Embed Size (px)
Citation preview

Aneurysm treatment redefinedAneurysm treatment redefined
The cerebrovascular program at the The cerebrovascular program at the Oregon Oregon Neurosciences Neurosciences InstituteInstitute
By Erik Hauck, MD, PhD; Medical Director

ObjectivesObjectives
• Natural history of aneurysms
• Standard treatment for aneurysms
• Advanced treatment for giant aneurysms
• Dealing with complications of SAH:
- Hydrocephalus
- Ischemia
• Watch real-time surgery
• Case discussion
Dr. Hauck patient iphone.wmv

Aneurysms & Evolution in medicineAneurysms & Evolution in medicine400 BC400 BC Hippocrates: Apoplexy
1658 Wepfer: Ischemia vs Hemorrhage
1664 Willis: Circle of Willis
1765 Biumi: First clear description
1885 Horsley: Carotid Ligation for AN
1891 Quincke: LP - SAH
1927 Moniz: Cerebral angio
1931 Dott: Wrap
1937 Dandy: Clip
1966 Pool: Microscope
1991 Guglielmi: Coil
1997 Higashida: Stent

Dandy’s Dandy’s
sketchsketch
of the first of the first
Aneurysm Aneurysm
Clip 1937Clip 1937

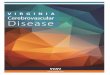
Incidence of stroke in the USIncidence of stroke in the US
Aneurysms:

(GCNKSS: 1993-94 and 1999). Source: Stroke 2006;37;2473-2478.
206
247
42
11
44
11
156
181
226 219
0
50
100
150
200
250
Ischemic Intracerebral
hemorrhage
Subarachnoid
hemorrhage
Inc
ide
nc
e p
er
10
0,0
00
White '93-94 White '99 Black '93-94 Black '99
Incidence of stroke in the USIncidence of stroke in the US
Relevance

Year #1 Summary: 467 proceduresYear #1 Summary: 467 procedures
• Craniotomies 69 aneurysm (tumor) 2323 (11)
AVM 77
EC-IC bypass 3
Gamma Knife 5
• Cath proc 274 aneurysm 2626
AVM 1010
Stroke acute/delayed 12/17
dx angio 186
• Carotid proc 22 CEA 8
CAS (inc. 11 AN) 14
• CSF Shunting 42
• Spine 67 AVM (tumor) 33 (3)
50 aneurysms50 aneurysms

Year 1, 50 aneurysmsYear 1, 50 aneurysms
• 40 Patients treated (1.2 AN/pt)– 20 ruptured (50%), 2 pt had add. unrupt. ANs
treated
– 20 unruptured (50%)
• 49 intra-cranial Aneurysms treated (49 proc)– 26 coil (5 stent/coil) [55.3%]
– staged x 2 patients, 2 aneurysm per session x 2
– 23 crani [46.9%]
• 1 extra-cranial Aneurysm treated (1 proc)

Lane County (n=351,715 in 2010)Lane County (n=351,715 in 2010)

Prevalence of aneurysmsPrevalence of aneurysms
• ~ 3% in the US population

Prevalence of aneurysmsPrevalence of aneurysms
• ~ 3% in the US population
• 10.551 people in Lane county

Prevalence of aneurysmsPrevalence of aneurysms
• ~ 3% in the US population
• 10.551 people in Lane county
• 6 people here now

SizeSize
Small & Giant

LocationLocation
Brisman JL, Song JK, Newell DW. Cerebral aneurysms. NEJM 2006; 355:928-939

Risk of Rupture (ISUIA)
ISUIA. Lancet. 2003 Jul 12;362(9378):103-10.
Size Anterior Circulation Posterior Circulation
0 - 6 0 – 1.5% 2.5 – 3.4%
7 – 12 2.6% 14.5%
13 - 24 14.5% 18.4%
25+ 40% 50%
5 year cumulative risk

Average size for ruptured ANAverage size for ruptured AN
• 7.5 mm (n= 161) J Neurosurg. 1987 Jan;66(1):23-9.
• 7.1 mm (n=64) Neurosurgery. 2011 Feb 4.
• 6.28 mm (n=889) J Kor Neurosur Soc. 2009;45(2):85-89.
6 6 –– 7 mm7 mm

Outcome after ruptureOutcome after rupture
• Mortality 33% Inhouse. J Neurosurg.2003;99:810–817.
• Mortality 45% (30 days). Stroke. 1994;25:1342–1347.
• Mortality 50% (29 days). Practical Applications. 1969.
Mortality of rupture ~ 40%Mortality of rupture ~ 40%Quoted after the American Stroke Association, Guidelines for SAH, 2009

Treatment Goals
Introduction
~ Prevent Rupture
~ Prevent Spasm
~ Prevent Stroke
~ Treat ICP
~ Treat HCP
~ Ensure Functional
Survival

Treatment Option
• Endovascular (needle puncture in the groin)
• Surgery

The The cerebrovascularcerebrovascular teamteam
MD Erik Hauck, MD
PA Nicole Wydra, PA
Clinic nurse Rosemary Parnell, RN
Clinic organizer Debi Steinbrenner
Clinic Manager Michele Daniels, RN (OHVI)

The The cerebrovascularcerebrovascular familyfamily
Hauck,Hauck,CerebrovascularCerebrovascular
Neurosurgery Neurosurgery &Interventional &Interventional
RadiologyRadiology
Gallo, NSIGallo, NSI
Kokkino, ONSKokkino, ONSThompson, IRThompson, IR
KeiperKeiper, SBC, SBC
Englander, Englander, NeurologyNeurology
Lippincott, Lippincott, NeurologyNeurology
Skalabrin, Skalabrin, NeurohospitalistNeurohospitalist
Rughani, Rughani, IntensivistIntensivist
Littell, Littell, HospitalistHospitalist
Jill Jill HoggardHoggard--GreenGreen, ,
PeaceHealthPeaceHealth
Young, EDYoung, ED
Duke, CT Duke, CT surgerysurgery
DeHaas,DeHaas,Vascular SurgeryVascular Surgery
Padgett, Padgett, CardiologyCardiology

NeuroNeuro--biplane Room, Smart ORsbiplane Room, Smart ORs

DSA R VADSA R VA• 58 yo man
• TIA with LOC / confusion
• Complete recovery
• HTN

R R PteryonalPteryonal ApproachApproach

- No deficit
- D/c POD #3

# Sex Age Size Side TAO IOAR 3rd nerve paresis f/u LOS comp symptom GOS
[mm] [min] temporary permanent [months] [days]
1 F 29 5 R 14 no Yes no 12 3 - - 5
2 F 37 3 R none no No no 1 6 - - 5
3 M 38 4.4 L 20 no No no 6 5 - - 5
4 F 42 6 R 10 no No no 1 4 - - 5
5 F 45 4.2 R 11 no No no 6 5 - - 5
6 F 46 3.3 R 2 no Yes no 12 3 small ICH - 5
7 F 48 5 L 9 no No no 12 4 - - 5
8 F 50 3.8 R none no No no 24 6 post op ileus resolved 5
9 F 51 6 R 11 no No no 2 4 - - 5
10 F 52 2 R none no No no 12 4 - - 5
11 M 52 2.5 L 5 no Yes no 12 4
4th nerve
palsy
intermittent double
vision 4
12 F 54 5 R none no No no 6 4 - - 5
13 F 55 4 R none no No no 12 5 -
unchanged minor
preoperative
disability 4
14 F 55 2.6 R 7 no Yes no 1 5 -
overall 'less energy' as
prior to surgery 4
15 F 63 6 R 8 no No no 12 5 - - 5
16 F 65 5 R 10 no Yes no 12 4 -
unchanged minor
preoperative
disability 4
17 M 65 4 R 8 no No no 2 4 - - 5
18 F 70 3 L 8 yes Yes no 2 5 small infarct
temporary weakness,
completely
resolved 5
19 F 70 6 R 8 no Yes no 12 5 - - 5
20 F 71 4.5 R 5 yes Yes no 12 7 - - 5
21 F 74 5.1 L none no No no 24 4 - - 5
ClipClip

Larger basilar apexLarger basilar apexAneurysm,Aneurysm,Stent/CoilStent/Coil

Small Aneurysm, Small Aneurysm, ClipClip

Multiple aneurysms Multiple aneurysms 48 F, ruptured a-com

Giant aneurysmsGiant aneurysms

DirectDirectclippingclipping

‘Saccular’(based on a ‘normal’ parent vessel)

‘Fusiform’(no ‘normal’ parent vessel)
Drake CG, PeerlessSJ. Giant fusiform intracranial aneurysms:
review of 120 patients treated surgically from 1965 to 1992. J
Neurosurg. 1997 Aug;87(2):141-62.

Giant Aneurysm, ClipGiant Aneurysm, Clip
36 mm

Carotid ligationCarotid ligation
26 yo M, L eye blind, 3.1 cm AN

TraditionalTraditionalBypassBypass--InterpositionInterposition

Low Low –– flow bypass, STA flow bypass, STA -- MCAMCA

HarvestingHarvesting
the the
graftgraft

Opening the DuraOpening the Dura

Exposing the Exposing the recipientrecipient

Custom fittingCustom fitting

Starting the Starting the anastomosisanastomosis

StitchingStitching

Bypass techniqueBypass technique

Inspection of the final resultInspection of the final result

Post op Post op angioangio & safety pin& safety pin

ELANA ELANA Technique Technique –– high flow high flow graftgraft

ELANA ELANA ‘High flow bypass’‘High flow bypass’

Direct Direct coilingcoiling

Waffle Cone Technique
Please, avoid the ‘leaky cherry’ !

Pipeline Pipeline EmbolizationEmbolization DeviceDevice
- Braided mash cylinder
- 48 microfilaments
- platinum and cobalt chromium strands
- mounted on a flexible microwire

Carotid cavernous giant aneurysmCarotid cavernous giant aneurysmPRE PRE –– POST POST
a/p view

Treating complications of SAHTreating complications of SAH
Vasospasm
• medical management
• surgical treatment of ICP & HCP
• interventional treatment

Treating complications of SAHTreating complications of SAH
Hydrocephalus
• lumbar drain
• ventric
• shunt
• endoscopy

Real time brain endoscopyReal time brain endoscopy

Detailed CASE PresentationDetailed CASE Presentation
02668138

Clinical backgroundClinical background
• Young mother with a 7 months old baby boy
• Bad H/A, N/V, lethargy, but fully oriented
• Hx of migraines
• Left homonymous hemianopsia

CT on admission

MR on admission

VA AngiogramVA Angiogram

R & L CCA AngiogramR & L CCA Angiogram

FindingsFindings
• R occipital AVM, 61 mm largest diameter
• Deep venous drainage
• Eloquent brain
• No clear feeding artery aneurysms
• Spetzler-Martin Grade V AVM
• Intraparenchymal / intraventricularhemorrhage
• Large Venous Varix (Venous aneurysm)

Treatment PlanTreatment Plan
• Preoperative embolization in 1 or 2 stages
• Surgical resection of the AVM after sufficient embolization
• Patient was awaiting treatment the following day

Catastrophic eventCatastrophic event
• I am at home, ‘not’ on call
• Around midnight, the phone rings
• The pt, while talking to the nurse, turned over and became unresponsive, comatose, the nurse reports: “the right pupil does not respond to light, she is barely breathing”
• The pt is sent for a CT and requires intubation
• I rush to the hospital within minutes

New CTNew CT

Emergent ventric immediately after CT

Clinical courseClinical course
• The patient is in a deep coma in near death condition
• The patient is prepared for emergent embolization and emergency surgery
• Then, the fixed pupil on the right side starts to react
• The intracranial pressure is high normal

Pre & Post Pre & Post emoblizationemoblization, single shot, single shot

Then to the OR…Then to the OR…
• Hours under the microscope …
• Then back to the cath-lab …

Post op Post op angioangio: Complete resection: Complete resection

Hospital courseHospital course
• Patient made slow improvements (such as little movements here and there)
• Was eventually weaned from the ventilator
• Was eventually transferred to rehab
• Followed up with me in the office after 2 months

II--phone video taken in the officephone video taken in the office(2 months follow(2 months follow--up)up)

THANKS!!!THANKS!!!

Thanks !!!Thanks !!!

mRS baselinemRS dischargemRS 3 monthsmRS 6 monthsmRS 12 months
Mean f/u time 6.4 ± 4.9 months
FollowFollow--upup





Aneurysms: Eugene Aneurysms: Eugene vsvs the worldthe world
..

1 year Disability & Death (1 year Disability & Death (mRSmRS > 2)> 2)
• All patients (n=40): 6/40 15% [2.5%/12.5%]
• Unruptured (n=20): 1/20 5% [ 5% / 0% ]– ISUIA data (n= 2368): 7.1% - 13.7% [ 7.2% - 12% / 0% - 2.7%]
• Ruptured (n=20): 6/20 30% [ 5% / 25% ]- ISAT data (n= 1594): 23.7% - 30.6% [ 18.2 – 20.6% / 8.1% - 10.1%]

SAH: Eugene SAH: Eugene vsvs ISATISAT
Eugene ISAT
SAH grade I – III 11 / 20 (55%) 1611 / 1736 (92.8%)
SAH grade IV & V 9 / 20 (45%) 125 / 1736 (7.2%)
Eugene SAH patients presented in the worst possible condition with the worst prognosis 6.2 x
more often than included ISAT patients


IschemicIschemicStrokeStroke