Embed Size (px)
Citation preview
[From FerneIius’ Universa Medicina, Geneva, r679.1
BOOKSHELF BROWSING THE EVOLUTION OF HERNIORRHAPHY
FREDERIC W. TAYLOR, M.D.
INDIANAPOLIS, IND.
FOREWORD
T HE nature of this articIe precIudes any attempt at an exhaustive recita1 of the countIess methods which have
been advocated for hernia1 repair. Such a work wouId require vohrmes. Throughout the deveIopment of surgery, no subject has received more comment than that of hernia. Relatively few cures were effected by the earIy operations and each successive generation of our medical forebears devised its own means for deaIing with the condi- tion. Some of these were advances, most of them were oId procedures with onIy minor variations in technique to suit or identify their particuIar sponsor.
To chronicIe a11 of these variations wouId serve IittIe purpose except as an insight into the capabiIities of the particuIar operator. Of more interest surgicaIly is just how the probIem of hernia was deaIt with technicaIIy in Iight of the knowledge and means of the various periods. It is from this angle that we propose to discuss the subject with emphasis on the technica evolution of herniorrhaphy rather than on the character and accompIishments of those who brought about that evolution. In so doing we pass over rapidly or omit
entireIy many operators who exerted great influence in other fieIds but who did IittIe to aIter or improve the treatment of hernia.
LittIe attempt has been made in this review to transIate origina manuscripts. Standard works of medicaI and surgica1 history have been freeIy used and with few exceptions the foreign materiaI has been taken from EngIish or French transIations.
A chronoIogica1 sequence of the methods of hernia1 repair is IogicaI. But as wiI1 be seen, these methods overIap frequentIy and in some instances revert back to an entireIy different age. In general, each earIy operator deaIt with al1 types of hernia in the same manner. As hernias in the region of the groin were not differentiated accu- rateIy unti1 quite Iate in medical history, our descriptions will be those for inguina1 hernia unIess otherwise stipuIated.
EGYPTIAN AGE
In the translations of the several papyri deaIing with the medical knowIedge of Egypt’ it is rather disappointing not to find adequate descriptions of hernia. That this malady frequentIy had to be deaIt with cannot be doubted. However many
‘31

I32 American JOUIIL~I of Surgery TayIor-EvoIution of Herniorrhaphy JULY. 1933
of the descriptions which pass for those of scrota1 hernia might fit equahy we11 for hydroceIe or varicoceIe. PracticaIIy no attempt was made at anatomica diagnosis though the cIinica1 pictures described are quite vivid and in many cases Ieave IittIe doubt as to the true nature of the condi- tion. Occasiona compIete descriptions of intestina1 obstruction are noted. One of these from the Ebers Papyrus, “ . . . a person who suffers from an obstruction in the abdomen and thou kindest that it (tumor) goes-and-comes under thy lingers Iike oi1 in a tube . . . ” and “ . . . a skin tumor on the outside of the body above his genitaIs ” is most certainIy that of an incarcerated inguina1 hernia.
In genera1 the treatment of acute intes- tina obstruction and hence incarcerated hernia, consisted in cathartics and hot appIications to the abdomen. This kil1 or cure method must have taken a heavy to11 and its divergent resuIts added greatIy to the mystery of the true condition at hand. Egyptian Surgery did not include opening the abdomina1 cavity. However this pro- cedure was carried out by the Hindus in a period which overIapped the ancient civiI- ization of Egypt and Greece (1500 B.C.-700
A.D.). Nothing is known about the Hindu technica methods except that the abdomen was occasionaIIy opened, obstructions re- Iieved and at times intestines sutured.
The treatment of simpIe hernia by the Egyptians consisted in appIying snugly fitting bandages to the region in an attempt to maintain reduction or give support to the Iarge scrotal type of hernia. If the same ski11 was used in appIying these as that demonstrated in the bandaging of mum- mies it is fair to assume that this method produced quite an effective form of truss. It is probable that hydrocele and numerous afllictions of the testes were treated in a simiIar manner.
GREEK AND ROMAN PERIOD
The older Greeks, though carefu1 cIin- ica1 observers, possessed Iittle anatomical knowledge. As a resuIt they added Iittle
to the treatment of hernia then used aIong the opposite shores of the Mediterranean. For intestinal obstruction which might be caused by an incarcerated hernia they continued with the use of cathartics and added a more popuIar treatment, the cIyster. Of this Iatter procedure frequent mention is made in the works attributed to Hippocrates and the suggestion is also given that this faiIing an attempt shouId be made to i&late the bowe1 by rectum using a pipe and bIadder. At times such bowe1 stranguIation proceeded to an ulcera- tion through the Iower abdomina1 waI1 forming an enterostomy with a “fetid dis- charge giving a poor outlook.” Toward the middIe of the Greek era reduction by traxis was added as a treatment for stranguIations (Praxagoras of Cos, circa 400 B.C.). Soon after this period, surgery started on its somewhat devious course to the present soIution of the problem of hernia. Surgery incIuding the cautery became accepted forms of treatment.
No records remain of the actua1 tech- nique of Greek hernia1 repair. Accurate descriptions are however preserved in the works of some of the Greek physicians who migrated to Rome. Our most compIete descriptions are those of CeIsus (25 A.D.).
He folIowed cIosely the work of AscIepiades of Bithynia (I 24 B.C.), the founder of Greek medicine in Rome. The methods of hernial repair used by CeIsus wiI1 be taken up in detai1 as they formed much of the basis for operative procedure unti1 the nineteenth century.
CeIsus gave some very good descriptions of the contents of hernia1 sacs and con- trasted them with hydroceIe. The reIation between the scrotum and the abdomina1 cavity however was not appreciated. It was thought that the testicIe was in some way responsibIe for the rupture and conse- quently it was removed at operation. In his treatment of hernia Celsus advocated the foIIowing: (I) preoperative treatment consisting of one to three days’ fast fol- Iowed by a clyster; (2) incision over lower inguinal region and upper scrotum carried

NEW SERIES Vm. XXI, No. I TayIor-Evolution of Herniorrhaphy A mericnn Jwl-n:ii d Sujgcry 133
down to hernia1 sac; (3) margins of wound heId apart by two skin hooks and sac isoIated from its surrounding structures; (4) sac opened, care being taken not to injure testicIe or intestines; (5) if the patient was a child the testicIe was re- moved but in a “robust man” it was again dropped back into the scrotum; (6) intes- tines reduced and heId so by severa sutures in base of sac and adjacent tissues; (7) if a smaII portion of the omentum was pres- ent in the sac it might be safeIy reduced but if Iarge it was transfixed by two Iiga- tures and the dista1 portion excised; (8) vinegar dressing appIied and wound usu- aIIy Ieft open to granulate. OccasionaIIy, loose interrupted skin sutures were in- serted; (9) At times strips of skin were excised from the wound margins so as to bring about more extensive granulation and hence a heavier scar to repair the defect; (IO) Long ends of Iigatures were aIlowed to protrude from the wound; these came away “easiIy without pain or hemor- rhage when suppuration was we11 estab- Iished.” The aponeurosis was not incised in any of these oIder operations.
CeIsus did not use the cautery to any extent and obtained hemostasis by means of Iinen Iigatures. He did not operate upon strangulated hernia “where the flesh is hard and the tumor does not reduce.” Instead, pouItices to the abdomen, supine position, bIeeding and cIysters were advo- cated. CeIsus also advised against opera- tion of oIder people where the condition was far advanced. In chiIdren he reduced the hernia and attempted to effect a cure bv means of snug bandages. OnIy after the failure of these, was operation advised. A typica repair of the period and one most IikeIv to achieve success is that iIIustrated in Figure I.
Celsus described three methods of um- bilica1 hernia repair. Of these he preferred and used the third method Iisted beIow. i I) After dissecting out the sac, two sutures on a needIe were passed through the base of the empty sac. One of these was tied on either side thus ahowing the tissue above
to mortify. HeaIing was by granulation. (2) Same as above except that sac was opened and intestine pushed back into the abdomen with the examining finger before sutures were inserted. (3) With the patient standing a Iine was traced on the skin about the base of the hernia. Then with the patient supine and the intestine reduced, the sac was puIIed out and a strong suture passed around its base at the site of the tracing. The portion of the sac above the Iigature was cauterized and the wound aIIowed to granuIate.
The postoperative care of this period consisted of rest in bed for approximately one month, IocaI treatment of the inevit- able suppurating wound and a mysterious dietary regimen to satisfy the whims of the operator. NeedIess to say the success of these repairs would depend IargeIy upon the amount of firm scar tissue resuIting from the heaIing process. This fact was we11 known by our ancient masters.
MIDDLE AGES
With the disintegration of the Roman Empire and the Ioss of a11 strong centraI- ized government, the weII-advanced art of surgery sank to a IeveI from which it did not recover fuIIy unti1 the sixteenth century. During this period but few opera- tors approached the degree of technical perfection attained by the later Greeks and Romans.
PauI of Aegina (625-690 A.D.) was the Iast of the Greek Schooi to add anything of vaIue to the operative cure of hernia. This worker foIIowed very cIoseIy the methods used by CeIsus but modified them to suit his own originaIity and at times to the betterment of the operation. In the repair of earIy or smaII hernias he advised the foIIowing practice: i I) dissec- tion of the sac from its surrounding tissues, cord and test&, Ieaving the Iatter intact; (2) inversion of the sac into the peritoneal cavity by means of a probe; 13) suture of the base of the inverted sac and withdrawal of probe thus Ieaving peritoneum un- opened; (1) postoperative care consisting
134 American Journal of Surgery TayIor-EvoIution of Herniorrhaphy Jury. 1933
of IocaI dressings of oil, wine or vinegar to ink or the testicIe was Iifted over the pubis the wound. The patient was kept in bed and a simiIar outIine made. (2) The pa- for an unspecified Iength of time. tient was put on a tabIe and the hernia
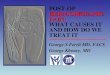
FIG. I. Hernial repair used by contemporaries of CeIsus (25 A.D.). Its use was continued with slight modification we11 into 19th century. (I) Exposure of sac projecting beneath externa1 ring with ligatures in place. (2) Ligatures tied, one on either side of sac and fundus excised with cord and testicIe. (3) Cauterization of entire area. Healing by granuIation.
PauI occasionaIIy used the cautery to effect a cure as did CeIsus. GeneraIIy the testicIe was removed at operation. This was partIy because it was beIieved to be one of the causes of hernia and partIy because it usuaIIy became infected by the operation, sIoughing out Iater and thus deIaying convaIescence.
By the end of the fourteenth century there were six recognized methods of hernia1 repair. These, in addition to the ever-present bandages, pouItices and drugs were as foIIows:
(I) Modified Method of G&us, iIIustrated in Figure I.
The sac was dissected to its base, Iigated and the testicIe removed. (Advocated by Roger, I 170-1240; Theodoric, 1205-1252; Guy de ChauIiac, 1300-1368.)
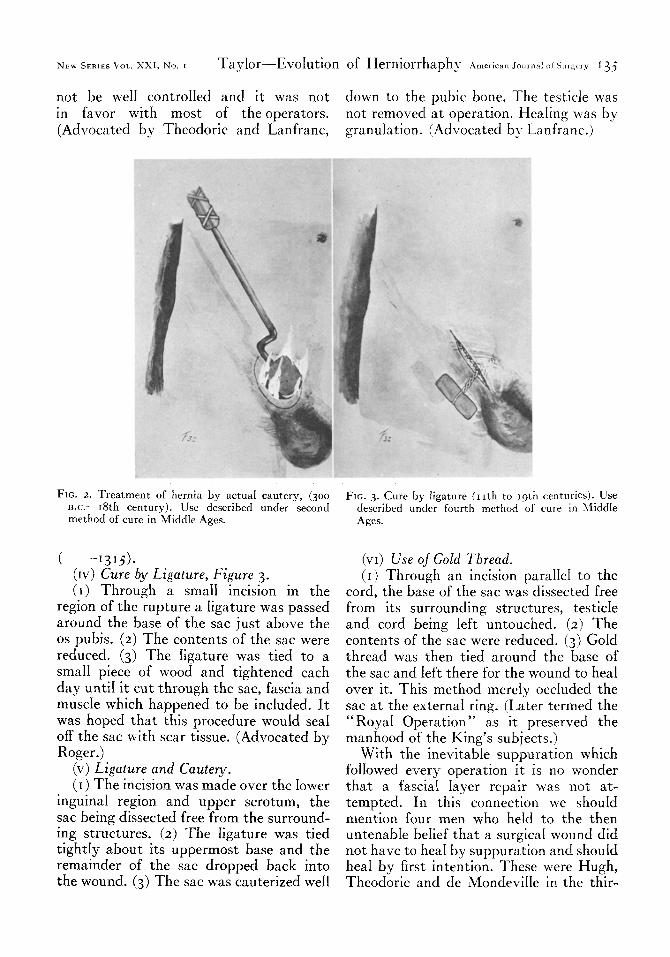
(JI) Use of Actual Cautery, Figure 2. (I) With the patient standing, the
hernia1 sweIIing was outlined at its base in
reduced. (3) The outIined area was cauter- ized unti1 cIose to the OS pubis, care being taken not to injure intestine or testicIe. (4) The wound was treated IocaIIy and the usua1 dietary regimen administered. In genera1 the diet consisted of smaI1 amounts of simpIe food and Iarge quantities of wine and water. FoIIowing the foregoing pro- cedure AIbucasis (10 I 3-1106) kept his patients in bed for forty days andthen aIIowed forty days sIow convaIescence. The cIosing of the inguina1 canal and strengthening of the abdominal waI1 again depended upon the resulting cicatrix. (Method advocated by AIbucasis, Roger, Theodore, and Guy de ChauIiac.)
(III) Use of “ Coutere Potentiel.” This method was identical with that of
the actua1 cautery except that strong caustic or acid was used to cause a cicatrix instead of the hot iron. The extent of the Iesion thus formed by this method couId
NEW SERIES \OL. XXI, No. I TayIor-Evolution of Herniorrhaphy A m&can Journal ot Surgery I3 j
not be we11 controIled and it was not down to the pubic bone. The testicle was in favor with most of the operators. not removed at operation. HeaIing was by (Advocated by Theodoric and Lanfranc, granulation. (Advocated bJ- Lanfranc.)
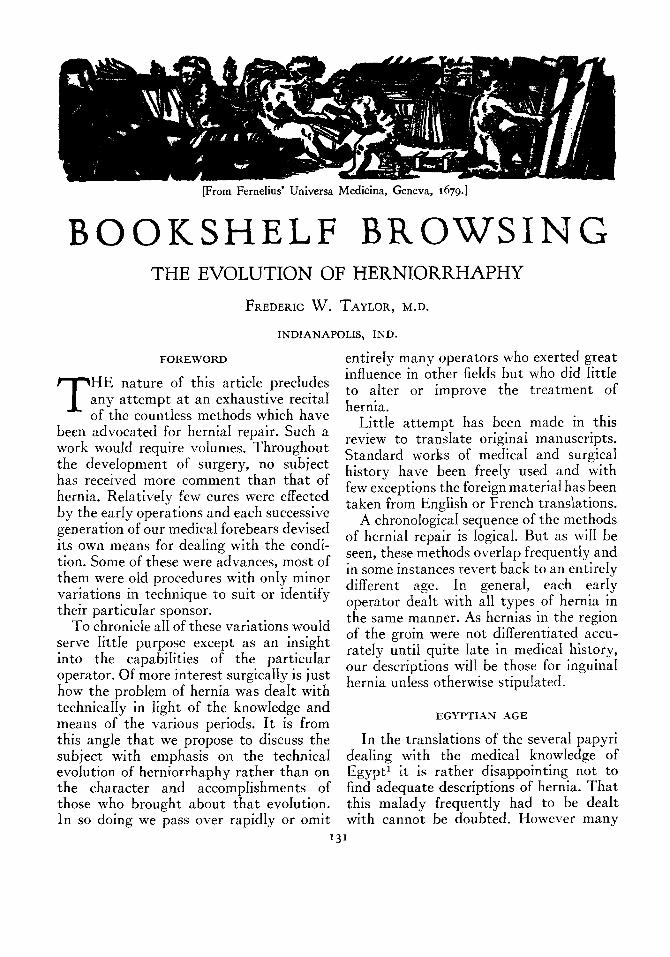
FIG. 2. Treatment of hernia by actuai cautery, (300 B.C.-18th century). Use described under second method of cure in Middle Ages.
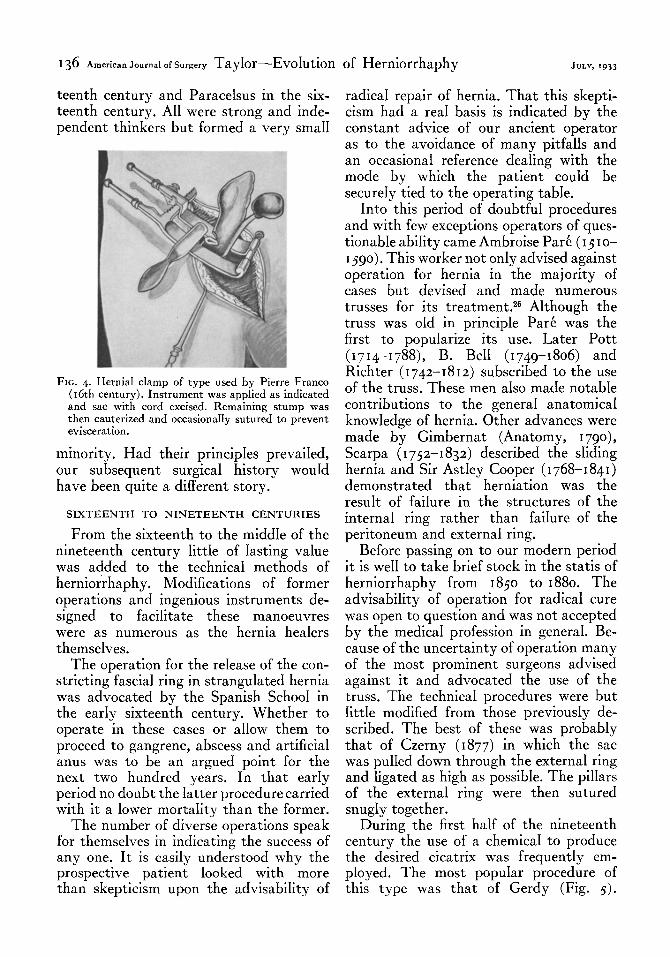
( -1315). (Iv) Cure by Ligature, Figure 3. (I) Through a small incision in the
region of the rupture a Iigature was passed around the base of the sac just above the OS pubis. (2) The contents of the sac were reduced. (3) The Iigature was tied to a smaI1 piece of wood and tightened each day unti1 it cut through the sac, fascia and muscIe which happened to be incIuded. It was hoped that this procedure wouId sea1 off the sac with scar tissue. (Advocated by Roger.)
(v) Ligature and Cuutery. (I > The incision was made over the Iower
inguina1 region and upper scrotum, the sac being dissected free from the surround- ing structures. (2) The Iigature was tied tightIy about its uppermost base and the remainder of the sac dropped back into the wound. (3) The sac was cauterized we11
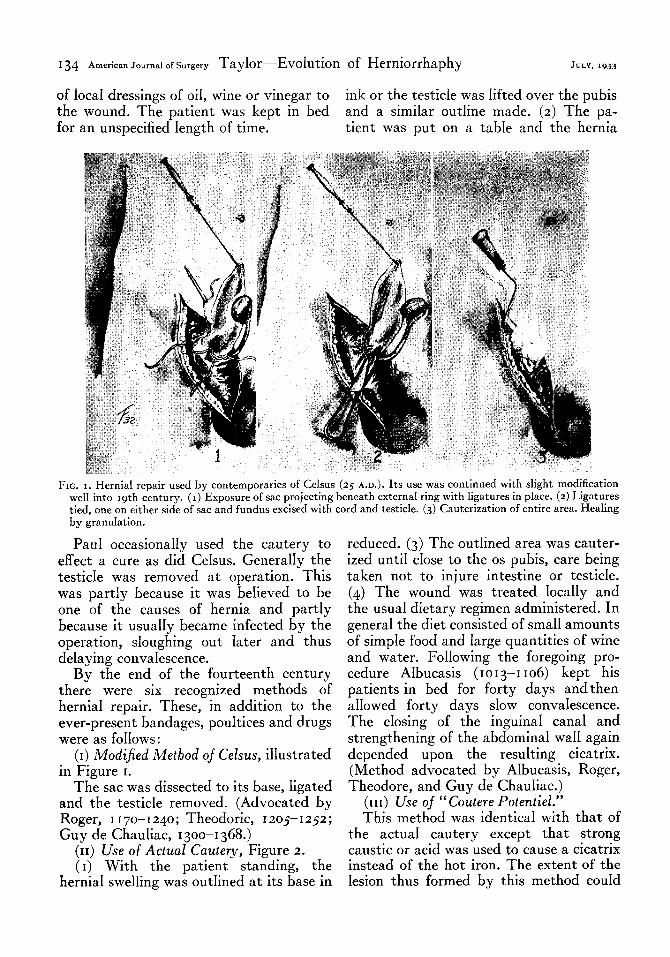
FIG. 3. Cure by ligature (11th to 19th centuries). Use described under fourth method of cure in MiddIe Ages.
(VI) Use oJ Gold Thread. (I) Through an incision paraIIe1 to the
cord, the base of the sac was dissected free from its surrounding structures, testicIe and cord being left untouched. (2) The contents of the sac were reduced. (3) GoId thread was then tied around the base of the sac and Ieft there for the wound to hea over it. This method mereIy occIuded the sac at the externa1 ring. (Later termed the “ RoyaI Operation” as it preserved the manhood of the King’s subjects.)
With the inevitable suppuration which foIIowed every operation it is no wonder that a fascia1 Iayer repair v\:as not at- tempted. In this connection we shouId mention four men who heId to the then untenabIe beIief that a surgica1 wound did not have to hea by suppuration and shouId hea by first intention. These were Hugh, Theodoric and de MondeviIIe in the thir-
136 A merican ~~~~~~~ of surgery TayIor-EvoIution of Herniorrhaphy JULY, 19x3
teenth century and ParaceIsus in the six- teenth century. AI1 were strong and inde- pendent thinkers but formed a very smaI1
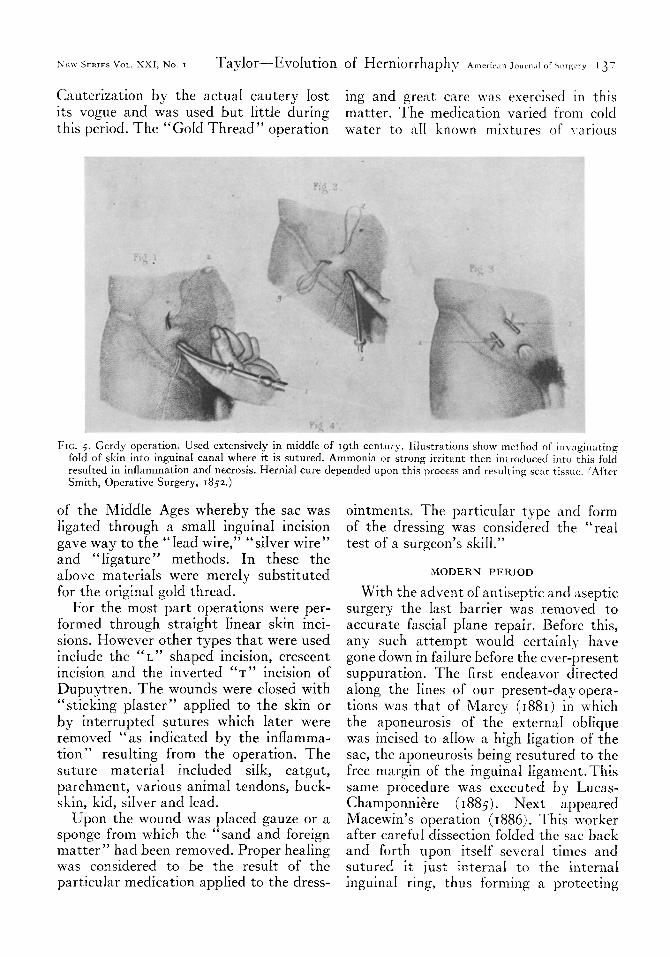
FIG. 4. Hernial clamp of type used by Pierre Franc0 (16th century). Instrument was applied as indicated and sac with cord excised. Remaining stump was then cauterized and occasionally sutured to prevent evisceration.
minority. Had their principIes prevaiIed, our subsequent surgica1 history wouId have been quite a different story.
SIXTEENTH TO NINETEENTH CENTURIES
From the sixteenth to the middIe of the
Into this period of doubtfu1 procedures and with few exceptions operators of ques- tionabIe abiIity came Ambroise Par& (15 I o- I 590). This worker not onIy advised against operation for hernia in the majority of cases but devised and made numerous trusses for its treatment.26 Although the truss was oId in principIe Pa& was the first to popuIarize its use. Later Pott (1714-1788), B. Be11 (1749-1806) and Richter (1742-1812) subscribed to the use of the truss. These men aIso made notabIe contributions to the genera1 anatomica knowIedge of hernia. Other advances were made by Gimbernat (Anatomy, 1 Tgo), Scarpa (I 752-1832) described the sIiding hernia and Sir AstIey Cooper (I 768-1841) demonstrated that herniation was the resuIt of faiIure in the structures of the interna ring rather than faiIure of the peritoneum and externa1 ring.
nineteenth century IittIe of Iasting vaIue was added to the technica methods of herniorrhaphy. Modifications of former operations and ingenious instruments de- signed to faciIitate these manoeuvres were as numerous as the hernia heaIers themseIves.
The operation for the reIease of the con- stricting fascia1 ring in stranguIated hernia was advocated by the Spanish SchooI in the earIy sixteenth century. Whether to operate in these cases or aIIow them to proceed to gangrene, abscess and artificia1 anus was to be an argued point for the next two hundred years. In that earIy period no doubt the Iatter procedure carried with it a Iower mortaIity than the former.
Before passing on to our modern period it is we11 to take brief stock in the statis of herniorrhaphy from 1850 to 1880. The advisabiIity of operation for radica1 cure was open to question and was not accepted by the medica profession in generaI. Be- cause of the uncertainty of operation many of the most prominent surgeons advised against it and advocated the use of the truss. The technica procedures were but IittIe modified from those previousIy de- scribed. The best of these was probably that of Czerny (1877) in which the sac was puIIed down through the external ring and ligated as high as possibIe. The pilIars of the external ring were then sutured snugIy together.
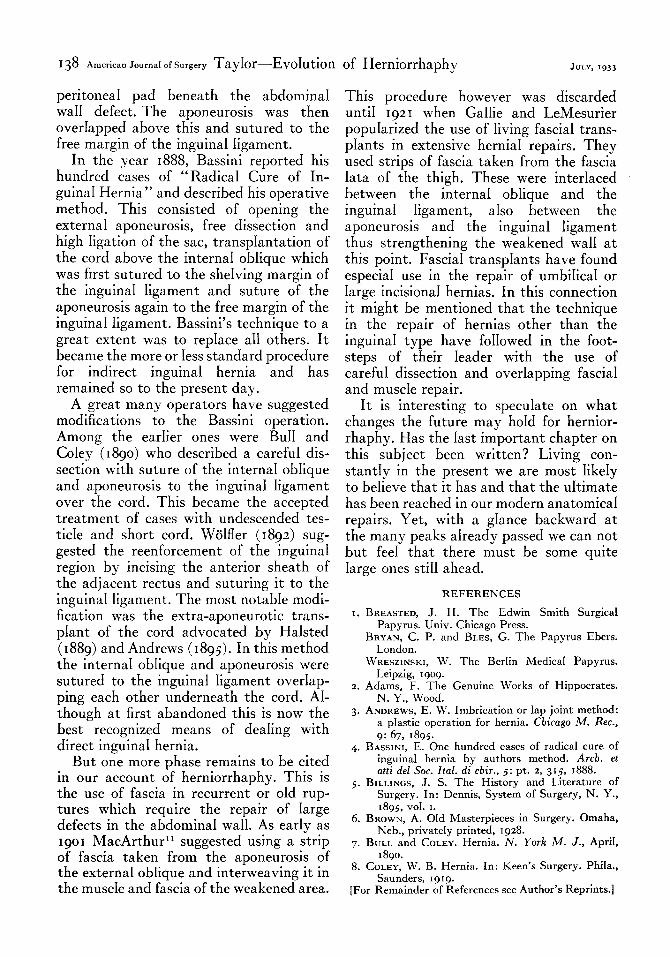
The number of diverse operations speak During the first haIf of the nineteenth for themseIves in indicating the success of century the use of a chemica1 to produce any one. It is easiIy understood why the the desired cicatrix was frequentIy em- prospective patient Iooked with more pIoyed. The most popuIar procedure of than skepticism upon the advisabiIity of this type was that of Gerdy (Fig. 5).
radica1 repair of hernia. That this skepti- cism had a rea1 basis is indicated by the constant advice of our ancient operator as to the avoidance of many pitfaIIs and an occasiona reference deaIing with the mode by which the patient couId be secureIy tied to the operating tabIe.
K‘n\\ SFKIES VOL. XXI, No. I TayIor-EvoIution of Herniorrhaphv A meric.in .iourn;ll of Sorg%~,v 13”
Cauterization by the actuaI cautery Iost ing and great care was exercised in this its vogue and was used but IittIe during matter. The medication varied from cold this period. The “GoId Thread” operation water to a11 known mixtures of \,arious
FIG. 5. Gerdy operation. Used extensively in middle of 19th century. Illustrations show method of invoginating fold of skin into inguinal canal where it is sutured. Ammonia or strong irritant then introduced into this foId resuked in inflammation and necrosis. Hernia1 cure depended upon this process and resulting scar tissue. (After Smith, Operative Surgery, 1852.)
of the MiddIe Ages whereby the sac was ligated through a smaI1 inguina1 incision gave way to the “Iead wire,” “siIver wire” and “ Iigature ” methods. In these the above materiaIs were mereIy substituted for the origina gold thread.
For the most part operations were per- formed through straight Iinear skin inci- sions. However other types that were used include the “L” shaped incision, crescent incision and the inverted “T” incision of Dupuytren. The wounds were cIosed with “stickmg pIaster” appIied to the skin or by interrupted sutures which Iater were removed “as indicated by the inffamma- tion ” resuIting from the operation. The suture materia1 incIuded silk, catgut, parchment, various anima1 tendons, buck- skin, kid, siIver and Iead.
Upon the wound was pIaced gauze or a sponge from which the “sand and foreign matter” had been removed. Proper heaIing was considered to be the resuIt of the particuIar medication appIied to the dress-
ointments. The particuIar type and form of the dressing was considered the “rea1 test of a surgeon’s skiI1.”
MODERN PERIOD
With the advent of antiseptic and aseptic surgery the Iast barrier was removed to accurate fascia1 pIane repair. Before this, any such attempt wouId certainIy have gone down in faiIure before the ever-present suppuration. The first endeavor directed aIong the Iines of our present-dayopera- tions was that of Marcy (1881) in which the aponeurosis of the externa1 obIique was incised to aIIow a high ligation of the sac, the aponeurosis being resutured to the free margin of the inguina1 Iigament.This same procedure was executed by Lucas- Champonniere ( I 883). Next appeared Macewin’s operation (I 886). This worker after carefu1 dissection foIded the sac back and forth upon itseIf severa times and sutured it just internal to the inter& inguina1 ring, thus forming a protecting
138 A merican ~~~~~~~ of surgery TayIor-EvoIution of Herniorrhaphy
peritonea1 pad beneath the abdomina1 waII defect. The aponeurosis was then overrapped above this and sutured to the free margin of the inguina1 Iigament.
In the year 1888, Bassini reported his hundred cases of “ RadicaI Cure of In- guina1 Hernia” and described his operative method. This consisted of opening the externa1 aponeurosis, free dissection and high Iigation of the sac, transpIantation of the cord above the interna obIique which was first sutured to the sheIving margin of the inguinal Iigament and suture of the aponeurosis again to the free margin of the inguinal Iigament. Bassini’s technique to a great extent was to repIace a11 others. It became the more or Iess standard procedure for indirect inguina1 hernia and has remained so to the present day.
A great many operators have suggested modifications to the Bassini operation. Among the earIier ones were BuII and CoIey (1890) who described a carefu1 dis- section with suture of the interna obIique and aponeurosis to the inguina1 Iigament over the cord. This became the accepted treatment of cases with undescended tes- ticIe and short cord. WaIfI er (1892) sug- gested the reenforcement of the inguinal region by incising the anterior sheath of the adjacent rectus and suturing it to the inguina1 Iigament. The most notabIe modi- fication was the extra-aponeurotic trans- pIant of the cord advocated by HaIsted (1889) and Andrews (1895). In this method the interna obIique and aponeurosis were sutured to the inguina1 Iigament overIap- ping each other underneath the cord. AI- though at first abandoned this is now the best recognized means of deaIing with direct inguina1 hernia.
But one more phase remains to be cited in our account of herniorrhaphy. This is the use of fascia in recurrent or oId rup- tures which require the repair of Iarge defects in the abdomina1 waI1. As earIy as IgoI MacArthur” suggested using a &rip of fascia taken from the aDoneurosis of
I
the externa1 oblique and interweaving it in the muscIe and fascia of the weakened area.
This procedure however was discarded unti1 Igzr when GaIIie and LeMesurier popuIarized the use of Iiving fascia1 trans- pIants in extensive hernia1 repairs. They used strips of fascia taken from the fascia Iata of the thigh. These were interlaced between the interna obIique and the inguina1 Iigament, aIso between the aponeurosis and the inguina1 Iigament thus strengthening the weakened waI1 at this point. Fascia1 transpIants have found especia1 use in the repair of umbiIica1 or Iarge incisiona hernias. In this connection it might be mentioned that the technique in the repair of hernias other than the inguina1 type have foIIowed in the foot- steps of their Ieader with the use of carefu1 dissection and overIapping fascia1 and muscIe repair.
It is interesting to specuIate on what changes the future may hoId for hernior- rhaphy. Has the Iast important chapter on this subject been written? Living con- stantIy in the present we are most IikeIy to beIieve that it has and that the uItimate has been reached in our modern anatomica repairs. Yet, with a gIance backward at the many peaks aIready passed we can not but fee1 that there must be some quite Iarge ones stiI1 ahead.
REFERENCES
I. BREASTED, J. H. The Edwin Smith SurgicaI Papyrus. Univ. Chicago Press.
BRYAN, C. P. and BLES, G. The Papyrus Ebers. London.
WRESZINSKI, W. The BerIin MedicaI Papyrus. Leipzig, 1909.
2. Adams, F. The Genuine Works of Hippocrates. N. Y., Wood.
3. ANDREWS, E. W. Imbrication or Iap joint method: a pIastic operation for hernia. Cbicqo M. Rec., g:-67, 1895:
A. BASSINI. E. One hundred cases of radica1 cure of 1
inguiial hernia by authors method. Arch. et atti de1 Sot. Ital. di cbir., 3: pt. 2, 315, 1888.
5. BILLINGS, J. S. The History and Literature of Surgery. In: Dennis, System of Surgery, N. Y., 1895, vo1. I.
6. BROWN, A. OId Masterpieces in Surgery. Omaha, Neb., privateIy printed, 1928.
7. BULL and COLEY. Hernia. N. York M. J., ApriI, 1890.
8. COLEY, W. B. Hernia. In: Keen’s Surgery. Phila., Saunders, IgIg.
[For Remainder of References see Author’s Reprints.]