Embed Size (px)
Citation preview

119Pavlos MSAOUEL, et al.: Validation of the Greek ERI Questionnaire
vals 1.39 to 8.38, p=0.007, respectively). Conclusions: The translated and adapted Greek version is compa-rable with the original ERI instrument in terms of valid-ity and factorial structure and is suitable for assessment of the psychosocial work environment of Greek health-care professionals.(J Occup Health 2012; 54: 119–130)
Key words: Effort-reward imbalance questionnaire (ERIQ), Greek validation,Health professionals, Occupational stress, Psychometric properties
Accumulating evidence over the last few decades has demonstrated the negative impact of psychologi-cally adverse occupational characteristics on employee health and performance1).
The effort-reward imbalance (ERI) model2), which focuses on the lack of social reciprocity and fairness between efforts spent and rewards received at work, has been widely tested and proven to be particu-larly successful in elucidating occupational stress phenomena. The extrinsic effort scale represents the demanding aspects and obligations of the work envi-ronment, whereas the extrinsic rewards scale includes gains offered or promised via social and contractual reciprocity in terms of esteem, financial compensa-tion, career opportunities and job security. The ERI model postulates that a mismatch between effort and reward can elicit strong negative emotions and asso-ciated psychobiological stress reactions. In addition to the above extrinsic components, the ERI model includes an intrinsic, personal determinant of high cost/low gain conditions characterized by overcommit-ment. The “overcommitment” dimension reflects the motivational personality elements that foster excessive ambition and devotion to work due to an underlying
Abstract: The Effort-reward Imbalance Question-naire in Greek: Translation, Validation and Psycho-metric Properties in Health Professionals: Pavlos MSAOUEL, et al. Greek Junior Doctors and Health Scientists Society, Greece—Objectives: The aim of the present study was to translate, adapt and validate the Effort-reward imbalance (ERI) questionnaire in a sample of Greek healthcare professionals. Methods: An internationally recommended methodology was followed to perform translation of the ERI instrument into the Greek language. The questionnaire was then randomly administered to 600 Greek physicians, nurses, physiotherapists and laboratory staff, and 456 question-naires with no missing data on the ERI items were returned (76% response rate). Tool validation included assessment of internal consistency, factorial structure, discriminant validity and presence of floor or ceiling effects. Criterion validity was demonstrated by investi-gating the association of theoretically relevant ERI summary measurements with respondents’ self-rated health. Results: The Greek version of the ERI ques-tionnaire showed good psychometric properties. Cronbach’s alpha values were 0.79, 0.72 and 0.75 for the three ERI scales of effort, reward and overcommit-ment respectively. Exploratory factor analysis yielded a 5-factor solution that closely reflected the original theoretical ERI model. Significant associations were found between respondents’ age, gender and specific occupation with ERI scores. ERI ratio and “overcom-mitment” scores in the highest tertiles were associated with elevated odds ratios (OR) of below-average self-rated health (OR=5.38, 95% confidence intervals 1.77 to 16.38, p=0.003, and OR=3.41, 95% confidence inter-
The Effort-reward Imbalance Questionnaire in Greek: Translation, Validation and Psychometric Properties in Health Professionals
Pavlos Msaouel1, 2, Nikolaos C Keramaris1, Alexandros P Apostolopoulos1, Nikolaos Syrmos1, Theocharis Kappos1, Athanasios Tasoulis1, Elli-Sophia Tripodaki1, Evangelia Kagiampaki3, Ioannis Lekkas1 and Johannes Siegrist4
1Greek Junior Doctors and Health Scientists Society, Greece, 2Department of Internal Medicine, Jacobi Medical Center, Albert Einstein College of Medicine, USA, 3Sismanoglio General Hospital of Attica, Greece and 4Department of Medical Sociology, University of Dűsseldorf, Dűsseldorf, Germany
J Occup Health 2012; 54: 119–130 Journal ofOccupational Health
Received Sep 22, 2011; Accepted Jan 15, 2012Published online in J-STAGE Feb 7, 2012Correspondence to: P. Msaouel, Greek Junior Doctors and Health Scientists Society, Greece (e-mail: [email protected])

120 J Occup Health, Vol. 54, 2012
need for social approval and esteem. A number of recent studies have shown significant associations of job stress, as predicted by the ERI model, with health outcomes and objective physiologic measures such as increased likelihood of coronary heart disease3–5), cortisol dysregulation6) and decreased salivary immu-noglobulin A levels7) among employees exposed to effort-reward imbalance. These data support the util-ity of the ERI model in elucidating the health effects of occupational stress.
The three ERI components can be measured by an established 23-item questionnaire that uses Likert-type response options8). This questionnaire utilizes a two-step procedure in answering the questions measuring effort and reward whereby respondents are first asked to indicate whether an item describes a typical experience in their work situation, and those who answer “yes” are then asked to specify, on a 4-point Likert scale, the extent of their distress by that experience. This information is ultimately reduced into a uniform 5-point Likert scale for each item. On the other hand, the overcommitment component is measured using a 4-point Likert scale ranging from strongly disagree to strongly agree. Recent method-ological evidence9) has suggested that a 4-point Likert-scaled response that simply has one dimension with four answers ranging from strongly disagree to strong-ly agree in the items measuring effort and reward can provide results that are highly comparable to those obtained with the two-step procedure. This simplified procedure may also produce less missing data. Thus, Siegrist et al.10) recently proposed to uniformly apply the 4-point Likert scheme used in the overcommit-ment component in all three scales of the ERI ques-tionnaire.
The Greek labor market is currently facing a mani-fold crisis and is in need of urgent reforms11). A number of interventions aimed at increasing competi-tiveness and labor market flexibility are currently being implemented. These conditions may, however, also increase job instability and reduce wages, labor benefits and pensions. Furthermore, the Greek economic system has traditionally been encumbered with inequities in social and institutional exchange as well as procedural and relational injustices11). The ERI model assesses several of these factors and, furthermore, it disentangles the extrinsic (struc-tural) from the intrinsic (personal) components of the psychosocial conditions that may affect occupa-tional stress. In addition, the ERI paradigm is more linked to macroeconomic labor market conditions and addresses issues of distributive justice and fair-ness8, 12). Therefore, the ERI model may be particular-ly useful in assessing and addressing work stress and its adverse effects among Greek workers. A number
of recent studies have demonstrated the high preva-lence of occupational stress and burnout among Greek health professionals13, 14). These results justify further evaluation of the psychosocial work environment of Greek health professionals using the ERI model.
The aim of the present study was to adapt the ERI questionnaire into the Greek language and to investigate its internal consistency and psychometric properties in a sample of Greek health-care workers. To our knowledge, this is the first application of the ERI questionnaire in the Greek language. The Greek version of the ERI questionnaire uses the simpli-fied uniform 4-point Likert scale format to measure all three ERI scales. A secondary aim was therefore to evaluate the factorial structure of this simplified instrument. Moreover, we assessed the association of the extrinsic effort and reward imbalance and of the overcommitment scale with self-reported health.
Materials and Methods
Participants and data collectionWe conducted a cross-sectional study on Greek
health professionals (physicians, nurses, physio-therapists and laboratory technicians). Based on the commonly accepted rule recommending a sample of at least 10–15 subjects per questionnaire item to achieve adequate power for factor analysis15), we determined that at least 345 fully completed question-naires would have to be collected for the purposes of our study. Prior response rates in surveys conducted by our group ranged between 77.8–90.9%14, 16). We therefore administered the Greek ERI survey to 600 health professionals anticipating that even a lower than expected response rate of 60% would provide 360 completed responses. The questionnaire was administered to physicians, nursing and laboratory staff randomly chosen from 9 major Greek hospitals (1st I.K.A., 251 G.N.A., Aglaia Kyriakou, Alexandra, Asklipiio, Evangelismos, K.A.T., Metaxa hospi-tals of Athens and AHEPA University Hospital of Thessaloniki) representing 2 large Greek cities (Athens and Thessaloniki). The questionnaire was also administered to physiotherapists participating in two separate physiotherapy scientific meetings. The ques-tionnaires were distributed personally by the research team. Participation was elective, and all participants were approached during breaks from work or training, were informed that responses would be fully anony-mous and were blinded to the scope and purpose of the study. The participants were asked to return the completed questionnaires to a sealed box provided in each hospital or scientific meeting. A total of 525 questionnaires were returned (participation rate 86.9%). Questionnaires with missing data on the ERI items (n=69) were excluded from the study analysis (456

121Pavlos MSAOUEL, et al.: Validation of the Greek ERI Questionnaire
questionnaires included in the analysis; final response rate 76%). Table 1 lists the respondents’ demographic profile and occupations.
Ethical considerationsThe study complied with Greek requirements for
survey studies and received ethical approval from the Scientific committee of K.A.T. Hospital (protocol no. 2306/11-2-11) and permission from the authorized personnel at each institution (i.e., the department or scientific meeting Chair).
QuestionnaireThe original ERI instrument is a 23-item ques-
tionnaire that evaluates the 3 dimensions of the ERI model: extrinsic effort (measured by 6 items), extrinsic reward (measured by 11 items) and over-commitment (measured by 6 items). Based on the developer’s recommendation10), a modified version was used whereby all 23 items were rated using a 4-point Likert scale ranging from strongly disagree to strongly agree. After variable recoding procedures, total effort, reward and overcommitment scores were calculated by the sum of the scores of the corre-sponding items. The theoretical range for the effort and overcommitment scales was 6–24, with higher values indicating more intense effort and overcom-mitment, respectively. The reward scale score range was 11–44, with lower values corresponding to less
reward. These three components are all associated with the core theoretical ERI construct in a second-order factor structure. The reward dimension may further be analyzed into three components named esteem, job promotion and job security8). Based on the ERI scale scores, two theoretically relevant summary measures were calculated. The first was the extrinsic effort/reward ratio constructed using the effort score as the nominator and the reward score, multiplied by a correction factor of 0.5454 (=6/11) to adjust for the number of items, as the denominator. This measurement provides an approximate estimate of the potential mismatch between extrinsic effort and reward at work. Individuals with scores in the upper tertile were considered to have an excessive asym-metry between costs and gains at work, which may expose them to increased psychosocial stress. The second theoretically critical measure was the overcom-mitment scale, whereby scores in the upper tertile indicate an unhealthy personal style of coping with occupational demands and reward expectancies. To determine the Greek ERI questionnaire’s criterion validity, we followed a similar methodology to the one used for the original development of the instru-ment8). Accordingly, participants were asked to rate their perceived general health on a 6-point Likert scale ranging from very bad to very good. Self-rated health was transformed into a dichotomous variable (below/above average health).
TranslationThe Minimal Translation Criteria established by
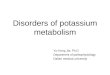
the Medical Outcomes Trust17) were followed during the translation of the ERI questionnaire from English to Greek. Accordingly, two independent bilingual Greek translators independently forward translated the English version of the ERI questionnaire into Greek, and a third reviewer (PM) reconciled the two versions. The reconciled Greek version was pilot tested in 10 health-care professionals, and a cognitive debriefing process was used to identify potential linguistic issues as well as the subjects’ understanding of each item of the questionnaire. Relevant issues were discussed in a debriefing summary, and any necessary changes were incorporated into the questionnaire. This version was then given to a native English speaker and profession-al translator who was blinded to the original English version of the ERI instrument and who back-translated the reconciled Greek questionnaire into English. The back-translation was then sent to the developer of the original questionnaire (JS) for comparative review and comments. The final version (Fig. 1) was retested in 10 health-care professionals, and a cognitive debrief-ing process was again undertaken.
Table 1. Profile of the study participants (n=456)
Mean ± Standard Deviation
Age in years(range 19–61)
35.1 ± 7.2
n (%)
Age groupa
≤30 yr 125 (27.4)
31–40 yr 213 (46.7)
>40 yr 92 (20.2)
Missing values 26 (5.7)
Gendera
Male 216 (47.4)
Female 228 (50)
Missing values 12 (2.6)
Occupationa
Physician 258 (56.6)
Nurse 141 (30.9)
Physiotherapist 51 (11.2)
Laboratory technician 6 (1.3)
aThe values in parentheses represent the percentage of the study’s 456 respondents.

122 J Occup Health, Vol. 54, 2012
Fig. 1. The English and Greek versions of the effort-reward imbalance questionnaire.

123Pavlos MSAOUEL, et al.: Validation of the Greek ERI Questionnaire
Statistical analysisData analysis was performed with SPSS-PC V.15.0.
The internal consistency of the Greek ERI scales was assessed by examining the Cronbach’s alpha coefficient and the corrected item-total correlations. Cronbach’s alpha values >0.7 and corrected item-total correlations >0.3 were considered to be accept-able15). Exploratory factor analysis was performed using principal axis extraction and varimax rotation. Kaiser normalization was used to determine the opti-mal factorial solution. A Bartlett’s test of sphericity with p<0.05 and a Kaiser-Meyer-Olkin (KMO) test of ≥0.7 were used to assess sample adequacy and appro-priateness of factor analysis. Discriminative validity was evaluated by Kruskal-Wallis analysis of variance for multiple group comparisons and by the Mann-Whitney U test for two-group comparisons of the ERI scales between different age, gender and occupational groups. Criterion validity was assessed by binary
logistic regression tests using the dichotomous coding of self-rated health (below/above average) as the dependent variable. A p-value of <0.05 was consid-ered statistically significant. p values of post hoc paired comparisons were adjusted with the Bonferroni method.
Results
Study populationParticipants’ age distribution, genders and occupa-
tions are provided in Table 1. Although the small sample of laboratory technicians was included in further analysis, repeated testing of all study calcula-tions by excluding the laboratory technicians did not substantially alter any of the results provided in this study (data not shown). ERI ratio scores >1.0 were found in 368 respondents (80.7%). Tables 2 shows the mean scores for each measured ERI scale.
Table 2. Mean ± standard deviation (SD) scores, Cronbach’s α and item-total correlation coefficients (uncorrected/corrected) of the effort-reward imbalance (ERI) scales among the study participants (n=456)
Mean ± SD Scores (range) Effort Reward
Esteem rewards
component
Job security and prospects
rewards component
Reciprocal/fair job rewards component
Overcom-mitment
Effort (α=0.79) ERI1 2.97 ± 0.78 (1–4) 0.79/0.66 –0.17 –0.04 –0.26 –0.10 0.41
ERI2 2.98 ± 0.80 (1–4) 0.66/0.47 –0.24 –0.04 –0.26 –0.25 0.24
ERI3 3.26 ± 0.64 (1–4) 0.72/0.60 –0.06 0.06 –0.20 –0.02 0.31
ERI4 2.61 ± 0.84 (1–4) 0.69/0.51 –0.29 –0.18 –0.24 –0.22 0.40
ERI5 3.08 ± 0.72 (1–4) 0.63/0.46 –0.12 –0.05 –0.14 –0.08 0.20
ERI6 3.15 ± 0.73 (1–4) 0.74/0.61 –0.07 0.04 –0.24 0.02 0.28
Reward (α=0.72)Esteem component
ERI7 2.33 ± 1.08 (0–4) 0.04 0.56/0.38 0.8 –0.001 0.30 –0.03
ERI8 2.74 ± 0.97 (0–4) 0.08 0.47/0.30 0.75 –0.06 0.21 –0.11
ERI9 2.58 ± 0.78 (1–4) –0.05 0.60/0.48 0.70 0.15 0.36 –0.11
ERI10 2.72 ± 0.76 (1–4) –0.30 0.55/0.42 0.55 0.29 0.31 –0.30
Job security and prospects rewards component
ERI11 2.31 ± 0.88 (1–4) –0.25 0.48/0.33 0.14 0.71 0.28 –0.19
ERI12 2.36 ± 0.83 (1–4) –0.20 0.45/0.30 0.09 0.78 0.21 –0.31
ERI13 2.44 ± 0.92 (1–4) –0.25 0.39/0.21 0.02 0.76 0.15 –0.27
Reciprocal/ fair job rewards component
ERI14 2.51 ± 0.83 (1–4) 0.01 0.56/0.42 0.30 0.14 0.74 –0.15
ERI15 2.47 ± 0.81 (1–4) –0.17 0.69/0.59 0.45 0.22 0.79 –0.15
ERI16 2.27 ± 0.78 (1–4) –0.08 0.60/0.49 0.30 0.26 0.73 –0.13
ERI17 1.63 ± 0.74 (1–4) –0.23 0.38/0.24 0.08 0.19 0.57 –0.03
Overcommitment (α=0.75)
OC1 2.44 ± 0.76 (1–4) 0.35 –0.20 –0.12 –0.27 –0.06 0.57/0.37
OC2 2.35 ± 0.80 (1–4) 0.39 –0.24 –0.11 –0.29 –0.14 0.75/0.60
OC3 2.48 ± 0.83 (1–4) 0.13 –0.17 –0.11 –0.10 –0.16 0.54/0.31
OC4 2.68 ± 0.83 (1–4) 0.34 –0.17 –0.08 –0.22 –0.08 0.69/0.51
OC5 2.30 ± 0.79 (1–4) 0.34 –0.26 –0.14 –0.28 –0.16 0.80/0.68
OC6 2.22 ± 0.77 (1–4) 0.22 –0.19 –0.16 –0.21 –0.05 0.68/0.51

124 J Occup Health, Vol. 54, 2012
TranslationThe first pretested version of the Greek ERI ques-
tionnaire used the original two-step 5-point Likert scale response format for the effort and reward scales. One of the 10 health professionals (10%) reported problems understanding this choice format. No other specific problems were encountered during the translation and cognitive debriefing process. The developer of the original instrument commented that a Greek verb used in items ERI7 and ERI8 of the questionnaire was back-translated to “accept”, a word that might result in imprecise interpretation of these questions by respondents. Following these sugges-tions, we adopted the simplified 4-point scheme for all ERI items and replaced the first verb on items ERI7 and ERI8 with a Greek word corresponding to the verb “receive” (Fig. 1). Follow-up pilot testing of the revised Greek questionnaire showed that the instrument was comprehensible and easy to answer. Missing data among the 525 returned questionnaires ranged from 1 (0.2%) for items ERI8, ERI14 and OC3 to 14 (2.7%) for item 14. Overall, 69 of the 525 (13.1%) returned questionnaires had missing data for at least one of the 23 items.
Internal consistencyThe Cronbach’s alpha and corrected i tem-
total correlation coefficients are shown in Table 2. Reliability analysis of each ERI scale showed accept-able alpha values: 0.79 for effort, 0.72 for reward and 0.75 for overcommitment, indicating satisfactory inter-nal consistency of the Greek ERI questionnaire. All corrected item-total correlation coefficients were above the threshold of 0.3, suggesting acceptable consistency of the items defining the respective scales with the exception of ERI13 (0.21) and ERI17 (0.24) (Table 2).
Factorial validityThe factor loadings and factorial structure of the
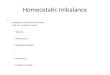
Greek ERI questionnaire based on exploratory factor analysis are shown in Fig. 2. The KMO measure of sampling adequacy was equal to 0.84, and Bartlett’s test of sphericity was statistically significant (p<0.001), supporting the factorability of the correlation matrix obtained from the Greek ERI items. Kaiser’s criterion yielded a 5-factorial solution with all effort items on factor 1, all overcommitment items on factor 2 and the reward items on the remaining 3 factors. This is consistent with the original theoretical ERI model by Siegrist et al.8), which postulated that the reward dimension is a latent factor constructed from the 3 domains of esteem rewards, job security rewards and promotion prospects rewards. The 5-factorial struc-ture of the Greek ERI questionnaire accurately reflects the theoretical components of the ERI model with
two minor exceptions: Item ERI15 (adequate respect and prestige at work) loaded more strongly on factor 3, and item ERI11 (poor job promotion prospects) loaded on factor 5 (Fig. 2). We accordingly labelled factor 3 as reciprocal/fair job rewards, factor 4 as esteem rewards and factor 5 as job security and pros-pects rewards.
Discriminant validityWe assessed the discriminative validity of the Greek
ERI test between different age groups, genders and health-care occupations and the results are shown in Table 3. There was no significant effect of gender on the effort, overcommitment and ERI ratio scores. However, women reported significantly higher reward scores compared with men (p=0.008). Respondents in the 31–40 yr old age group had significantly higher effort, overcommitment and ERI ratio scores compared with health professionals ≤30 yr old (p values <0.05). There was no significant difference in the reward scale between these two groups. ERI measurements did not differ significantly between higher-aged (>40 yr old) and lower-aged (≤30 yr old) respondents. The ERI ratio and reward scores were also found to be significantly higher in 31–40-year-old participants compared with the higher-aged group (p=0.003 and p<0.001 respectively). Physicians and nurses did not differ significantly with regards to the effort and overcommitment scales. However, Greek nurses demonstrated significantly higher reward grades compared with physicians (p<0.001). Greek physi-cians had significantly higher ERI ratio scores as well as significantly lower reward scores compared with physiotherapists (p<0.05). Greek nurses also demon-strated significantly higher effort scores compared with physiotherapists (p=0.006).
Criterion validityWe evaluated one aspect of criterion validity of the
Greek ERI instrument by assuming that health-care workers who scored high on the two theoretically crit-ical summary measures (ERI ratio and overcommit-ment) would be at increased risk of having poor self-rated general health. This hypothesis was confirmed by logistic regression analyses, both unadjusted and after adjustment for respondent age, gender and occu-pation, as shown in Table 4. Respondents with scores at the highest tertiles of the ERI ratio and overcom-mitment scale were significantly more likely to report below average self-rated health compared with those in the lowest tertiles. Respondents with an ERI ratio >1 were again significantly more likely to report below average general health compared with respon-dents with an ERI ratio <1 in both unadjusted (OR=5.36; 95% CI 1.27–22.62; p=0.022) and adjusted for age,

125Pavlos MSAOUEL, et al.: Validation of the Greek ERI Questionnaire
gender and occupation (OR=4.98; 95% CI 1.16–21.43; p=0.031) multivariate analyses. These results demon-strate that the Greek version of the ERI questionnaire can detect groups of employees at risk for low self-rated health.
Floor or ceiling effectsWe used the quality criteria recommended by
Terwee et al.18) to assess for floor or ceiling effects. The highest possible score of 24 was only achieved by 21 respondents (4.6%) for the effort scale and by 1 respondent (0.2%) for the overcommitment scale. The lowest reward score of 11 was not achieved by
any respondent. Thus, floor and ceiling effects were found to be absent in our study in all three ERI scales, further supporting the strong psychometric quality of the Greek ERI instrument.
Discussion
The content validity of the Greek ERI questionnaire was supported by the pilot-testing and debriefing of an initial cohort of health-care professionals. Participants in the pilot-testing process found the uniform 4-point Likert scale, recently suggested by Siegrist et al.10) and ultimately employed in the present study, to be acceptable and easier to understand compared with
Fig. 2. Factorial structure and factor loadings of the Greek effort-reward imbalance (ERI) items following principal axis extraction and varimax rotation.
Factor 1 Factor 2 Factor 3 Factor 4 Factor 5
Eigenvalue 4.99 2.85 1.84 1.47 1.16
Percentage of variance 11.62% 10.16% 7.25% 6.81% 5.35%

126 J Occup Health, Vol. 54, 2012
the more complicated response formats used in the original ERI instrument8). This was further supported by the low levels of missing data for the ERI items as well as the high overall response rate among the study’s 600 health-care workers who received the questionnaire, which was significantly higher than what is typical in surveys of physicians19).
The internal consistency of the ERI scales was satisfactory, although two items in the reward dimen-sion demonstrated slightly lower corrected item-total correlation coefficients, indicating that these two ques-tions show weaker item discrimination. Exploratory
factor analysis of the Greek ERI instrument repro-duced the original 5-factor ERI structure8) with the effort and overcommitment dimensions demonstrating an identical factorial pattern to the original ERI model (Fig. 2). The reward scale, which is considered to be a latent dimension consisting of 3 separate first-order factors, also demonstrated a similar factorial struc-ture to the original ERI concept, with two interesting exceptions being items ERI15, which loaded on two separate factors, and ERI11, which clearly loaded on a separate factor compared with ERI14, ERI16 and ERI17. These results indicate slight variations
Table 3. Comparisons of ERI scale and ERI ratio scores between different age, gender and health-care occupation groups
Efforta p value Rewarda p value Overcommitmenta p value ERI ratioa p value
Age
≤30 yr 17.5 ± 2.9 (6–24)b
0.009b 26.7 ± 4.3 (13–37)
0.063b 13.9 ± 2.8 (7–22)b 0.003b 1.25 ± 0.35 (0.50–2.52)b
0.003b
31–40 yr 18.4 ± 3.5 (6–24)b
0.168c 25.5 ± 5.1 (12–41)c
<0.001c 14.8 ± 3.4 (6–24)b 0.213c 1.40 ± 0.47(0.39–3.38)b, c
0.003c
>40 yr 17.8 ± 3.0 (6–24)
>0.5d 28.0 ± 4.9 (17–39)c
0.159d 14.1 ± 3.3 (6–22) >0.5d 1.22 ± 0.38 (0.33–2.48)c
>0.5d
Gender
Male 18.1 ± 3.1 (10–24)
>0.5e 25.7 ± 4.8 (12–38)d
0.008e 14.3 ± 3.2 (6–22) 0.475e 1.35 ± 0.43 (0.58–3.38)
0.127e
Female 18.0 ± 3.3 (6–24)
27.0 ± 4.9 (13–41)d
14.5 ± 3.2 (6–24) 1.28 ± 0.38 (0.33–2.48)
Occupation
Physician 17.9 ± 3.5 (6–24)
>0.5f 25.3 ± 4.8 (12–38)e, f
<0.001f 14.7 ± 3.2 (6–24) >0.5f 1.37 ± 0.45 (0.33–3.38)f
0.438f
0.15g <0.001g 0.114g <0.001g
>0.5h 0.354h >0.5h >0.5h
Nurse 18.6 ± 2.7 (12–24)g
0.006i 27.6 ± 4.7 (15–39)e
>0.5i 14.4 ± 3.2 (6–23) 0.378i 1.29 ± 0.37 (0.63–2.93)
0.072i
>0.5j >0.5j >0.5j >0.5j
Physio-therapist
17.1 ± 2.6 (12–23)g
>0.5k 28.1 ± 4.3 (20–41)f
>0.5k 13.7 ± 2.9 (6–22) >0.5k 1.14 ± 0.26 (0.67–2.01)f
>0.5k
Laboratory technician
18.3 ± 2.9 (16–24)
28.7 ± 4.5 (20–32)
13.3 ± 2.6 (9–17) 1.23 ± 0.48 (0.92–2.20)
Total 18.0 ± 3.2 (6–24)
26.4 ± 4.9 (12–41)
14.5 ± 3.2 (6–24) 1.32 ± 0.41 (0.33–3.38)
aData presented as the mean ± standard deviation (range), bPaired comparisons between the ≤30 and 31–40-year-old groups, cPaired comparisons between the 31–40 and >40-year-old groups, dPaired comparisons between the ≤30 and >40-year-old groups, ePaired comparisons between the male and female groups, fPaired comparisons between physicians and nurses, gPaired comparisons between physicians and physiotherapists, hPaired comparisons between physicians and laboratory technicians, iPaired comparisons between nurses and physiotherapists, jPaired comparisons between nurses and laboratory technicians, kPaired comparisons between physiotherapists and laboratory technicians, The p values of all post hoc paired comparisons were adjusted with the Bonferroni method.

127Pavlos MSAOUEL, et al.: Validation of the Greek ERI Questionnaire
in the psychometric properties of the Greek version compared with the original ERI questionnaire, which may be due to differences in concept interpretation, linguistic differences in emotionally toned words and other cultural nuances. It should be noted that in comparison to many previous linguistic and cultural adaptations of the ERI questionnaire that have yielded divergent factorial patterns (e.g., a 4-factorial instead of 5-factorial solution)20–23), the Greek ERI factor struc-ture replicated more closely the original ERI model. The 3-factorial components of the reward dimension in the Greek adaption were termed esteem rewards, reciprocal / fair job rewards and job security and pros-pects rewards, respectively. It should also be noted that although previous investigations have suggested that the question assessing physical workload effort (item ERI5) can be omitted in white-collar occupation samples, we decided to include it in the present study because we hypothesized that physical workload may be a more prominent part of the daily task profile of Greek health professionals due to the distinct charac-teristics of the Greek health care work environment as indicated by several previous reports24–26). Indeed, this item demonstrated satisfactory internal consistency, discrimination and factorial properties in our sample, suggesting that the six-item version of the effort scale may be used in Greek health-care workers.
Although research has shown that the dichotomized measure of the ERI ratio (with values >1.0 indicat-ing an imbalance between high effort and low reward) can result in significant information reduction27), the fact that a considerable majority of Greek health-care workers (80.7%) had a >1.0 ERI ratio is indicative of a substantial effort-reward mismatch in this popu-lation. Data from other countries have consistently shown high levels of ERI and its association with adverse health events in health-care professionals28–31). Additional research will therefore be required to further corroborate and elucidate the potential impact of the occupational effort and reward asymmetry on the performance and health of Greek health-care employees.
The results of the present study did not indicate gender differences with regard to effort and overcom-mitment among Greek health-care workers. However, women scored significantly higher on the reward dimension compared with men. The effect of gender on the reward scale has not been consistent across different populations, with some studies reporting higher or no difference in rewards scores of men compared with women8, 32), while others have indicated a reverse effect21, 28) that is in agreement with the pres-ent findings. Furthermore, we found that health-care workers in the middle age group of our study sample
Table 4. Multivariate association (multivariable logistic regression) of the effort-reward imbalance (ERI) ratio and the effort, reward and overcommitment scales with below average self-rated health. Numbers in parentheses represent the tertile cutoff values
Unadjusted Adjusted for age, gender and occupation
OR 95% CI p value OR 95% CI p value
ERI Ratio
Lowest tertile (≤1.10) 1.00 — — 1.00 — —
Middle tertile (1.11 to 1.39) 3.85 1.26–11.83 0.018 3.41 1.06–10.94 0.040
Highest tertile (>1.39) 5.65 1.91–16.73 0.002 5.38 1.77–16.38 0.003
Effort
Lowest tertile (≤16) 1.00 — — 1.00 — —
Middle tertile (17 to 19) 1.92 0.74–4.98 0.180 2.18 0.77–6.18 0.141
Highest tertile (>19) 3.22 1.25–8.31 0.016 2.98 1.06–8.44 0.039
Reward
Lowest tertile (≤23) 1.00 — — 1.00 — —
Middle tertile (24 to 29) 0.52 0.26–1.04 0.066 0.52 0.24–1.11 0.091
Highest tertile (>29) 0.40 0.17–0.96 0.040 0.39 0.15–1.01 0.052
Overcommitment
Lowest tertile (≤12) 1.00 — — 1.00 — —
Middle tertile (13 to 16) 2.99 1.14–7.86 0.026 2.64 0.97–7.14 0.057
Highest tertile (>16) 4.04 1.70–9.62 0.002 3.41 1.39–8.38 0.007
CI: Confidence interval; OR: Odds ratio.

128 J Occup Health, Vol. 54, 2012
demonstrated significantly higher ERI ratio scores compared with the youngest and oldest age groups. This finding is consistent with previous data in a population of German workers10), although other inves-tigations have reported different patterns or no signifi-cant association between age and ERI scales20, 32). The age-specific pattern observed in the present Greek population of health-care workers is particularly important, as stronger associations between effort-reward imbalance and physiological outcomes have been reported in middle-aged populations compared with younger or older adults33). Variability in ERI ratio scores may be attributed to differences in career perspectives, expectations and personal challenges across age strata. In addition, occupation-specific differences were noted among Greek health-care professionals, with physicians reporting significantly lower occupational reward compared with nurses and physiotherapists. Greek physiotherapists also demonstrated significantly lower ERI ratio scores compared with physicians as well as significantly lower effort scores compared with nurses. Further research will be required to clarify the components of gender-, age- and occupation-specific ERI and job stress among Greek workers, taking into consideration the Greek cultural background, working environment and idiosyncrasies of the labor market and system. With regards to criterion validity, the present study demonstrated that Greek health-care workers scoring in the upper ERI ratio and overcommitment tertiles were significantly more likely to report below-average general health independently of age, gender or specific occupation. Although the categorization of continuous measures may result in considerable loss of informa-tion, several studies have shown that upper tertile ERI ratio and overcommitment scores are associated with elevated odds of poor self-rated health8, 34), and previous investigations have shown that such analyses based in categorizations are comparable to continuous measures35, 36).
The limitations of this study include the cross-sectional design, which prevented determination of causality. Although prospective studies in differ-ent populations have shown a causal association of the ERI components with adverse psychosomatic effects1, 4, 5), future research should investigate the asso-ciations of the Greek ERI questionnaire with objec-tive measurements of health. Reporting bias is also a possible confounder of the observed relationship between ERI measurements and subjective health, since the present study did not control for the effects of personal style responses such as negative affectiv-ity. On the other hand, several previous investigations have shown that such factors do not invalidate the association of ERI scales with health37, 38). Attrition
analyses could not be performed due to the lack of detailed demographic records for public employees in Greece as well as the fact that we were unable to collect any further data on nonrespondents, in order to fully protect their anonymity. It should also be noted that the samples included in this study were some-what heterogeneous in terms of professions, consist-ing mainly of physicians, nurses and physiotherapists. This heterogeneity was intentional, as it allowed the Greek ERI instrument to be tested in a broader spec-trum of health-care professionals. Given the relatively robust factorial structure and internal consistency, it is unlikely that the psychometric parameters presented here vary substantially between subgroups. However, the results of the present study may only be general-ized in physicians, nurses and physiotherapists, and further testing of the instrument should be conducted across occupational groups and sectors other than health care. It should also be noted that although no floor or ceiling effects were detected in our study, future investigations should remain vigilant for the emergence of such effects in the Greek population as the economic crisis continues.
In conclusion, the present study demonstrated that the Greek translated ERI questionnaire is a reliable and psychometrically valid tool for the assessment of asymmetric exchanges between occupational effort and rewards in health-care workers. Our findings indicate satisfactory properties in terms of internal consistency as well as factorial, discriminative and criterion validity. Furthermore, this study adds to a growing body of evidence demonstrating the applica-bility of a simplified, uniform response format used in all ERI scales. The Greek ERI instrument is avail-able for epidemiologic studies on occupational stress and health and can be used to guide future individual and organizational interventions. To this aim, future studies should additionally investigate the psychomet-ric properties of shorter versions of the Greek ERI instrument10, 39) that can be even more easily utilized in large-scale investigations.
Acknowledgments: The authors would like to thank Kleio Nikolopoulou and Eirini Tamvaki for the forward-translations of the English ERI questionnaire to Greek and Carol Spanos for the back-translation of the instrument to English. We are also grateful to Drs. Vassilis Gizas and George Koussidis for their valuable assistance with questionnaire distribution.
References
1) Tsutsumi A, Kawakami N. A review of empirical studies on the model of effort-reward imbalance at work: reducing occupational stress by implementing a new theory. Soc Sci Med 2004; 59: 2335–59.

129Pavlos MSAOUEL, et al.: Validation of the Greek ERI Questionnaire
2) Siegrist J. A theory of occupational stress. In: Dunham J, editor. Stress in the workplace: Past, present and future. London: Whurr Publishers; 2000. p.52–66.
3) Kivimaki M, Virtanen M, Elovainio M, Kouvonen A, Vaananen A, Vahtera J. Work stress in the etiology of coronary heart disease—a meta-analysis. Scand J Work Environ Health 2006; 32: 431–42.
4) van Vegchel N, de Jonge J, Bosma H, Schaufeli W. Reviewing the effort-reward imbalance model: draw-ing up the balance of 45 empirical studies. Soc Sci Med 2005; 60: 1117–31.
5) Siegrist J. Effort-reward imbalance at work and cardiovascular diseases. Int J Occup Med Environ Health 2010; 23: 279–85.
6) Bellingrath S, Weigl T, Kudielka BM. Cortisol dysregulation in school teachers in relation to burn-out, vital exhaustion, and effort-reward-imbalance. Biol Psychol 2008; 78: 104–13.
7) Wright BJ. Effort-reward imbalance is associated with salivary immunoglobulin a and cortisol secre-tion in disability workers. J Occup Environ Med 2011; 53: 308–12.
8) Siegrist J, Starke D, Chandola T, et al. The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med 2004; 58: 1483–99.
9) Tsutsumi A, Iwata N, Wakita T, Kumagai R, Noguchi H, Kawakami N. Improving the measure-ment accuracy of the effort-reward imbalance scales. Int J Behav Med 2008; 15: 109–19.
10) Siegrist J, Wege N, Puhlhofer F, Wahrendorf M. A short generic measure of work stress in the era of globalization: effort-reward imbalance. Int Arch Occup Environ Health 2009; 82: 1005–13.
11) Mitsopoulos M, Pelagidis T. Understanding the crisis in Greece : from boom to bust. Hampshire (NY): Palgrave Macmillan; 2011.
12) Levi L, Bartley M, Marmot M, et al. Stressors at the workplace: theoretical models. Occup Med 2000; 15: 69–106.
13) Kiekkas P, Spyratos F, Lampa E, Aretha D, Sakellaropoulos GC. Level and correlates of burnout among orthopaedic nurses in Greece. Orthop Nurs 2010; 29: 203–9.
14) Msaouel P, Keramaris NC, Tasoulis A, et al. Burnout and training satisfaction of medical resi-dents in Greece: will the European work time direc-tive make a difference? Hum Resour Health 2010; 8: 16.
15) Field AP. Discovering statistics using SPSS. 3rd ed. Los Angeles: SAGE Publications; 2009.
16) Avgerinos ED, Msaouel P, Koussidis GA, Keramaris NC, Bessas Z, Gourgoulianis K. Greek medical students’ career choices indicate strong tendency towards specialization and training abroad. Health Policy 2006; 79: 101–6.
17) Medical Outcomes Trust: Trust introduces new translation criteria. Trust Bulletin 5: 3–4.
18) Terwee CB, Bot SD, de Boer MR, et al. Quality
criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol 2007; 60: 34–42.
19) Kellerman SE, Herold J. Physician response to surveys. A review of the literature. Am J Prev Med 2001; 20: 61–7.
20) Zurlo MC, Pes D, Siegrist J. Validity and reliabil-ity of the effort-reward imbalance questionnaire in a sample of 673 Italian teachers. Int Arch Occup Environ Health 2010; 83: 665–74.
21) Li J, Yang W, Cheng Y, Siegrist J, Cho SI. Effort-reward imbalance at work and job dissatisfaction in Chinese healthcare workers: a validation study. Int Arch Occup Environ Health 2005; 78: 198–204.
22) Chor D, Werneck GL, Faerstein E, Alves MG, Rotenberg L. The Brazilian version of the effort-reward imbalance questionnaire to assess job stress. Cad Saude Publica 2008; 24: 219–24.
23) Tsutsumi A, Ishitake T, Peter R, Siegrist J, Matoba T. The Japanese version of the Effort-Reward Imbalance Questionnaire: a study in dental techni-cians. Work & Stress 2001; 15: 86–96.
24) Alexopoulos EC, Tanagra D, Detorakis I, et al. Knee and low back complaints in professional hospital nurses: occurrence, chronicity, care seeking and absenteeism. Work 2011; 38: 329–35.
25) Alexopoulos EC, Burdorf A, Kalokerinou A. A comparative analysis on musculoskeletal disorders between Greek and Dutch nursing personnel. Int Arch Occup Environ Health 2006; 79: 82–8.
26) Antoniou ASG, Davidson MJ, Cooper CL. Occupational stress, job satisfaction and health state in male and female junior hospital doctors in Greece. Journal of Managerial Psychology. [doi:10.1108/02683940310494403]. 2003; 18: 592–621.
27) Pikhart H, Bobak M, Pajak A, et al. Psychosocial factors at work and depression in three countries of Central and Eastern Europe. Soc Sci Med 2004; 58: 1475–82.
28) Li J, Yang W, Cho SI. Gender differences in job strain, effort-reward imbalance, and health function-ing among Chinese physicians. Soc Sci Med 2006; 62: 1066–77.
29) Buddeberg-Fischer B, Klaghofer R, Stamm M, Siegrist J, Buddeberg C. Work stress and reduced health in young physicians: prospective evidence from Swiss residents. Int Arch Occup Environ Health 2008; 82: 31–8.
30) Tsutsumi A, Kayaba K, Nagami M, et al. The Effort-reward Imbalance Model: Experience in Japanese Working Population. J Occup Health 2002; 44: 398–407.
31) Tsutsumi A, Kawanami S, Horie S. Effort-reward imbalance and depression among private practice physicians. Int Arch Occup Environ Health 2012; 85: 153–61.
32) Lau B. Effort-reward imbalance and overcommit-ment in employees in a Norwegian municipality: a cross sectional study. J Occup Med Toxicol 2008; 3: 9.
33) Loerbroks A, Schilling O, Haxsen V, Jarczok MN,

130 J Occup Health, Vol. 54, 2012
Thayer JF, Fischer JE. The fruits of ones labor: effort-reward imbalance but not job strain is related to heart rate variability across the day in 35-44-year-old workers. J Psychosom Res 2010; 69: 151–9.
34) Weyers S, Peter R, Boggild H, Jeppesen HJ, Siegrist J. Psychosocial work stress is associated with poor self-rated health in Danish nurses: a test of the effort-reward imbalance model. Scand J Caring Sci 2006; 20: 26–34.
35) Pikhart H, Bobak M, Siegrist J, et al. Psychosocial work characteristics and self rated health in four post-communist countries. J Epidemiol Community Health 2001; 55: 624–30.
36) Niedhammer I, Tek ML, Starke D, Siegrist J. Effort-reward imbalance model and self-reported health:
cross-sectional and prospective findings from the GAZEL cohort. Soc Sci Med 2004; 58: 1531–41.
37) Bosma H, Peter R, Siegrist J, Marmot M. Two alternative job stress models and the risk of coro-nary heart disease. Am J Public Health 1998; 88: 68–74.
38) Joksimovic L, Starke D, vd Knesebeck O, Siegrist J. Perceived work stress, overcommitment, and self-reported musculoskeletal pain: a cross-sectional investigation. Int J Behav Med 2002; 9: 122–38.
39) Leineweber C, Wege N, Westerlund H, Theorell T, Wahrendorf M, Siegrist J. How valid is a short measure of effort-reward imbalance at work? a replication study from Sweden. Occup Environ Med 2010; 67: 526–31.