Embed Size (px)
Citation preview
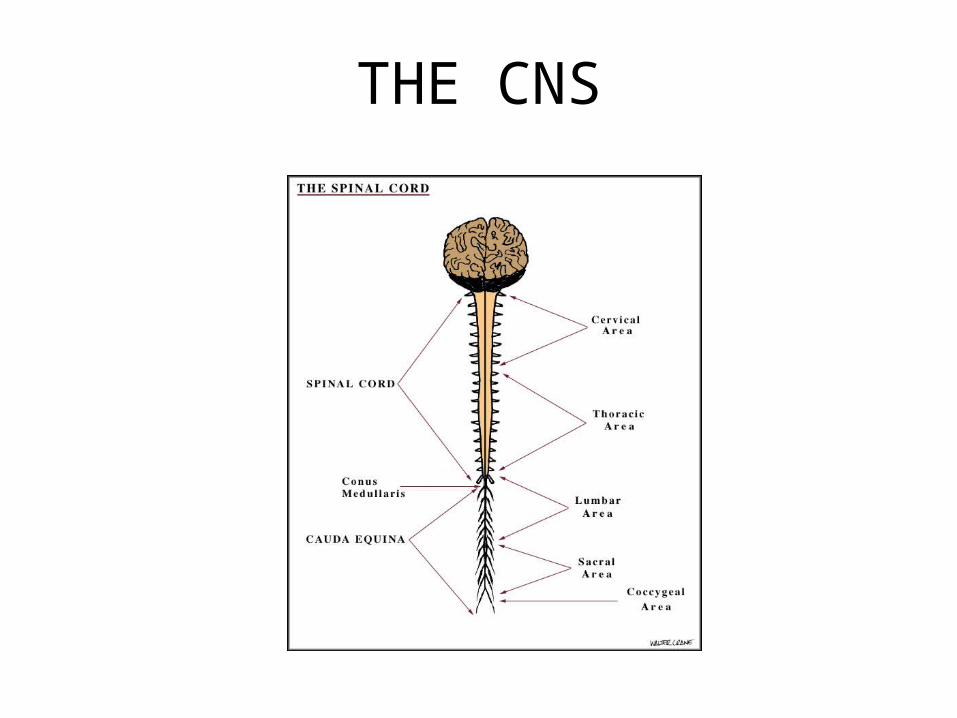
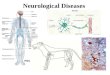
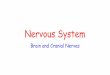
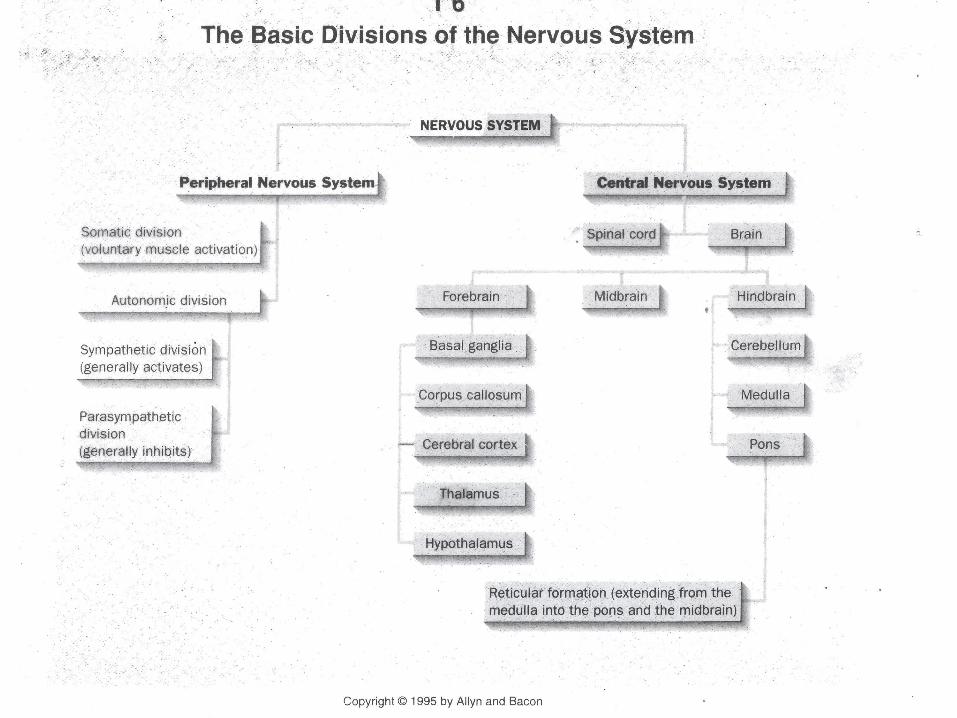
THE CNS
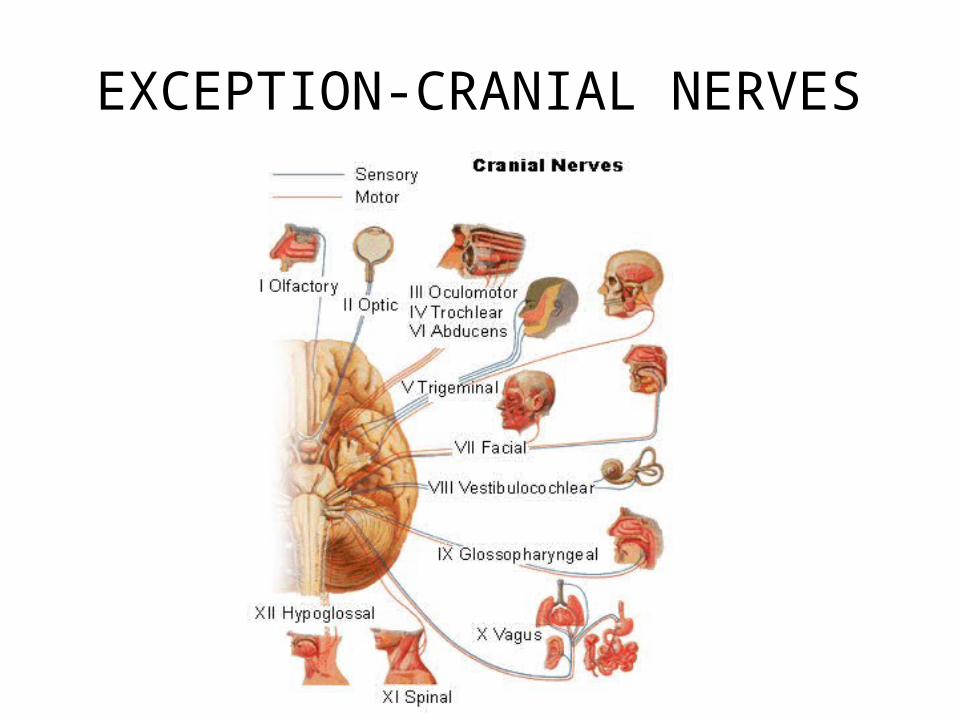
EXCEPTION-CRANIAL NERVES
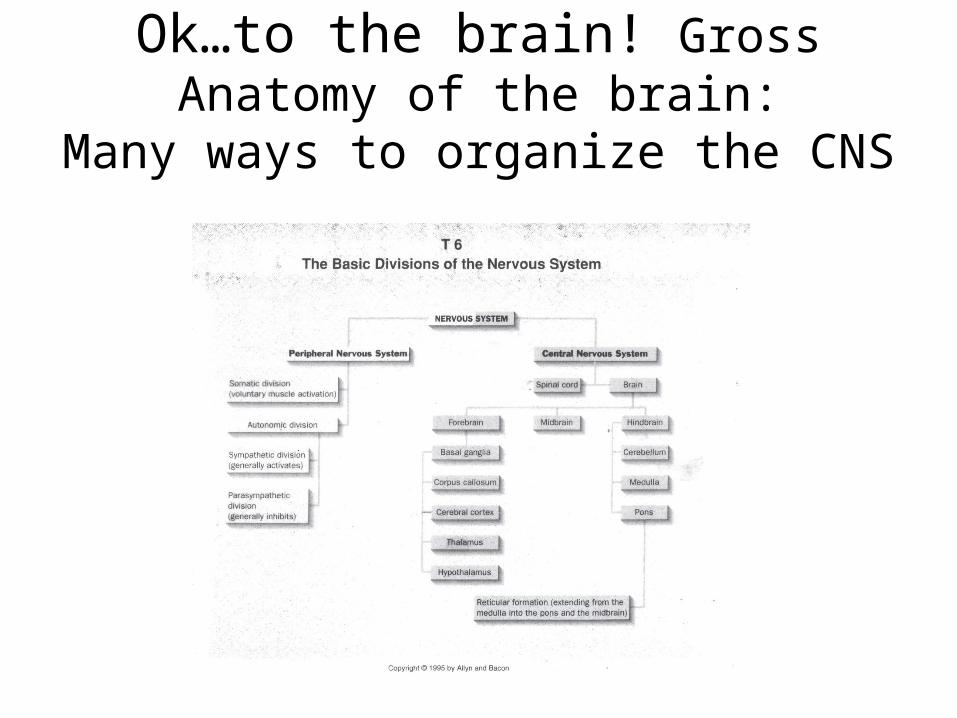
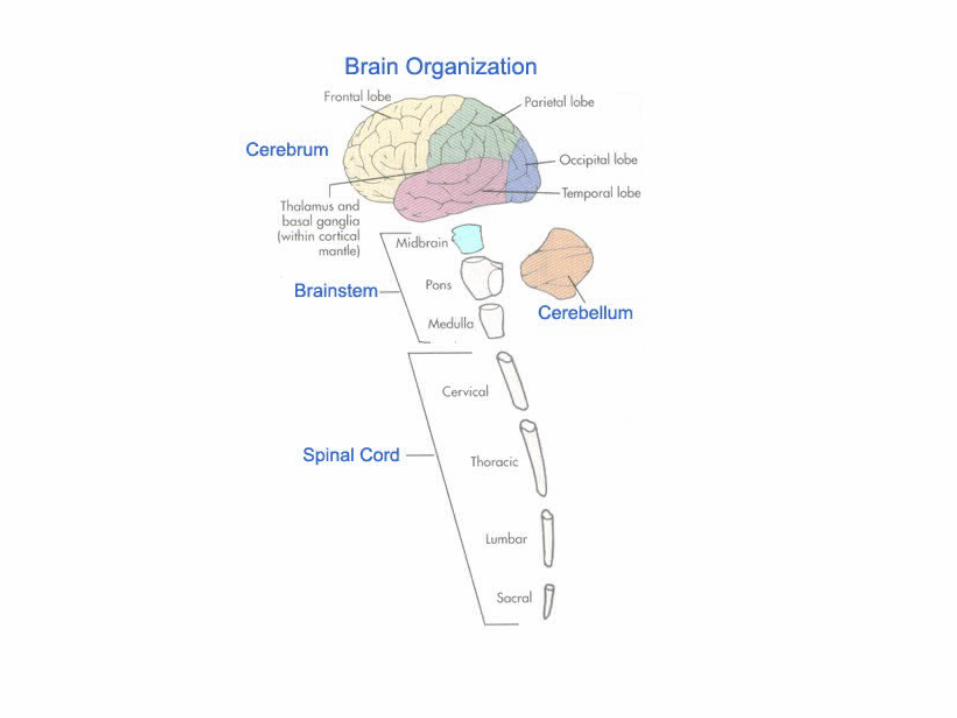
Ok…to the brain! Gross Anatomy of the brain:
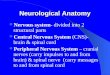
Many ways to organize the CNS
Here’s a good one!
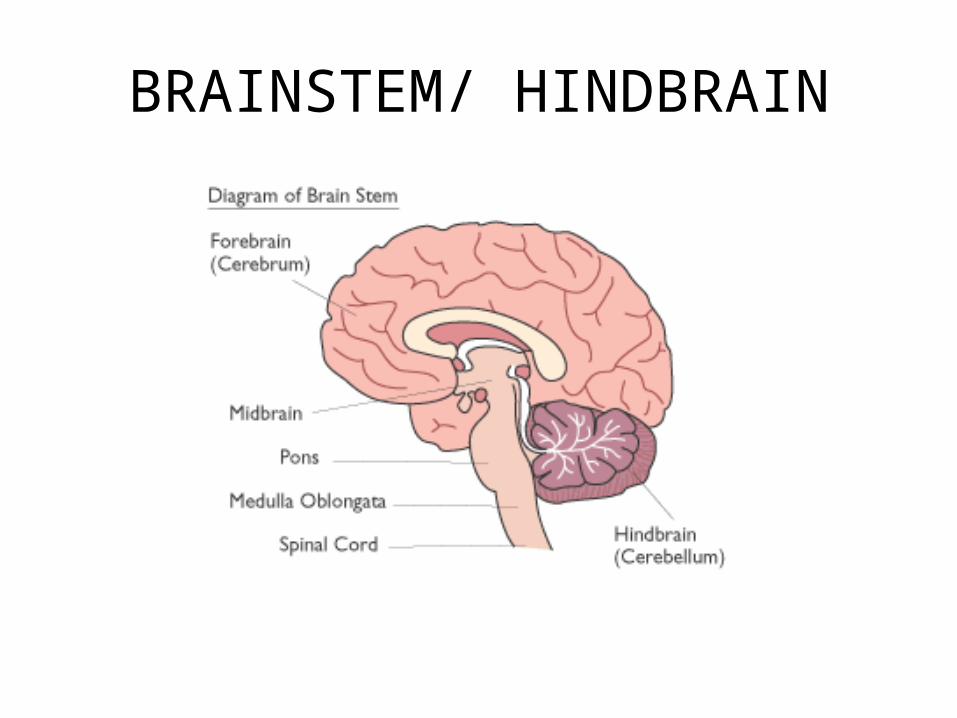
BRAINSTEM/ HINDBRAIN
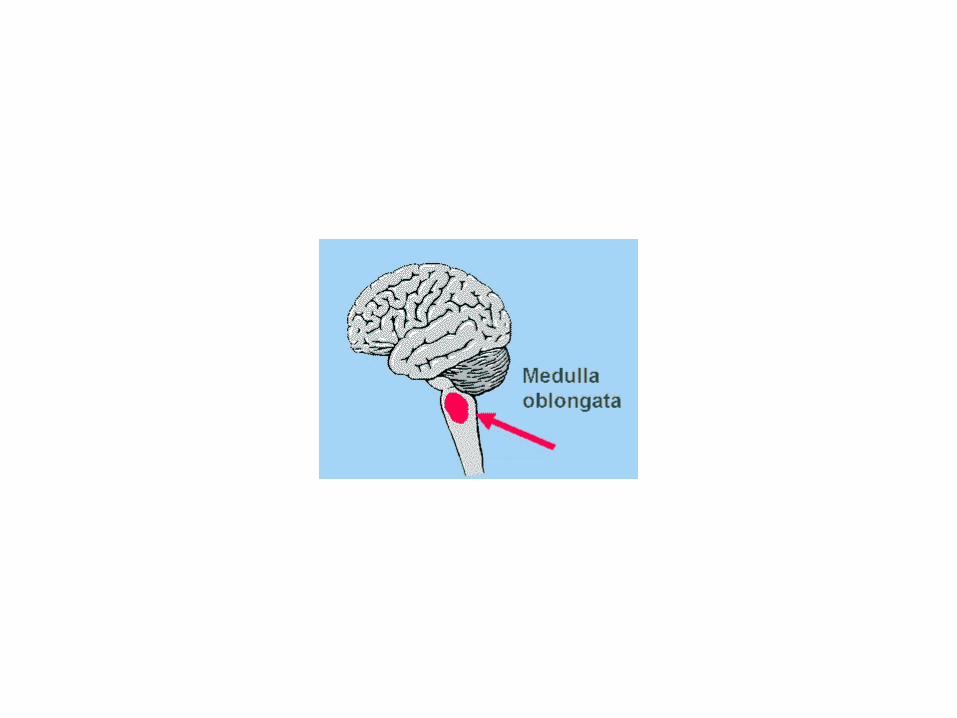
Bainstem (Medulla) critical functions
• Ascending and Descending Fiber Tracts
• All parasympathetic tone– HR
• Temp• BP• Etc
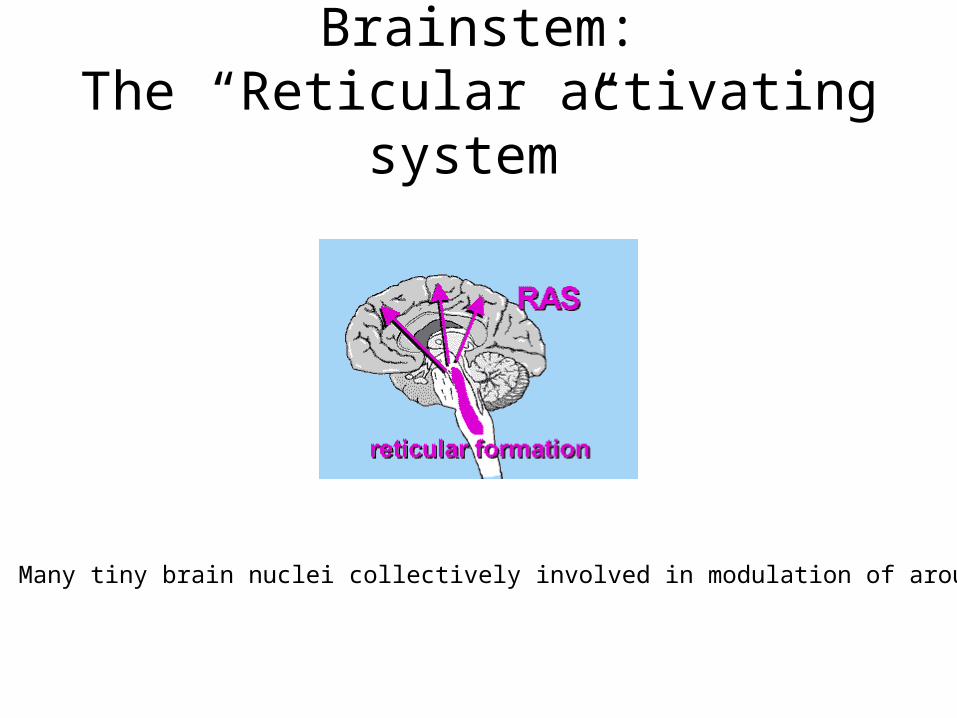
Brainstem:The “Reticular activating system”
Many tiny brain nuclei collectively involved in modulation of arousal
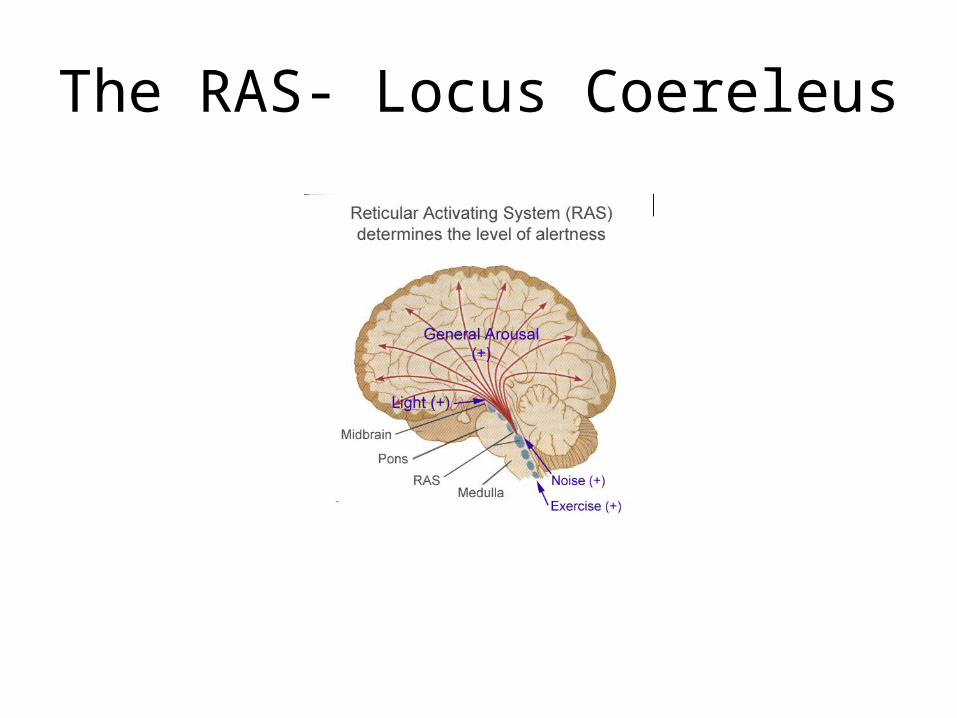
The RAS- Locus Coereleus
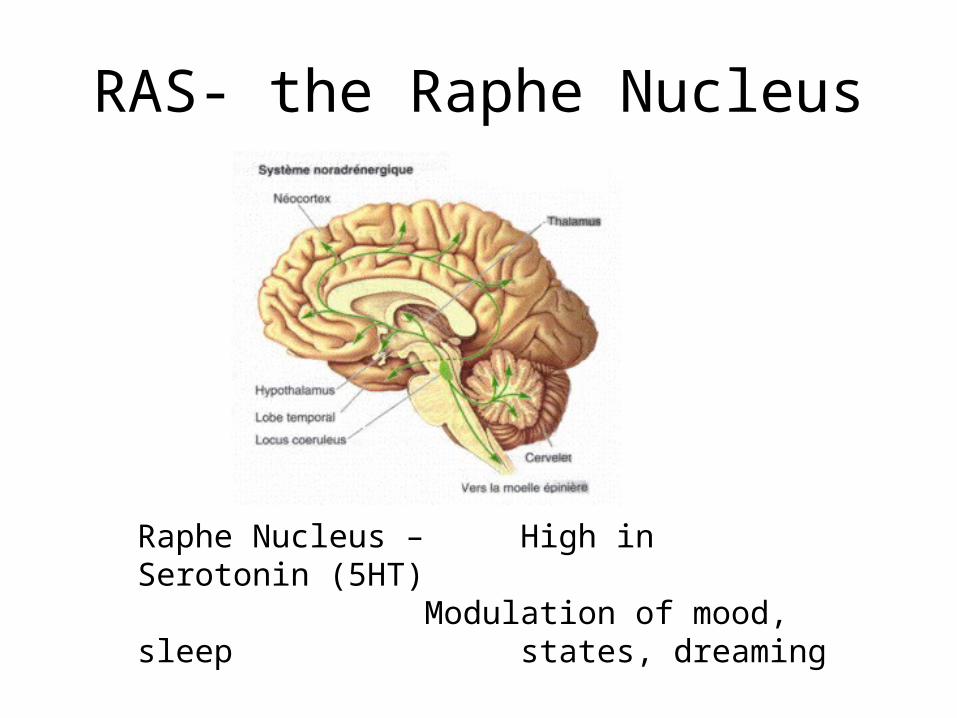
RAS- the Raphe Nucleus
Raphe Nucleus – High in Serotonin (5HT)Modulation of mood, sleep states, dreaming
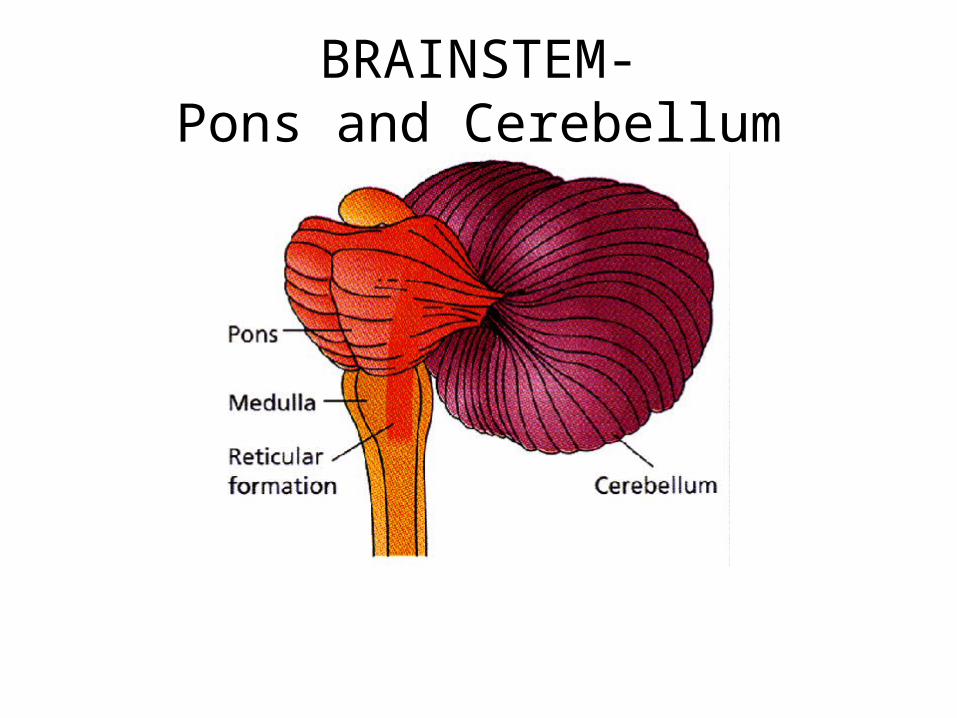
BRAINSTEM-Pons and Cerebellum
Behavioral Functions of the Cerebellum
• Direction
• Amplitude
• Force
• Timing– Posture– Motor learning/speech
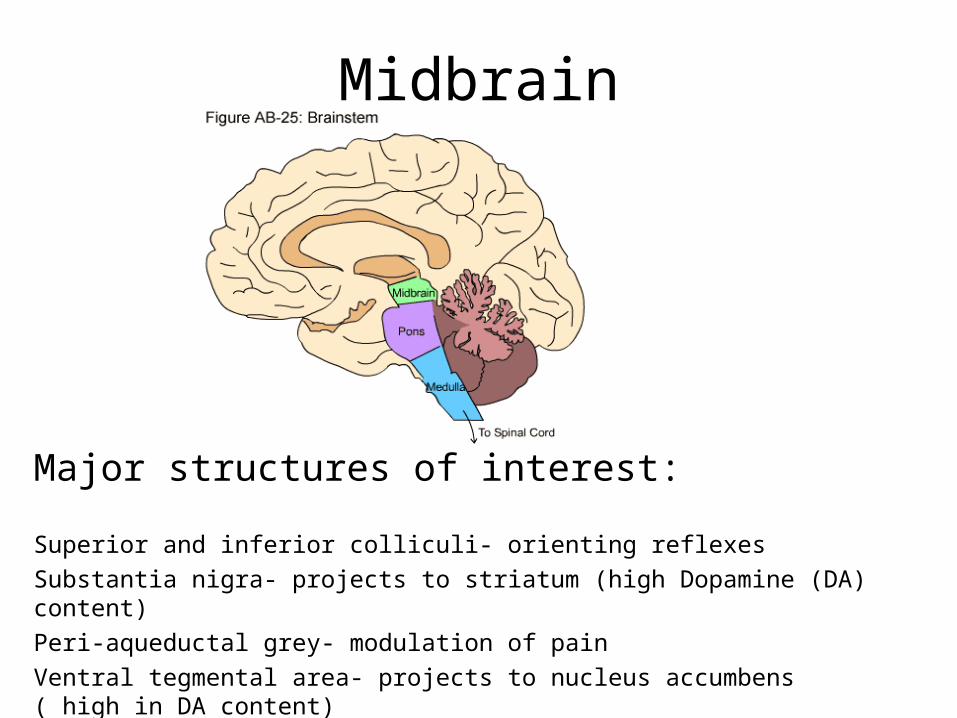
Midbrain
Major structures of interest:
Superior and inferior colliculi- orienting reflexes
Substantia nigra- projects to striatum (high Dopamine (DA) content)
Peri-aqueductal grey- modulation of pain
Ventral tegmental area- projects to nucleus accumbens ( high in DA content)
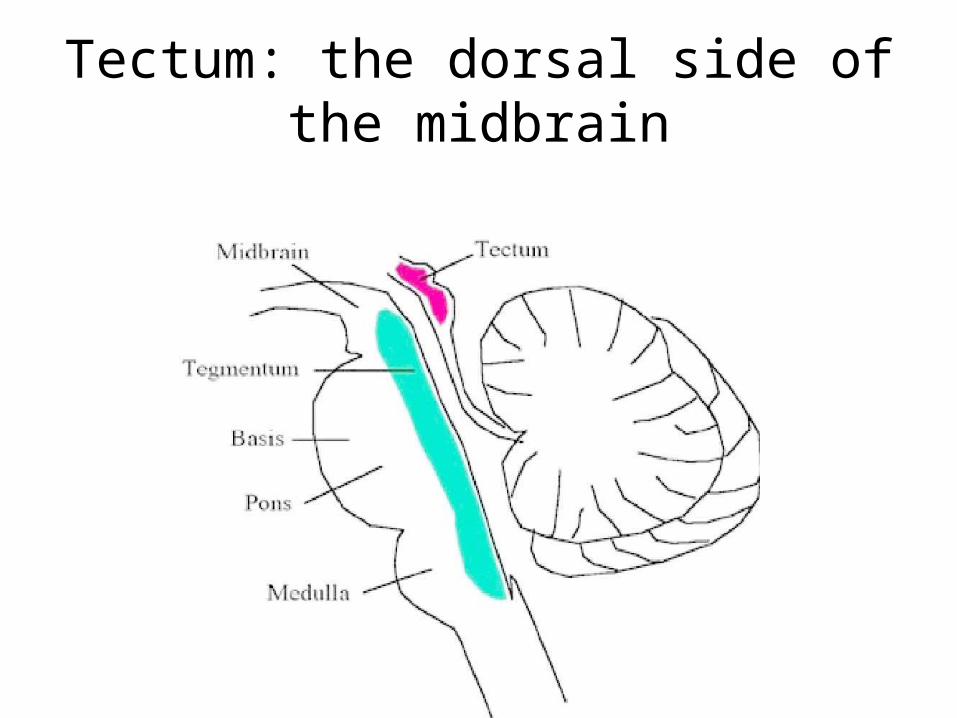
Tectum: the dorsal side of the midbrain
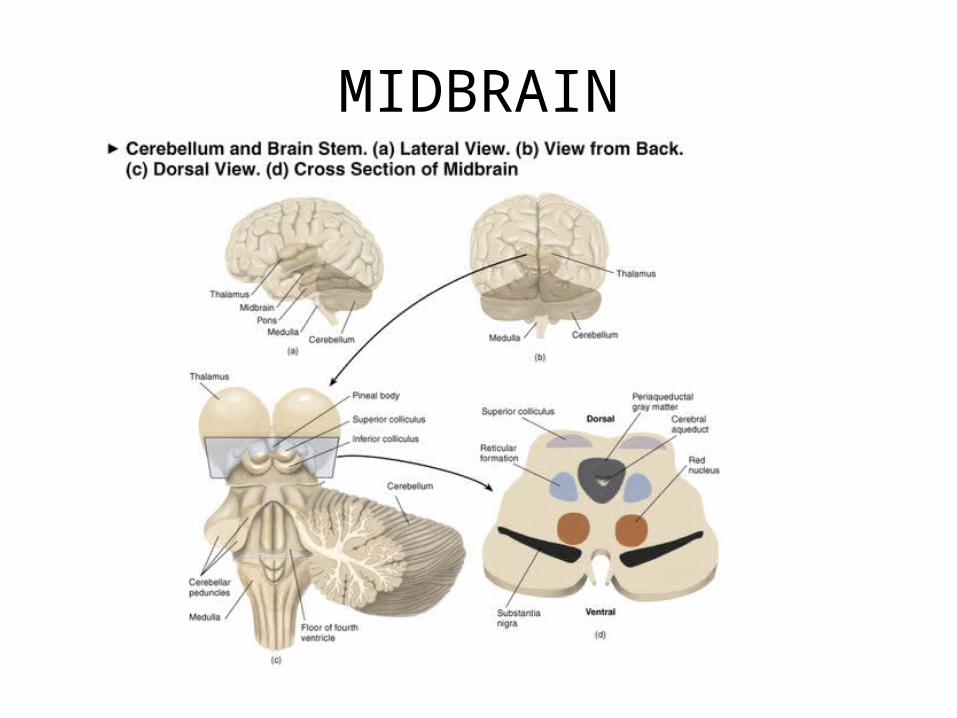
MIDBRAIN
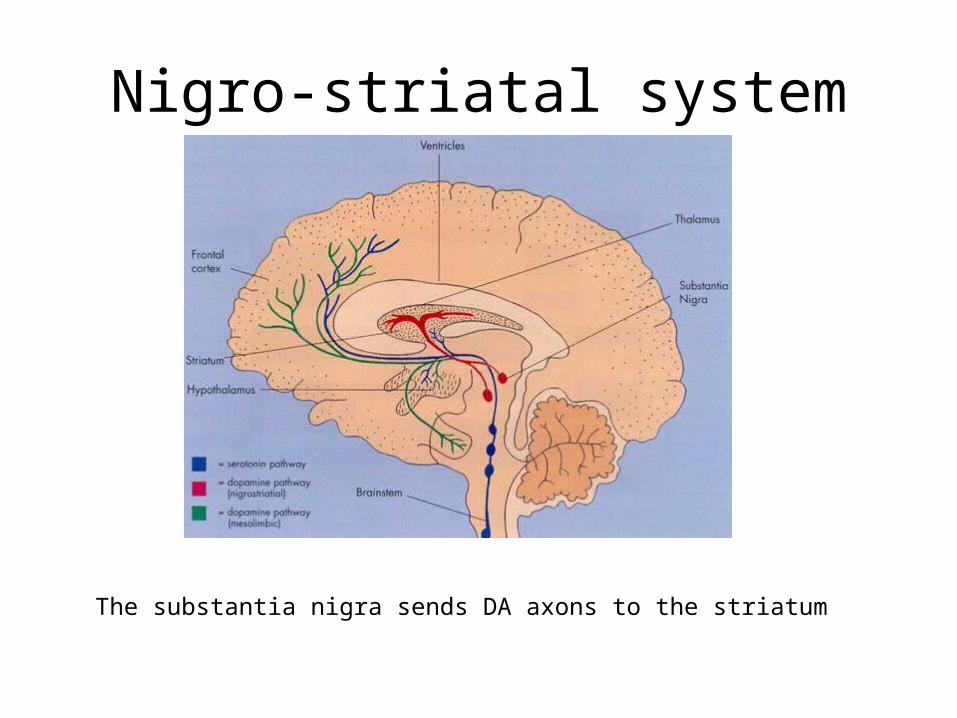
Nigro-striatal system
The substantia nigra sends DA axons to the striatum
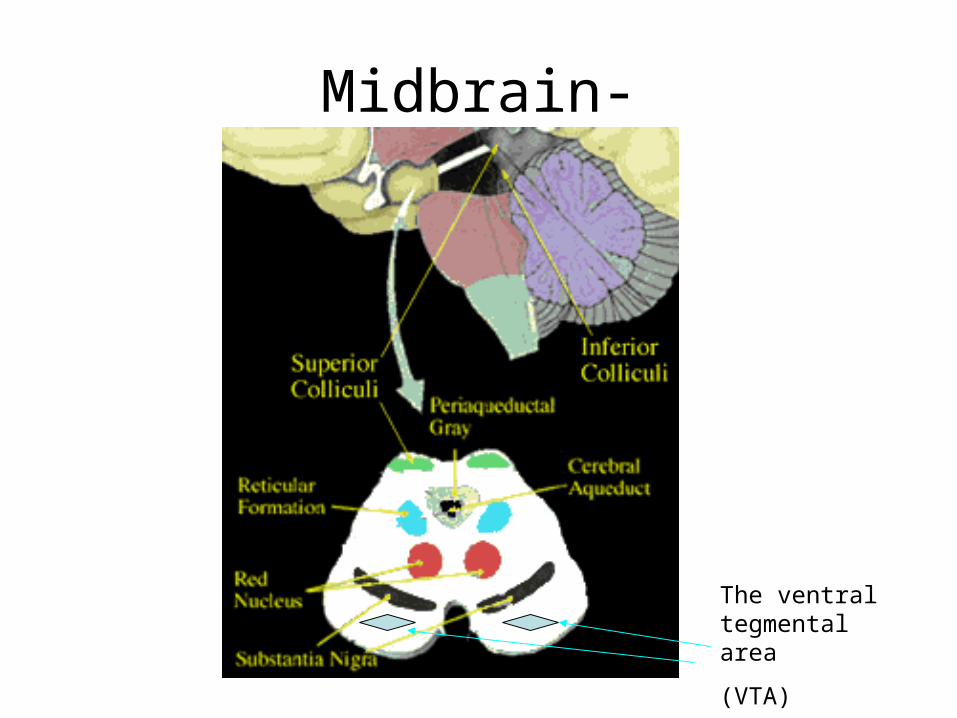
Midbrain-
The ventral tegmental area
(VTA)
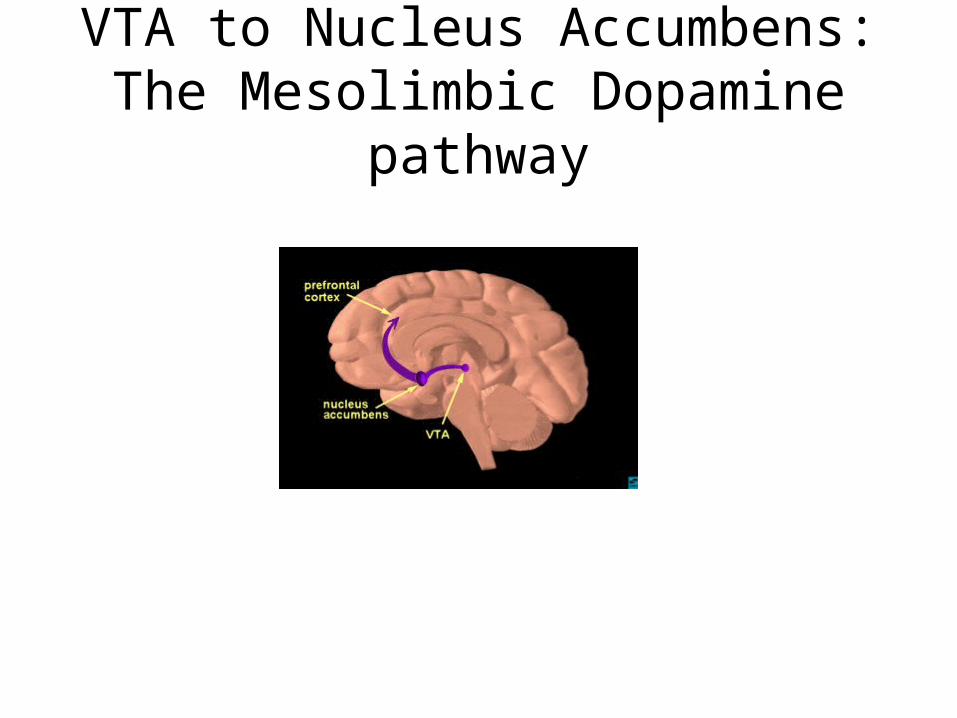
VTA to Nucleus Accumbens: The Mesolimbic Dopamine pathway
Diencephalon
Thalamus, Hypothalamus and Pituitary gland
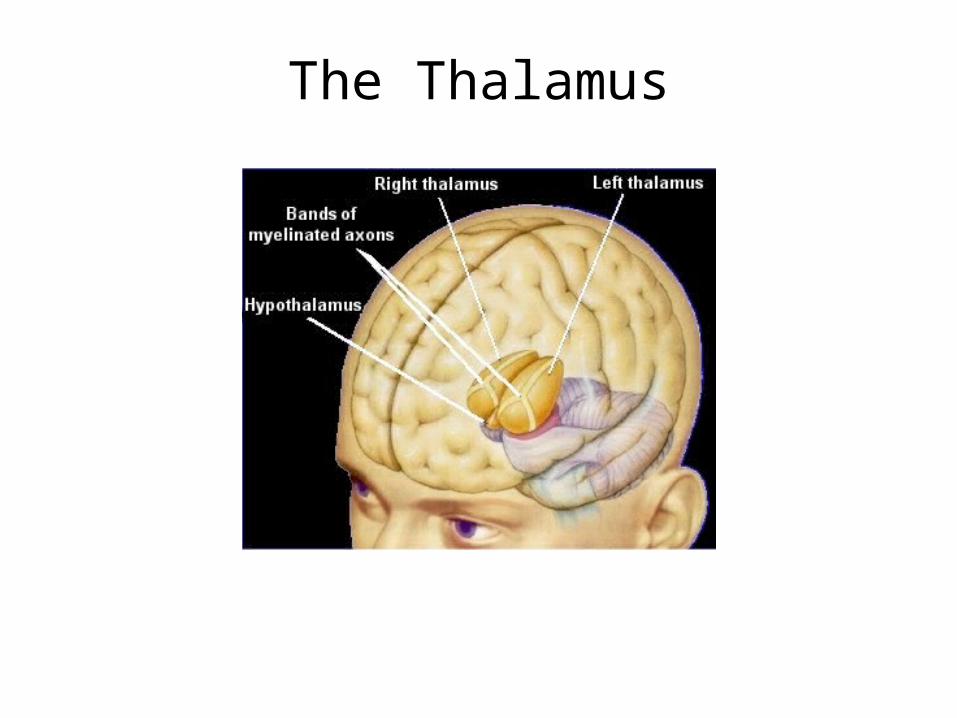
The Thalamus
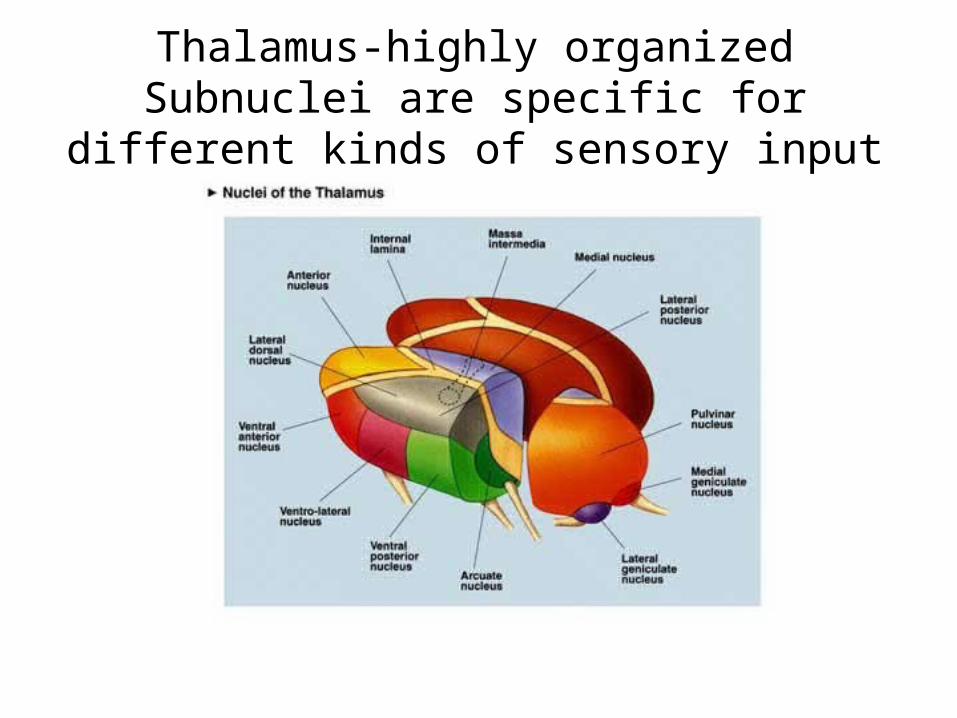
Thalamus-highly organizedSubnuclei are specific for different kinds of
sensory input
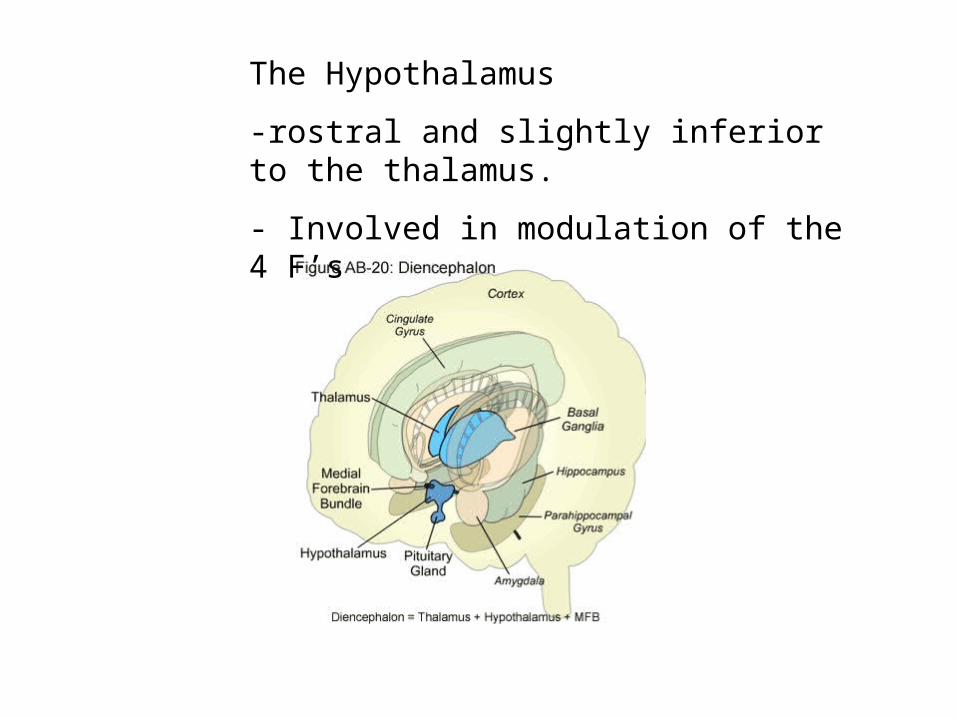
The Hypothalamus
-rostral and slightly inferior to the thalamus.
- Involved in modulation of the 4 F’s
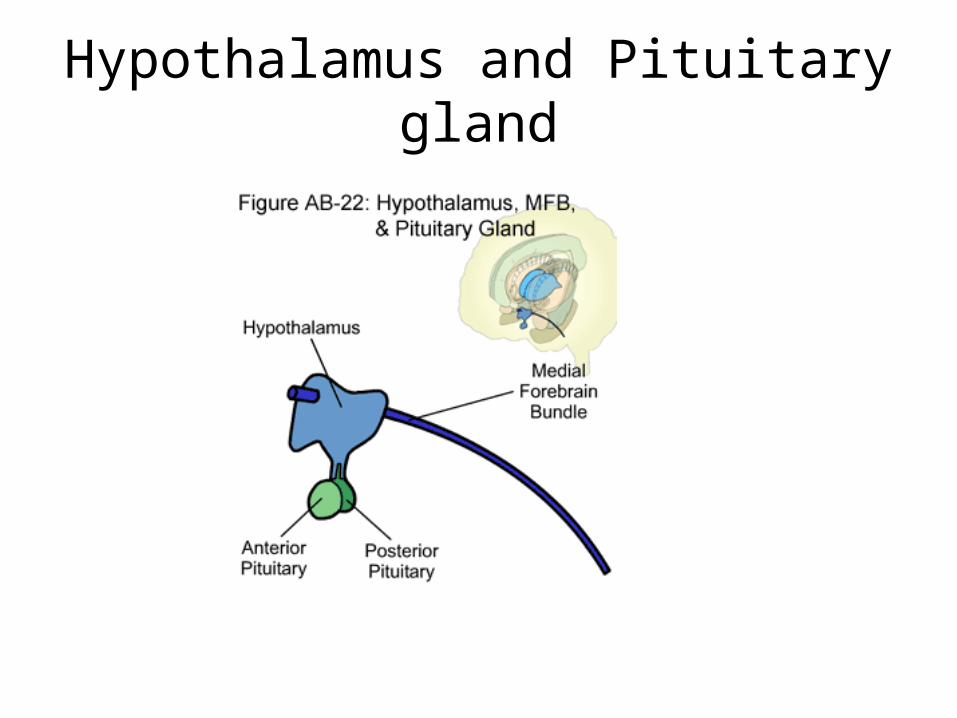
Hypothalamus and Pituitary gland
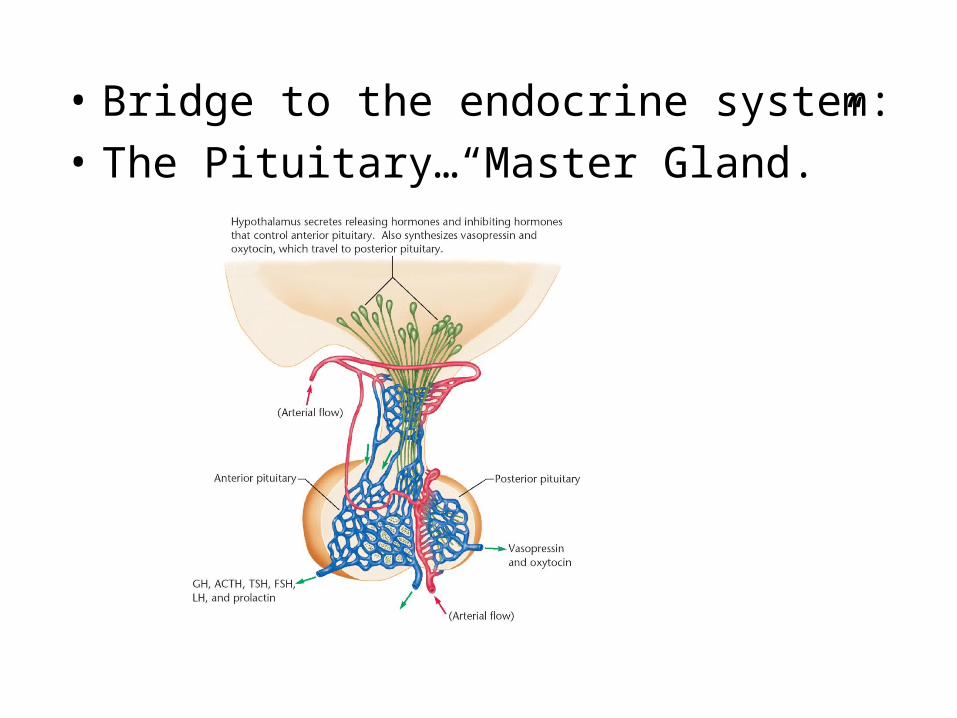
• Bridge to the endocrine system:
• The Pituitary…“Master Gland.”
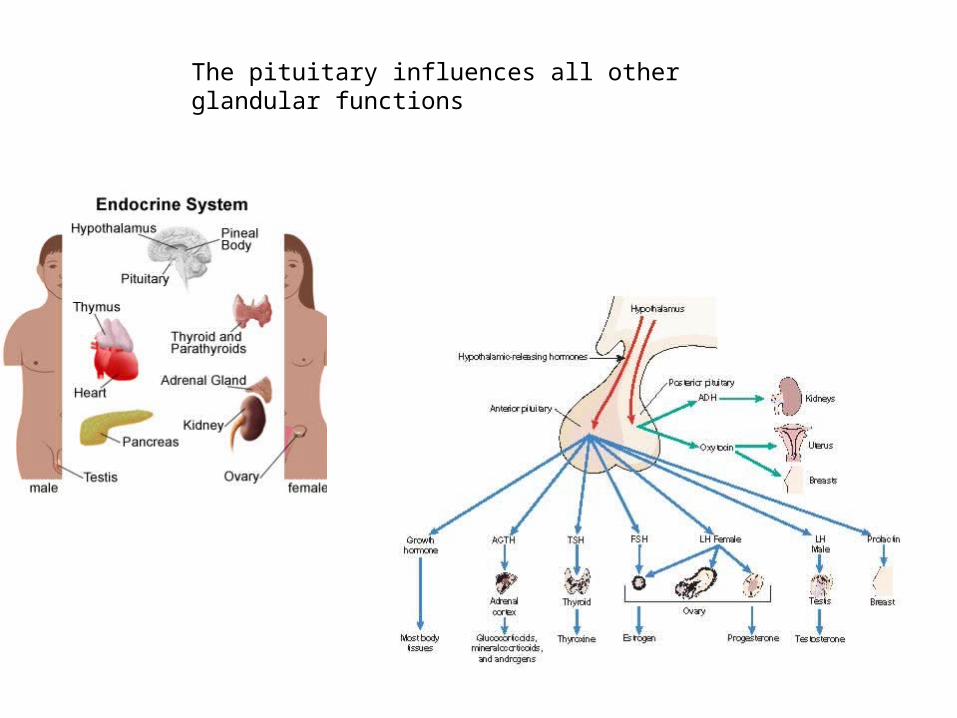
The pituitary influences all other glandular functions
Forebrain
• (Telencephalon)– Cortex
• Basal ganglia• Limbic System
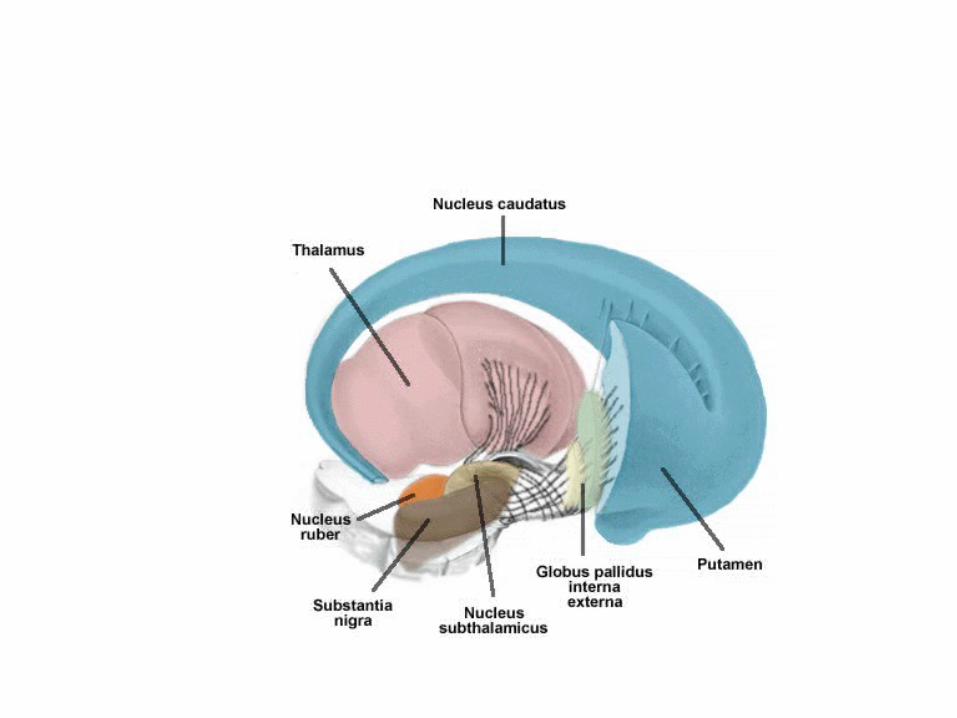
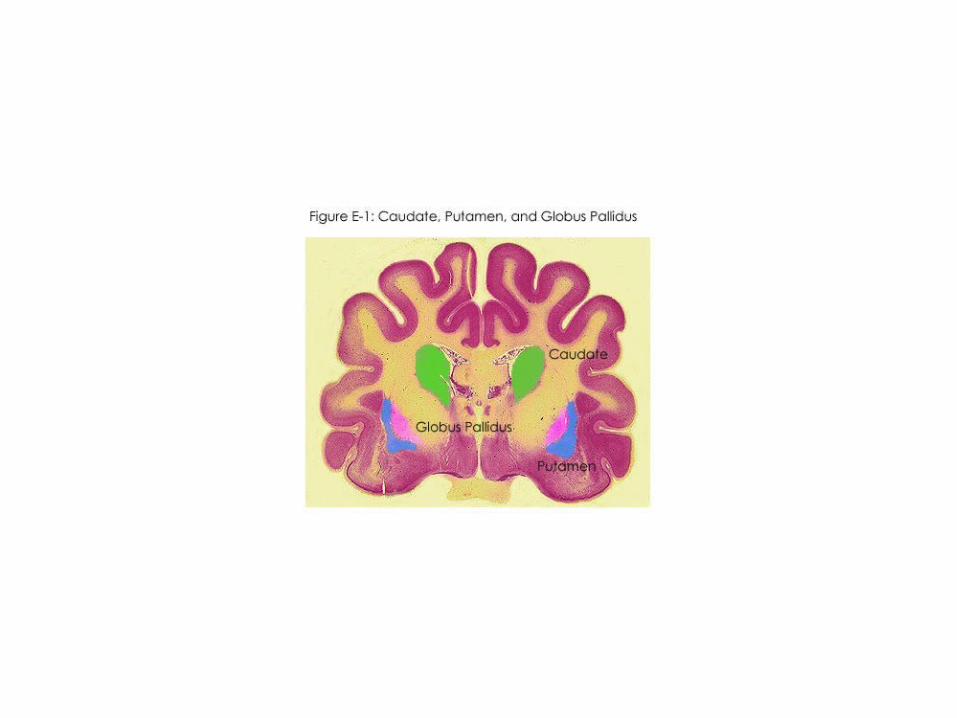
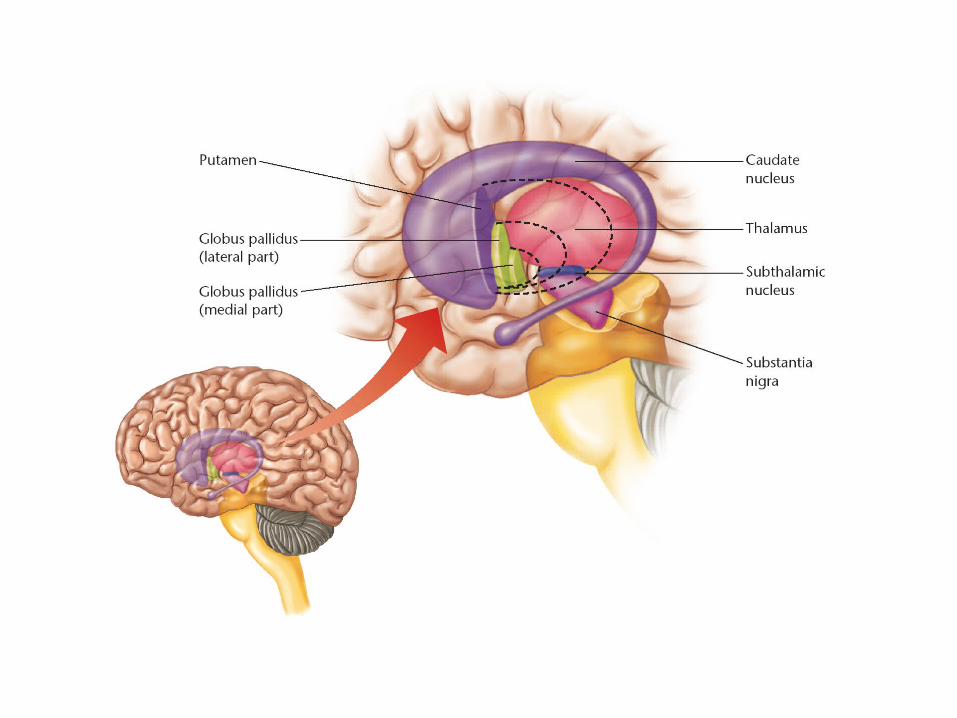
Basal Ganglia
• Neostriatum– Caudate nucleus and putamen
• Globus Pallidus
• Substantia nigra
• others
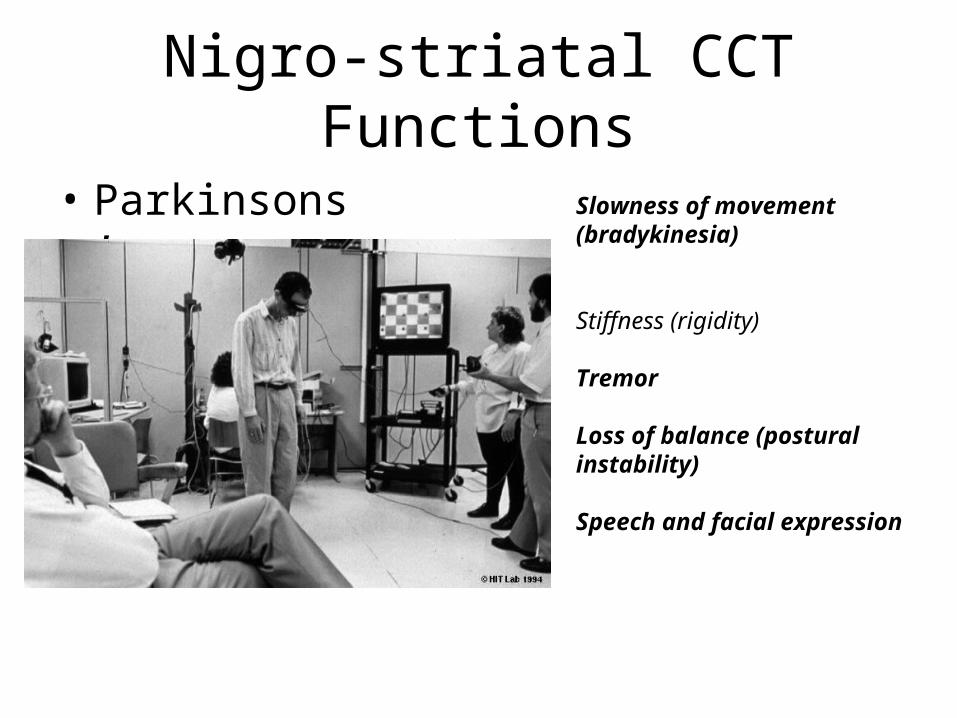
Nigro-striatal CCT Functions
• Parkinsons’ Slowness of movement (bradykinesia)
Stiffness (rigidity)
Tremor
Loss of balance (postural instability)
Speech and facial expression
**Difficulty in initiating Movement

Striatal-Pallidal CCT functions?
• Huntingtons
• Tourettes’ -
Tourettes• Tourette syndrome (TS) is a neurological disorder characterized by
repetitive, stereotyped, involuntary movements and vocalizations called tics. The early symptoms of TS are almost always noticed first in childhood, with the average onset between the ages of 7 and 10 years. TS occurs in people from all ethnic groups; males are affected about three to four times more often than females. It is estimated that 200,000 Americans have the most severe form of TS, and as many as one in 100 exhibit milder and less complex symptoms such as chronic motor or vocal tics or transient tics of childhood. Although TS can be a chronic condition with symptoms lasting a lifetime, most people with the condition experience their worst symptoms in their early teens, with improvement occurring in the late teens and continuing into adulthood.
• Tics are classified as either simple or complex. Simple motor tics are sudden, brief, repetitive movements that involve a limited number of muscle groups. Some of the more common simple tics include eye blinking and other vision irregularities, facial grimacing, shoulder shrugging, and head or shoulder jerking. Simple vocalizations might include repetitive throat-clearing, sniffing, or grunting sounds. Complex tics are distinct, coordinated patterns of movements involving several muscle groups. Complex motor tics might include facial grimacing combined with a head twist and a shoulder shrug. Other complex motor tics may actually appear purposeful, including sniffing or touching objects, hopping, jumping, bending, or twisting. Simple vocal tics may include throat-clearing, sniffing/snorting, grunting, or barking. More complex vocal tics include words or phrases. Perhaps the most dramatic and disabling tics include motor movements that result in self-harm such as punching oneself in the face or vocal tics including coprolalia (uttering swear words) or echolalia (repeating the words or phrases of others). Most patients experience peak tic severity before the mid-teen years with improvement for the majority of patients in the late teen years and early adulthood. Approximately 10 percent of those affected have a progressive or disabling course that lasts into adulthood.
• Tics are involuntary. They are brief, repetitive movements, which are either motor such as blinking or head jerking, or vocal such as
throat clearing.
• Huntington's Chorea is principally characterized by hyperkinesias - abnormal, purposeless, involuntary motor movements that can occur spontaneously or only when the patient is trying to do something. These movements may be repetitive or non-repetitive.
• Sudden jerky, involuntary movements (chorea) throughout your body
• A wide, prancing gait • Severe problems with balance and coordination • Difficulty shifting your gaze without moving your head • Hesitant, halting or slurred speech • Inability to swallow • Dementia
Huntington’s chorea
LIMBIC SYSTEM
• Basal forebrain• Interconnected• Affective responses• Impulsive…low consciousness
– Many structures• Amygdala• Hippocampus• Septum/ nucleus accumbens- will be discussed later
Amygdala: general emotional significance of environmental stimuli
– evaluate the significance of stimuli and generate emotional responses
– generate hormonal secretions and autonomic reactions that accompany strong emotions
– damage causes “psychic blindness” and the inability to recognize fear in facial expressions and voice
– Projects to hypothalamus, Hippocampus, cortex
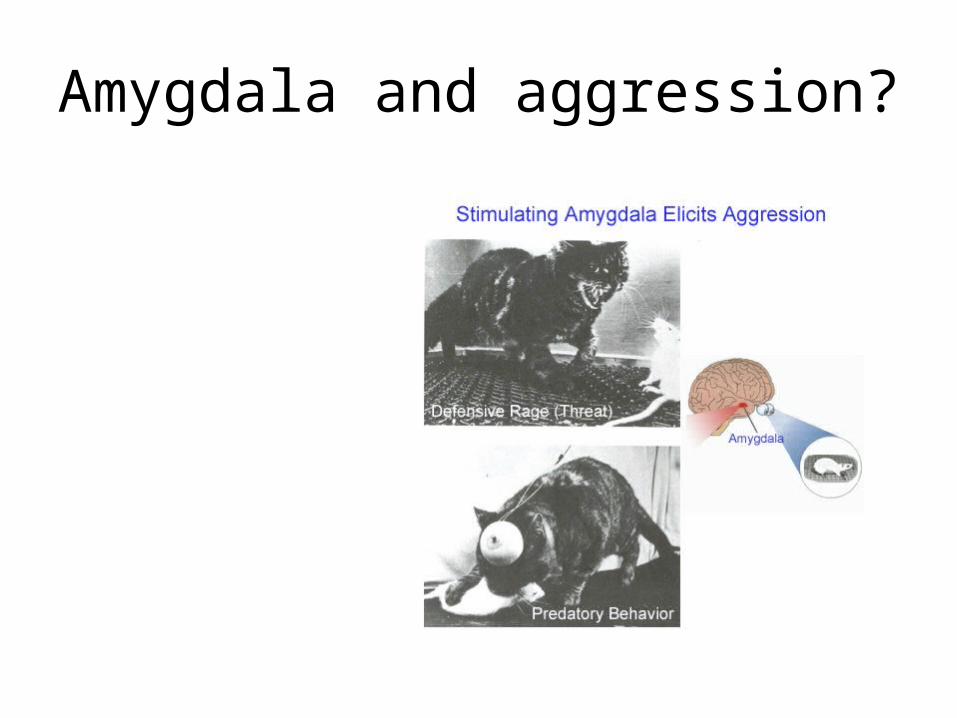
Amygdala and aggression?
Amygdala and fear?
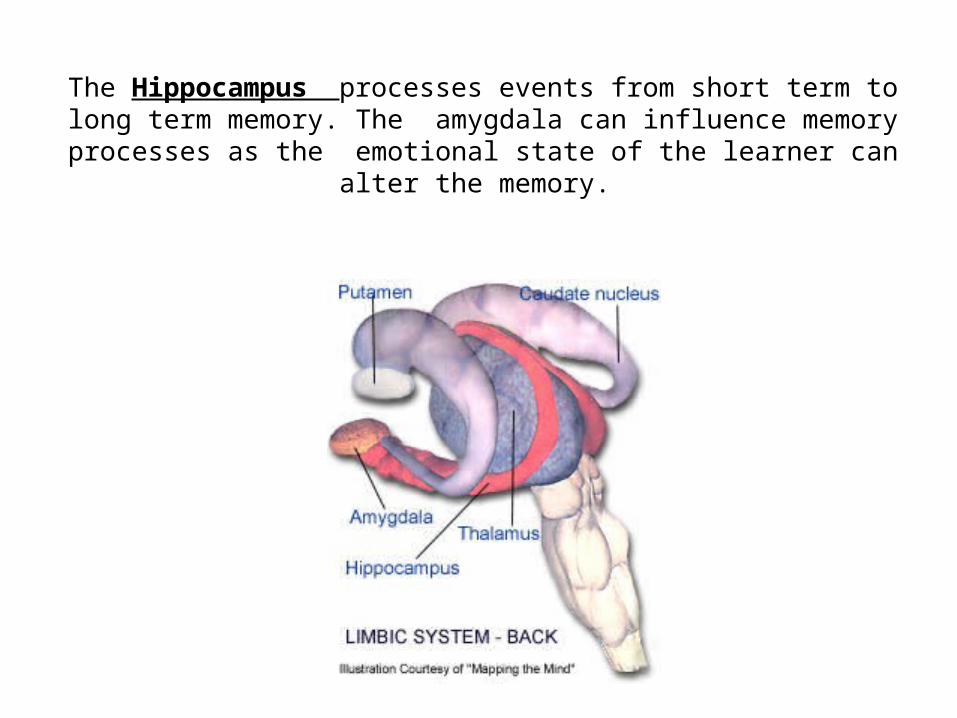
The Hippocampus processes events from short term to long term memory. The amygdala can influence memory processes as the
emotional state of the learner can alter the memory.
CEREBRAL CORTEX
• Wrinkled
• Thin
• Layered
• Interconnected
• Plastic
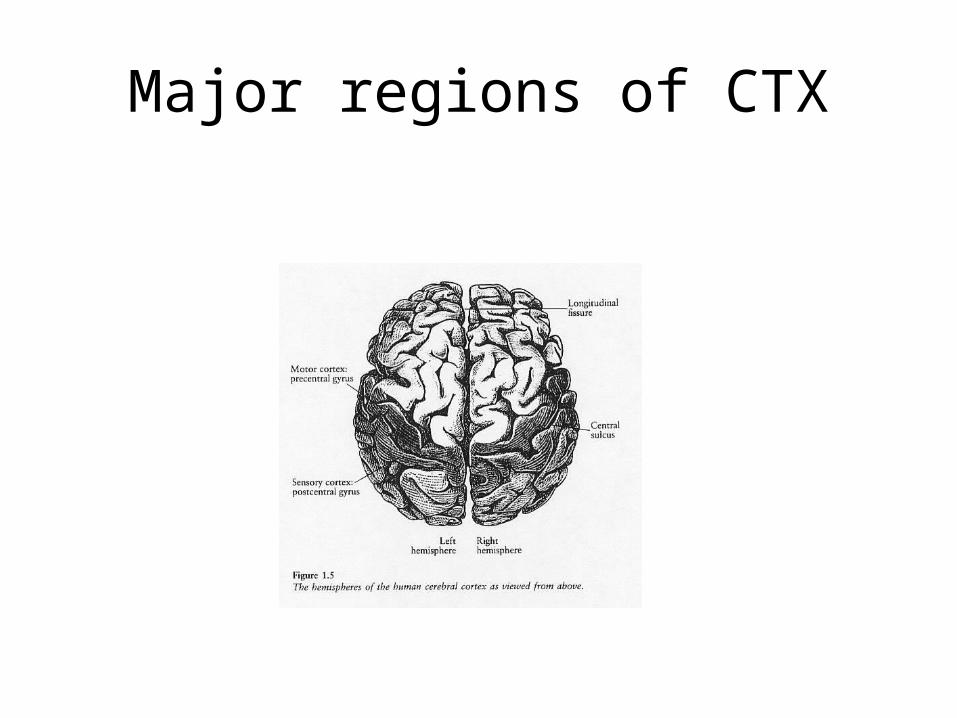
Major regions of CTX
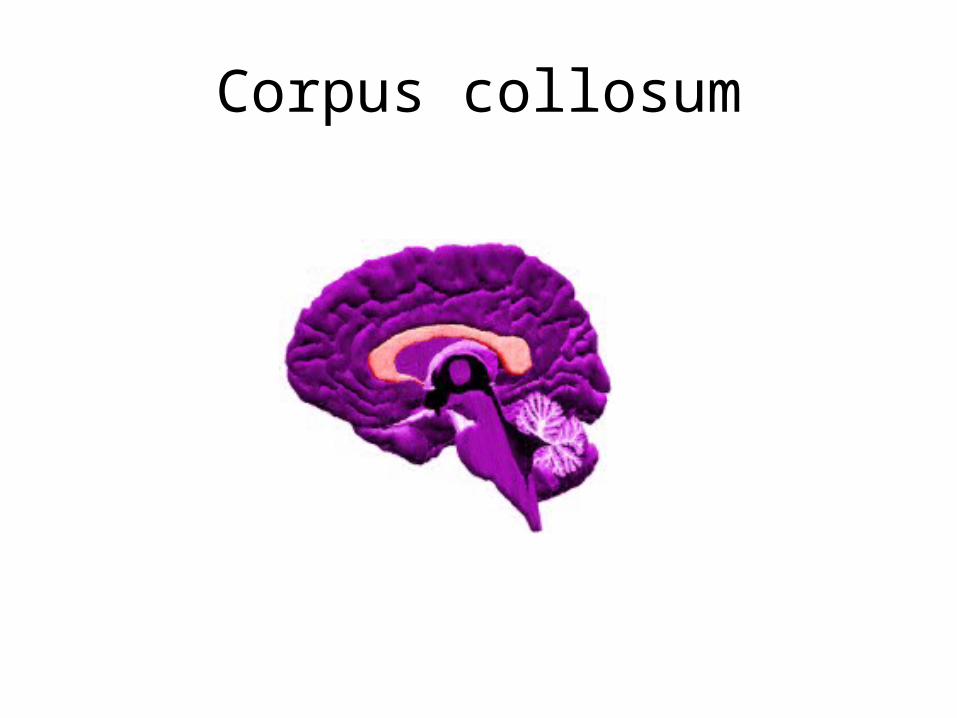
Corpus collosum
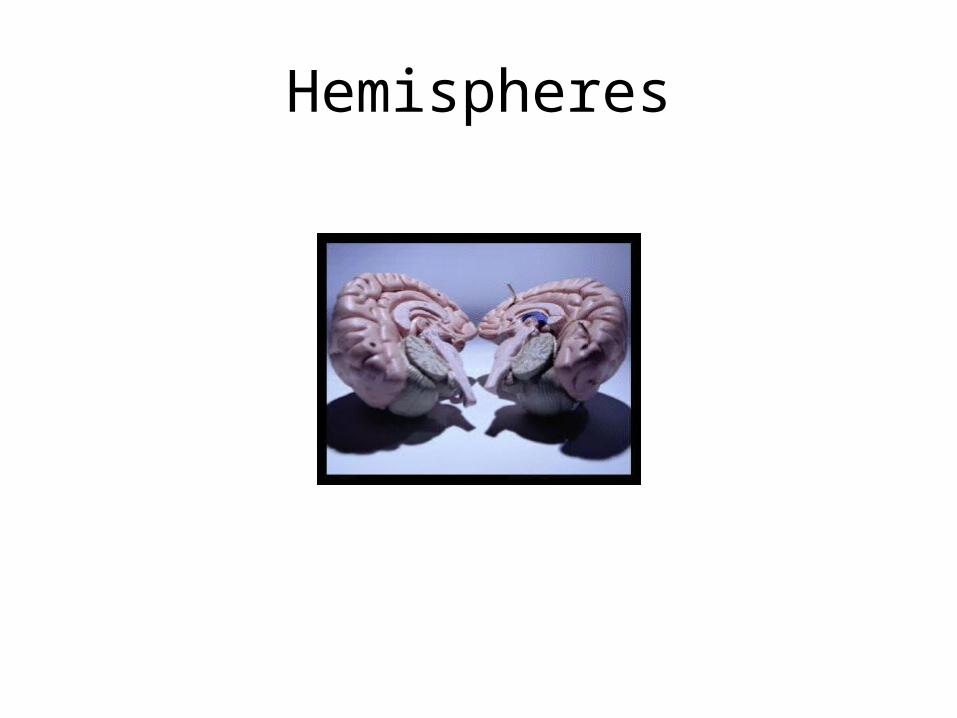
Hemispheres
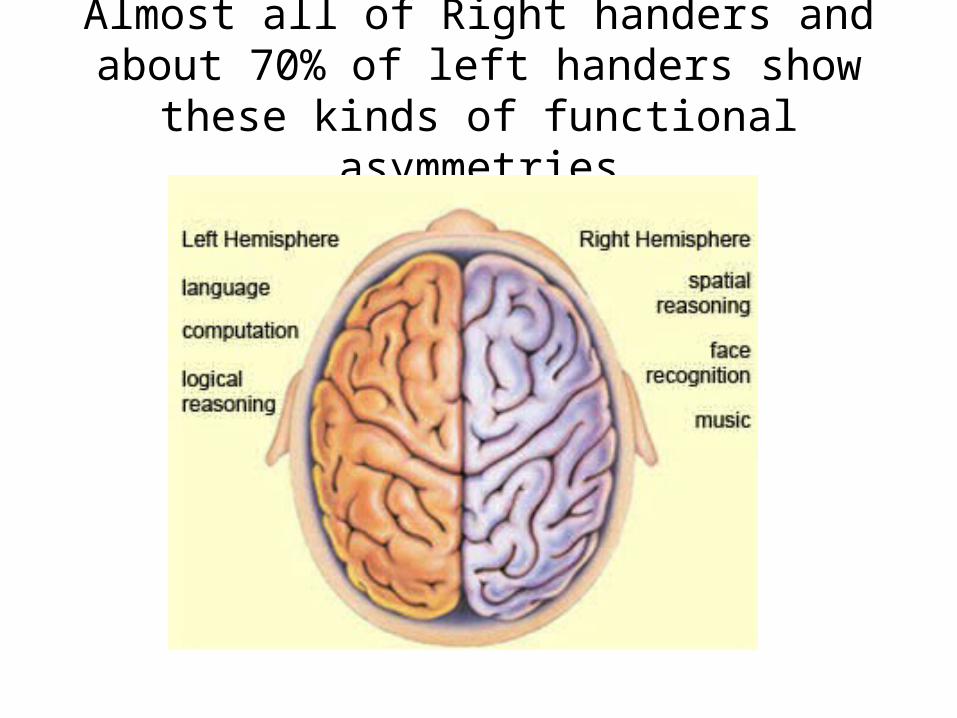
Almost all of Right handers and about 70% of left handers show these kinds of
functional asymmetries
Emotion and the cerebral hemispheres
• Catastrophic (left hemisphere cortex lost)
• vs
• indifferent reactions (right cortex lost) to cortical damage
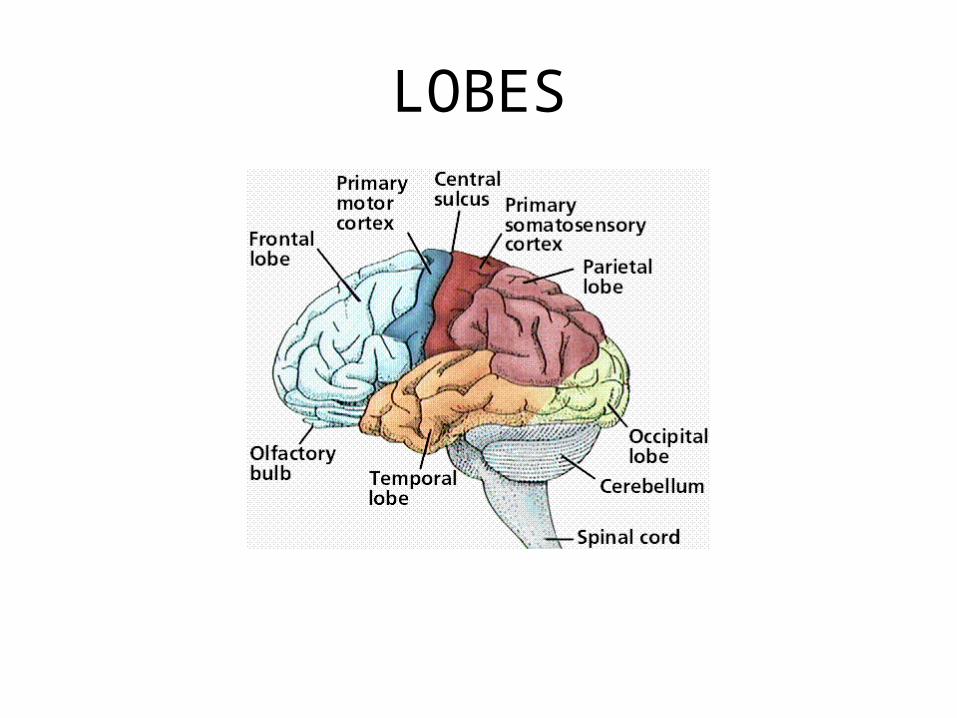
LOBES
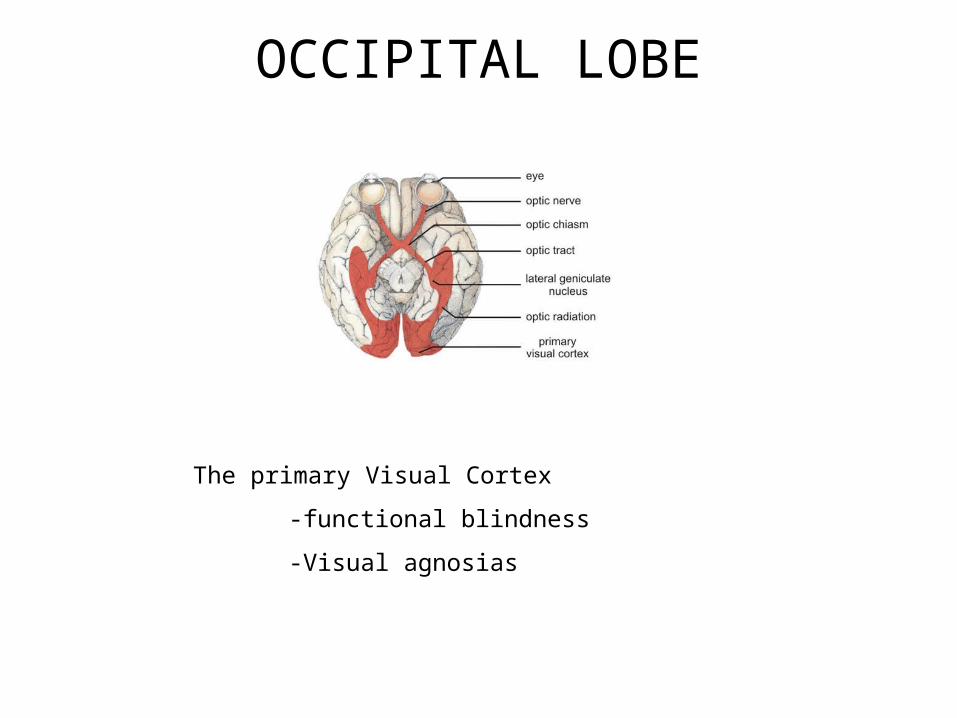
OCCIPITAL LOBE
The primary Visual Cortex
-functional blindness
-Visual agnosias
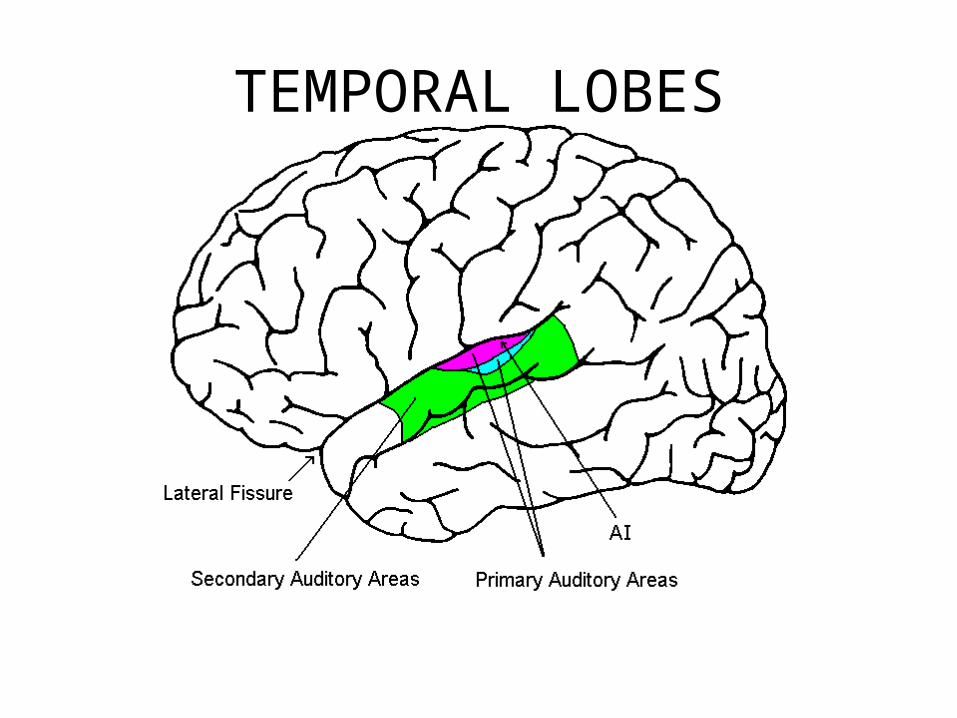
TEMPORAL LOBES
Temporal lobe damage may result in any number of problems
including any of these syndromes
Functional deafness-Anomias
-Aprosodia-Werniches’ syndrome
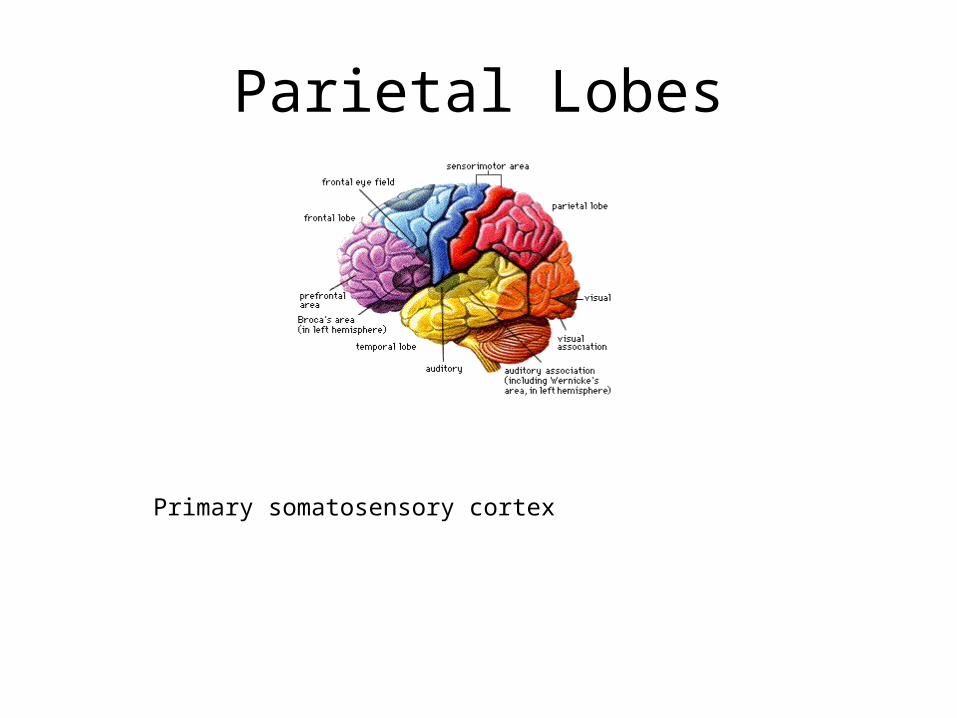
Parietal Lobes
Primary somatosensory cortex
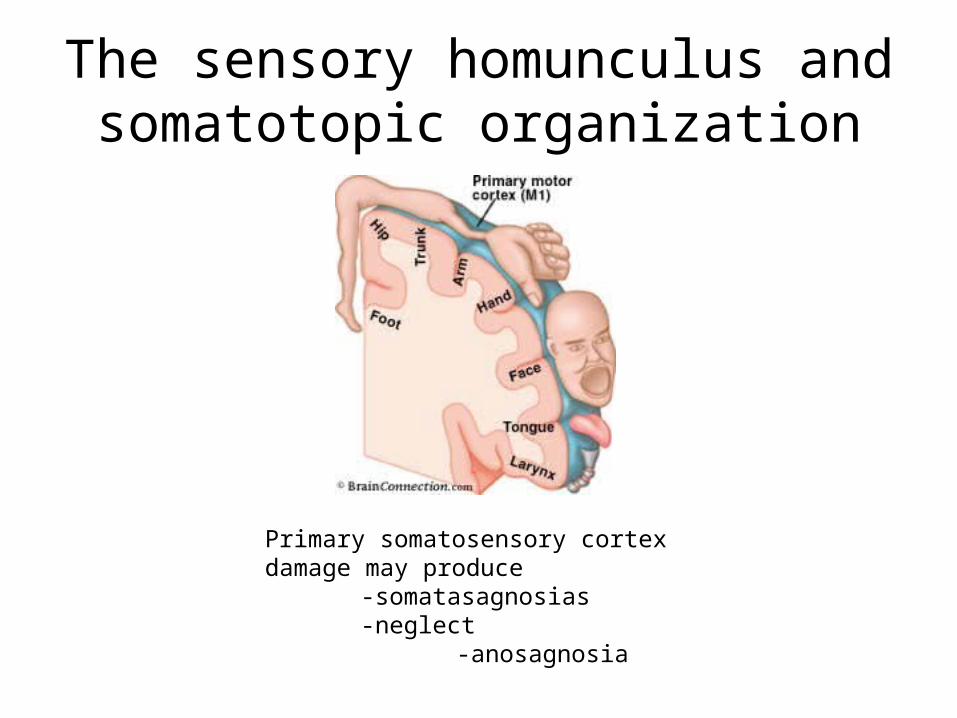
The sensory homunculus and somatotopic organization
Primary somatosensory cortex damage may produce
-somatasagnosias-neglect
-anosagnosia
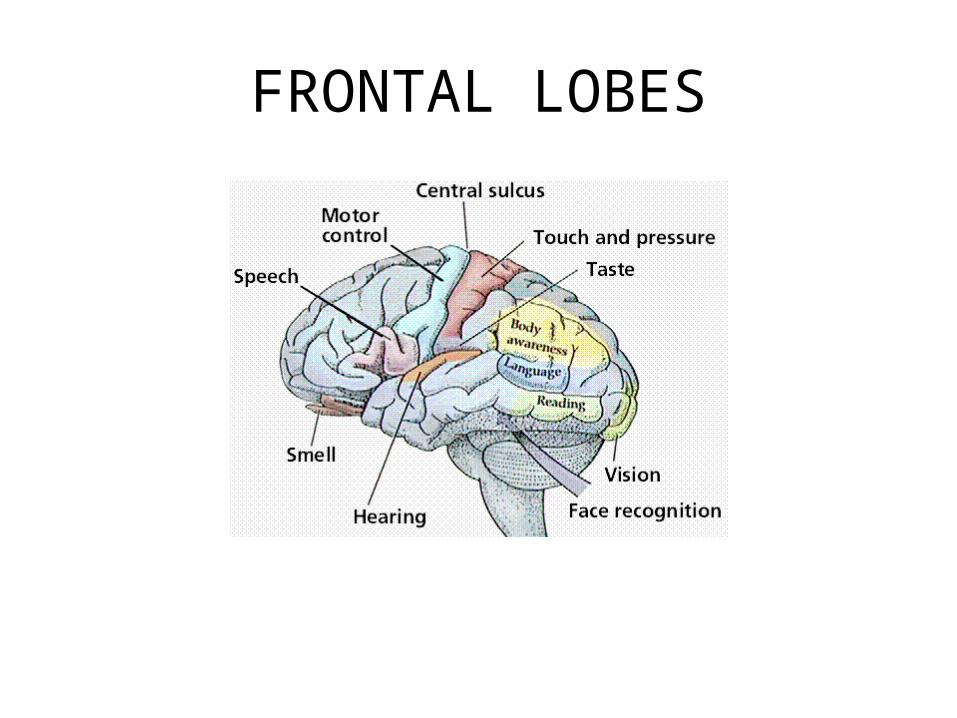
FRONTAL LOBES
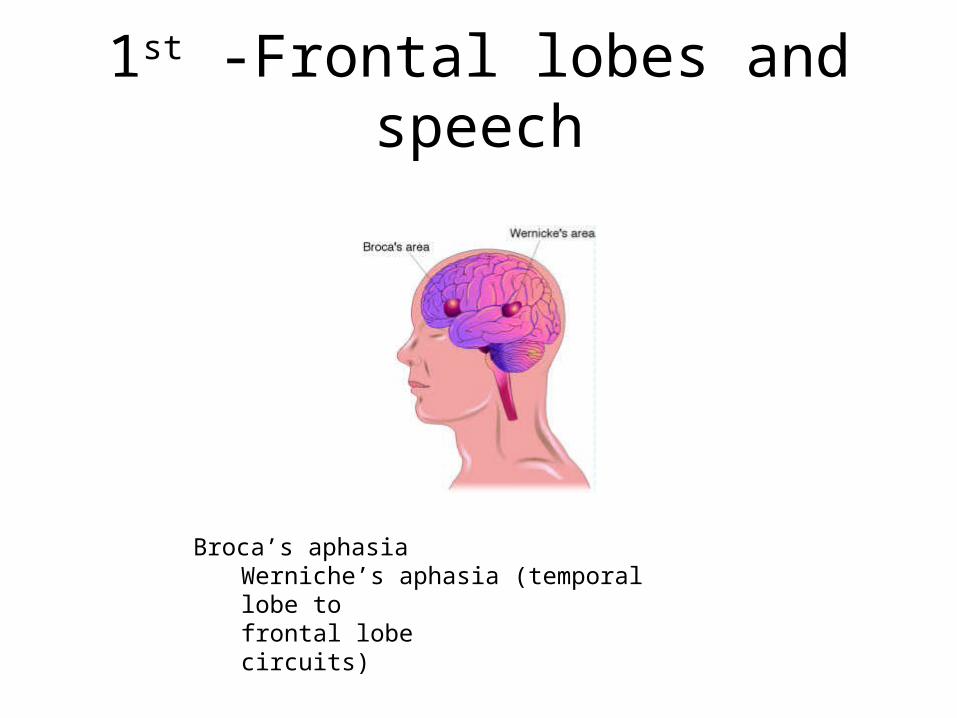
1st -Frontal lobes and speech
Broca’s aphasiaWerniche’s aphasia (temporal lobe to
frontal lobe circuits)
What about the rest of the frontal lobe?-Phineas Gage
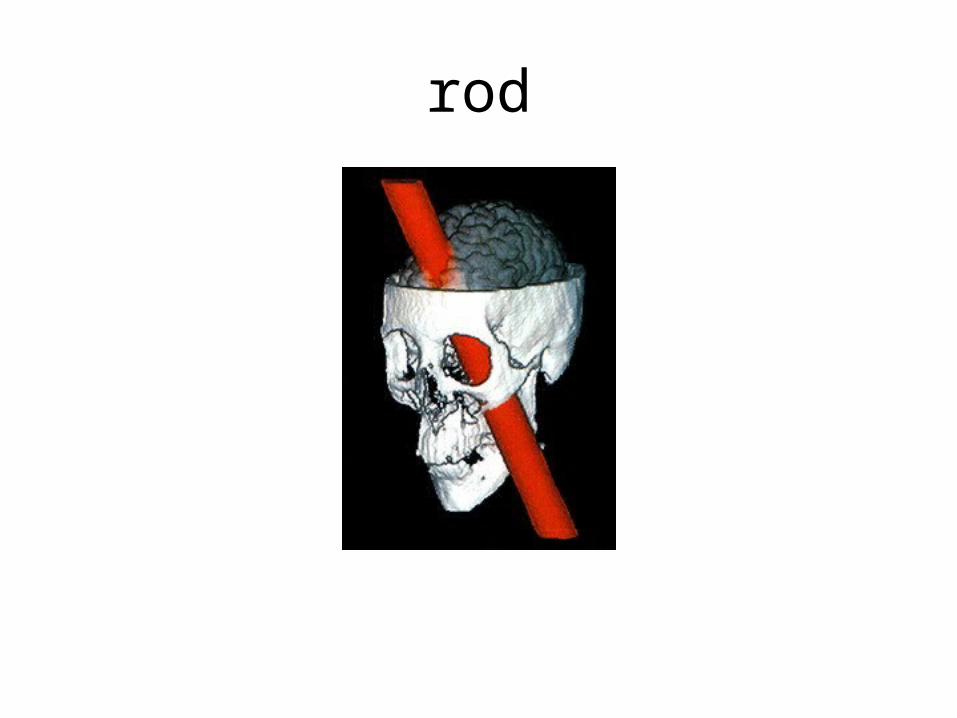
rod
Brain-Based Theory of Emotions• Frontal lobes
– influence people’s conscious emotional feelings and ability to act in planned ways based on feelings (e.g., effects of prefrontal lobotomy)
– Some scientists contend that the prefrontal cortex normally acts as a brake that can suppress urges or impulses by communicating with other brain areas that mediate fear and aggression, such as the amygdala.
left frontal lobe may be most involved in processing positive emotionsright frontal lobe involved with negative emotions
ParietalFrontal
Occipital
Temporal
General frontal Lobe functionsAwareness
Judgment , planning and anticipation
Personality
Conscious emotions
Organization and mental flexibility
Attention and concentration
Initiation and inhibition of behavior
Testing frontal lobe functionWCST

Inhibition of subcortical impulses; hypofrontality
Hypofrontality and aggression• Several recent examinations of violent individuals also jibe with this idea.
For example, a brain imaging study of murderers found evidence that, on average, the prefrontal cortex as well as some deeper brain areas, including the amygdala, functioned abnormally. Impaired activity also appeared in a preliminary examination of psychopaths with extensive criminal records who, as a group, generally are prone to violence.
• In another recent study, researchers examined a group of men who were registered at temporary employment agencies and lived in the general population, but were assessed as violent and antisocial. Compared with normal individuals, on average, the violent men had smaller prefrontal areas. Researchers also recently tested another group of people assessed to have moderately violent and impulsive personalities. Again the prefrontal cortex and aggression circuit seem to play a role. The "hot heads" performed poorly on several tasks thought to involve the front brain area, as well as the amygdala, compared with their more even-keeled counterparts, according to preliminary results.