Embed Size (px)
Citation preview
RESEARCH ARTICLE
The Consequences of Consanguinity on the Rates ofMalformations and Major Medical Conditions at Birthand in Early Childhood in Inbred PopulationsJo€el Zlotogora1* and Stavit A. Shalev2
1Department of Community Genetic, Public Health Services, and Hebrew University, Jerusalem, Israel2Genetic Institute, Ha’Emek Medical Center, Afula, and Rappaport School of Medicine, Technion, Haifa, Israel
Received 25 April 2010; Accepted 12 May 2010
The rate of malformations and major medical conditions in early
childhood was analyzed in a single village according to the degree
of relationship between the parents. In the village, 70–80% of the
marriages are between descendants of the founders and therefore
consanguineous. In the period 1992–2003, in 99 of 2,610
children, a major malformation was diagnosed at birth and seven
additional fetuses were aborted because of a severe malforma-
tion. A significant medical condition was diagnosed in 38 addi-
tional children in early childhood. The total of 144 cases with
malformations or a major medical condition represented
5.52% (95% CI: 4.64–6.4) of the live births. Three
malformations/disorders were relatively frequent: Down syn-
drome, esophageal atresia, and profound deafness. The rate of
malformations and significant medical conditions was 7.77% (95
CI: 5.68–9.86) when the parents were first cousins and 3.63%
(95% CI: 2.11–5.15) when they were not related (P¼ 0.002,
Fisher’s exact test). Offspring of parents that were second cousins
or closer but less than first cousin had a risk that was similar to
the one of offspring of couples that were more distantly related.
We propose therefore, that in inbred populations, all the couples
that are not related as first cousins but in which the spouses
are both descendants of the founders should be considered as
related. The high prevalence of profound deafness in the village is
due to mutations in the Connexin 26 gene, while the relatively
high frequency of Down syndrome is not explained by maternal
age only. � 2010 Wiley-Liss, Inc.
Key words: consanguinity; inbred populations; malformations;
deafness; esophageal atresia; Down syndrome
INTRODUCTION
Consanguineous marriages have always been frequent and in the
last century much emphasis was focused on their possible adverse
health outcomes [Bittles and Black, 2010]. However, many of the
studies that have been conducted on consanguinity have often
lacked adequate controls [Khlat and Khoury, 1991]. Therefore, the
present study was performed in a well-defined population, a
Muslim village in Israel of 11,000 inhabitants founded about
300 years ago by few ancestors. In a 10 km distance from the village
is located a large Arab town as well as several other Arab villages.
This village was chosen at random in 1995 as the site for a pilot
project implementing genetic counseling in the Arab community.
Since the beginning of the project the data have been entered into a
pedigree computer program (Reunion, Leister Production, Inc.)
and are constantly updated being used for clinical and for research
purposes [Zlotogora et al., 2002, 2006].
The purpose of the study was to determine the rate of malfor-
mations and major medical conditions in early childhood accord-
ing to the degree of relationship between the parents.
SUBJECTS AND METHODS
For the analysis we included all couples in which at least one spouse
was born in the village and still living in it at the time of the study.
The year of birth of the women was used as a reference since it is
the date most frequently recorded in the database. It was
almost always possible to determine the exact relationship between
the spouses when both partners were descended from the
*Correspondence to:
Jo€el Zlotogora, Department of Community Genetics, Building 67 Sheba
Medical Center, Ramat Gan, Israel. E-mail: [email protected]
Published online 15 July 2010 in Wiley InterScience
(www.interscience.wiley.com)
DOI 10.1002/ajmg.a.33537
How to Cite this Article:Zlotogora J, Shalev SA. 2010. The
consequences of consanguinity on the rates of
malformations and major medical conditions
at birth and in early childhood in inbred
populations.
Am J Med Genet Part A 152A:2023–2028.
� 2010 Wiley-Liss, Inc. 2023
founders. In this patriarchal community, a woman is almost always
living with her husband family. When a man marries a woman
from another village, the couple generally lives in the husband’s
village.
The database was initiated by gathering information through
personal interviews with families in the village, and is updated
yearly since 1992, including all the live births in the village and
malformations diagnosed at birth with data from the Israeli registry
of malformations in live newborn infants [Zlotogora et al., 2003].
The medical information was collected from the family physicians
in the village, and the Genetic Institute of Ha’Emek Hospital. In
recent years, the data obtained in genetic consultations are con-
stantly updated. Because of the geographical location of the village
and the personal links which have developed since the beginning of
the project between the authors and the physicians working in the
village, almost all the referrals from the village are to the Genetic
Institute either for genetic counseling or genetic and prenatal tests.
The data were analyzed in 2009 in order to include diseases
appearing in the first 5 years of life; only children born before
2003 with major malformations and diseases leading to disability
were included in the study (Additional Information). To avoid the
bias of multiply affected pregnancies in families with a known
inherited syndrome or chromosomal aberration, recurrent dia-
gnoses leading to termination of pregnancy were not included in the
study (Additional Information).
RESULTS
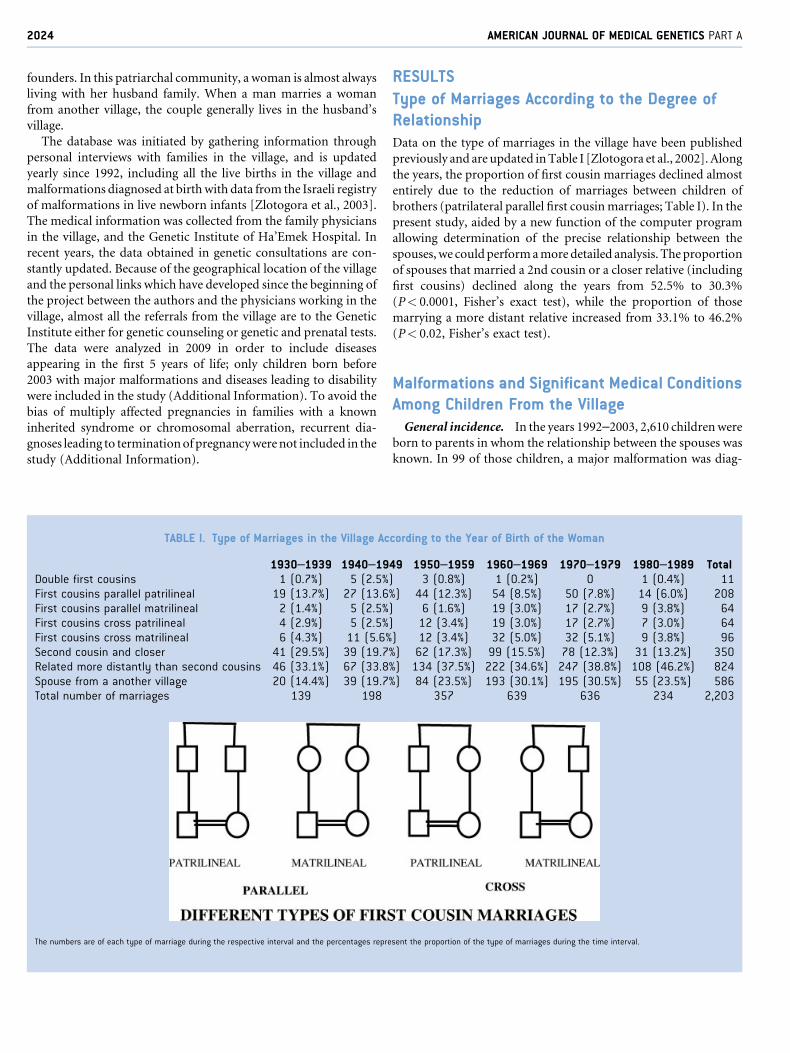
Type of Marriages According to the Degree ofRelationshipData on the type of marriages in the village have been published
previously and are updated in Table I [Zlotogora et al., 2002]. Along
the years, the proportion of first cousin marriages declined almost
entirely due to the reduction of marriages between children of
brothers (patrilateral parallel first cousin marriages; Table I). In the
present study, aided by a new function of the computer program
allowing determination of the precise relationship between the
spouses, we could perform a more detailed analysis. The proportion
of spouses that married a 2nd cousin or a closer relative (including
first cousins) declined along the years from 52.5% to 30.3%
(P< 0.0001, Fisher’s exact test), while the proportion of those
marrying a more distant relative increased from 33.1% to 46.2%
(P< 0.02, Fisher’s exact test).
Malformations and Significant Medical ConditionsAmong Children From the Village
General incidence. In the years 1992–2003, 2,610 children were
born to parents in whom the relationship between the spouses was
known. In 99 of those children, a major malformation was diag-
TABLE I. Type of Marriages in the Village According to the Year of Birth of the Woman
1930–1939 1940–1949 1950–1959 1960–1969 1970–1979 1980–1989 TotalDouble first cousins 1 (0.7%) 5 (2.5%) 3 (0.8%) 1 (0.2%) 0 1 (0.4%) 11First cousins parallel patrilineal 19 (13.7%) 27 (13.6%) 44 (12.3%) 54 (8.5%) 50 (7.8%) 14 (6.0%) 208First cousins parallel matrilineal 2 (1.4%) 5 (2.5%) 6 (1.6%) 19 (3.0%) 17 (2.7%) 9 (3.8%) 64First cousins cross patrilineal 4 (2.9%) 5 (2.5%) 12 (3.4%) 19 (3.0%) 17 (2.7%) 7 (3.0%) 64First cousins cross matrilineal 6 (4.3%) 11 (5.6%) 12 (3.4%) 32 (5.0%) 32 (5.1%) 9 (3.8%) 96Second cousin and closer 41 (29.5%) 39 (19.7%) 62 (17.3%) 99 (15.5%) 78 (12.3%) 31 (13.2%) 350Related more distantly than second cousins 46 (33.1%) 67 (33.8%) 134 (37.5%) 222 (34.6%) 247 (38.8%) 108 (46.2%) 824Spouse from a another village 20 (14.4%) 39 (19.7%) 84 (23.5%) 193 (30.1%) 195 (30.5%) 55 (23.5%) 586Total number of marriages 139 198 357 639 636 234 2,203
The numbers are of each type of marriage during the respective interval and the percentages represent the proportion of the type of marriages during the time interval.
2024 AMERICAN JOURNAL OF MEDICAL GENETICS PART A
nosed at birth, and seven additional fetuses were aborted because of
a severe malformation. A significant medical condition was dia-
gnosed in 38 additional older children. Profound deafness and
mental retardation were the most frequent diagnoses in those
children (Additional Information). During the years 1992–2003,
144 cases with malformations or major medical conditions were
diagnosed (5.52% live births; 95% CI: 4.64–6.4). Among those
cases, three conditions were particularly frequent: Down syndrome,
esophageal atresia, and profound deafness.
Down syndrome was diagnosed in 10 instances (0.38% live births;
95% CI: 0.14–0.62), 8 being trisomy 21 and 2 unbalanced trans-
locations. Among these 10 cases, in 3 the parents were first cousins,
in 4 they were more distantly related, and in the other 3 the parents
were not related. Two Down syndrome children whose parents were
first cousins presented each with a major malformation: Hirsch-
prung disease in one and esophageal atresia in the other.
Esophageal atresia was diagnosed in 11 cases (including one child
with Down syndrome, see above; 0.42% live births; 95% CI:
0.17–0.67). In two of the families the parents were first cousins,
and in the other six they were more distantly related.
Isolated profound deafness was diagnosed in eight of the children
(0.31% live births; 95% CI: 0.1–0.52) all as a result of mutations in
the Connexin 26 gene. One child was born to first cousin parents,
and the other seven were born to distantly related parents.
Incidence of malformations and significant medical conditions
according to the relationships between the parents
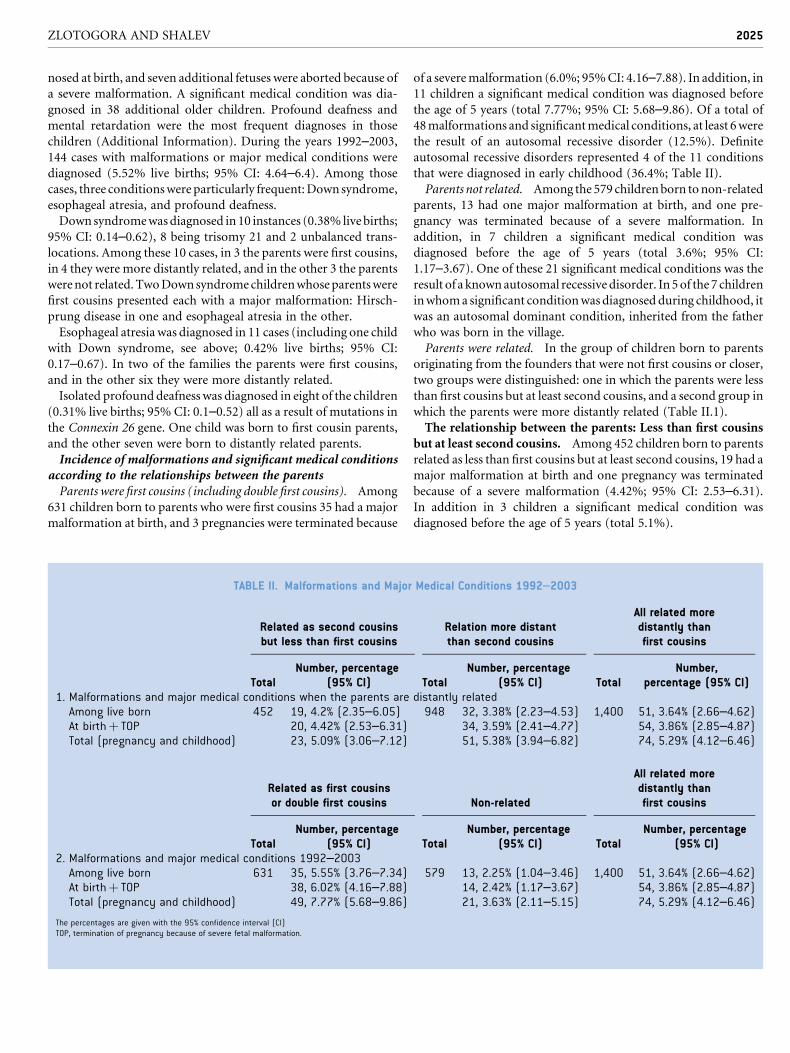
Parents were first cousins (including double first cousins). Among
631 children born to parents who were first cousins 35 had a major
malformation at birth, and 3 pregnancies were terminated because
of a severe malformation (6.0%; 95% CI: 4.16–7.88). In addition, in
11 children a significant medical condition was diagnosed before
the age of 5 years (total 7.77%; 95% CI: 5.68–9.86). Of a total of
48 malformations and significant medical conditions, at least 6 were
the result of an autosomal recessive disorder (12.5%). Definite
autosomal recessive disorders represented 4 of the 11 conditions
that were diagnosed in early childhood (36.4%; Table II).
Parents not related. Among the 579 children born to non-related
parents, 13 had one major malformation at birth, and one pre-
gnancy was terminated because of a severe malformation. In
addition, in 7 children a significant medical condition was
diagnosed before the age of 5 years (total 3.6%; 95% CI:
1.17–3.67). One of these 21 significant medical conditions was the
result of a known autosomal recessive disorder. In 5 of the 7 children
in whom a significant condition was diagnosed during childhood, it
was an autosomal dominant condition, inherited from the father
who was born in the village.
Parents were related. In the group of children born to parents
originating from the founders that were not first cousins or closer,
two groups were distinguished: one in which the parents were less
than first cousins but at least second cousins, and a second group in
which the parents were more distantly related (Table II.1).
The relationship between the parents: Less than first cousins
but at least second cousins. Among 452 children born to parents
related as less than first cousins but at least second cousins, 19 had a
major malformation at birth and one pregnancy was terminated
because of a severe malformation (4.42%; 95% CI: 2.53–6.31).
In addition in 3 children a significant medical condition was
diagnosed before the age of 5 years (total 5.1%).
TABLE II. Malformations and Major Medical Conditions 1992–2003
Related as second cousinsbut less than first cousins
Relation more distantthan second cousins
All related moredistantly thanfirst cousins
TotalNumber, percentage
(95% CI) TotalNumber, percentage
(95% CI) TotalNumber,
percentage (95% CI)1. Malformations and major medical conditions when the parents are distantly related
Among live born 452 19, 4.2% (2.35–6.05) 948 32, 3.38% (2.23–4.53) 1,400 51, 3.64% (2.66–4.62)At birth þ TOP 20, 4.42% (2.53–6.31) 34, 3.59% (2.41–4.77) 54, 3.86% (2.85–4.87)Total (pregnancy and childhood) 23, 5.09% (3.06–7.12) 51, 5.38% (3.94–6.82) 74, 5.29% (4.12–6.46)
Related as first cousinsor double first cousins Non-related
All related moredistantly thanfirst cousins
TotalNumber, percentage
(95% CI) TotalNumber, percentage
(95% CI) TotalNumber, percentage
(95% CI)2. Malformations and major medical conditions 1992–2003
Among live born 631 35, 5.55% (3.76–7.34) 579 13, 2.25% (1.04–3.46) 1,400 51, 3.64% (2.66–4.62)At birth þ TOP 38, 6.02% (4.16–7.88) 14, 2.42% (1.17–3.67) 54, 3.86% (2.85–4.87)Total (pregnancy and childhood) 49, 7.77% (5.68–9.86) 21, 3.63% (2.11–5.15) 74, 5.29% (4.12–6.46)
The percentages are given with the 95% confidence interval (CI)TOP, termination of pregnancy because of severe fetal malformation.
ZLOTOGORA AND SHALEV 2025
The relationship between the parents was less than second
cousins. Among 948 children born to parents more remotely
related than second cousins, 32 had a major malformation at
birth and two pregnancies were terminated because of a severe
malformation (total 3.59%; 95% CI: 2.41–4.77). In 17 children, a
significant medical condition was diagnosed before the age of
5 years (total 5.38%).
Since for each of the parameters examined the differences among
the groups were not significant, the analysis was also performed as
one group referred to as ‘‘distantly related’’ (Table II.2). Of a total of
1,400 children born to parents distantly related, 74 malformations
and significant medical conditions were diagnosed (5.29%; 95% CI:
4.12–6.46), and at least 17 were the result of an autosomal recessive
disorder (22.7%). Definite autosomal recessive disorders repre-
sented 9 of the 20 conditions that were diagnosed in the first 5 years
of life (45%).
DISCUSSION
While modernization led to significant changes in marital oppor-
tunities, marriages within the community remain the preference
and in the village studied proportions of inter-village marriages
remained in the same range representing approximately 20–30% of
the total [Zlotogora et al., 2002]. Among Muslims consanguineous
marriages are traditional, even though not recommended in Islam.
In the Arab world, the most frequent type of consanguineous
marriages has been between first cousins and among those,
marriages between children of brothers (patrilineal parallel) have
been the preferred type of marriages for various reasons, one of
which being the avoidance of parceling the lands of the family. With
the disappearance of the advantages of this specific type of
marriages in the village, a significant decline in the total proportion
of patrilineal parallel first cousin marriages was observed, from
13.6% to 6%. The rate of the other three types of first cousin
marriages remained in a similar range during the years (Table I). A
similar decline in the prevalence of first cousin marriages has also
been observed in other Arab populations of the region [Jaber et al.,
2000; Hamamy et al., 2005; Sharkia et al., 2008; Assaf and Khawaja,
2009]. These changes are probably due to various factors, mostly the
internal changes in the society but also education programs,
including media campaigns particularly emphasizing the medical
risks of first cousin marriages. On the other hand, other advantages
of consanguinity such as the possibility for both spouses to keep
living near their close relatives, staying in the village in which they
were born, are also achieved in rural societies by marriages between
distant relatives. Indeed, in the period of the survey, while the
proportion of marriages between close relatives (2nd cousins and
closer) in the village declined from 52.5% to 30.3% (P< 0.0001,
Fisher’s exact test), the rates of distantly related marriages rose from
33.1% to 46.2% (P< 0.02, Fisher’s exact test).
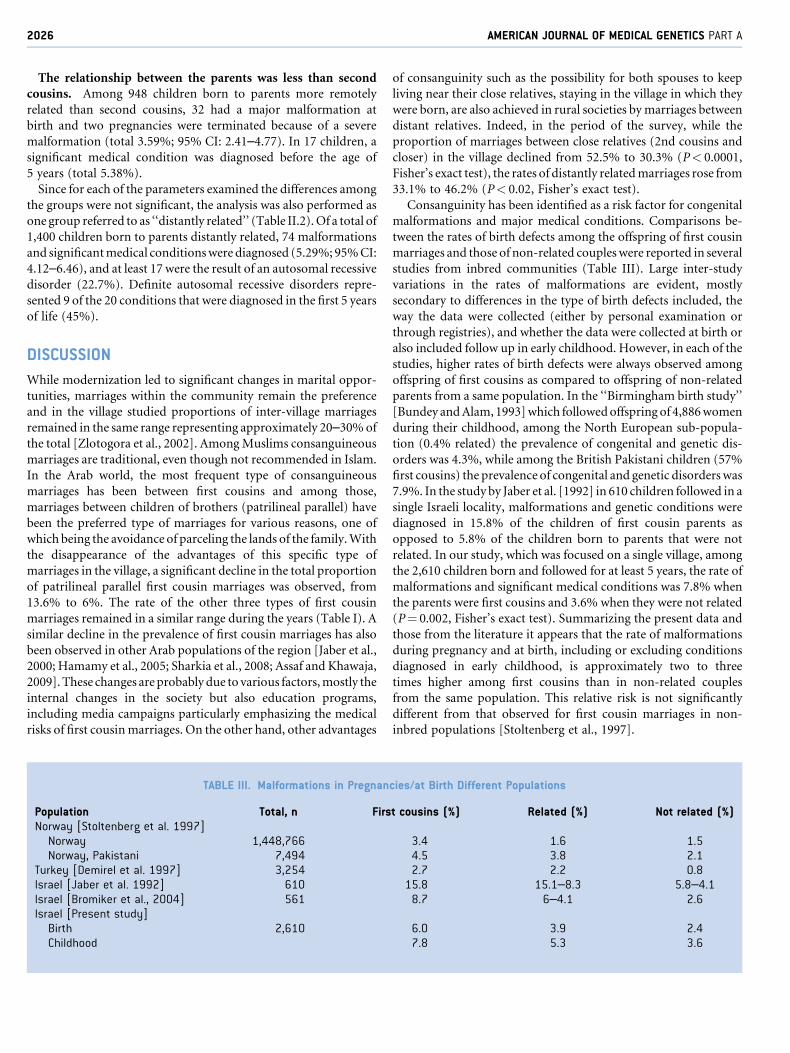
Consanguinity has been identified as a risk factor for congenital
malformations and major medical conditions. Comparisons be-
tween the rates of birth defects among the offspring of first cousin
marriages and those of non-related couples were reported in several
studies from inbred communities (Table III). Large inter-study
variations in the rates of malformations are evident, mostly
secondary to differences in the type of birth defects included, the
way the data were collected (either by personal examination or
through registries), and whether the data were collected at birth or
also included follow up in early childhood. However, in each of the
studies, higher rates of birth defects were always observed among
offspring of first cousins as compared to offspring of non-related
parents from a same population. In the ‘‘Birmingham birth study’’
[Bundey and Alam, 1993] which followed offspring of 4,886 women
during their childhood, among the North European sub-popula-
tion (0.4% related) the prevalence of congenital and genetic dis-
orders was 4.3%, while among the British Pakistani children (57%
first cousins) the prevalence of congenital and genetic disorders was
7.9%. In the study by Jaber et al. [1992] in 610 children followed in a
single Israeli locality, malformations and genetic conditions were
diagnosed in 15.8% of the children of first cousin parents as
opposed to 5.8% of the children born to parents that were not
related. In our study, which was focused on a single village, among
the 2,610 children born and followed for at least 5 years, the rate of
malformations and significant medical conditions was 7.8% when
the parents were first cousins and 3.6% when they were not related
(P¼ 0.002, Fisher’s exact test). Summarizing the present data and
those from the literature it appears that the rate of malformations
during pregnancy and at birth, including or excluding conditions
diagnosed in early childhood, is approximately two to three
times higher among first cousins than in non-related couples
from the same population. This relative risk is not significantly
different from that observed for first cousin marriages in non-
inbred populations [Stoltenberg et al., 1997].
TABLE III. Malformations in Pregnancies/at Birth Different Populations
Population Total, n First cousins (%) Related (%) Not related (%)Norway [Stoltenberg et al. 1997]
Norway 1,448,766 3.4 1.6 1.5Norway, Pakistani 7,494 4.5 3.8 2.1
Turkey [Demirel et al. 1997] 3,254 2.7 2.2 0.8Israel [Jaber et al. 1992] 610 15.8 15.1–8.3 5.8–4.1Israel [Bromiker et al., 2004] 561 8.7 6–4.1 2.6Israel [Present study]
Birth 2,610 6.0 3.9 2.4Childhood 7.8 5.3 3.6
2026 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

However, as discussed above, in recent decades several inbred
populations have shown a tendency of progressive decline in first
cousin marriages rates, concomitant to a rise of marriages between
more distantly related individuals [Jaber et al., 2000; Hamamy et al.,
2005; Sharkia et al., 2008]. Therefore, another important piece of
information is the estimate of the risk conferred by marriages
between more distantly related individuals in inbred communities.
In a large population study performed in the Norwegian registry
focusing on stillbirths and live births at gestational age of 16 weeks
or more among 1,448,766 children born to Norwegians without a
recent immigration background, the rate of malformations was
3.4% when the parents were first cousins, 1.6% when the parent
were distantly related and 1.5% when the parents were not related.
In the same study, among Norwegian Pakistani couples the rate of
malformations at birth was 4.5% for first cousins, 3.8% for distantly
related spouses, and 2.1% when the parents were not related
[Stoltenberg et al., 1997]. The observation that in an inbred
community such as the Norwegian Pakistani as opposed to non-
inbred populations, the risk at birth for couples that are distantly
related is higher than in non-related couples was confirmed here
and in several other studies [Jaber et al., 1992; Zlotogora, 2002].
However, while individuals are considered to be related only when
they are second cousin or closer, We have shown that in an inbred
community, offspring of parents that are second cousins or closer
but less than first cousin have a similar risk as offspring of parents
more distantly related (5.1% and 5.5%, respectively; P¼ 0.8). This
observation is explained by the fact that in inbred populations,
marriages within the community occurred from generation to
generation increasing the genetic resemblance between individuals
as demonstrated by the calculation of the inbreeding coefficients or
using molecular data [Bittles and Egerbladh, 2005; Woods et al.,
2006]. We propose therefore, that in inbred populations, all the
couples that are not related as first cousins but in which the spouses
are both descendants of the founders should be considered as
related. The main implication is for genetic counseling since those
couples have a higher risk than non-related couples even though
the difference is not statistically significant (5.3% and 3.6%,
respectively; P¼ 0.133).
In the period of the study, three disorders were particularly
frequent in the village, raising in each case the question of a possible
genetic cause. Indeed, all the cases of isolated profound deafness in
the village were due to recessive mutations in the gene for Connexin
26. While an increased proportion of first cousin marriages is
usually observed among the parents of individuals affected with
autosomal recessive diseases, this was not the case for connexin 26
related deafness in the village. The observation that the rate of first
cousin marriages among the parents of deaf children was not
different from the one of all the couples in the village is explained
by a 17% general carrier frequency of mutations in the connexin
26 gene in this village [Zlotogora et al., 2006]. It is that high
frequency of the mutants alleles that makes each couple in which
both spouses were born in the village at an almost similar risk
whatever the relationship. Similar observations were made for other
frequent diseases as for instance as sickle-cell anemia in Saudi
Arabia [El Mouzan et al., 2008].
The frequency of esophageal atresia between the years 1992 and
2003 was much higher in the village (0.42% live births; 95% CI:
0.17–0.67) than the one observed in the general Israeli Muslim
population (0.02% live births; 95% CI: 0.01–0.03) [Zlotogora et al.,
2003]. The possibility of a syndromic form of the malformation was
raised but was not supported after clinical re-examination of the
affected children. Since there were no instances of esophageal
atresia among the 2,114 live births in the 6 following years
(2004–2009), it may be that this was an unexplained transient
cluster of cases.
Down syndrome was the third disorder relatively frequent in the
village during the period of the study—0.38% live births (95% CI:
0.14–0.62) as opposed to 0.16% live births (95% CI: 0.12–0.20) in
the general Muslim population [Zlotogora et al., 2010]. Most of the
cases were trisomy 21, while the mean age of the women at birth in
the village was not different from the one in the Israeli Muslim
population. In Kuwait, a relatively high frequency of Down syn-
drome was linked to consanguinity as an independent factor and
the relative risk was approximately four times higher for closely
related than for non-related parents [Alfi et al., 1980; Farag and
Teebi, 1988]. However, this observation was not confirmed in other
studies [Roberts et al., 1991; Hook, 1992]. We did not observe an
increased consanguinity rate among the parents of affected cases,
and in none of the families reported here there was a recurrence of
Down syndrome or any other trisomy. In the 6-year period of
following our present study for which we have complete data
(2004–2009), trisomy 21 was diagnosed in six other instances out
of 2,114 live births (0.28%; 95% CI: 0.05–0.51). This continuing
high incidence of Down syndrome raises the possibility that it may
be a true phenomenon prompting us to continue to investigate the
existence of possible genetic factors.
REFERENCES
Alfi OS, Chang R, Azen SP. 1980. Evidence for genetic control of non-disjunction in man. Am J Hum Genet 32:477–483.
Assaf S, Khawaja M. 2009. Consanguinity trends and correlates in thePalestinian Territories. J Biosoc Sci 41:107–124. [Epub 2008 Jun 13].
Bittles AH, Black ML. 2010. Consanguinity, human evolution and complexdiseases PNA. 107:1779–1786. Epub 2009 Sep 23.
Bittles AH, Egerbladh I. 2005. The influence of past endogamy andconsanguinity on genetic disorders in northern Sweden. Ann Hum Genet69:549–558.
Bromiker R, Glam-Baruch M, Gofin R, Hammerman C, Amitai Y. 2004.Association of parental consanguinity with congenital malformationsamong Arab newborns in Jerusalem. Clin Genet 66:63–66.
Bundey S, Alam H. 1993. A five-year prospective study of the health ofchildren in different ethnic groups, with particular reference to the effectof inbreeding. Eur J Hum Genet 1:206–219.
Demirel S, Kaplano�glu N, Acar A, Bodur S, Paydak F. 1997. The frequencyof consanguinity in Konya, Turkey, and its medical effects. Genet Couns8:295–301.
El Mouzan MI, Al Salloum AA, Al Herbish AS, Qurachi MM, Al OmarAA. 2008. Consanguinity and major genetic disorders in Saudi children:A community-based cross-sectional study. Ann Saudi Med 28:169–173.
Farag TI, Teebi AS. 1988. Possible evidence for genetic predisposition tonondisjunction in man. J Med Genet 25:136–137.
ZLOTOGORA AND SHALEV 2027

Hamamy H, Jamhawi L, Al-Darawsheh J, Ajlouni K. 2005. Consanguineousmarriages in Jordan: Why is the rate changing with time? Clin Genet67:511–516.
Hook EB. 1992. Consanguinity and Down syndrome in the ShetlandIslands. Hum Genet 89:462.
Jaber L, Merlob P, Bu X, Rotter JI, Shohat M. 1992. Marked parentalconsanguinity as a cause for increased major malformations in an IsraeliArab community. Am J Med Genet 44:1–6.
Jaber L, Halpern GJ, Shohat T. 2000. Trends in the frequencies of consan-guineous marriages in the Israeli Arab community. Clin Genet 58:106–110.
Khlat M, Khoury M. 1991. Inbreeding and diseases: Demographic, genetic,and epidemiologic perspectives. Epidemiol Rev 13:28–41.
Roberts DF, Roberts MJ, Johnston AW. 1991. Genetic epidemiology ofDown’s syndrome in Shetland. Hum Genet 87:57–60.
Sharkia R, Zaid M, Athamna A, Cohen D, Azem A, Zalan A. 2008. Thechanging pattern of consanguinity in a selected region of the Israeli Arabcommunity. Am J Hum Biol 20:72–77.
Stoltenberg C, Magnus P, Lie RT, Daltveit AK, Irgens LM. 1997. Birth defectsand parental consanguinity in Norway. Am J Epidemiol 145:439–448.
Woods CG, Cox J, Springell K, Hampshire DJ, Mohamed MD, McKibbinM, Stern R, Raymond FL, Sandford R, Malik Sharif S, Karbani G, AhmedM, Bond J, Clayton D, Inglehearn CF. 2006. Quantification of homozy-gosity in consanguineous individuals with autosomal recessive disease.Am J Hum Genet 78:889–896. [Epub 2006 Mar 21].
Zlotogora J. 2002. What is the birth defect risk associated with consan-guineous marriages. Am J Med Genet 109:70–71.
Zlotogora J, Habiballa H, Odatalla A, Barges S. 2002. Changing familystructure in a modernizing society: A study of marriage patterns in asingle Muslim village in Israel. Am J Human Biol 14:680–682.
Zlotogora J, Haklai Z, Rotem N, Georgi M, Berlovitz I, Leventhal A, AmitaiY. 2003. Relative prevalence of malformations at birth amongdifferent religious communities in Israel. Am J Med Genet Part A122A:59–62.
Zlotogora J, Carasquillo M, Barges S, Shalev SA, Hujerat Y, Chakravarti A.2006. High incidence of deafness in an isolated community from threefrequent Connexin 26 mutations. Genetic Testing 10:40–43.
Zlotogora J, Haklai Z, Rotem N, Georgi M, Rubin L. 2010. The impact ofprenatal diagnosis and termination of pregnancy on the relative inci-dence of malformations at birth among Jews and Muslim Arabs in Israel.Isr Med Assoc J (in press).
2028 AMERICAN JOURNAL OF MEDICAL GENETICS PART A