Embed Size (px)
DESCRIPTION
Â
Citation preview

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
The correlation Between Vitamin D Metabolite Levels With Relapse
Rate And Disability In Multiple Sclerosis
Hussein Mohamad Hussein1, Nabiel Abdel
* E-mail of the corresponding author
Abstract
Background: Multiple sclerosis is a major cause of disability in young a
protective effect of Vitamin D on multiple sclerosis is supported by the reduced risk associated with sun exposure and use of
Vitamin D supplements. Moreover, high circulating levels of Vitamin D have be
Objectives: The aim of this study is to clarify the relationship between vitamin D metabolite level and disability and relapse rate
in multiple sclerosis. Methods: Fifty four Multiple sclerosis
sex and same geographical areas,35 (64.8 %) patients were with relapsing remitting type,9 (16.6 %) patients were primary
progressive type and 10 (18.6 %) patients were secondary progressive typ
demyelinated neurological diseases including 18 with chronic inflammatory demyelinating polyneuropathy, 6 were Gillian Barrie
syndrome and 4 were acute demyelinating encephalomyelitis, and the remaining
multiple sclerosis patients and controls are subjected to assessment of 25(OH) D serum level by RIA.
statistically significant difference between patients and controls, also very high stat
patients, and disability and relapse rate .
Conclusion: There is an important role of vitamin D in outcome of multiple sclerosis and the relapsing rate of the relapsing
remitting type
Keywords: multiple sclerosis,vitamin D,relapse,disability
1. Introduction
In the Multiple sclerosis (MS) is a major caus
MS are high because of its long duration, the early loss of productivity, the need for assistance in activities of daily
living and the use of immunomodulatory treatments and multidisciplina
considered a hereditary disease. However, a number of
developing the disease.2,3 Although genetic susceptibility explains the clustering of MS within families, it cannot
fully explain the geographical variations in MS frequency and the changes in risk that occur with migrat
support the action of strong environmental factors. Different environmental factors, both of infectious and non
infectious origin have been proposed as risk factors for MS,
immunomodulator, and several studies have shown that administration of the biologically active 1,
25-dihydroxyvitamin D prevents experimental autoimmune encephalomyelitis (EAE) onset and progression in mice.
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
87
The correlation Between Vitamin D Metabolite Levels With Relapse
Rate And Disability In Multiple Sclerosis
Nabiel Abdel-Hakeem Metwally2, Mahmoud Mohamad Hassan
Hashish3
1. Al-Azhar school of medicine,Cairo.
2. Al-Azhar school of medicine, Assuit.
3. National research centre, Cairo.
mail of the corresponding author : [email protected]
Multiple sclerosis is a major cause of disability in young adults. Vitamin D is a potent
protective effect of Vitamin D on multiple sclerosis is supported by the reduced risk associated with sun exposure and use of
Vitamin D supplements. Moreover, high circulating levels of Vitamin D have been associated with lower risk of multiple sclerosis.
: The aim of this study is to clarify the relationship between vitamin D metabolite level and disability and relapse rate
Fifty four Multiple sclerosis patients fulfilling McDonald's criteria and 70 controls matched in age,
sex and same geographical areas,35 (64.8 %) patients were with relapsing remitting type,9 (16.6 %) patients were primary
progressive type and 10 (18.6 %) patients were secondary progressive type. For the control group, 28 of them were with non
demyelinated neurological diseases including 18 with chronic inflammatory demyelinating polyneuropathy, 6 were Gillian Barrie
syndrome and 4 were acute demyelinating encephalomyelitis, and the remaining forty two were apparently healthy controls. All
multiple sclerosis patients and controls are subjected to assessment of 25(OH) D serum level by RIA.
statistically significant difference between patients and controls, also very high statistically significant negative correlation in all
patients, and disability and relapse rate .
There is an important role of vitamin D in outcome of multiple sclerosis and the relapsing rate of the relapsing
multiple sclerosis,vitamin D,relapse,disability
Multiple sclerosis (MS) is a major cause of disability in young adults. The social costs associated with
MS are high because of its long duration, the early loss of productivity, the need for assistance in activities of daily
living and the use of immunomodulatory treatments and multidisciplinary health care.
disease. However, a number of genetic variations have been shown to increase the risk of
Although genetic susceptibility explains the clustering of MS within families, it cannot
fully explain the geographical variations in MS frequency and the changes in risk that occur with migrat
support the action of strong environmental factors. Different environmental factors, both of infectious and non
infectious origin have been proposed as risk factors for MS,4 among these, vitamin D status, as vitamin D is a potent
, and several studies have shown that administration of the biologically active 1,
dihydroxyvitamin D prevents experimental autoimmune encephalomyelitis (EAE) onset and progression in mice.
www.iiste.org
The correlation Between Vitamin D Metabolite Levels With Relapse
Rate And Disability In Multiple Sclerosis
, Mahmoud Mohamad Hassan2*, Adel Ferig Abu-Zed
Vitamin D is a potent immunomodulator and the
protective effect of Vitamin D on multiple sclerosis is supported by the reduced risk associated with sun exposure and use of
en associated with lower risk of multiple sclerosis.
: The aim of this study is to clarify the relationship between vitamin D metabolite level and disability and relapse rate
fulfilling McDonald's criteria and 70 controls matched in age,
sex and same geographical areas,35 (64.8 %) patients were with relapsing remitting type,9 (16.6 %) patients were primary
e. For the control group, 28 of them were with non-MS
demyelinated neurological diseases including 18 with chronic inflammatory demyelinating polyneuropathy, 6 were Gillian Barrie
forty two were apparently healthy controls. All
multiple sclerosis patients and controls are subjected to assessment of 25(OH) D serum level by RIA. Results: very high
istically significant negative correlation in all
patients, and disability and relapse rate .
There is an important role of vitamin D in outcome of multiple sclerosis and the relapsing rate of the relapsing
e of disability in young adults. The social costs associated with
MS are high because of its long duration, the early loss of productivity, the need for assistance in activities of daily
ry health care.1 Multiple sclerosis is not
been shown to increase the risk of
Although genetic susceptibility explains the clustering of MS within families, it cannot
fully explain the geographical variations in MS frequency and the changes in risk that occur with migration, which
support the action of strong environmental factors. Different environmental factors, both of infectious and non
among these, vitamin D status, as vitamin D is a potent
, and several studies have shown that administration of the biologically active 1,
dihydroxyvitamin D prevents experimental autoimmune encephalomyelitis (EAE) onset and progression in mice.

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
Also the protective effect of Vitamin D on multiple sclerosis i
exposure and use of Vitamin D supplements. Moreover, high circulating levels of Vitamin D have been associated
with lower risk of multiple sclerosis.
and the main MS-linked HLA-DRB1*1501 allele and evidence showing that vitamin D levels are significantly lower
in patients with MS as compared to controls. Direct genomic signaling by active vitamin D
through the vitamin D receptor (VDR), which is present in multiple cells of the immune system as well as in
neurons and glial cells in the human brain. Activation of the VDR by vitamin D stimulates a shift from
pro-inflammatory T-helper cell-1 (Th1) responses to anti
concentration of 25(OH) D is the best indicato
that obtained from food and supplements and has a fairly long circulating half
circulating 1,25(OH)2D is generally not a good indicator of vitamin D status
hours and serum concentrations are closely regulated by parathyroid hormone, calcium, and phosphate. Levels of
1,25(OH)2D do not typically decrease until vitamin D deficiency is severe.
2. Patients and Methods
According to line of treatment 43 (79.7 %) patients were treated by corticosteroids, 7 (13 %) patients treated
by disease modifying drugs other than corticosteroids, 3 (5.5 %) patients received combined treatment in the form of
corticosteroids and another disease modifying agent, and one (1.8 %) patient received no specific treatment. The
following patients were excluded from the study: Patients with decreased serum albumin, or receiving
anticonvulsants, those with advanced renal disease, mal
patients received vitamin D. The control were divided into 2 subgroups: (A) including 28 patients with demyelinting
neurological diseases other than MS including 18 patients with Chronic Inflammatory Demyelintin
Polyradiculoneuropathy (CIDP), with a mean duration ± SD of
neurophysiological studies and no significantly related cervical MRI findings, 6 patients with Gillian Barrie
Syndrome (GBS), with a mean duration ±
neurophysiologic studies and CSF findings and 4 patients with ADEM Acute Disseminated Encephalomyelitis
(ADEM), with a mean duration ± SD ( 4.5 ± 1.3) months, diagnosed clinically and supported b
subgroup (B) including 42 healthy subjects. The patients were subjected to a full medical history taking, full
neurological examination, and assessment of the patient disability state using the Expanded Disability Status Scale
(EDSS). All participants (cases and controls) were underwent CBC, liver and renal function tests, stool analysis,
serum albumin and assessment of the Serum vitamin D (25 hydroxyvitamin D) which was done using the
Radio-Immune-Assay (RIA) performed in the Hormone assay
relationship between serum level of 25 hydroxyvitamin D and clinical MS severity, disability as expressed by
EDSS-score and MS subtypes. Data were collected and statistically analyzed. Statistics were
Epi - info. Software, version 6.04. A word processing, data base and statistics program (WHO, 2001).
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
88
Also the protective effect of Vitamin D on multiple sclerosis is supported by the reduced risk associated with sun
exposure and use of Vitamin D supplements. Moreover, high circulating levels of Vitamin D have been associated
with lower risk of multiple sclerosis.5 Moreover, a newly identified gene-environment interac
DRB1*1501 allele and evidence showing that vitamin D levels are significantly lower
in patients with MS as compared to controls. Direct genomic signaling by active vitamin D
vitamin D receptor (VDR), which is present in multiple cells of the immune system as well as in
and glial cells in the human brain. Activation of the VDR by vitamin D stimulates a shift from
1 (Th1) responses to anti-inflammatory T-helper-2 (Th2) responses.
concentration of 25(OH) D is the best indicator of vitamin D status, it reflects vitamin D produced cutaneously and
that obtained from food and supplements and has a fairly long circulating half-life of 15 days. However, the
circulating 1,25(OH)2D is generally not a good indicator of vitamin D status because it has a short half
hours and serum concentrations are closely regulated by parathyroid hormone, calcium, and phosphate. Levels of
1,25(OH)2D do not typically decrease until vitamin D deficiency is severe.10,11
According to line of treatment 43 (79.7 %) patients were treated by corticosteroids, 7 (13 %) patients treated
by disease modifying drugs other than corticosteroids, 3 (5.5 %) patients received combined treatment in the form of
disease modifying agent, and one (1.8 %) patient received no specific treatment. The
following patients were excluded from the study: Patients with decreased serum albumin, or receiving
anticonvulsants, those with advanced renal disease, mal-absorption syndrome, end-stage liver disease, smoking, and
patients received vitamin D. The control were divided into 2 subgroups: (A) including 28 patients with demyelinting
neurological diseases other than MS including 18 patients with Chronic Inflammatory Demyelintin
Polyradiculoneuropathy (CIDP), with a mean duration ± SD of 4.2±0.9 year and the diagnosis confirmed by
neurophysiological studies and no significantly related cervical MRI findings, 6 patients with Gillian Barrie
Syndrome (GBS), with a mean duration ± SD of (5±1.3) week, diagnosed clinically and supported by
neurophysiologic studies and CSF findings and 4 patients with ADEM Acute Disseminated Encephalomyelitis
(ADEM), with a mean duration ± SD ( 4.5 ± 1.3) months, diagnosed clinically and supported b
subgroup (B) including 42 healthy subjects. The patients were subjected to a full medical history taking, full
neurological examination, and assessment of the patient disability state using the Expanded Disability Status Scale
participants (cases and controls) were underwent CBC, liver and renal function tests, stool analysis,
serum albumin and assessment of the Serum vitamin D (25 hydroxyvitamin D) which was done using the
Assay (RIA) performed in the Hormone assay unit, National Institute Center at Cairo to study the
relationship between serum level of 25 hydroxyvitamin D and clinical MS severity, disability as expressed by
score and MS subtypes. Data were collected and statistically analyzed. Statistics were
info. Software, version 6.04. A word processing, data base and statistics program (WHO, 2001).
www.iiste.org
s supported by the reduced risk associated with sun
exposure and use of Vitamin D supplements. Moreover, high circulating levels of Vitamin D have been associated
environment interaction between vitamin D
DRB1*1501 allele and evidence showing that vitamin D levels are significantly lower
in patients with MS as compared to controls. Direct genomic signaling by active vitamin D (1,25(OH)2) occurs
vitamin D receptor (VDR), which is present in multiple cells of the immune system as well as in
and glial cells in the human brain. Activation of the VDR by vitamin D stimulates a shift from
2 (Th2) responses.5,6,7,8,9. Serum
r of vitamin D status, it reflects vitamin D produced cutaneously and
life of 15 days. However, the
because it has a short half-life of 15
hours and serum concentrations are closely regulated by parathyroid hormone, calcium, and phosphate. Levels of
According to line of treatment 43 (79.7 %) patients were treated by corticosteroids, 7 (13 %) patients treated
by disease modifying drugs other than corticosteroids, 3 (5.5 %) patients received combined treatment in the form of
disease modifying agent, and one (1.8 %) patient received no specific treatment. The
following patients were excluded from the study: Patients with decreased serum albumin, or receiving
stage liver disease, smoking, and
patients received vitamin D. The control were divided into 2 subgroups: (A) including 28 patients with demyelinting
neurological diseases other than MS including 18 patients with Chronic Inflammatory Demyelinting
and the diagnosis confirmed by
neurophysiological studies and no significantly related cervical MRI findings, 6 patients with Gillian Barrie
SD of (5±1.3) week, diagnosed clinically and supported by
neurophysiologic studies and CSF findings and 4 patients with ADEM Acute Disseminated Encephalomyelitis
(ADEM), with a mean duration ± SD ( 4.5 ± 1.3) months, diagnosed clinically and supported by brain MRI, and
subgroup (B) including 42 healthy subjects. The patients were subjected to a full medical history taking, full
neurological examination, and assessment of the patient disability state using the Expanded Disability Status Scale
participants (cases and controls) were underwent CBC, liver and renal function tests, stool analysis,
serum albumin and assessment of the Serum vitamin D (25 hydroxyvitamin D) which was done using the
unit, National Institute Center at Cairo to study the
relationship between serum level of 25 hydroxyvitamin D and clinical MS severity, disability as expressed by
score and MS subtypes. Data were collected and statistically analyzed. Statistics were done by computer using
info. Software, version 6.04. A word processing, data base and statistics program (WHO, 2001).

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
3. Results
In this study, regarding the 25(OH) D serum levels and gender of the patient
results showed in table (1):
Table (1): 25(OH) D serum levels and gender of the patients and controls
Case group
controls
Diseased
Healthy
Relation of 25(OH)D levels to sex difference appear to be with no statistical significance in both MS and control
groups, but with very high statistical significance in healthy control and be of low lev
There is a mild positive correlation (Correlation Coef= 0.1), between duration of illness in years and disease
severity as expressed by EDSS with no statistical significance, as shown in table (
Table (2): relation between duration of i
EDSSDisease duration
4.09±1.93.8±2.9
As regard comparison of 25(OH)D serum levels between case and control groups, the result showed in
table (3)
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
89
In this study, regarding the 25(OH) D serum levels and gender of the patients and controls, we found the
): 25(OH) D serum levels and gender of the patients and controls
Sex (OH)D mean ± SD
F 33 ± 21
M 34.3 ± 24.4,
F 54.1 ± 17.2
M 49.3 ± 19.7,
F 49.4 ± 11.4
M 86±11.4
Relation of 25(OH)D levels to sex difference appear to be with no statistical significance in both MS and control
groups, but with very high statistical significance in healthy control and be of low levels in females.
There is a mild positive correlation (Correlation Coef= 0.1), between duration of illness in years and disease
severity as expressed by EDSS with no statistical significance, as shown in table (2):
): relation between duration of illness in MS and EDSS
Correlation Coef. EDSS
0.1 4.09±1.9
As regard comparison of 25(OH)D serum levels between case and control groups, the result showed in
www.iiste.org
s and controls, we found the
P value
0.8
0.5
0.000
Relation of 25(OH)D levels to sex difference appear to be with no statistical significance in both MS and control
els in females.
There is a mild positive correlation (Correlation Coef= 0.1), between duration of illness in years and disease
P value
0.45
As regard comparison of 25(OH)D serum levels between case and control groups, the result showed in

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
Table (3): The serum level of 25(OH
Very high statistical significance between the patient and control groups and appear to be lower in case group.
The comparison of 25(OH)D levels and status in both case and control groups subtypes, the results showed in
table (4).
Table (4):25(OH)D serum level and status
Su
btyp
es
gro
up t
ype/
/ Ite
m
Total
Patient group
(MS)
RRMS
PPMS
SPMS
Total
Diseased control
CIDP
GBS
ADEM
Diseased control, 25(OH)D , Mean
Comparative group
P value
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
90
The serum level of 25(OH)D in the case and control groups.
al significance between the patient and control groups and appear to be lower in case group.
The comparison of 25(OH)D levels and status in both case and control groups subtypes, the results showed in
25(OH)D serum level and status in different groups
25(OH) D status:
P v
alue
25 (
OH
)
Mea
n±S
D
num
ber
deficient
21
0.0
16
33.3±21.7 54
10 39.3±23.6 35
6 19.6±7.4 9
5 25.2±14.6 10
0.000
P
0
0.0
00
52.7±17.7 28
0 59.5±1.8 18
0 42.7±10.7 6
0 78.4±11.1 4
P
Patient group (MS)
25(OH)D , Mean ± SD: 33.3 ± 21.7
Healthy control, 25(OH)D , Mean ± SD: 59.9
± 21.4
Diseased control, 25(OH)D , Mean
± SD: 52.7 ± 17.7
0.0000.000
www.iiste.org
al significance between the patient and control groups and appear to be lower in case group.
The comparison of 25(OH)D levels and status in both case and control groups subtypes, the results showed in
25(OH) D status:
Norm.
Insuff.
11 22
11 14
0 3
0 5
0.000 0.000
14 14
4 14
6 0
4 0
0.7 ---
Healthy control, 25(OH)D , Mean ± SD: 59.9
± 21.4
0.000

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
Healthy control
For comparison of 25(OH)D levels between each MS subtypes and control group (healthy and diseased), the
results shown in table (5).
Table (5) Comparison of 25(OH)D levels in each MS subtypes to controls
RRMS (39.3±23.6)MS subtype
Diseased
control
Comp. group
52.7±17.7
25(OH)D,
mean ± SD
0.3
P value
Twenty five (OH)D levels is significantly lower in MS subtypes compared to the controls.
As regard comparison between 25(OH)D levels and MS severity assessed by EDSS, the results showed in table (
Table (6): 25(OH)D levels in relation to EDSS
No. of cases
EDSS, Mean ± SD
25(OH)D Mean ± SD
Very high significant negative relation between 25(OH)D serum levels and
score
In MS group, RRMS subtype, with 19 patient in relapse and 16 patient in remission, the comparison between
25(OH)D levels in patients during relapse and those during remission, table (
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
91
0
59.9±21.4
42
0.000
P
For comparison of 25(OH)D levels between each MS subtypes and control group (healthy and diseased), the
) Comparison of 25(OH)D levels in each MS subtypes to controls:
SPMS (25.2±14.6)PPMS (19.6±7.4) MS (39.3±23.6)
Diseased
control
Healthy
control
Diseased
control
Healthy
control
52.7±17.7
59.9±21.4
52.7±17.7
59.9±21.4
0.0002
0.0001
0.0001
0.0001
Twenty five (OH)D levels is significantly lower in MS subtypes compared to the controls.
As regard comparison between 25(OH)D levels and MS severity assessed by EDSS, the results showed in table (
): 25(OH)D levels in relation to EDSS
25 (46.3%) ≥
4
29 (53.7%)
<4
6±1.2 2.5±0.5
15±4.9 47±14.3
Very high significant negative relation between 25(OH)D serum levels and disease severity as expressed in EDSS
In MS group, RRMS subtype, with 19 patient in relapse and 16 patient in remission, the comparison between
25(OH)D levels in patients during relapse and those during remission, table (7).
www.iiste.org
20 22
For comparison of 25(OH)D levels between each MS subtypes and control group (healthy and diseased), the
SPMS (25.2±14.6)
Healthy control Diseased
control
59.9±21.4 52.7±17.7
0.0001 0.0002
Twenty five (OH)D levels is significantly lower in MS subtypes compared to the controls.
As regard comparison between 25(OH)D levels and MS severity assessed by EDSS, the results showed in table (6).
P value
0.000
0.000
disease severity as expressed in EDSS
In MS group, RRMS subtype, with 19 patient in relapse and 16 patient in remission, the comparison between

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
Table (7): 25(OH)D levels during relapse and remission
Total (35)
No. of cases
39.3±23.6
25(OH)D
Mean ± SD
The serum levels of 25(OH)D is significantly lower during relapse than remis
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
92
): 25(OH)D levels during relapse and remission
Remission (n=16) Relapse (n= 19)
31.4±20.9
29.5±23.6
The serum levels of 25(OH)D is significantly lower during relapse than remission.
www.iiste.org
P value
0.005

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
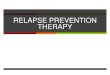
Figure (1): correlation between MS duration
and EDSS
There is mild positive correlation (P=0.45),
between duration of illness in years and disease
severity assessed by EDSS, with no statistical
significance (P=0.45).
Figure (3): correlation between 25(OH) D
levels and age of diseased controls.
There is a strong negative correlations between
vitamin D levels and age of participants, with a
very high statistical significance (P=0.000).
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
93
Figure (1): correlation between MS duration
There is mild positive correlation (P=0.45),
between duration of illness in years and disease
severity assessed by EDSS, with no statistical
etween 25(OH) D
levels and age of diseased controls.
There is a strong negative correlations between
vitamin D levels and age of participants, with a
very high statistical significance (P=0.000).
Figure (2): correlation between 25(OH) D levels
and age of MS patients.
There is a negligible negative correlation between
vitamin D levels and age of participants, with no
statistical significance (P=0.8).
Figure (4): correlation between 25(OH) D levels
and age of healthy controls.
There is a strong negative correlatio
vitamin D levels and age of participants, with a
very high statistical significance (P=0.000).
www.iiste.org
Figure (2): correlation between 25(OH) D levels
and age of MS patients.
There is a negligible negative correlation between
vitamin D levels and age of participants, with no
Figure (4): correlation between 25(OH) D levels
and age of healthy controls.
There is a strong negative correlations between
vitamin D levels and age of participants, with a
very high statistical significance (P=0.000).

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
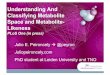
Fig. (5) Correlation between disease duration
in MS patients and EDSS.
There is a moderate positive correlation
between disease duration in MS patients and
disease severity assessed by EDSS, with statistical
insignificance (P=0.1).
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
94
Fig. (5) Correlation between disease duration
There is a moderate positive correlation
between disease duration in MS patients and
disease severity assessed by EDSS, with statistical
Fig. (6) Correlation between disease duration in
MS patients and D levels.
There is a moderate negative correlation between
disease duration in MS patients and vitamin D
serum levels, with statistical insignificance
(P=0.1)
www.iiste.org
Fig. (6) Correlation between disease duration in
There is a moderate negative correlation between
in MS patients and vitamin D
serum levels, with statistical insignificance

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
3.3Discussion
In the studied subjects the patients were including 39 female with 25(OH)D mean ± SD of 33 ± 21, and 15 male
with 25(OH)D mean ± SD of 34.3 ± 24.4, t
in females than in males. In healthy controls the 25(OH)D levels were less in females than in males. These results are
in agreement with El-Ghoneimy, et al
between female and male, and not in agreement with the study of
found that women with MS had significantly higher 25(OH) concentrations than men with MS. In the studied
patients, the 25(OH)D serum level was lower than that of the controls, these results are in concordance with the study
of Correale et al5 who found that, MS population had lower 25(OH) D than controls, and in concordance with the
study of Lucas et al17 and the study of
low 25(OH)D levels than controls. However the study of Kragt et al
(OH) D and MS in women, also the study of Barnes et al
women with MS, but in our study we found that 25 vitamin D deficiency was evident in both women and men.
Regarding to diseases subtypes, 25(OH)D deficiency was more evident in PPMS, compared to SPMS and RRMS,
these results are in accordance with Smolders et al
significantly lower in the progressive forms of
disagreement with Correale et al5 who found no signific
patients with healthy controls, but in our study we found that 25(OH)D levels were more deficient in PPMS than
other MS subtypes and controls. The serum level of 25(OH)D in the studied patients in relat
determined by EDSS scale score, there was a very high significant negative correlation in all MS patients, and was
being more evident in PPMS and RRMS. These results are in accordance with
and van der Mei et al21 who found that, lower levels of 25(OH) were associated with higher EDSS and the study of
Smolders, et al7 who found that, 25(OH)D concentrations were inversely associated with disease severity Score.
These results are disagree with the study of El
correlation between 25(OH)D level and disease severity, as assessed by EDSS, but in our study we found that, a very
high statistically significant negative correlation between 25(OH)D level and disease severity, as assessed by EDSS,
this may be due to exclusion of vitamin D medicated patients in our study. There was a very significant negative
correlation between the 25(OH)D serum levels and the relapse rate. This relation is in consistent with the study
Smolders et al7 and Smolders22 who found that, Serum 25(OH) D levels were associated inversely with relapse rate,
also the 25(OH)D serum levels are low during relapse than in remission, these results are consistent with the study of
Correale et al5 who found that, significantly lower levels of both vitamin D metabolites 25(OH)D in patients during
exacerbation than patients during remission. Also our results were in accordance with SoiluHanninen
that 25(OH) D serum levels were s
remission.
5. Conclusion
The serum levels of 25(OH) D are lower in MS patients with a negative correlation when compared to the severity of the disease and to the relapsing rate in t
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
95
In the studied subjects the patients were including 39 female with 25(OH)D mean ± SD of 33 ± 21, and 15 male
with 25(OH)D mean ± SD of 34.3 ± 24.4, there was no significant sex difference ,while in the diseased it was high
in females than in males. In healthy controls the 25(OH)D levels were less in females than in males. These results are
Ghoneimy, et al14 who found that no statistically significant difference in vitamin D level
between female and male, and not in agreement with the study of Dam et al15 and the stu
found that women with MS had significantly higher 25(OH) concentrations than men with MS. In the studied
patients, the 25(OH)D serum level was lower than that of the controls, these results are in concordance with the study
who found that, MS population had lower 25(OH) D than controls, and in concordance with the
and the study of Lonergan et al18 who found that there was significantly more patients had
low 25(OH)D levels than controls. However the study of Kragt et al19 reported an inverse relationship between 25
(OH) D and MS in women, also the study of Barnes et al16 who found that, vitamin D level
women with MS, but in our study we found that 25 vitamin D deficiency was evident in both women and men.
Regarding to diseases subtypes, 25(OH)D deficiency was more evident in PPMS, compared to SPMS and RRMS,
ccordance with Smolders et al7 who found that circulating levels of 25(OH)D metabolites were
significantly lower in the progressive forms of MS when compared to RRMS. But our results were in partial
who found no significant difference when comparing 25(OH)D levels of PPMS
patients with healthy controls, but in our study we found that 25(OH)D levels were more deficient in PPMS than
other MS subtypes and controls. The serum level of 25(OH)D in the studied patients in relat
determined by EDSS scale score, there was a very high significant negative correlation in all MS patients, and was
being more evident in PPMS and RRMS. These results are in accordance with Bianca Weinstock
who found that, lower levels of 25(OH) were associated with higher EDSS and the study of
who found that, 25(OH)D concentrations were inversely associated with disease severity Score.
These results are disagree with the study of El-Ghoneimy14 who found that, there was no statistical
correlation between 25(OH)D level and disease severity, as assessed by EDSS, but in our study we found that, a very
high statistically significant negative correlation between 25(OH)D level and disease severity, as assessed by EDSS,
be due to exclusion of vitamin D medicated patients in our study. There was a very significant negative
correlation between the 25(OH)D serum levels and the relapse rate. This relation is in consistent with the study
who found that, Serum 25(OH) D levels were associated inversely with relapse rate,
also the 25(OH)D serum levels are low during relapse than in remission, these results are consistent with the study of
who found that, significantly lower levels of both vitamin D metabolites 25(OH)D in patients during
exacerbation than patients during remission. Also our results were in accordance with SoiluHanninen
that 25(OH) D serum levels were significantly lower during acute exacerbations when compared to periods of
The serum levels of 25(OH) D are lower in MS patients with a negative correlation when compared to the severity of the disease and to the relapsing rate in the relapsing remitting type.
www.iiste.org
In the studied subjects the patients were including 39 female with 25(OH)D mean ± SD of 33 ± 21, and 15 male
here was no significant sex difference ,while in the diseased it was high
in females than in males. In healthy controls the 25(OH)D levels were less in females than in males. These results are
stically significant difference in vitamin D level
and the study of Barnes et al16 who
found that women with MS had significantly higher 25(OH) concentrations than men with MS. In the studied
patients, the 25(OH)D serum level was lower than that of the controls, these results are in concordance with the study
who found that, MS population had lower 25(OH) D than controls, and in concordance with the
found that there was significantly more patients had
reported an inverse relationship between 25
who found that, vitamin D levels were higher only in
women with MS, but in our study we found that 25 vitamin D deficiency was evident in both women and men.
Regarding to diseases subtypes, 25(OH)D deficiency was more evident in PPMS, compared to SPMS and RRMS,
who found that circulating levels of 25(OH)D metabolites were
MS when compared to RRMS. But our results were in partial
ant difference when comparing 25(OH)D levels of PPMS
patients with healthy controls, but in our study we found that 25(OH)D levels were more deficient in PPMS than
other MS subtypes and controls. The serum level of 25(OH)D in the studied patients in relation to disease severity
determined by EDSS scale score, there was a very high significant negative correlation in all MS patients, and was
Bianca Weinstock-Guttman et al20
who found that, lower levels of 25(OH) were associated with higher EDSS and the study of
who found that, 25(OH)D concentrations were inversely associated with disease severity Score.
who found that, there was no statistically significant
correlation between 25(OH)D level and disease severity, as assessed by EDSS, but in our study we found that, a very
high statistically significant negative correlation between 25(OH)D level and disease severity, as assessed by EDSS,
be due to exclusion of vitamin D medicated patients in our study. There was a very significant negative
correlation between the 25(OH)D serum levels and the relapse rate. This relation is in consistent with the study
who found that, Serum 25(OH) D levels were associated inversely with relapse rate,
also the 25(OH)D serum levels are low during relapse than in remission, these results are consistent with the study of
who found that, significantly lower levels of both vitamin D metabolites 25(OH)D in patients during
exacerbation than patients during remission. Also our results were in accordance with SoiluHanninen22 who found
ignificantly lower during acute exacerbations when compared to periods of
The serum levels of 25(OH) D are lower in MS patients with a negative correlation when compared to the

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
References
1- Pugliatti M, Rosati G, Carton H and et al. the epidemiology of Multiple Sclerosis in Europe. Europian J of Neurol
2006; 13: 700-722.
2- Dyment DA, Ebers GC and Sadovnick AD. Genetics of Multiple Sclerosis. Lancet
3- Compaston A and Coles A. Multiple Sclerosis, Lancet 2002; 359 (9313): 1221
4- Marrie RA. Environmental risk factors in Multiple Sclerosis etiology. Lancet Neurol 2004; 3 (12), 709
5- Correale J, Ysrraelit MC and Gaitan MI. Immunomodulatory effects of vitamin D in Multiple Sclerosis. Brain
2009; 132: 1146-1160.
6- Eyles DW, Smith S, Kinobe R and et al. Distribution of vitamin D receptor and 1
brain. J Chemical Neuroanatomy 2005; 29: 21
7- Smolders J, Menheere P, Kessels A and et al. Association of Vitamin D metabolite levels with relapse rate and
disability in Multiple Sclerosis. Multiple Sclerosis 2008; 14(9): 1220
8- Handunnetthi L, Ramagopalan SV
2010; 74(23): 1905-10.
9- Holmoy T. Vitamin D status modulates the immune response to Epstein Barr virus: Synergistic effect o
in multiple sclerosis. Med Hypotheses 2008; 70(1): 66
10- Holick MF. Vitamin D deficiency. The New Engl J of Med 2007; 357(3):266
11- Josa M. Frischer, Stephan Bramow, Assunta Dal
neurodegeneration in Multiple Sclerosis brains. Brain 2009; 132 (5): 1175
12- McDonald WI, Compaston A and Edan G. Recommended diagnostic criteria for Multiple Sclerosis: guidelines
from the international panel on the diagnosis of Multiple Scle
13- Kragt JJ, Thompson AJ, Montalban X
primary progressive MS. Neurology.
14- El-Ghoneimy AT, Gad AH, H, Samir H, et al. Contribution of Vitamin D to the Pathogenesis of Multiple Sclerosis
and its Effect on Bone. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery 2009; 46
15-Dam TTL, von Mühlen D and Barrett
physical function in older adults. Osteoporosis International
16- Barnes MS, Bonham MP, Robson PJ, et al. Assessment of 25
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
96
Pugliatti M, Rosati G, Carton H and et al. the epidemiology of Multiple Sclerosis in Europe. Europian J of Neurol
Dyment DA, Ebers GC and Sadovnick AD. Genetics of Multiple Sclerosis. Lancet Neurol 2004; 3 (92): 104
Compaston A and Coles A. Multiple Sclerosis, Lancet 2002; 359 (9313): 1221-1231.
Marrie RA. Environmental risk factors in Multiple Sclerosis etiology. Lancet Neurol 2004; 3 (12), 709
d Gaitan MI. Immunomodulatory effects of vitamin D in Multiple Sclerosis. Brain
Eyles DW, Smith S, Kinobe R and et al. Distribution of vitamin D receptor and 1-alpha hydroxylase in human
brain. J Chemical Neuroanatomy 2005; 29: 21-30.
Smolders J, Menheere P, Kessels A and et al. Association of Vitamin D metabolite levels with relapse rate and
disability in Multiple Sclerosis. Multiple Sclerosis 2008; 14(9): 1220-1224.
Ramagopalan SV and Ebers GC. Multiple sclerosis, vitamin D, and HLA
Holmoy T. Vitamin D status modulates the immune response to Epstein Barr virus: Synergistic effect o
in multiple sclerosis. Med Hypotheses 2008; 70(1): 66-69.
Holick MF. Vitamin D deficiency. The New Engl J of Med 2007; 357(3):266-281.
Josa M. Frischer, Stephan Bramow, Assunta Dal-Bianco and et al. the relation between inflammation
neurodegeneration in Multiple Sclerosis brains. Brain 2009; 132 (5): 1175-1189.
McDonald WI, Compaston A and Edan G. Recommended diagnostic criteria for Multiple Sclerosis: guidelines
from the international panel on the diagnosis of Multiple Sclerosis. Ann Neurol 2001; 50: 121
Montalban X, and et al. Responsiveness and predictive value of EDSS and MSFC in
Neurology. 2008;70(13):1084-1091.
Ghoneimy AT, Gad AH, H, Samir H, et al. Contribution of Vitamin D to the Pathogenesis of Multiple Sclerosis
and its Effect on Bone. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery 2009; 46
Barrett-Connor EL. Sex-specific association of serum vitamin D levels with
Osteoporosis International J 2007; 20(5): 751-760.
Barnes MS, Bonham MP, Robson PJ, et al. Assessment of 25-hydroxyvitamin D and 1, 25
www.iiste.org
Pugliatti M, Rosati G, Carton H and et al. the epidemiology of Multiple Sclerosis in Europe. Europian J of Neurol
Neurol 2004; 3 (92): 104-110.
Marrie RA. Environmental risk factors in Multiple Sclerosis etiology. Lancet Neurol 2004; 3 (12), 709-718.
d Gaitan MI. Immunomodulatory effects of vitamin D in Multiple Sclerosis. Brain
alpha hydroxylase in human
Smolders J, Menheere P, Kessels A and et al. Association of Vitamin D metabolite levels with relapse rate and
sclerosis, vitamin D, and HLA-DRB1*15. Neurology
Holmoy T. Vitamin D status modulates the immune response to Epstein Barr virus: Synergistic effect of risk factors
Bianco and et al. the relation between inflammation and
McDonald WI, Compaston A and Edan G. Recommended diagnostic criteria for Multiple Sclerosis: guidelines
rosis. Ann Neurol 2001; 50: 121-127.
, and et al. Responsiveness and predictive value of EDSS and MSFC in
Ghoneimy AT, Gad AH, H, Samir H, et al. Contribution of Vitamin D to the Pathogenesis of Multiple Sclerosis
and its Effect on Bone. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery 2009; 46 (1): 209-222.
specific association of serum vitamin D levels with
hydroxyvitamin D and 1, 25-dihydroxyvitamin

Journal of Biology, Agriculture and HealthcareISSN 2224-3208 (Paper) ISSN 2225Vol 2, No.11, 2012
D3 concentrations in male and female multiple sclerosis patients and control volunteers, Multiple Sclerosis 2007;
13: 670–672.
17- Lucas RM, Ponsonby AL, Dear K and et al. Sun exposure and vitamin D are independent risk factors for CNS
demyelination. Neurology, 2011; 76 (6): 540
18-Lonergan R, Kinsella K, Fitzpatrick
status and HLA genotype. J Neurol Neurosurg Psychiatry 2011;82:237.
19- Kragt J, van Amerongen B, Killestein J, et al. Higher levels of 25
incidence of multiple sclerosis only in women. Multiple Scl
20- Bianca Weinstock-Guttman, Robert Ziv
and MRI outcomes in multiple sclerosis patients. J Neurol Neurosurg Psychiatry 2011;82:189
21- Van der Mei I, Ponsonby AL, Engelsen O, et al. The high prevalence of vitamin D insufficiency across Australian
populations is only partly explained by season and latitude. Environ Health Perspect 2007; 115(8): 1132
22- Smolders J. Vitamin D and Multiple Sclerosis: Correlation, Causality, and Controversy Autoimmune Diseases
2011, Article ID 629538, 3 pages.
23- SoiluHanninen M, Laaksonen M, Laitinen I, et al. A longitudinal study of serum 25
parathyroid hormone levels indicate the importance of vitamin D and calcium homeostasis regulation in multiple
sclerosis. J Neurol Neurosurg Psychiatr 2008;79:152
Journal of Biology, Agriculture and Healthcare 3208 (Paper) ISSN 2225-093X (Online)
97
D3 concentrations in male and female multiple sclerosis patients and control volunteers, Multiple Sclerosis 2007;
y AL, Dear K and et al. Sun exposure and vitamin D are independent risk factors for CNS
demyelination. Neurology, 2011; 76 (6): 540-548.
Fitzpatrick P and et al. Multiple sclerosis prevalence in Ireland: relationship t
status and HLA genotype. J Neurol Neurosurg Psychiatry 2011;82:237.
Kragt J, van Amerongen B, Killestein J, et al. Higher levels of 25-hydroxyvitamin D are associated with a lower
incidence of multiple sclerosis only in women. Multiple Sclerosis 2009;15:9-15.
Robert Zivadinov, Jun Qu, et al. Vitamin D metabolites are associated with clinical
and MRI outcomes in multiple sclerosis patients. J Neurol Neurosurg Psychiatry 2011;82:189
Van der Mei I, Ponsonby AL, Engelsen O, et al. The high prevalence of vitamin D insufficiency across Australian
populations is only partly explained by season and latitude. Environ Health Perspect 2007; 115(8): 1132
J. Vitamin D and Multiple Sclerosis: Correlation, Causality, and Controversy Autoimmune Diseases
SoiluHanninen M, Laaksonen M, Laitinen I, et al. A longitudinal study of serum 25-hydroxyvitamin D and intact
parathyroid hormone levels indicate the importance of vitamin D and calcium homeostasis regulation in multiple
sclerosis. J Neurol Neurosurg Psychiatr 2008;79:152-157.
www.iiste.org
D3 concentrations in male and female multiple sclerosis patients and control volunteers, Multiple Sclerosis 2007;
y AL, Dear K and et al. Sun exposure and vitamin D are independent risk factors for CNS
P and et al. Multiple sclerosis prevalence in Ireland: relationship to vitamin D
hydroxyvitamin D are associated with a lower
, et al. Vitamin D metabolites are associated with clinical
and MRI outcomes in multiple sclerosis patients. J Neurol Neurosurg Psychiatry 2011;82:189-195.
Van der Mei I, Ponsonby AL, Engelsen O, et al. The high prevalence of vitamin D insufficiency across Australian
populations is only partly explained by season and latitude. Environ Health Perspect 2007; 115(8): 1132-1139.
J. Vitamin D and Multiple Sclerosis: Correlation, Causality, and Controversy Autoimmune Diseases
ydroxyvitamin D and intact
parathyroid hormone levels indicate the importance of vitamin D and calcium homeostasis regulation in multiple

This academic article was published by The International Institute for Science,
Technology and Education (IISTE). The IISTE is a pioneer in the Open Access
Publishing service based in the U.S. and Europe. The aim of the institute is
Accelerating Global Knowledge Sharing.
More information about the publisher can be found in the IISTE’s homepage:
http://www.iiste.org
CALL FOR PAPERS
The IISTE is currently hosting more than 30 peer-reviewed academic journals and
collaborating with academic institutions around the world. There’s no deadline for
submission. Prospective authors of IISTE journals can find the submission
instruction on the following page: http://www.iiste.org/Journals/
The IISTE editorial team promises to the review and publish all the qualified
submissions in a fast manner. All the journals articles are available online to the
readers all over the world without financial, legal, or technical barriers other than
those inseparable from gaining access to the internet itself. Printed version of the
journals is also available upon request from readers and authors.
IISTE Knowledge Sharing Partners
EBSCO, Index Copernicus, Ulrich's Periodicals Directory, JournalTOCS, PKP Open
Archives Harvester, Bielefeld Academic Search Engine, Elektronische
Zeitschriftenbibliothek EZB, Open J-Gate, OCLC WorldCat, Universe Digtial
Library , NewJour, Google Scholar