Text of ProcedureOriginal Text of Procedure
Not Currently Coded by CPCSSNNot Currently Coded by CPCSSN
1.3 Million Records1.3 Million Records

31
Vaccines
What the doctor typedWhat the doctor typed
93% Recoded by CPCSSN (ATC)93% Recoded by CPCSSN (ATC)
960 K Records960 K Records
46% Coded by Doctor (DIN)46% Coded by Doctor (DIN)

32
Disease Cases
173,000 Records173,000 Records
Case Definitions are developed by CPCSSN and are in the process ofbeing validated through chart reviews
How a Case is identified is recorded in this table
Allows full traceability for each case
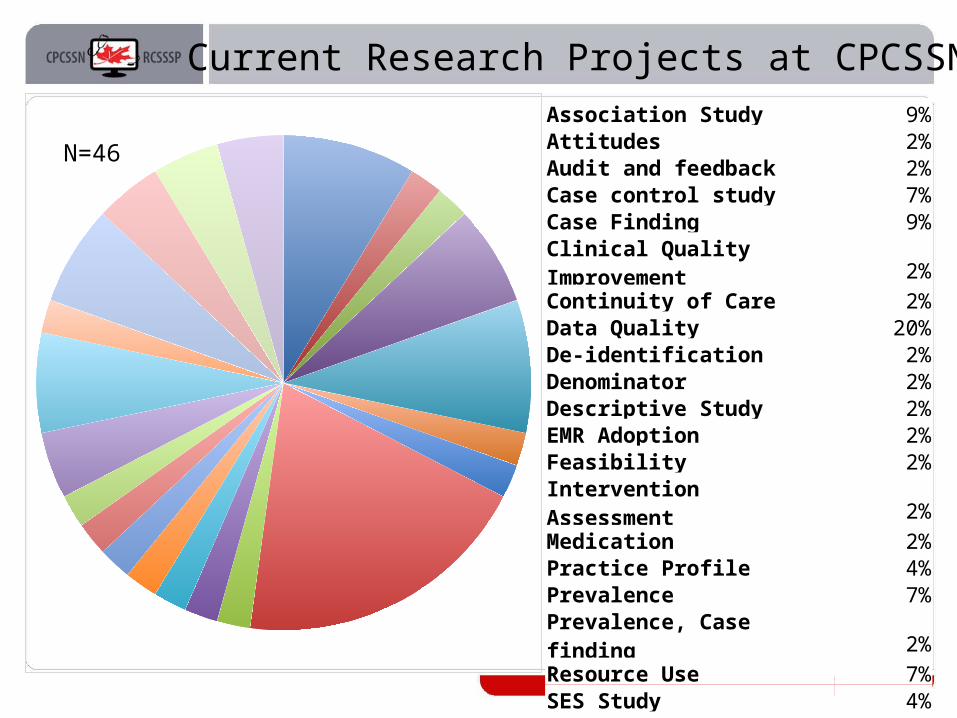
Current Research Projects at CPCSSN
N=46
Association Study 9%Attitudes 2%Audit and feedback 2%Case control study 7%Case Finding 9%Clinical Quality Improvement 2%Continuity of Care 2%Data Quality 20%De-identification 2%Denominator 2%Descriptive Study 2%EMR Adoption 2%Feasibility 2%Intervention Assessment 2%Medication 2%Practice Profile 4%Prevalence 7%Prevalence, Case finding 2%Resource Use 7%SES Study 4%Treatment pattern 4%Validation 4%

Research Opportunities• Population Health and Epidemiological Studies
– Incidence/Prevalence of disease– Impact of SES on health– Rates of treatment for diseases– Rates of disease control– Burden of illness and multi-morbidity
• Clinical –database studies– Comparative effectiveness– Case-Control– Exposure-Outcome– Quality Improvement– Associations– Intervention-Outcome– Guideline effectiveness
34

35
Research Opportunities• Clinical –prospective, interventional studies
– Conduct pragmatic RCTs –data is already collected– Conduct in-clinic interventions– Not ready for these yet
• Health Services– EMR adoption– Resource Utilization (consults, labs, procedures)– Policy Intervention (cross-province comparisons)– Patient behaviors –frequency of visits– Medical errors and patient safety

36
Research Opportunities• Health informatics
– Natural language processing– Machine learning– De-identification algorithms– Predictive Analytics
• eHealth and mHealth– Develop and test apps using CPCSSN data– Patient education apps with their own data– Apps for healthcare providers to educate patients
about their disease with nice visualizations

37
Research Using CPCSSN Data
ResearcherLetter of
Intent
CPCSSN Research
Committee
Writes
Letter of Intent
Reviews
1 page, includes: Researchers, Organization, Research Title,
Objective, Methodology, Data Required
Approved
1. Resubmit2. Not Feasible
3. Outside Mandate
No
Researcher
1. Protocol2. Data Access Request Form
3. Data Sharing Agreement
Letter of Acceptance Yes
Writes
CPCSSN Research
Committee
CPCSSN Data
ResearcherInvoice

38
Goodies For Today• Copy of the presentation: The Art of the Possible: Using CPCSSN
Data for Primary Care Research• Sample of CPCSSN data for 200 patients
– Anonymized and scrambled to protect patient privacy– (MS Access file format)
• CPCSSN database entity relationship diagram (ERD)• CPCSSN database data dictionary• CPCSSN central repository data holdings summary• CPCSSN Data Access Request Form Central Repository• Process for Requesting Access to CPCSSN Data

39
Next Steps• Sign a License Agreement today to get your copy of
the CPCSSN Data Product
• Evaluate the data CPCSSN has
• Plan your next grant application around CPCSSN data
• Add CPCSSN Data as a budget item into your next grant application– You can contact us to get a quote

40
Contact
Tyler Williamson, Senior Epidemiologist Canadian Primary Care Sentinel Surveillance Network
Centre for Studies in Primary CareQueen’s UniversityKingston ON K7L 5E9
Tel: (613) 533-9300, Ext. 73838Fax: (613) 533-9302e-mail: [email protected]


Thanks to all Funders, Stakeholders, Partners, AND sentinel Physicians
Cette publication a été réalisée grâce au financement de l'Agence de la santé publique du Canada. Les opinions exprimées ici ne reflètent pas nécessairement celles de l'Agence de la santé publique du Canada.
Funding for this publication was provided by the Public Health Agency of Canada The views expressed herein do not necessarily represent the views of the Public Health Agency of Canada.





























