Embed Size (px)
Citation preview

A S S O C I A T I O N R E P O R T S
Dental chairs
Acceptable
Elegan, JSA, JSR, SPD-5, VSA & VSR, Syntex Dental Products
Dental porcelains and ceram ics
Provisionally Acceptable
Dicor, Dentsply International
Dental X-ray equipment
Acceptable
Healthco Lumix III, Healthco Co
Endosseous implants
Provisionally Acceptable
Biotes, Bofors Nobelpharma
Nitrous oxide/oxygen scavenging equipment
Acceptable
Porter/Brown Clean-Air Scavenging Equipment, Porter Instrum ent Co
Powered oral hygiene devices
Provisionally Acceptable
Interplak, Dental Research Corp
Recogn ition program for products not currently
covered by a formal acceptance program or certifi
cation program
Additions
Caridex 100, National Patent Dental Products, IncCentrays, Coopercare, IncCentwins, Coopercare, IncIdeal Sutures, Interstate Drug Exchange, IncLactona Toothbrushes & Stimulator, Lactona CorpSuper-Dent Sutures, Rugby Laboratories
T h e following p roducts have been rem oved from the list o f classified den ta l m aterials, in strum en ts, and equipm ent.
Crown and bridge and temporary crown and bridge
resins
Acceptable
SR-Isosit-PE, Degussa
Nitrous-oxide/oxygen scavenging equipment
Acceptable
Brown Mask, Summit Services Brown Scavenger, MDT Corp
--------------------JA B A --------------------This informational report was prepared by the
council in December 1985. Address requests for reprints to the Council on Dental Materials, Instruments, and Equipment.
The effects of blue light on the retina and the use of protective filtering glasses
Council on Dental Materials, Instruments, and Equipment
D en ta l office p e rso n n el shou ld use pro tective filte ring devices, e ith e r eyeglasses o r eye shields, while curing
visible light-activated resins.1 O phthalm ic re search into the appearance o f blue light lesions has no t ru led ou t the possibility th a t short wavelength light (light with wavelengths o f less than 500 nm ) may contribute to the p rem atu re aging o f the retina and to senile m acular degenera tion2 (the decreasing ability o f the m acular region o f the retina to provide visual acuity). N ear ultraviolet and blue lights also may cause the form ation o f cataract. M acular degeneration is a m ajor cause o f visual loss in o lder people in the U nited States.3 Also, reports indicate that light-induced retinal dam age can be hastened by increased exposure to visible light with wavelengths o f less than 500 nm. This effect is photochem ical ra th e r than therm al o r s tru c tu ra l.4' 7 T h e m acular d e g en e ra tio n is a m o n g th e m ost active re se a rc h a rea s in ophthalm ology. Most o f the d a ta on light- induced re tinal dam age have been derived from studies o f animals and have not been confirm ed in studies o f hum ans. A lthough no direct cause-and-effect re la tio n sh ip has been docum ented fo r dental visible light-curing unit use, the council recom m ends the use o f ap p ro priate, protective, filtering eyeglasses.1
T h e ocular m edia (composed o f the cornea,
aqueous media, crystalline lens, and vitreous hum or) passes light between 400 and 1,400 nm to the retina (the range o f the visual spectrum is approxim ately 400 to 700 nm ).8 As the lens ages, it acts as a natural absorber o f wavelengths o f betw een 320 and 400 nm .2 In addition, the lens provides partial protection to the retina from blue light. This protection increases with age, as the lens becomes m ore yellow. W hen the lens is rem oved after cataract surgery, this natu ra l filter is rem oved, causing exposure of ultraviolet and near blue lights to the retina. T h e fovea, o r the m acular region o f the retina, provides the eye with the m ost sensitive visual acuity. It is com posed alm ost entirely o f the color-sensitive cone cells o f the retina. It is this vital zone that may be subjected to p rem ature aging by increased exposure to ultraviolet and blue lights (up to wavelengths o f approxim ately 500 nm). Dental visible light-activated resin system s are polymerized by light in the 470-nm ra n g e . C u r r e n tly av a ilab le v is ib le lig h t- activating units generally transm it light beginn ing a t approxim ately 370 nm and peaking at 470 nm . Some units continue to transm it light beyond 700 nm .9' 12 T h e specific range depends prim arily on the filters in the unit. It is the area o f less than 500 nm that is o f specific concern.
T h e use o f appropria te , protective eyeglasses when operating visible light-curing units is rec
om m ended by the council1 and by the C enter fo r Devices and Radiological H ealth/Food and D ru g A dm in is tra tion .9 Protective eyeglasses sh o u ld f i lte r o u t m ost o f th e in ten sity o f wavelengths o f less than 500 nm.
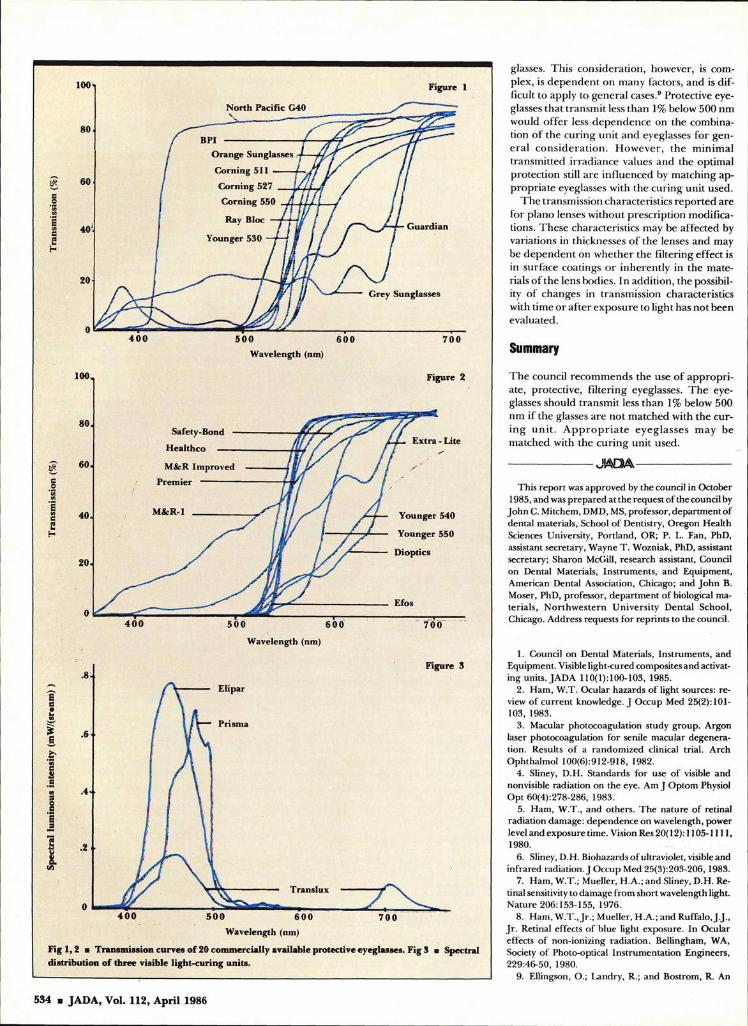
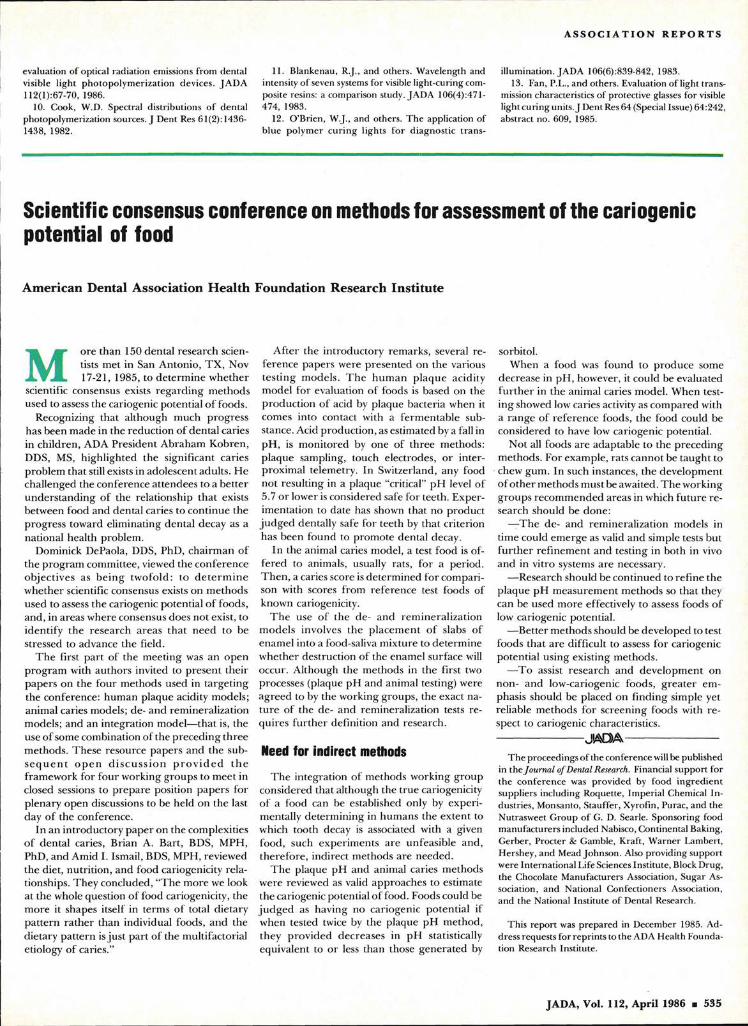
T h e council’s laboratory recently m easured the transm ission characteristics o f 20 com m ercially available p ro tective eyeglasses.13 T h e transm ission curves are shown in Figures 1 and2. As noted in the illustrations, considerable d ifferences exist am ong the glasses and, thus, the protection that they offer. Users o f visible light-curing units should be aware that p ro tective eyeglasses should be selected carefully fo r adequate protection o f the eyes. As emission spectra o f various curing units d iffer (Fig 3), the possible protection offered by eyeglasses that transm it some irradiance at levels o f less than 500 nm would depend on a specific cu ring unit and the specific set o f protective eyeglasses. It is possible that com binations may exist that result in little o r no irradiance at levels o f less than 500 nm reach ing the eyes o f the user; fo r exam ple, w hen the transm ission region o f the eyeglasses at levels o f less than 500 nm corresponds to the no emission intensity in that region from the curing units. Fu rtherm ore , even if some irradiance o f less than 500 nm is transm itted th ro u g h the eyeglasses, the irradiance m ight have been reduced to a safe level by the eye-
JADA, Vol. 112, April 1986 ■ 533
Grey Sunglasses
Translux
0 7 0 0Wavelength (nm)
Fig 1 ,2 ■ Transmission curves o f 20 commercially available protective eyeglasses. Fig 3 distribution o f three visible light-curing units.
Spectral
5 0 0 6 0 0Wavelength (nm)
7 0 0
Figure 2
North Pacific G40
Figure 1
Guardian
Safety-Bond -
Healthco ------
M&R Improved Premier -----------
M&R-l Younger 540
Younger 550
Dioptics
Extra - Lite
Prisma
7 0 0
Figure 3
EUpar
6 0 0
Wavelength (nm)
glasses. T h is consideration , however, is com plex, is d ep en d en t on m any factors, and is d ifficult to apply to general cases.9 Protective eyeglasses th a t transm it less than 1% below 500 nm would o ffe r less depen d en ce on the com bination o f the curing u n it an d eyeglasses fo r gene ra l c o n sid e ra tio n . H ow ever, th e m inim al transm itted irrad iance values and the optim al protection still a re influenced by m atching ap p ro p ria te eyeglasses with the curing un it used.
T h e transm ission characteristics rep o rted are fo r p iano lenses w ithout prescrip tion m odifications. T hese characteristics may be affected by variations in thicknesses o f the lenses and may be d ep en d en t on w hether the filtering effect is in surface coatings o r inheren tly in the m aterials o f th e lens bodies. In addition, the possibility o f changes in transm ission characteristics with tim e o r a fte r exposure to light has no t been evaluated.
Summary
T h e council recom m ends the use o f ap p ro p riate, protective, filtering eyeglasses. T h e eyeglasses should transm it less than 1% below 500 nm if the glasses are no t m atched with the cu rin g u n it. A p p r o p r ia te ey eg lasses m ay be m atched with the cu rin g un it used.
------------------- J A D A ----------------------
This report was approved by the council in October 1985, and was prepared at the request o f the council by
John C. Mitchem, DMD, MS, professor, departm ent of dental materials, School o f Dentistry, Oregon Health Sciences University, Portland, OR; P. L. Fan, PhD, assistant secretary, Wayne T . Wozniak, PhD, assistant secretary; Sharon McGill, research assistant, Council on Dental Materials, Instrum ents, and Equipment, American Dental Association, Chicago; and John B. Moser, PhD, professor, departm ent of biological materials, N orthw estern U niversity Dental School, Chicago. Address requests for reprints to the council.
1. Council on Dental Materials, Instruments, and Equipment. Visible light-cured composites and activating units. JADA 110(1): 100-103, 1985.
2. Ham, W.T. Ocular hazards o f light sources: review o f current knowledge. J Occup Med 25(2): 101- 103, 1983.
3. Macular photocoagulation study group. Argon laser photocoagulation for senile macular degeneration. Results o f a random ized clinical trial. Arch Ophthalmol 100(6):912-918, 1982.
4. Sliney, D.H. Standards for use o f visible and nonvisible radiation on the eye. Am J Optom Physiol O pt 60(4):278-286, 1983.
5. Ham, W.T., and others. The nature o f retinal radiation damage: dependence on wavelength, power level and exposure time. Vision Res 20( 12): 1105-1111,1980.
6. Sliney, D.H. Biohazards o f ultraviolet, visible and infrared radiation. J Occup Med 25(3):203-206, 1983.
7. Ham, W.T.; Mueller, H.A.; and Sliney, D.H. Retinal sensitivity to damage from short wavelength light. Nature 206:153-155, 1976.
8. Ham, W.T., Jr.; Mueller, H.A.; and Ruffalo, J.J., Jr . Retinal effects o f blue light exposure. In Ocular effects o f non-ionizing radiation. Bellingham, WA, Society o f Photo-optical Instrumentation Engineers, 229:46-50, 1980.
9. Ellingson, O.; Landry, R.; and Bostrom, R. An
534 ■ JADA, Vol. 112, April 1986
A S S O C I A T I O N R E P O R T S
evaluation of optical radiation emissions from dental visible light photopolym erization devices. JADA 112(l):67-70, 1986.
10. Cook, W.D. Spectral distributions o f dental photopolymerization sources. J Dent Res 61(2): 1436- 1438, 1982.
11. Blankenau, R.J., and others. Wavelength and intensity of seven systems for visible light-curing composite resins: a comparison study. JADA 106(4):47l- 474, 1983.
12. O ’Brien, W.J., and others. T he application of blue polym er curing lights fo r diagnostic trans
illumination. JADA 106(6):839-842, 1983.13. Fan, P.L., and others. Evaluation o f light trans
mission characteristics of protective glasses for visible light curing units. J Dent Res 64 (Special Issue) 64:242, abstract no. 609, 1985.
Scientific consensus conference on methods for assessment of the cariogenic potential of food
A m erica n D en ta l A sso c ia tio n H ea lth F o u n d a tio n R esearch In stitu te
M ore than 150 dental research scientists m et in San A ntonio, T X , Nov 17-21, 1985, to de term ine w hether
scientific consensus exists regard ing m ethods used to assess the cariogenic potential o f foods.
Recognizing th a t a lthough m uch progress has been m ade in the reduction o f den ta l caries in children , ADA President A braham K obren, DDS, MS, highlighted the significant caries problem th a t still exists in adolescent adults. He challenged the conference a ttendees to a b e tte r un d erstan d in g o f the re lationship th a t exists betw een food and dental caries to continue the progress tow ard elim inating den tal decay as a national health problem .
Dominick DePaola, DDS, PhD, chairm an o f the p rogram com m ittee, viewed the conference ob jec tives as b e in g tw ofo ld : to d e te rm in e w hether scientific consensus exists on m ethods used to assess the cariogenic potential o f foods, and, in areas w here consensus does no t exist, to iden tify th e research a reas th a t need to be stressed to advance the field.
T h e first p a rt o f the m eeting was an open program with au thors invited to p resen t their p apers on the four m ethods used in targe ting the conference: hum an plaque acidity m odels; anim al caries m odels; de- and rem ineralization m odels; and an integration m odel—th at is, the use o f some com bination o f the p reced ing th ree m ethods. T hese resource papers and the subs e q u e n t o p e n d is c u s s io n p r o v id e d th e fram ew ork for fo u r working groups to m eet in closed sessions to p rep are position papers for p lenary open discussions to be held on the last day o f the conference.
In an in troductory p ap er on the complexities o f den tal caries, Brian A. B art, BDS, MPH, PhD, and Amid I. Ismail, BDS, MPH, reviewed the diet, nutrition , and food cariogenicity re lationships. T hey concluded, “T h e m ore we look at the whole question o f food cariogenicity, the m ore it shapes itself in term s o f total d ietary p a tte rn ra th e r than individual foods, and the dietary p a tte rn is ju st part o f the m ultifactorial etiology o f caries.”
A fter the in troductory rem arks, several reference papers were p resen ted on the various tes tin g m odels. T h e h u m an p laque acidity m odel fo r evaluation o f foods is based on the p roduction o f acid by plaque bacteria when it com es in to contact with a fe rm entab le substance. Acid production , as estim ated by a fall in pH , is m onitored by one o f th ree m ethods: p laque sam pling, touch electrodes, o r inter- proxim al telem etry. In Switzerland, any food no t resulting in a plaque “critical” pH level o f 5.7 o r lower is considered safe fo r teeth. E xperim entation to date has shown that no product
ju d g e d dentally safe fo r teeth by that criterion has been found to prom ote dental decay.
In the anim al caries m odel, a test food is o ffe red to animals, usually rats, fo r a period. T h en , a caries score is d e term ined fo r com parison with scores from reference test foods o f known cariogenicity.
T h e use o f the de- and rem ineralization m odels involves th e p lacem en t o f slabs o f enam el into a food-saliva m ixture to de term ine w hether destruction o f the enam el surface will occur. A lthough the m ethods in the first two processes (plaque pH and anim al testing) were agreed to by the working groups, the exact natu re o f the de- and rem ineralization tests requires fu rth e r definition and research.
Need for indirect methods
T h e integration o f m ethods w orking group considered that although the true cariogenicity o f a food can be established only by experim entally determ in ing in hum ans the ex ten t to which tooth decay is associated with a given food, such experim ents are unfeasible and, th erefo re , indirect m ethods a re needed.
T h e plaque pH and anim al caries m ethods w ere reviewed as valid approaches to estim ate the cariogenic potential o f food. Foods could be ju d g e d as having no cariogenic po ten tial if when tested twice by the plaque pH m ethod, they prov ided decreases in pH statistically equivalent to o r less than those generated by
sorbitol.W hen a food was found to p roduce some
decrease in pH , however, it could be evaluated fu r th e r in the anim al caries m odel. W hen testing showed low caries activity as com pared with a ran g e o f reference foods, the food could be considered to have low cariogenic potential.
N ot all foods are adaptable to the p reced ing m ethods. For exam ple, rats canno t be taugh t to chew gum . In such instances, the developm ent o f o th e r m ethods m ust be aw aited . T h e w orking g roups recom m ended areas in which fu tu re re search should be done:
—T h e de- and rem ineralization m odels in tim e could em erge as valid and sim ple tests but fu r th e r refinem en t and testing in both in vivo and in vitro systems are necessary.
— Research should be continued to re fine the p laque pH m easurem ent m ethods so that they can be used m ore effectively to assess foods o f low cariogenic potential.
— B etter m ethods should be developed to test foods that are difficult to assess fo r cariogenic potential using existing m ethods.
— T o assist research an d developm en t on non- an d low-cariogenic foods, g rea te r em phasis should be placed on find ing sim ple yet reliable m ethods fo r screening foods with re spect to cariogenic characteristics.----------------------- J f tD A -------------------------
T he proceedings of the conference will be published in the Journa l o f Dental Research. Financial support for the conference was provided by food ingredient suppliers including Roquette, Imperial Chemical Industries, Monsanto, Stauffer, Xyrofin, Purac, and the Nutrasweet Group o f G. D. Searle. Sponsoring food manufacturers included Nabisco, Continental Baking, Gerber, Procter 8c Gamble, Kraft, W arner Lambert, Hershey, and Mead Johnson. Also providing support were International Life Sciences Institute, Block Drug, the Chocolate Manufacturers Association, Sugar Association, and National Confectioners Association, and the National Institute of Dental Research.
This report was prepared in December 1985. Address requests for reprints to the ADA Health Foundation Research Institute.
JADA, Vol. 112, April 1986 ■ 535





























