Embed Size (px)
Citation preview
The authors have no financial interest in the subject matter of this poster
Mohit Jain MD, Anita Panda MD, Murugesan Vanathi MD, Sudarshan Khokhar MD, Tanuj Dada MD
Topical Application of Autologous Platelet-Rich Plasma for Acute Ocular Chemical Burn
Dr Rajendra Prasad Centre for Ophthalmic SciencesAll India Institute of Medical Sciences, New Delhi, India

Introduction
Biological agents like autologous serum, umbilical cord serum have been used for restoration of ocular surface and control of inflammatory process owing to presence of significant concentrations of growth factors 1,2
Autologus PRP contain 5 t0 6 times higher concentration of growth factors 3 which are constantly released from α granules present in plateletsBefore activation
After activation
Platelets remain viable for 3-4 days
Has a lubricating property
Starts coagulation process and provides
fibrin scaffold
Contains 3- 4 times more platelets
Topical PRP is used in ocular surface disorder following LASIK, dry eye and dormant corneal ulcers1,2,3,4,5
Clinically used among musculoskeletal physicians, orthopedic surgeons, maxillofacial and plastic surgeons and dermatologists

Aim of the study Comparative evaluation of topical autologous PRP given
along with standard medical treatment with standard medical treatment alone in acute ocular chemical burns
Materials and methodsRandomized prospective comparative double blind case control study
The study population was recruited from a university-based cornea clinic and ophthalmology emergency department
Institutional Ethical Committee approval was sought and written informed consent was taken from participants
Inclusion criteria: Patients with grade III, IV & V ocular chemical injury Patients presenting within 3 days of injury
Exclusion criteria: Patients with impending perforation /perforated cornea
Materials and Methods
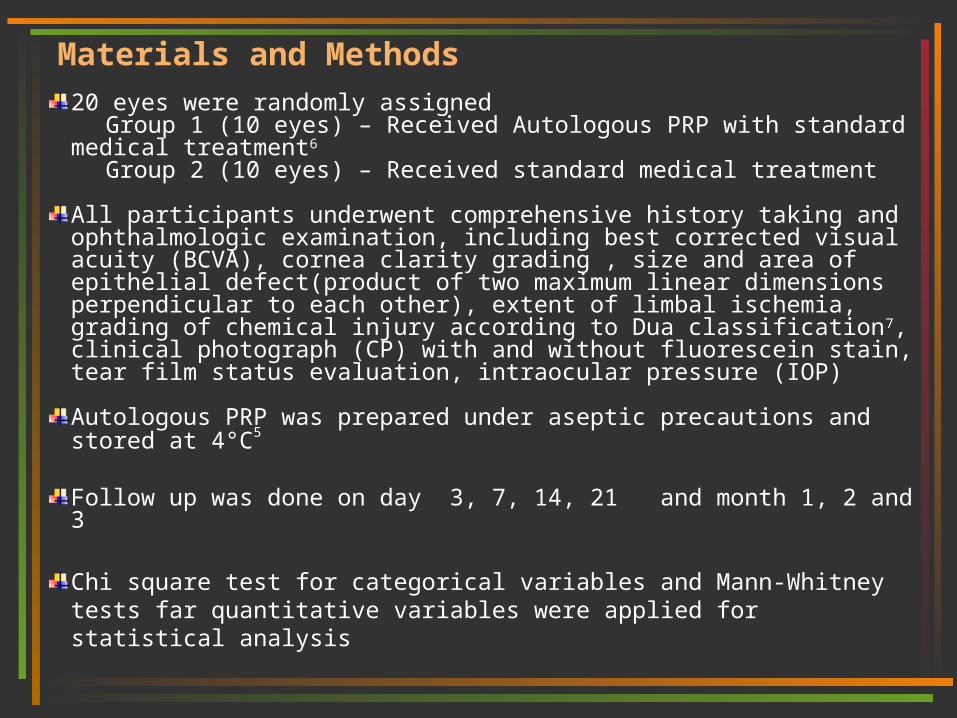
20 eyes were randomly assigned Group 1 (10 eyes) – Received Autologous PRP with standard
medical treatment6
Group 2 (10 eyes) – Received standard medical treatment
All participants underwent comprehensive history taking and ophthalmologic examination, including best corrected visual acuity (BCVA), cornea clarity grading , size and area of epithelial defect(product of two maximum linear dimensions perpendicular to each other), extent of limbal ischemia, grading of chemical injury according to Dua classification7, clinical photograph (CP) with and without fluorescein stain, tear film status evaluation, intraocular pressure (IOP)
Autologous PRP was prepared under aseptic precautions and stored at 4°C5
Follow up was done on day 3, 7, 14, 21 and month 1, 2 and 3
Chi square test for categorical variables and Mann-Whitney tests far quantitative variables were applied for statistical analysis

Table 1: Demographic data of Participants
Group 1 (Mean)
Group 2 (Mean)
P-VALUE
AGE(years)* 31.5 39.6 0.12
DURATION BETWEEM EXPOSURE AND RPC TREATMENT (days)*
2.2 2.1 0.8
CORNEA CLARITY# 2.7 2.4 0.624
LARGEST EPITHELIAL DEFECT DIMENSION(mm) #
7.65 6.44 0.435
EPITHELIAL DEFECT AREA(mm2) #
54.31 42.06 0.37
LIMBAL ISCHEMIA(clock hours)#
6.8 6.5 0.96
BCVA(log MAR)# 1.06 1.09 0.73
* Independent t test# Wilcoxon rank-sum (Mann-Whitney) test
Graph 1 Nature of chemical
No.
of
part
icip
an
ts

D0 D3 D7 D14 D21 M1 M2 M3
Group 1*
7.65±2.29,7.7(4.5-11)
4.80±2.82,3.35(1.8-10)
2.69±3.15,1.4(0.0-8.5)
1.16±1.31, 0.65(0-3.30)
0.53±0.72,0(0-1.8)
0.34±0.53,0 (0-1.4)
0.08±0.17,0(0-0.5)
0.0±0.0
Group 2*
6.44±3.58,6.25(1.3-11)
5.25±3.39,4.15(1.8-10.5)
5.06±3.64,3.65(2.5-11)
3.98±3.69,2.8(0-10.7)
2.98±4.02,1.5(0-10.8)
1.85±3.53,0(0-9.8)
0.90±1.91,0(0- 0.5)
0.0±0.0
P value 0.44 0.79 0.05 0.03 0.04 0.7 0.82 1
Table 2: Mean epithelial defect diameter (EDD) resolution
*EDD - Mean±SD, median(range) (mm)
Mean
ED
D
(mm
)
Time →
%ag
e d
ecre
ase
in
ED
D
Time →
Graph 2: Mean EDDGraph 3: % decrease in EDD

D0 D3 D7 D14 D21 M1 M2 M3
Group 1*
54.31±33.21,51.97(14.40-107.08)
25.79±31.74,8.04(1.26-88)
13.79±24.83,7(0-64.60)
1.69±2.67,0.21(0-6.93)
0.28±0.41,0(0-1`.26)
0.09±0.16,0(0-0.42)
0.21±0.4,0(0-0.15)
0-0(0-0)
Group 2*
42.06±44.53,25.55(.56-112)
32.63±39.31,13.52(1.62-100)
35.53±45.1613.78(5.25-111.60)
23.79±39.43,5.6(0-100.58)
20.82±41.23,1.43(0-104.76)
13.05±29.04,0(0-86.24)
0.08±170(0-0.50)
0-0(0-0)
P value
0.3 0.8 .02 .02 .01 0.69 0.82
Table 3: Mean epithelial defect area (EDA) progressionM
ean
ED
A
mm
2
Time →
The mean time to complete epithelialisation was 40±31.57 ,25.5 (7 to 90)days and47 ±26.15,30.0( 21 to 90) days,in group 1 and group 2 respectively . The difference was not statistically significant. (p=0.29) For grade 3 injuries mean time to complete epithelialisation was significantly less14 ± 7 ,14(7 to 21)days in group 1 compared to and 28.5 ±3.67,28.5(21 to 30)days in group 2. p value(0.006)
EDA - Mean±SD, median(range) (mm2)
Graph 4: Mean EDA
Corneaclarity
Group 1 Group 2
Total
1 1 2 3
2 4 4 08
3 4 4 08
4 1 0 1
Total 10 10 20
Corneaclarity
Group 1
Group 2
Total
1 1 4 5
2 1 3 4
3 3 1 4
4 5 2 7
Total 10 10 20
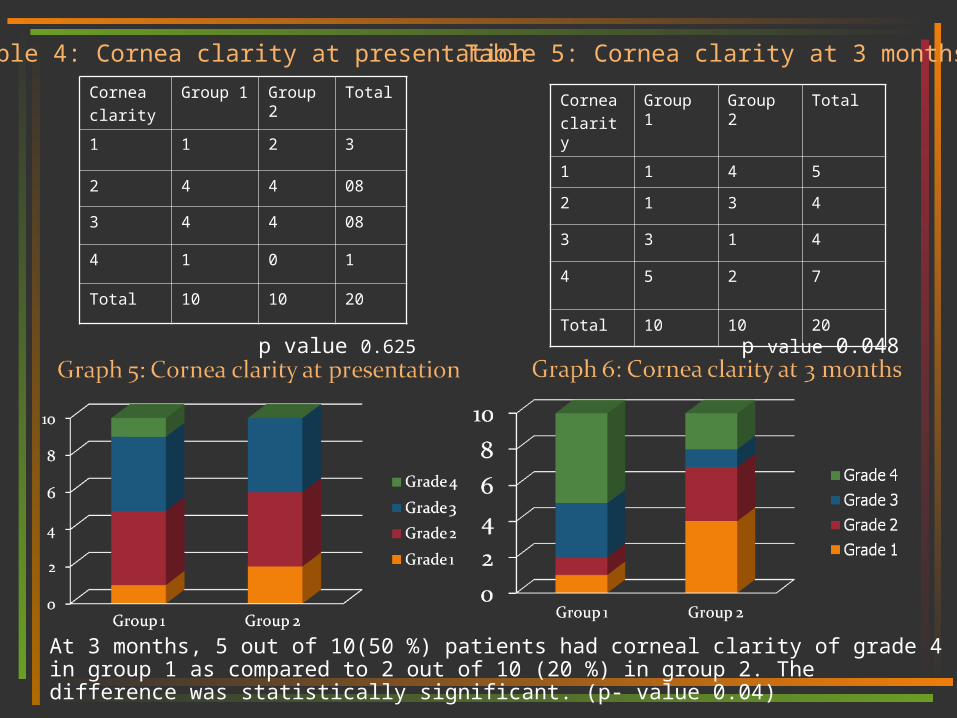
Table 4: Cornea clarity at presentation Table 5: Cornea clarity at 3 months
p value 0.048p value 0.625
At 3 months, 5 out of 10(50 %) patients had corneal clarity of grade 4 in group 1 as compared to 2 out of 10 (20 %) in group 2. The difference was statistically significant. (p- value 0.04)

Table 7: Complications
Complications Group 1
Group 2 P
value*
Increased intraocular pressure
3 4 0.9
Infiltrate 1 1 1
perforation 0 0 0
symblepheron 3 5 0.65
Entropion and ectropion 2 2 1
* Fisher exact test
[Mean±SD, median (range)]
BCVA at presentation BCVA at 3 months % improvement in BCVA
Group 1 1.06 ±18,1.0(.70-1.30) 0.66 ± .60,40(0.2-2.0) 33.64 ± 55.75,55.49(-80 to 100)
Group 2 1.09 ± 20,1.0(.70-1.30) 0.93 ± 0.35,0.85(0.30-1.30)
37.74 ± 9.66,36.70(-20 to 50)
p 0.73 0.07 .082
Table 6: BCVA

MONTH 1
DAY 14
DAY 7
GROUP 2
GROUP 1
MONTH 2 and 3
DAY 0

Addition of topical autologous PRP to standard treatment protocol helps in rapid re-epithelialisation of ocular surface and achieve better corneal clarity
There is a trend towards achieving better BCVA with addition of topical autologous PRP at 3 months (though not statistically significant)
We recommend use of topical autologous PRP therapy along with standard medical treatment in cases of ocular chemical injuries of grade3 , grade4 and grade5
Studies with larger sample size and longer follow up periods are required
Conclusions

References
1. Poon AC et al. Autologous serum eyedrops for dry eyes and epithelial defects: clinical and in vitro toxicity studies. Br J Ophthalmol. 2001 Oct; 85(10): 1188-97
2. Singh G et al. Epidermal growth factor in alkali burned corneal epithelial wound healing. Am J Ophthalmol. 1987 June; 103(6): 802-7
3. Alio JL et al. A Symptomatic dry eye treatment with autologous platelet-rich plasma. Ophthalmic Res. 2007 Mar; 39(3): 124-9
4. Alio JL et al. Use of autologous platelet-rich plasma in the treatment of dormant corneal ulcers. Ophthalmology. 2007 Jul; 114(7): 1286-1293
5. Alio JL et al. Treatment of ocular surface syndrome after LASIK with autologous platelet-rich plasma. J Refract Surg. 2007 Jun; 23(6): 617-9
6. Brodovsky SC et al. Management of alkali burns: 11 year retrospective review. Ophthalmology. 2000 Oct; 107(10): 1829-35
7. Dua HS et al. A new classification of ocular surface burns. Br J Ophthalmol. 2001 Nov; 85(11): 1379-83
AcknowledgementsDr. T. Velpandian Associate Professor, Dept. of Ocular Pharmacology,AIIMSMr. Pankaj Gupta Dept. of Ocular Pharmacology,AIIMSDr. Manik Goel, MDDr. Amit Sobti, MDDr .Twinkle Parmar, MD
























![[2012] 13 S.C.R. 1 2 MURUGESAN AND ORS. A STATE THROUGH](https://img.pdfslide.net/doc/110x75/61c465b1c2f87c1f69106fc4/2012-13-scr-1-2-murugesan-and-ors-a-state-through-.jpg)