Embed Size (px)
Citation preview

European Journal of Obstetrics & Gynecology and Reproductive Biology 170 (2013) 497–500
The clinical significance of small endometrial polyps
Yaron Hamani a,*, Ido Eldar a, Hen Y. Sela b, Ernst Voss a, Ronit Haimov-Kochman a
a Division of Obstetrics and Gynecology, Hadassah Hebrew University Medical Centers, Mt. Scopus, Jerusalem, Israelb Division of Obstetrics and Gynecology, Hadassah Hebrew University Medical Centers, Ein Kerem, Jerusalem, Israel
A R T I C L E I N F O
Article history:
Received 17 August 2012
Received in revised form 19 May 2013
Accepted 5 July 2013
Keywords:
Endometrial polyps
Abnormal uterine bleeding
Hysteroscopy
A B S T R A C T
Objective: Small endometrial polyps are relatively common in asymptomatic women and may regress
spontaneously. In symptomatic women, the finding of a small polyp (<1 cm diameter) raises the
question of the clinical pertinence and necessity of excision. Sparse data are available on the
effectiveness of hysteroscopic excision of small polyps to manage abnormal uterine bleeding. The aim of
this study was to assess outcome after hysteroscopic excision of small endometrial polyps in
symptomatic patients.
Study design: This was an observational cohort study enrolling 255 premenopausal women presenting
with abnormal uterine bleeding and a small endometrial polyp on office hysteroscopy, undertaken
between January 2004 and February 2007. The study group was referred for polypectomy by operative
hysteroscopy. The outcome of the procedure was reviewed 6–12 months later by a telephone interview
to assess the pattern of uterine bleeding after the procedure and overall satisfaction.
Results: Significant improvement in the magnitude of bleeding was experienced by 70% of participants,
but only 30% of them reported return to regular menses. Satisfaction with the procedure was reported by
80%. Younger patients reported a less favorable bleeding pattern and were found to be less satisfied with
the outcome of the procedure.
Conclusions: Symptomatic women with small endometrial polyps can be treated safely and efficiently
with hysteroscopic excision. In the younger age group of patients, however, the outcome of the
procedure may be less favorable and may necessitate the addition of endometrial ablation to improve
outcome and increase patient satisfaction.
� 2013 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
European Journal of Obstetrics & Gynecology andReproductive Biology
jou r nal h o mep ag e: w ww .e lsev ier . co m / loc ate /e jo g rb
1. Introduction
Endometrial polyps are localized overgrowths of endometrialtissue containing glands, stroma and blood vessels, covered withepithelium [1]. The prevalence of endometrial polyps dependsupon the population being studied and the uterine imagingtechnique. Using saline infusion sonohysterography, endometrialpolyps could be found in 10% of asymptomatic premenopausalwomen older than 30 [2]. Polyps occur in all age groups but aremost commonly found in women aged 40–49 years [3]. Notably,some polyps, particularly the smaller ones (<1 cm) in asymptom-atic premenopausal women appear to regress spontaneously[4,5]. Polyps may be an incidental asymptomatic finding onroutine scanning, but they may also be associated with abnormaluterine bleeding in both pre- and postmenopausal women. Their
* Corresponding author at: Department of Obstetrics and Gynecology, The
Division of Obstetrics, Reproductive Endocrinology and Gynecologic Surgery,
Hebrew University Medical Center, Hadassah Mt. Scopus, P.O.B. 24035, Jerusalem
91240, Israel. Tel.: +972 2 584 4111; fax: +972 2 581 4210.
E-mail address: [email protected] (Y. Hamani).
0301-2115/$ – see front matter � 2013 Elsevier Ireland Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.ejogrb.2013.07.011
prevalence ranges from 20% in symptomatic premenopausalwomen up to 40% [6,7] in the postmenopausal period.
Abnormal uterine bleeding (AUB) has a significant deleteriouseffect on the quality of life of women. It is one of the most commonreasons cited by women attending gynecology outpatient clinics[8]. It is believed that the severity of the bleeding symptoms ofendometrial polyps depends on the size of the polyp [4].
In the past, patients often underwent hysterectomy to haltsevere bleeding, but today improvement in endoscopic diagnosishas led to more individualized management. Hysteroscopicpolypectomy has been considered effective in treating menorrha-gia and menometrorrhagia. While earlier studies have investigatedsmall polyps, they did not specifically address the question of theeffect of small polyp removal on bleeding patterns or quality of life[9–12], rather focusing on malignant potential or fertility out-comes. In these patients the bleeding disorder may be related toendometrial polyps, but could be dysfunctional endocrinologicaluterine bleeding with relative hyperestrogenic status. The aim ofthis study was to assess outcome after hysteroscopic excision ofsmall endometrial polyps in patients with abnormal uterinebleeding.

Y. Hamani et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 170 (2013) 497–500498
2. Materials and methods
2.1. Study population
This was an observational cohort study, conducted fromJanuary 2004 to February 2007. The study group (n = 255) includedpremenopausal women complaining of menorrhagia who werediagnosed with a single small endometrial polyp (<1 cm) whounderwent hysteroscopic polypectomy. Menorrhagia was definedas use of more than 5 pads a day or prolonged menstruation ofmore than 7 days by patient report. Prior medical treatment withprogestins or estrogen–progesterone preparations to regulatebleeding was recorded. Informed consent for the procedure wasobtained from all subjects. The diagnosis of a small endometrialpolyp was made pre-operatively by transvaginal ultrasonography(TVUS) and confirmed qualitatively during diagnostic hysterosco-py by experienced operators. Patients with adenomyosis ordiffused thick endometrium were not enrolled in the study group.Final diagnosis of endometrial polyp was obtained by histologicalexamination. Diagnostic hysteroscopy was not performed in 8patients because of either patient intolerance or technicaldifficulty. Excluded from the study group were women found tohave submucosal uterine leiomyomas (9 patients) more than onepolyp or diffuse thickened endometrium (16 patients), adeno-myosis (2 patients), or pathologic findings of endometrialhyperplasia or carcinoma (2 patients).
2.2. Measurements
The operative hysteroscopic procedures were performed witheither a monopolar (Storz, Germany) (69 patients) or a bipolarsystem (Gynecare, USA) (186 patients). The procedures werecarried out in a university teaching hospital setting by aprofessional team including two senior physicians and threephysicians in training under supervision.
The following parameters were recorded for each subject: age,parity, weight, duration of symptoms, pre-procedure hemoglobinlevel, duration of the procedure and the time elapsed since theprocedure. A telephone interview was obtained by a single non-physician, highly-trained interviewer, six to twelve monthsfollowing the procedure (Fig. 1).
Two hundred and twenty-nine women (89.8%) agreed torespond to the telephone questionnaire in the second stage ofthe study. This time-frame was chosen to provide optimalperspective on the procedure with the least recall bias. Thefollowing data were obtained from the telephone questionnaire:pattern of bleeding before and after the procedure, hysteroscopiccomplications, and overall satisfaction from the procedure. The
Total cases r eviewedn = 284
Isolated sm all polypsn = 255
Responded t o telephone interviewn = 229
Exclusions (n=29 ):Sub mucos al uterine leiomyomas , n= 9 more than o ne polyp or di ffuse thickened endometrium, n=16adenomyo sis , n=2pathologic fi ndings of end ome trial hype rplasia or carcinoma , n= 2
Lost to foll ow-upn = 26
Fig. 1. Collection of cases, exclusions, and losses to follow-up.
main outcome measure was the effect of the procedure onabnormal uterine bleeding. The secondary outcome was patientsatisfaction up to one year post-procedure. The participants wereasked to grade change in menstrual pattern on a scale of 1–4: 1: noimprovement; 2: slight improvement; 3: significant improvement;and 4: return to normal cycle. For analysis purposes grades 1–2 and3–4 were merged into two groups, failed and effective. Patientsrated their satisfaction: 1: not satisfied; 2: somewhat satisfied; 3:satisfied; and 4: highly satisfied. Again, for statistical analysissatisfaction level was grouped into unsatisfied (1–2) and satisfied(3–4).
2.3. Statistical analysis
We used Chi-square or Wilcoxon test, as appropriate, tocompare the characteristics for the dichotomies effectiveness andsatisfaction with treatment. Two logistic regression models wereperformed. Effectiveness and procedure satisfaction served asdependent variables and age, weight, parity, hemoglobin level,duration of symptoms, duration of the procedure and time elapsedfrom the procedure were entered as covariates. P < 0.05 wasconsidered a significant result. All statistical analyses wereperformed with SAS 9.1 (SAS Institute, Cary, NC).
3. Results
A total of 255 premenopausal women were eligible for thestudy. Patients’ characteristics are summarized in Table 1. Meanage was 44.9 � 3.8 years, and mean duration of menorrhagiacomplaints was 16.9 � 11.2 months. Prior hormone treatment toregulate bleeding had been prescribed in 44% (n = 112) of womenwithout satisfactory outcome. Anemia with hemoglobin below 12 g%was diagnosed in 34% of the women and 9.4% had a hemoglobin levelbelow 10 gm%. All cases had a final histological diagnosis of smallendometrial polyp.
Two hundred and twenty-nine women responded to thetelephone interview. Subjective improvement in magnitude ofbleeding was reported by 70% (n = 160) of women, but only 26%(n = 59) experienced return to regular menses. Additionally, 80%(n = 183) of the subjects reported satisfaction with the procedure.Fewer than 5% of the patients experienced substantial painfollowing the procedure, and only 18% (n = 42) remained overnightin the hospital. No serious complications were recorded. Sixwomen suffered minor complications, such as transient fever,pelvic inflammatory disease, cervical laceration and false route.
A univariate logistic regression model comparing the sub-groups of women reporting improvement in the magnitude ofmenstrual bleeding (favorable outcome) vs. those reporting a lackof change (failed outcome) for the following parameters: age,parity, weight, pre-procedure hemoglobin level, duration ofsymptoms, duration of the procedure and time elapsed fromoperative hysteroscopy to interview, revealed that patient age andparity differed significantly between the groups (Table 2). When
Table 1Baseline characteristics of the study cohort.
Mean � SD Median Range
Age (years) 44.9 � 3.8 46 29–53
Parity 3.7 � 1.7 4 0–12
Weight (kg) 62.8 � 7.9 62 46–89
Duration of symptoms (months) 16.9 � 11.2 12 4–60
Hemoglobin level at time of
procedure (g%)
11 � 1.3 11.1 6–14.4
Duration of procedure (min) 25.8 � 6.4 25 14–55
Time elapsed between procedure and
interview (months)
8.3 � 1.8 8 6–14
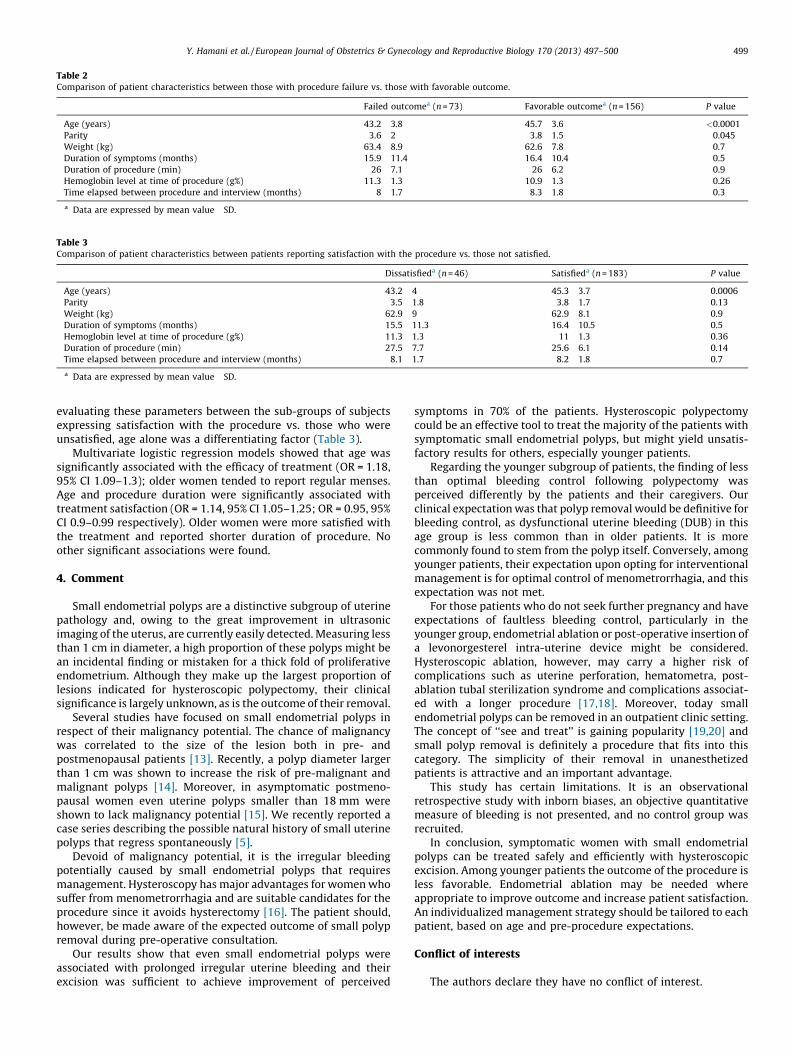
Table 2Comparison of patient characteristics between those with procedure failure vs. those with favorable outcome.
Failed outcomea (n = 73) Favorable outcomea (n = 156) P value
Age (years) 43.2 � 3.8 45.7 � 3.6 <0.0001
Parity 3.6 � 2 3.8 � 1.5 0.045
Weight (kg) 63.4 � 8.9 62.6 � 7.8 0.7
Duration of symptoms (months) 15.9 � 11.4 16.4 � 10.4 0.5
Duration of procedure (min) 26 � 7.1 26 � 6.2 0.9
Hemoglobin level at time of procedure (g%) 11.3 � 1.3 10.9 � 1.3 0.26
Time elapsed between procedure and interview (months) 8 � 1.7 8.3 � 1.8 0.3
a Data are expressed by mean value � SD.
Table 3Comparison of patient characteristics between patients reporting satisfaction with the procedure vs. those not satisfied.
Dissatisfieda (n = 46) Satisfieda (n = 183) P value
Age (years) 43.2 � 4 45.3 � 3.7 0.0006
Parity 3.5 � 1.8 3.8 � 1.7 0.13
Weight (kg) 62.9 � 9 62.9 � 8.1 0.9
Duration of symptoms (months) 15.5 � 11.3 16.4 � 10.5 0.5
Hemoglobin level at time of procedure (g%) 11.3 � 1.3 11 � 1.3 0.36
Duration of procedure (min) 27.5 � 7.7 25.6 � 6.1 0.14
Time elapsed between procedure and interview (months) 8.1 � 1.7 8.2 � 1.8 0.7
a Data are expressed by mean value � SD.
Y. Hamani et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 170 (2013) 497–500 499
evaluating these parameters between the sub-groups of subjectsexpressing satisfaction with the procedure vs. those who wereunsatisfied, age alone was a differentiating factor (Table 3).
Multivariate logistic regression models showed that age wassignificantly associated with the efficacy of treatment (OR = 1.18,95% CI 1.09–1.3); older women tended to report regular menses.Age and procedure duration were significantly associated withtreatment satisfaction (OR = 1.14, 95% CI 1.05–1.25; OR = 0.95, 95%CI 0.9–0.99 respectively). Older women were more satisfied withthe treatment and reported shorter duration of procedure. Noother significant associations were found.
4. Comment
Small endometrial polyps are a distinctive subgroup of uterinepathology and, owing to the great improvement in ultrasonicimaging of the uterus, are currently easily detected. Measuring lessthan 1 cm in diameter, a high proportion of these polyps might bean incidental finding or mistaken for a thick fold of proliferativeendometrium. Although they make up the largest proportion oflesions indicated for hysteroscopic polypectomy, their clinicalsignificance is largely unknown, as is the outcome of their removal.
Several studies have focused on small endometrial polyps inrespect of their malignancy potential. The chance of malignancywas correlated to the size of the lesion both in pre- andpostmenopausal patients [13]. Recently, a polyp diameter largerthan 1 cm was shown to increase the risk of pre-malignant andmalignant polyps [14]. Moreover, in asymptomatic postmeno-pausal women even uterine polyps smaller than 18 mm wereshown to lack malignancy potential [15]. We recently reported acase series describing the possible natural history of small uterinepolyps that regress spontaneously [5].
Devoid of malignancy potential, it is the irregular bleedingpotentially caused by small endometrial polyps that requiresmanagement. Hysteroscopy has major advantages for women whosuffer from menometrorrhagia and are suitable candidates for theprocedure since it avoids hysterectomy [16]. The patient should,however, be made aware of the expected outcome of small polypremoval during pre-operative consultation.
Our results show that even small endometrial polyps wereassociated with prolonged irregular uterine bleeding and theirexcision was sufficient to achieve improvement of perceived
symptoms in 70% of the patients. Hysteroscopic polypectomycould be an effective tool to treat the majority of the patients withsymptomatic small endometrial polyps, but might yield unsatis-factory results for others, especially younger patients.
Regarding the younger subgroup of patients, the finding of lessthan optimal bleeding control following polypectomy wasperceived differently by the patients and their caregivers. Ourclinical expectation was that polyp removal would be definitive forbleeding control, as dysfunctional uterine bleeding (DUB) in thisage group is less common than in older patients. It is morecommonly found to stem from the polyp itself. Conversely, amongyounger patients, their expectation upon opting for interventionalmanagement is for optimal control of menometrorrhagia, and thisexpectation was not met.
For those patients who do not seek further pregnancy and haveexpectations of faultless bleeding control, particularly in theyounger group, endometrial ablation or post-operative insertion ofa levonorgesterel intra-uterine device might be considered.Hysteroscopic ablation, however, may carry a higher risk ofcomplications such as uterine perforation, hematometra, post-ablation tubal sterilization syndrome and complications associat-ed with a longer procedure [17,18]. Moreover, today smallendometrial polyps can be removed in an outpatient clinic setting.The concept of ‘‘see and treat’’ is gaining popularity [19,20] andsmall polyp removal is definitely a procedure that fits into thiscategory. The simplicity of their removal in unanesthetizedpatients is attractive and an important advantage.
This study has certain limitations. It is an observationalretrospective study with inborn biases, an objective quantitativemeasure of bleeding is not presented, and no control group wasrecruited.
In conclusion, symptomatic women with small endometrialpolyps can be treated safely and efficiently with hysteroscopicexcision. Among younger patients the outcome of the procedure isless favorable. Endometrial ablation may be needed whereappropriate to improve outcome and increase patient satisfaction.An individualized management strategy should be tailored to eachpatient, based on age and pre-procedure expectations.
Conflict of interests
The authors declare they have no conflict of interest.

Y. Hamani et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 170 (2013) 497–500500
Contribution to authorship
All authors contributed to the manuscript sufficiently to justifytheir inclusion as authors, and take full responsibility for its contents.
Details of ethics approval
At the time the data were collected for this study, ethicsapproval was not required for this type of study.
Funding
No funding was received for this study.
References
[1] Peterson WF, Novak ER. Endometrial polyps. Obstet Gynecol 1956;8:40–9.[2] Clevenger-Hoeft M, Syrop CH, Stovall DW, Van Voorhis BJ. Sonohysterography
in premenopausal women with and without abnormal bleeding. Obstet Gyne-col 1999;94:516–20.
[3] Katz VL. Benign gynecologic lesions. In: Katz VL, Gretchen M, Lentz RAL, DavidM, Gershenson, editors. Comprehensive gynecology. 5th ed., Philadelphia:Mosby Elsevier; 2007.
[4] DeWaay DJ, Syrop CH, Nygaard IE, Davis WA, Van Voorhis BJ. Natural history ofuterine polyps and leiomyomata. Obstet Gynecol 2002;100:3–7.
[5] Haimov-Kochman R, Deri-Hasid R, Hamani Y, Voss E. The natural course ofendometrial polyps: could they vanish when left untreated? Fertil Steril2009;92. 828.e11–2.
[6] van Dongen H, Janssen CA, Smeets MJ, Emanuel MH, Jansen FW. The clinicalrelevance of hysteroscopic polypectomy in premenopausal women with ab-normal uterine bleeding. BJOG 2009;116:1387–90.
[7] Ryan GL, Syrop CH, Van Voorhis BJ. Role epidemiology, and natural history ofbenign uterine mass lesions. Clin Obstet Gynecol 2005;48:312–24.
[8] Bignardi T, Van den Bosch T, Condous G. Abnormal uterine and post-meno-pausal bleeding in the acute gynaecology unit. Best Pract Res Clin ObstetGynaecol 2009;23:595–607.
[9] Clark TJ, Godwin J, Khan KS, Gupta JK. Ambulatory endoscopic treatment ofsymptomatic benign endometrial polyps: a feasibility study. Gynecol Endosc2002;11:91–7.
[10] Stamatellos I, Apostolides A, Stamatopoulos P, Bontis J. Pregnancy rates afterhysteroscopic polypectomy depending on the size or number of the polyps.Arch Gynecol Obstet 2008;277:395–9.
[11] Lieng M, Istre O, Qvigstad E. Treatment of endometrial polyps: a systematicreview. Acta Obstet Gynecol Scand 2010;89:992–1002.
[12] Lee SC, Kaunitz AM, Sanchez-Ramos L, Rhatigan RM. The oncogenic potentialof endometrial polyps: a systematic review and meta-analysis. Obstet Gynecol2010;116:1197–205.
[13] Ben-Arie A, Goldchmit C, Laviv Y, et al. The malignant potential of endometrialpolyps. Eur J Obstet Gynecol Reprod Biol 2004;115:206–10.
[14] Wang JH, Zhao J, Lin J. Opportunities and risk factors for premalignant andmalignant transformation of endometrial polyps: management strategies. JMinim Invasive Gynecol 2010;17:53–8.
[15] Ferrazzi E, Zupi E, Leone FP, et al. How often are endometrial polyps malignantin asymptomatic postmenopausal women? A multicenter study. Am J ObstetGynecol 2009;200. 235.e1–6.
[16] Cravello L, D’Ercole C, Roge P, Boubli L, Blanc B. Hysteroscopic management ofmenstrual disorders: a review of 395 patients. Eur J Obstet Gynecol ReprodBiol 1996;67:163–7.
[17] Propst AM, Liberman RF, Harlow BL, Ginsburg ES. Complications of hys-teroscopic surgery: predicting patients at risk. Obstet Gynecol 2000;96:517–20.
[18] Jansen FW, Vredevoogd CB, van Ulzen K, Hermans J, Trimbos JB, Trimbos-Kemper TC. Complications of hysteroscopy: a prospective, multicenter study.Obstet Gynecol 2000;96:266–70.
[19] Bettocchi S, Ceci O, Di Venere R, et al. Advanced operative office hysteroscopywithout anaesthesia: analysis of 501 cases treated with a 5 Fr. bipolar elec-trode. Hum Reprod 2002;17:2435–8.
[20] Garuti G, Cellani F, Colonnelli M, Grossi F, Luerti M. Outpatient hysteroscopicpolypectomy in 237 patients: feasibility of a one-stop see-and-treat proce-dure. J Am Assoc Gynecol Laparosc 2004;11:500–4.