Embed Size (px)
Citation preview

2013-11-21
1
The Evolving Management of Advanced Lung Cancerof Advanced Lung Cancer
CAGPO October 19th, 2013
M. Vincent
MB ChB, FRCPC, MRCP(UK)Staff Medical Oncologist
Thoracic & GI MDT
London Regional Cancer Program
Professor
(Senate Stream)
Dept. of Oncology

2013-11-21
2
CONFLICT OF INTEREST• CEO:
Sarissa, Inc.• Scientific Advisory Boards:
SYM BioSciencesCritical Outcomes Technology Inc.Capital Royalty, Inc.
• Board of Directors:Lorus Therapeutics Inc.
• Speaker’s BureauBristol Myers SquibbBristol Myers SquibbEli Lilly, Inc.
• Honoraria:AmgenAstra ZenecaBristol Myers SquibbEli Lilly Inc.Hoffman La RocheSanofi-AventisBoehringer-Ingleheim
• Research Funding:Hoffman La Roche

2013-11-21
3
OBJECTIVES
• Clear overview of both A-NSCLC and SCLC
• Explore areas of research and interest in Small Cell Lung Cancer
• Emphasize biomarker testing & Rx decision impact
• Intro www.MyOncologyResource.com, online A-NSCLC Rx guide
• Case Study

2013-11-21
4

2013-11-21
5

2013-11-21
6
Lung Cancer: Histology
10% to 15%
Small-cellcarcinoma
L ll
Adenocarcinoma
40%10% to 15%
2 % 30%
Large-cell carcinoma
American Cancer Society. Lung cancer (non-small-cell). 2013.
25% to 30%
Squamous cell carcinoma

2013-11-21
7
Sensitivity.........87%Specificity.........98%
Sensitivity.........93%...........94%Specificity.........87%...........97%
Histopathology, 61:1017

2013-11-21
8

2013-11-21
9
Lung Cancer: Biomarkers in Adenocarcinoma

2013-11-21
10
EGFR Mutations Associated with Sensitivity to EGFR-TKIs
Nat Rev Cancer. 2007; 7: 169-81.

2013-11-21
11
GEFITINIB
a | Simplified illustration of signal transduction through the epidermal growth factor receptor (EGFR).
Ligand binding causes receptor dimerization. This leads to receptor autophosphorylation, which is inhibited by gefitinib.
b | Structure of gefitinib and its in vitro inhibitory activity against various tyrosine kinases. Gefitinib was originally
identified from structure–activity studies based around a 4-anilinoquinazoline lead series MAPK

2013-11-21
12
2003, June 12 2003, Nov. 28
CASE REPORT: Response to an EGFR-TKI
A RARE EVENT IN AN UNSELECTED CAUCASIAN
, ,
This was at a time before the mutation was recognised

2013-11-21
13

2013-11-21
14

2013-11-21
15
Rapid Response to CrizotinibRapid Response to Crizotinib
Pre-TreatmentPre-Treatment Crizotinib x 12 weeksCrizotinib x 12 weeks

2013-11-21
16
SO, HOW DO WE RECONCILE
HISTOLOGYHISTOLOGY
WITH
MOLECULAR BIOMARKERS?

2013-11-21
17
A-NSCLC
Non-Squamous
First, we need an approach to histopathology
Squamous Squamous
“NestedSets”AdenoCa LargeSets
Signet Cribri- BAC BAC Pap- Micro- Acinar SolidRing form Muc Non- illary pap
Muc
Non-N-E
Neuro-endocrine

2013-11-21
18
Acinar AdenocaAcinar Adenoca(±13% EGFR mt) (±35% EGFR mt)
Papillary AdenocaPapillary Adenoca Cribriform
80% ALK +
(? 35% EGFR mt+)
Micropapillary Micropapillary Solid Adenoca with MucinSolid Adenoca with Mucin Signet Ring
65% ALK +(Never EGFR mt+)
Bronchioloalveolar Adenoca, Bronchioloalveolar Adenoca, NonNon--mucinousmucinous
Bronchioloalveolar Adenoca,Bronchioloalveolar Adenoca,MucinousMucinous
(50% EGFR mt+) (Never EGFR mt+)

2013-11-21
19
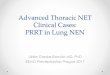
A-NSCLC: Algorithm Scaffold
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+
ALK+ WT/WT UNKNOWN
1L
1LM
2L2L
3L
2013-11-21
20
A-NSCLC: Algorithm Scaffold
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT UNKNOWN
1L
1LM
2L
3L

2013-11-21
21
Adenocarcinoma –Estimated Genomic Probabilities of KRAS and EGFR
Mutations
East Asia West
(Japan, Korea, Taiwan, HK) (USA, Australia)
6 studies 2 studies
n = 814 n = 116
Neversmokers
EGFR mt
KRAS mt
neither
70%
1%
29%
37%
0%
63%
Ever-smokers
EGFR mt
KRAS mt
neither
29%
17%
54%
8%
41%
51%
Shigematsu, Sakema, Takema, Bae, Tam
2013-11-21
22
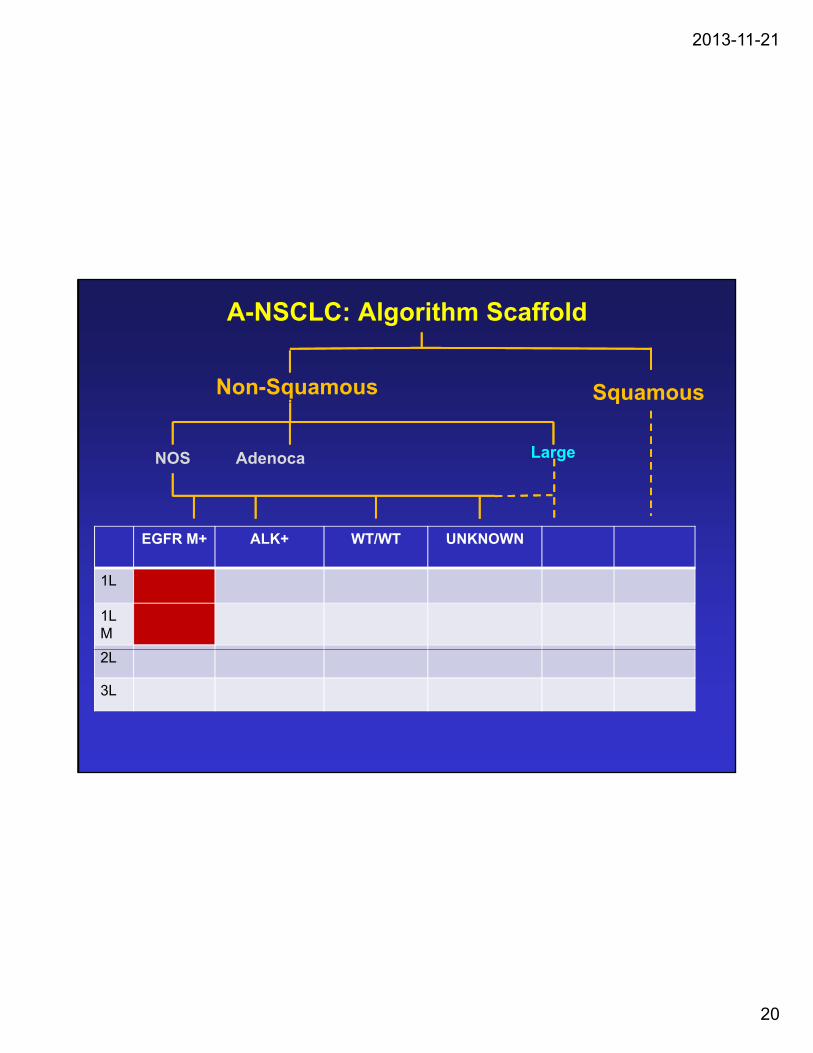
IPASS Study design
PatientsEndpoints
Gefitinib250 mg/day
1:1 randomization
Patients• Age ≥18 years
• Life expectancy≥ 12 weeks
• Adenocarcinoma histology
• Never smokers or light ex-smokers*
Primary• Progression free survival (non-inferiority)
Secondary• Objective response rate• Quality of life• Disease related symptoms
Carboplatin AUC 5 or 6 and Paclitaxel 200mg/m2 3 wkly
• PS 0-2
• Stage IIIB/IV
• Measurable disease
y p• Overall survival• Safety and tolerability
Exploratory• Biomarkers
•EGFR mutation•EGFR gene copy number•EGFR protein expression
22
*Never smokers:<100 cigarettes in lifetime; light ex-smokers: stopped 15 years ago and smoked 10 pack yrs
Carboplatin/paclitaxel was offered to gefitinib patients upon progression
PS, performance status; EGFR, epidermal growth factor receptor
EGFR protein expression

2013-11-21
23
Objective response rate in EGFR mutation positive and negative patients
Gefitinib Carboplatin / paclitaxel
EGFR M+ odds ratio (95% CI)= 2.75 (1.65, 4.60), p=0.0001
EGFR M- odds ratio (95% CI)= 0 04 (0 01 0 27) p=0 0013
Overallresponse
71.2%
47.3%
= 0.04 (0.01, 0.27), p=0.0013 rate (%)
1.1%
23.5%
(n=132) (n=129) (n=91) (n=85)
Odds ratio >1 implies greater chance of response on gefitinib Mok et al, Chicago 2008

2013-11-21
24
Progression-free survival in EGFR mutation positive and negative patients
EGFR mutation positive EGFR mutation negative
G fiti ib ( 91)
HR (95% CI) = 0.48 (0.36, 0.64)
p<0.0001
Gefitinib (n=132)Carboplatin / paclitaxel(n=129)
HR (95% CI) = 2.85 (2.05, 3.98)p<0.0001
0.6
0.8
1.0
rog
ress
ion-
free
vi
val
0.6
0.8
1.0
rog
ress
ion-
free
viva
l
Gefitinib (n=91)Carboplatin / paclitaxel (n=85)
0 4 8 12 16 20 240.0
0.2
0.4
6
Pro
babi
lity
of p
rsu
rv
At risk :
0 4 8 12 16 20 240.0
0.2
0.4
6
Pro
babi
lity
of p
rsu
rv
Months Months
Treatment by subgroup interaction test, p<0.0001
ITT populationCox analysis with covariates
132 71 31 11 3 0129 37 7 2 1 0
108103
GefitinibC / P
At risk :91 4 2 1 0 085 14 1 0 0 0
2158
Mok et al, Chicago 2008

2013-11-21
25
Overall Survival in EGFR mutation positive and negative
patientspatients
Fukuoka et al. JCO 2011
2013-11-21
26

2013-11-21
27
2013-11-21
28
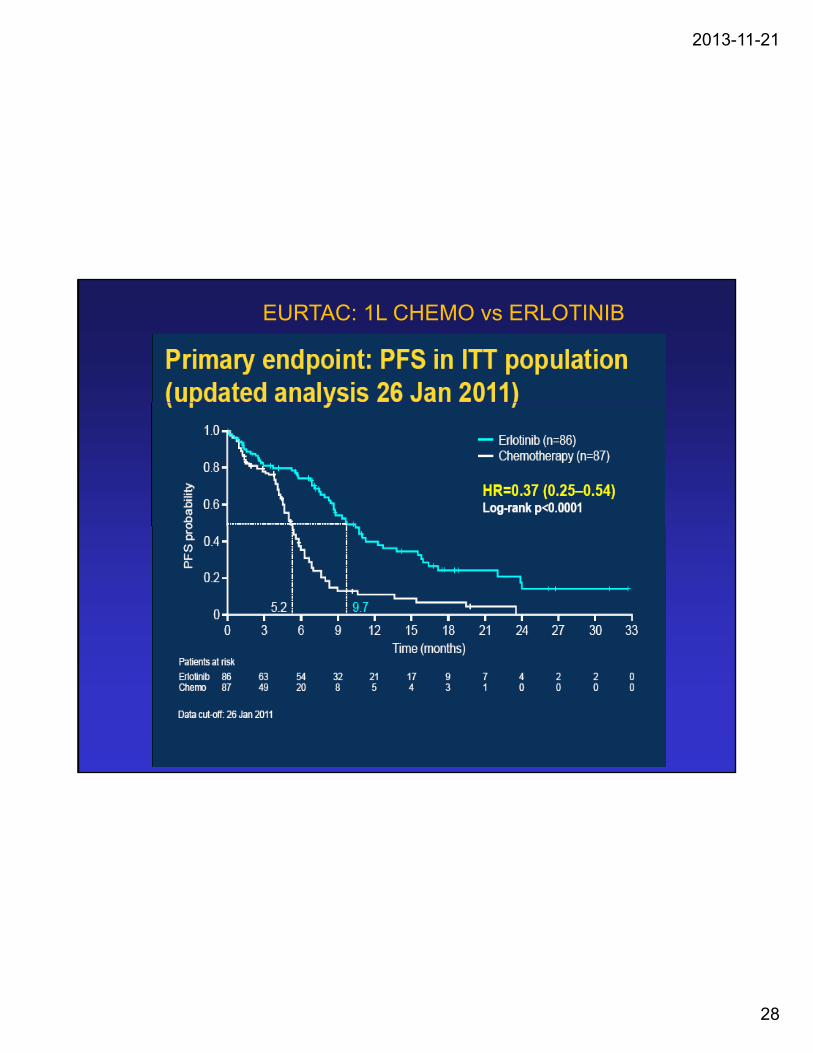
EURTAC: 1L CHEMO vs ERLOTINIB
2013-11-21
29
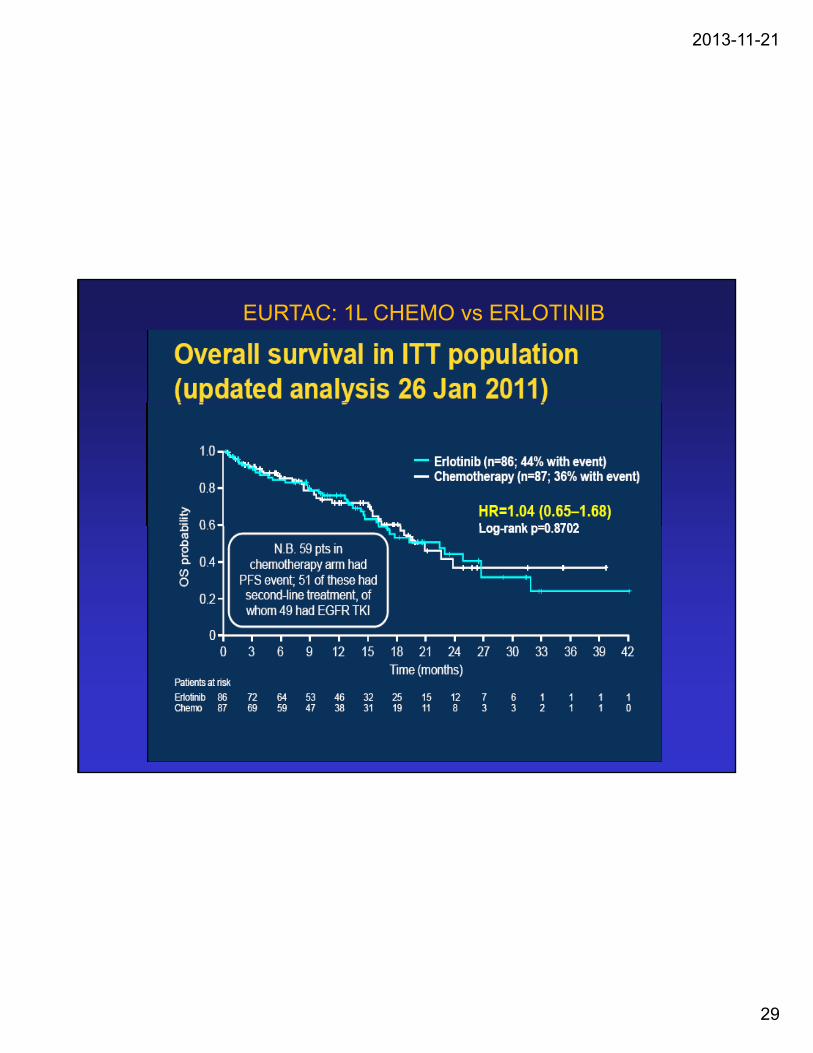
EURTAC: 1L CHEMO vs ERLOTINIB

2013-11-21
30

2013-11-21
31
2013-11-21
32
2013-11-21
33

2013-11-21
34
EGFR M+M+
Iressa … IPASS
or
Tarceva … EURTAC
or
1L+
1LM
Tomtovok … LUX-Lung 3

2013-11-21
35
A-NSCLC
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT UNKNOWN
1L+1LM
IressaorTarcevaorTomtovokTomtovok
2L Platinum doublet Alimta
3L TKI re-challenge?
2013-11-21
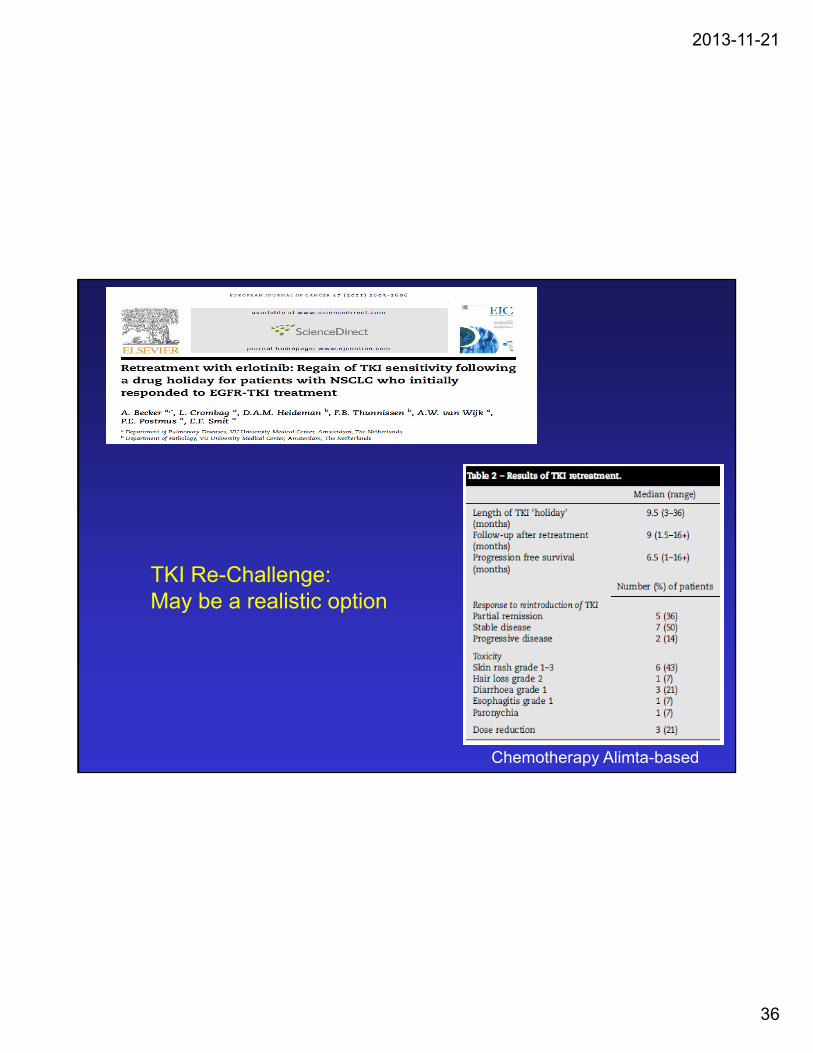
36
TKI Re-Challenge: May be a realistic option
Chemotherapy Alimta-based

2013-11-21
37
A-NSCLC: Algorithm Scaffold
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+
ALK+ WT/WT UNKNOWN
1L
1LM
2L2L
3L

2013-11-21
38

2013-11-21
39
ALK +
Xalkori (crizotinib)1L
US FDA 26/8/11+1LM

2013-11-21
40
Crizotinib(n=172a)
Pemetrexed(n=99a)
Docetaxel(n=72a)
PROFILE 1007:PFS of 2L Crizotinib vs Pemetrexed or Docetaxel
t
100(n=172 ) (n=99 ) (n=72 )
Events, n (%) 100 (58) 72 (73) 54 (75)
Median, mo 7.7 4.2 2.6
HRb (95% CI) 0.59 (0.43 to 0.80) 0.30 (0.21 to 0.43)
P 0.0004 <0.0001
of
surv
ival
wit
ho
ut
ress
ion
(%
)
80
60
40
Pro
bab
ility
op
rog 40
20
00 5 10 15 20 25
Time (months)
172 93 38 11 2 099 36 12 3 1 072 13 3 1 0
No. at riskCrizotinib
PemetrexedDocetaxel
aAs-treated population: excludes 1 patient in crizotinib arm who did not receive study treatment and 3 patients in chemotherapy arm who did not receive study treatment; bvs crizotinib

2013-11-21
41
ORRa by Independent Radiologic Review
ORR ratio: 3 4 (95% CI: 2 5 to 4 7); P<0 0001
65.3
ORR ratio: 3.4 (95% CI: 2.5 to 4.7); P<0.0001
Crizotinib (n=173b)
Chemotherapy (n=174b)80
60
65.7
Crizotinib (n=172c)
Pemetrexed (n=99c)
Docetaxel (n=72c)80
60
19.5OR
R (
%)
60
40
20
29.3
6 9
60
40
20
aRECIST v1.1; bITT population; cas-treated population
20
0Treatment
6.9
Treatment
20
0

2013-11-21
42
A-NSCLC: alternative schema for ALK +
Non-Squamous SquamousSquamous
NOS Adenoca Large
EGFR M+ ALK+ WT/WT UNKNOWN
1L
Platinum doublet
X 4
1LM Alimta PD
2L XalkoriPD…and
beyond?
2013-11-21
43
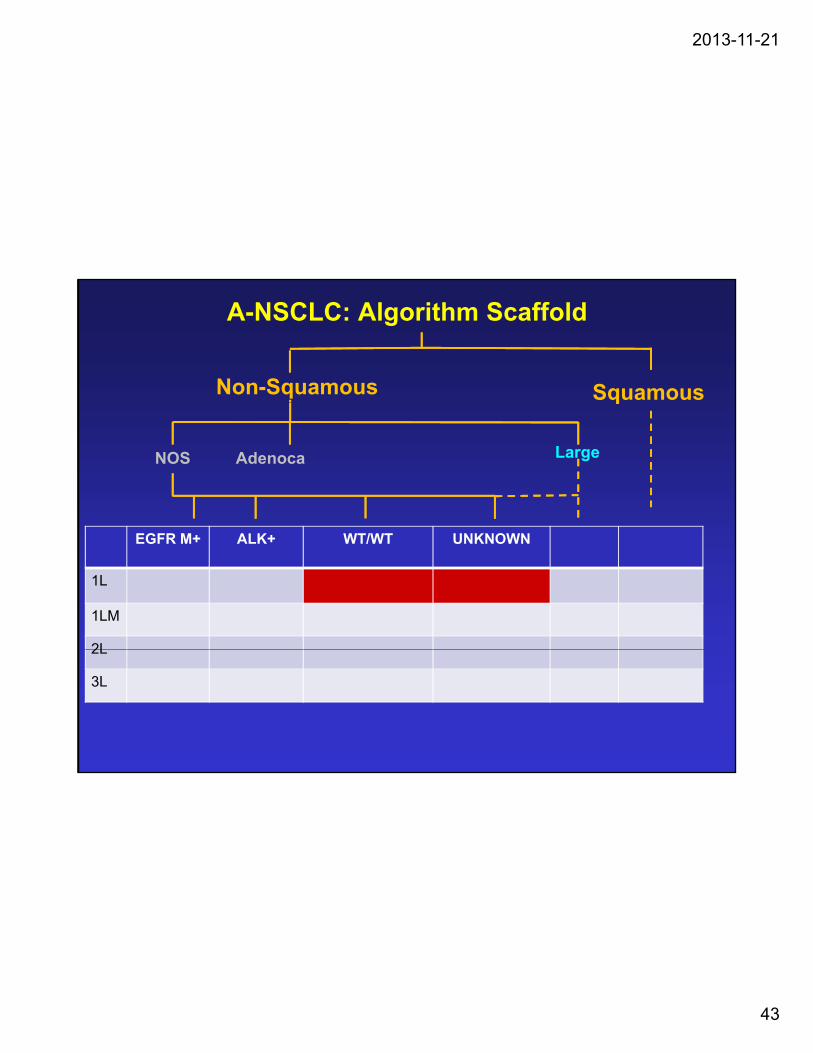
A-NSCLC: Algorithm Scaffold
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT UNKNOWN
1L
1LM
2L2L
3L

2013-11-21
44
NON-SMALL CELL LUNG CANCER
1st generation 2nd generation 3rd generation
Cyclophosphamide Ifosphamide PaclitaxelDocetaxel
Doxorubicin Mitomycin C GemcitabineDoxorubicin Mitomycin C Gemcitabine
Cisplatin (low dose) Cisplatin (high dose)Carboplatin
Oxaliplatin
Vincristine VinblastineVindesine
Vinorelbine
Methotrexate Etoposide Irinotecan
2013-11-21
45
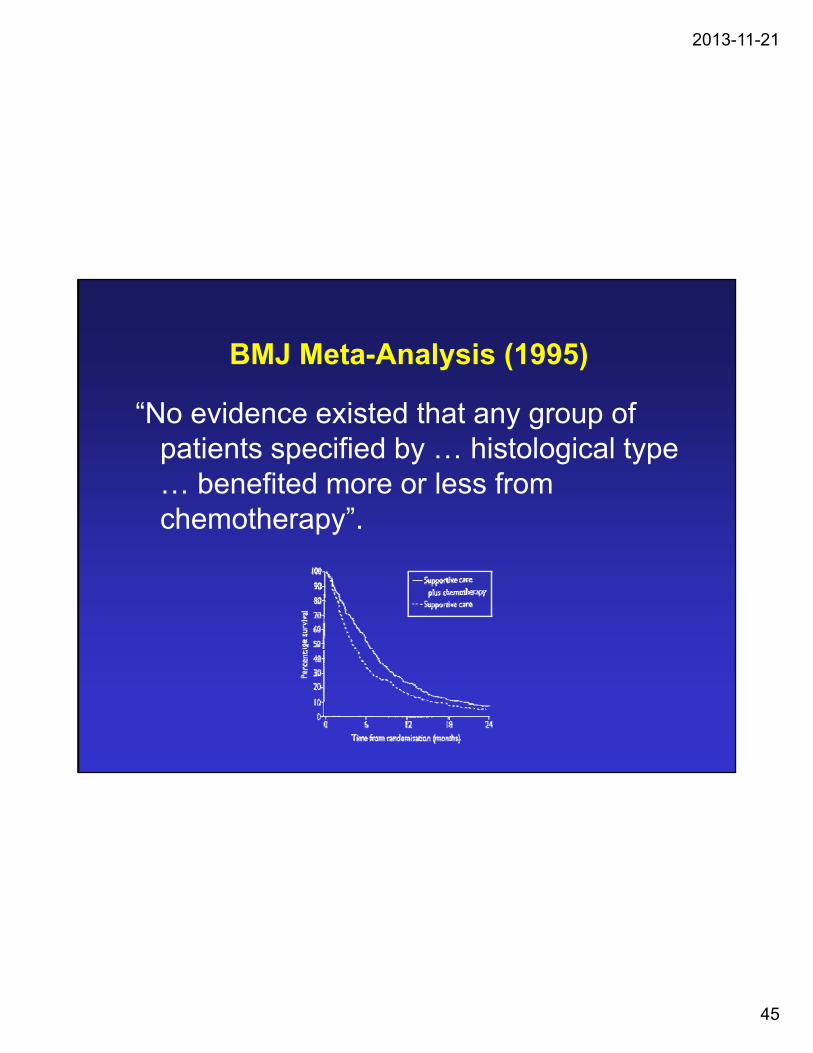
BMJ Meta-Analysis (1995)
“N id i d h f“No evidence existed that any group of patients specified by … histological type … benefited more or less from chemotherapy”.chemotherapy .

2013-11-21
46
NON-SMALL CELL LUNG CANCER
1st generation 2nd generation 3rd generation
Cyclophosphamide Ifosphamide PaclitaxelDocetaxel
Doxorubicin Mitomycin C GemcitabineDoxorubicin Mitomycin C Gemcitabine
Cisplatin (low dose) Cisplatin (high dose)Carboplatin
Oxaliplatin
Vincristine VinblastineVindesine
Vinorelbine
Methotrexate Etoposide Irinotecan

2013-11-21
47
Hitting the WallFirst-line chemotherapy options in NSCLC(E1594): comparable efficacy with platinum
doublets
1.0
0.8
0.6
Cisplatin/paclitaxelCisplatin/gemcitabineCisplatin/docetaxelf
surv
ival
Therapeutic plateau: overall survival <12 months
0.6
0.4
0.2
Cisplatin/docetaxelCarboplatin/paclitaxel
Pro
bab
ility
of
Schiller, et al. NEJM 2002
00 5 10 15 20 25 30
Time (months)
NSCLC = non-small cell lung cancer

2013-11-21
48
• Log-rank test for comparing
ECOG 1594: Efficacies by Histology
– OS and PFS distributions among different histology groups
– Survival in each histology group for different chemotherapy regimen
• Results:
– No difference in OS and PFS between the four histology groups
– No survival difference between the four chemotherapy regimens in each histology group
Regardless of histology types, OS and PFS were similar in
WCLC 2009 – Hoang et al, Abstract # PD6.4.1
chemonaive NSCLC patients treated with standard platin-based doublets involving paclitaxel, docetaxel, or gemcitabine!

2013-11-21
49
JMDB:Cis/Pem vs. Cis/Gem in First-Line NSCLC: Study Design
Randomization Factors
• Stage
• Performance status (PS) (0 vs 1)
Cisplatin 75 mg/m2 day 1 + Pemetrexed 500 mg/m2 day 1
Each cycle repeated
Cisplatin 75 mg/m2 day 1 + Gemcitabine 1250 mg/m2 days 1 & 8
(PS) (0 vs 1)
• Gender
• Histologic vs cytologic diagnosis
• History of brain metastases
REach cycle repeated
every 3 weeks up to 6 cycles
Gemcitabine 1250 mg/m days 1 & 8
Vitamin B12, folate, and dexamethasone given in both arms
Scagliotti et al. J Clin Oncol 2008 (In Press).
Cis/Pem, cisplatin/pemetrexed; Cis/Gem, cisplatin/gemcitabine

2013-11-21
50
Cis/Pem vs. Cis/Gem in First-line NSCLC: Overall Survival in Squamous Cell
Carcinoma and Adenocarcinoma / Large C llCell
1.0
ab
ilit
y
0.7
0.8
0.9 Cis/Pem in Ad or La (N=512) 11.8 mos (10.4, 13.2)
Cis/Gem in Ad or La (N=488) 10.4 mos (9.6, 11.2)
OS Median (95% CI)
Cis/Pem in Sq (N=244) 9.4 mos (8.4,10.2)
Cis/Gem in Sq (N=229) 10.8 mos (9.5, 12.1)
vera
ll S
urv
iva
l P
rob
a
0 2
0.3
0.4
0.5
0.6
0 q ( ) ( , )
Overall Survival Time (months) in Squamous Patients0 6 12 18 24 30
Ov
0.0
0.1
0.2

2013-11-21
51
Figure 1. Kaplan–Meier overall survival curves foroverall survival curves for the pemetrexed versus docetaxel study for each of the histologic . Subgroups:adenocarcinoma,large cell carcinoma, squamous cell carcinoma, and other NSCLC/NOS histologieshistologies.
Scagliotti, The Oncologist 2009; 14: 253-63

2013-11-21
52
A-NSCLC: Algorithm Scaffold
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT UNKNOWN
1L
1LM
2L2L
3L
2013-11-21
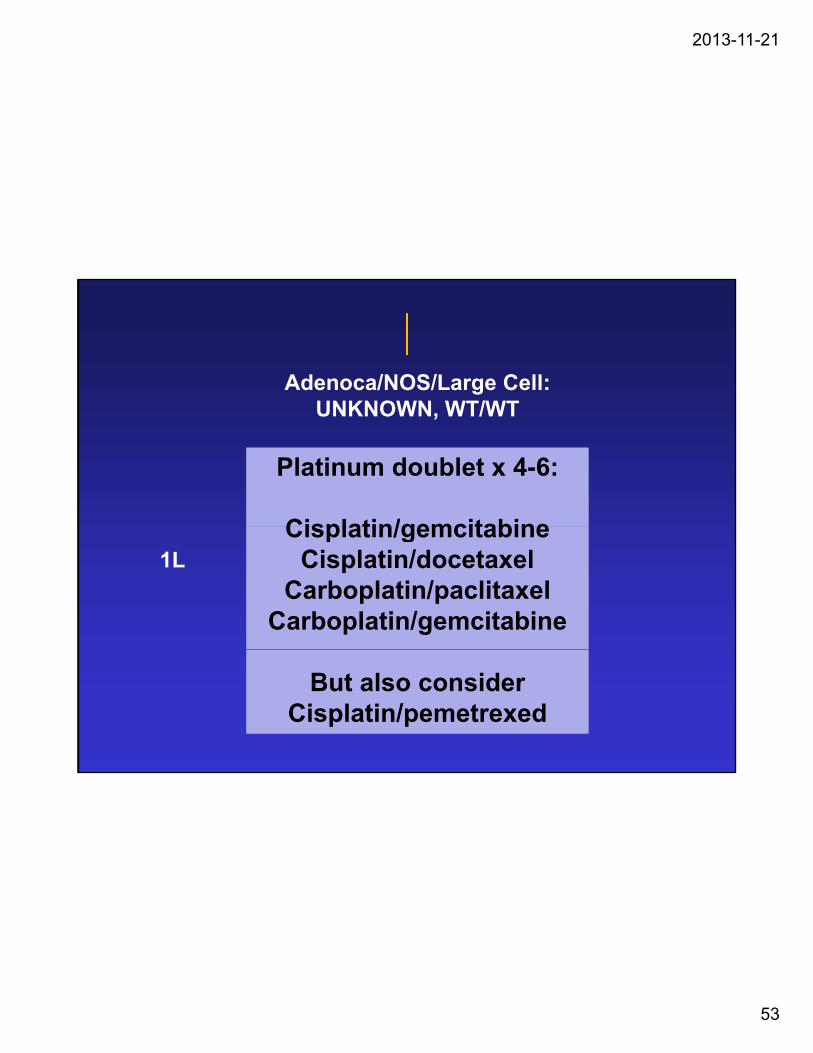
53
Adenoca/NOS/Large Cell:UNKNOWN WT/WTUNKNOWN, WT/WT
Platinum doublet x 4-6:
Cisplatin/gemcitabineCisplatin/gemcitabineCisplatin/docetaxel
Carboplatin/paclitaxelCarboplatin/gemcitabine
1L
But also considerCisplatin/pemetrexed

2013-11-21
54
Double-blind Placebo-controlled Multicenter Phase III Trial
JMEN: Study Design
Stage IIIB/IV NSCLC ECOG PS 0-1 4 prior cycles of gem,
doc or tax + cis or
Double-blind, Placebo-controlled, Multicenter, Phase III Trial
Pemetrexed 500 mg/m2
(d1,q21d) + BSC (N=441)*
doc, or tax + cis or carb, with CR, PR, or SD
Randomization factors: • gender• PS
Primary Endpoint = PFS2:1
Randomization
• PS• stage• best tumor
response• non-platinum drug• brain mets
*B12, folate, and dexamethasone given in both arms
Placebo (d1, q21d) + BSC (N=222)*

2013-11-21
55
Progression-free Survival by Histology
NonNon--squamous squamous Squamous Squamous
0 70.80.91.0
0 70.80.91.0
Pro
babi
lity
HR=0.47 (95% CI: 0.37-0.6)P <0.00001
HR=1.03 (95% CI: 0.77-1.5)P =0.896
0.10.20.30.40.50.60.7
0 00.10.20.30.40.50.60.7
Pemetrexed 4.4 mos Pemetrexed 2.4 mos
Placebo 1 8 mos
Placebo 2.5 mosog
ress
ion-
free
P
0 3 6 9 12 15 18 21 240.0
0 3 6 9 12 15 18 21 240.01.8 mos 5 os
Time (months) Time (months)
Pro

2013-11-21
56
Overall Survival by Histology
NonNon--squamous (n=481)squamous (n=481) Squamous (n=182)Squamous (n=182)
0.8
0.9
1.0
0.8
0.9
1.0
HR=0.70 (95% CI: 0.56-0.88)P =0.002
HR=1.07 (95% CI: 0.49–0.73)P =0.678
bilit
y
0.2
0.3
0.4
0.5
0.6
0.7
0.2
0.3
0.4
0.5
0.6
0.7
Pemetrexed 15.5 mos Pemetrexed 9.9 mos
Placebo 10.3 mos
Placebo 10.8 mosSu
rviv
al P
roba
b
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 480.0
0.1
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 480.0
0.1
S
Time (months) Time (months)

2013-11-21
57
Pemetrexed(N = 441)
Placebo(N = 222)
Treatment-related Toxicities*
( )%
( )%
Grade 3/4 Grade 3/4
Neutropenia‡ 3 0
Anemia 3 1
Leukopenia 2 1eu ope a
Fatigue‡ 5 1
Anorexia 2 0
Infection 1 0
Diarrhea 1 0
Nausea 1 1Nausea 1 1
Vomiting <1 0
Sensory neuropathy 1 0
Mucositis/Stomatitis 1 0*NCI CTC version 3.0‡P <0.05 for grade 3/4 rates of neutropenia and fatigue
2013-11-21
58
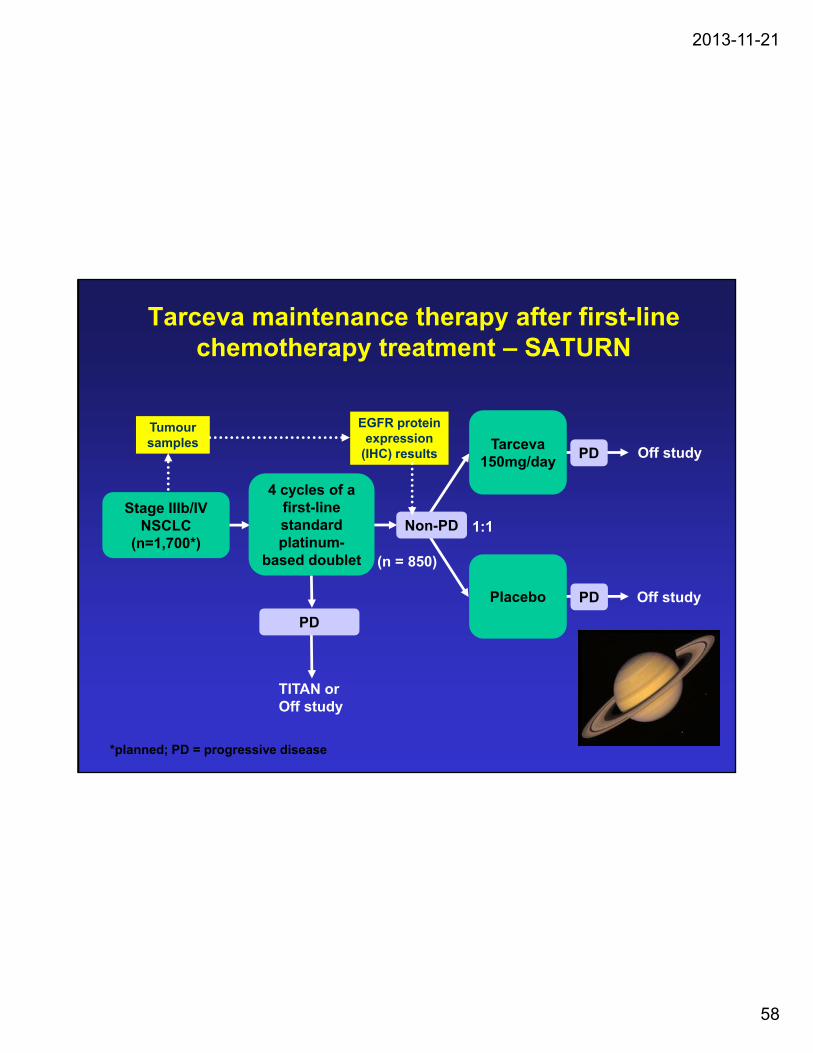
Tarceva maintenance therapy after first-line chemotherapy treatment – SATURN
Stage IIIb/IV NSCLC Non-PD
Tarceva150mg/day
Off studyPD
1:1
4 cycles of a first-line standard
Tumour samples
EGFR protein expression
(IHC) results
Placebo
NSCLC (n=1,700*)
Non-PD
PD
(n = 850)
1:1standard platinum-
based doublet
PD
Off study
TITAN or Off study
*planned; PD = progressive disease

2013-11-21
59
OS in patients with non-squamous disease
1.0
0.8
0 6bili
ty
HR=0.79 (0.64–0.96)
Log-rank p=0.0194
Erlotinib (n=272)0.6
0.4
0.2
OS
pro
bab
Erlotinib (n=272)
Placebo (n=257)
00 3 6 9 12 15 18 21 24 27 30 33 36
Time (months)
10.5 13.7
Cappuzzo et al. ESMO 2009

2013-11-21
60
OS according to response to first-line chemotherapy (ITT population)
bili
ty
1.0
0.8
0.6
1.0
0.8
0.6
Log-rank p=0.0019HR=0.72 (0.59–0.89)
Log-rank p=0.6181HR=0.94 (0.74–1.20)
SD CR/PR
OS
pro
ba 0.6
0.4
0.2
09.6 11.9
0.6
0.4
0.2
012.0 12.5
Erlotinib (n=252)
Placebo (n=235)
Erlotinib (n=184)
Placebo (n=210)
0 3 6 9 12 15 18 21 24 27 30 33 36
Time (months)
0 3 6 9 12 15 18 21 24 27 30 33 36
Time (months)
Measured from time of randomisation into the maintenance phase
Multivariate HR for OS in SD population 0.71, p=0.0019
2013-11-21
61
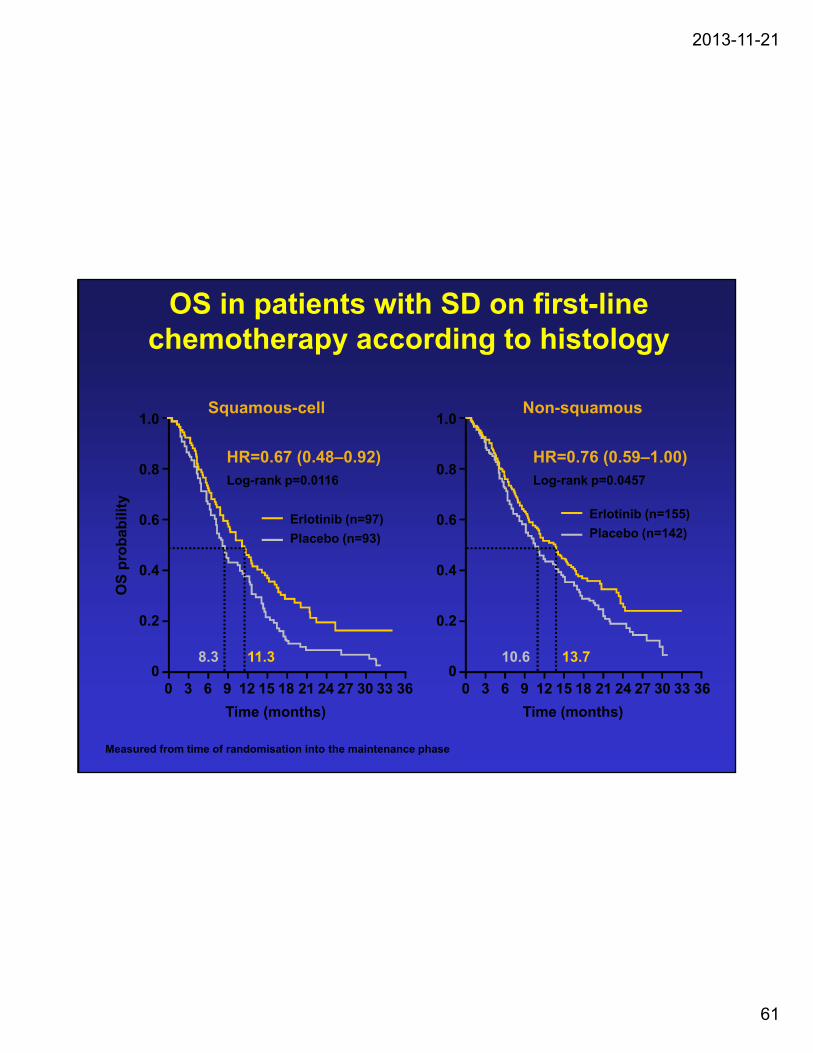
OS in patients with SD on first-line chemotherapy according to histology
S ll NSquamous-cell1.0
0.8
0.6
HR=0.76 (0.59–1.00)Log-rank p=0.0457
Erlotinib (n=155)
Non-squamous
HR=0.67 (0.48–0.92)Log-rank p=0.0116
Erlotinib (n=97) bili
ty
1.0
0.8
0.6
0.4
0.2
Placebo (n=142)( )
Placebo (n=93)
OS
pro
bab
0.4
0.2
00 3 6 9 12 15 18 21 24 27 30 33 36
Time (months)
10.6 13.70
0 3 6 9 12 15 18 21 24 27 30 33 36
Time (months)
8.3 11.3
Measured from time of randomisation into the maintenance phase
2013-11-21
62
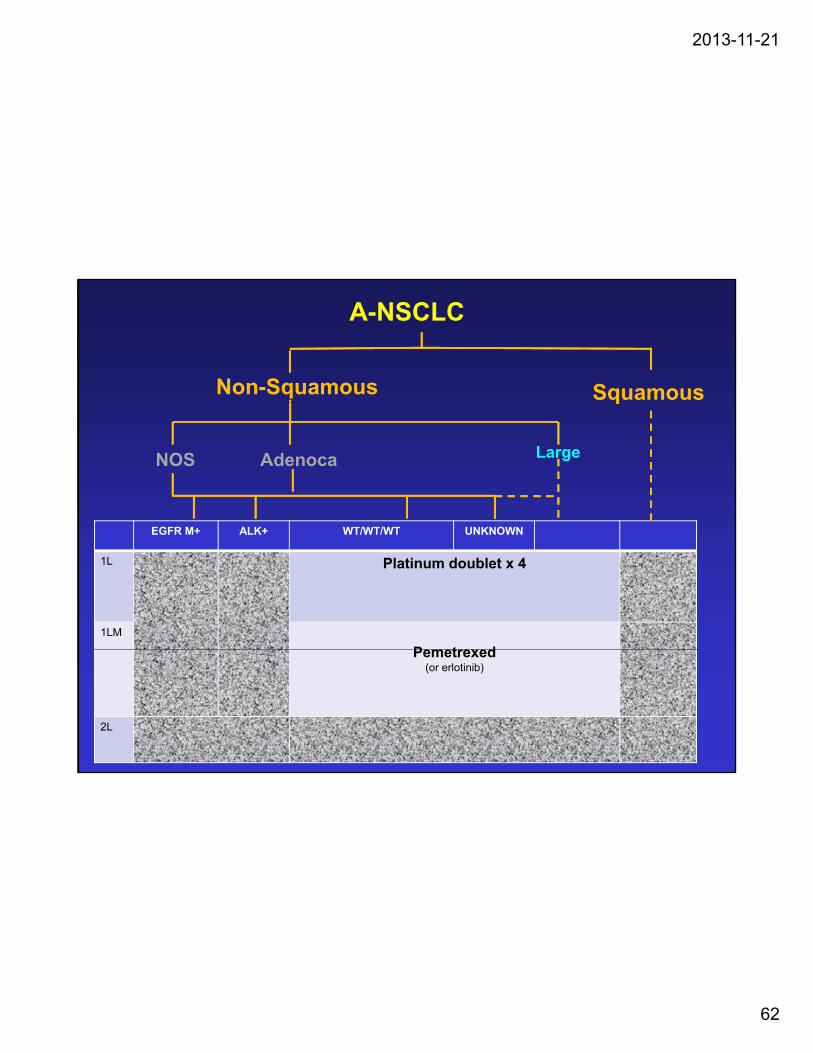
A-NSCLC
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT/WT UNKNOWN
1L Platinum doublet x 4
1LM
PemetrexedPemetrexed(or erlotinib)
2L

2013-11-21
63
A-NSCLC: Algorithm Scaffold
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT UNKNOWN
1L Platinum Doublet
(non-pemetrexed)
1LMSurveillance
(erlotinib)
2L
3L

2013-11-21
64
Doc75 (n=55)
Survival – TAX 317BDocetaxel 75mg/m2 vs BSC: Superior in 2nd Line
Median 7.5 mo vs. 4.6 moLog-rank p = 0.010
Doc75 (n=55)
BSC75 (n=49)1.0
0.9
0.8
0.7
rob
abili
ty
1-year 37% vs. 12%Chi-square p = 0.003
0.6
0.5
0.4
0.3
0.2
Cu
mu
lati
ve
P
0.1
0.0
0 3 6 9 12 15 18 21
Survival Time (months)
C

2013-11-21
65
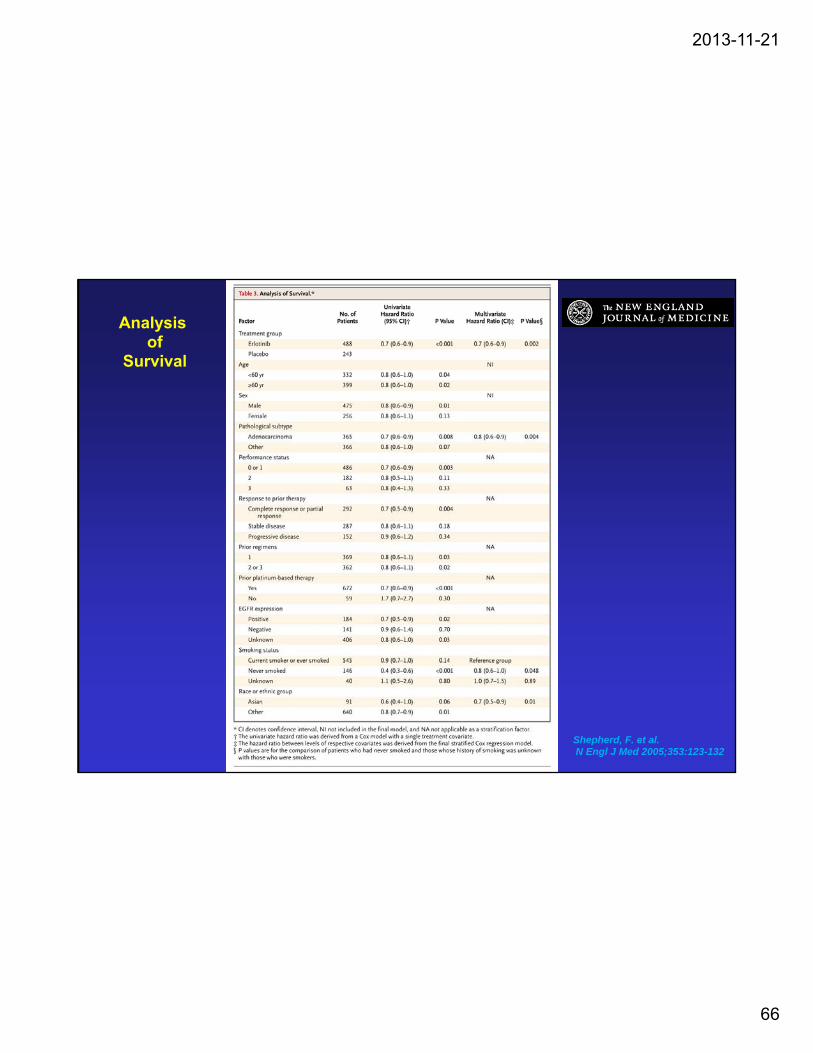
BR.21: Erlotinib vs Placebo in 2/3LOverall Survival
100
g
60
80___ Erlotinib
_____ Placebo*HR 0.71, p <0.0001
20
40 31%
22%
0 0.0 10.0 20.0
MonthsShepherd, F. et al. N Engl J Med 2005;353:123-132
2013-11-21
66
Analysisof
Survival
Shepherd, F. et al.N Engl J Med 2005;353:123-132

2013-11-21
67
BR21: A large subgroup benefit in pts with zero EGFR mutations
Clark GM et al. Clin Lung Cancer 2006

2013-11-21
68
A-NSCLC
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT/WT UNKNOWN
1L Platinum doublet x 4
1LM
AlimtaAlimta(or erlotinib)
(Or Surveillance)
2L Erlotinib(docetaxel not funded, no data)

2013-11-21
69
A-NSCLC: Algorithm Scaffold
Non-Squamous Squamous
EGFR M+ ALK+ WT/WT UNKNOWN
q
NOS Adenoca Large
EGFR M+ ALK+ WT/WT UNKNOWN
1L Platinum Doublet
(non-pemetrexed)
1LMS illSurveillance
(erlotinib)
2L ErlotinibOr Docetaxel
3L DocetaxelOr Erlotinib
2013-11-21
70
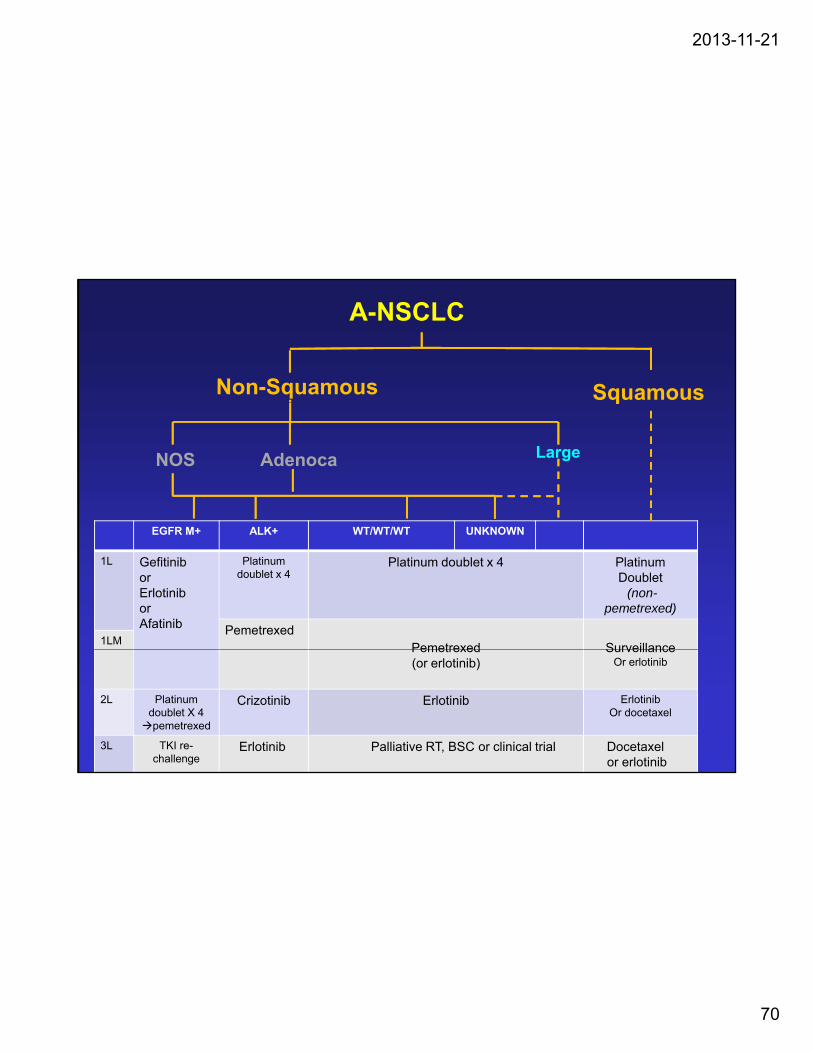
A-NSCLC
Non-Squamous Squamousq
NOS Adenoca Large
EGFR M+ ALK+ WT/WT/WT UNKNOWN
1L GefitiniborErlotiniborAfatinib
Platinum doublet x 4
Platinum doublet x 4 Platinum Doublet
(non-pemetrexed)
PemetrexedPemetrexed Surveillance
1LMPemetrexed(or erlotinib)
SurveillanceOr erlotinib
2L Platinum doublet X 4 pemetrexed
Crizotinib Erlotinib ErlotinibOr docetaxel
3L TKI re-challenge
Erlotinib Palliative RT, BSC or clinical trial Docetaxelor erlotinib

2013-11-21
71

2013-11-21
72

2013-11-21
73
2013-11-21
74
Met
HGF
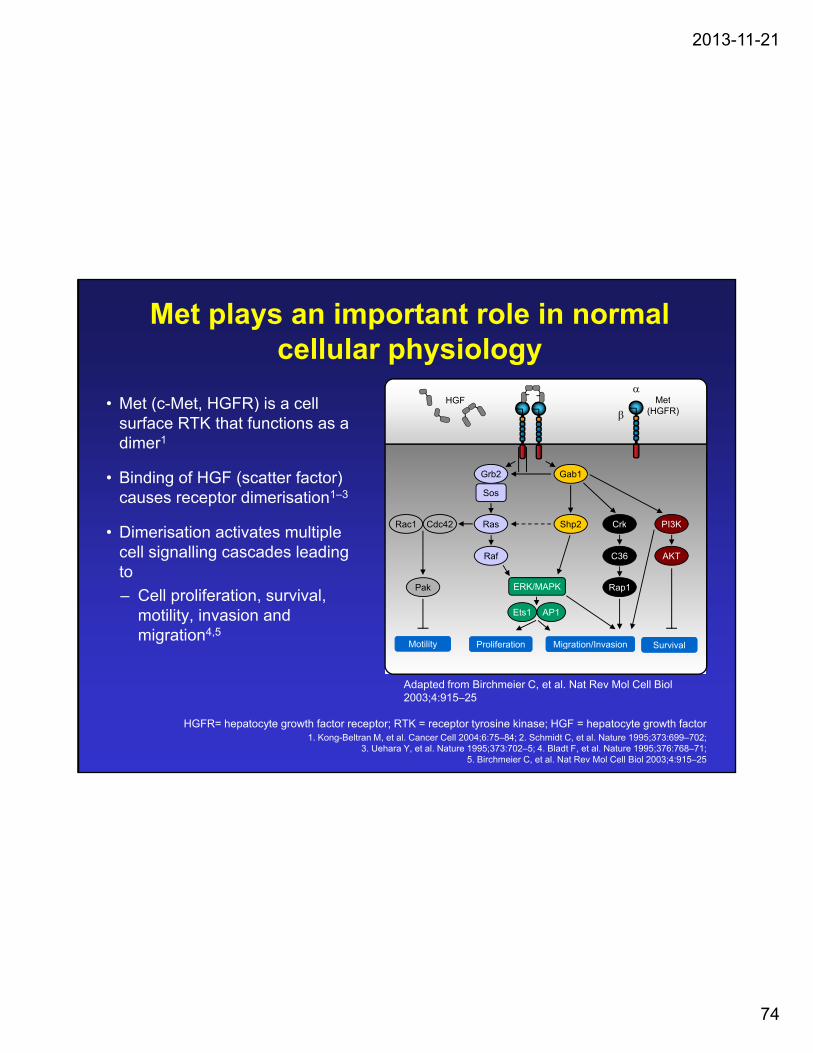
Met plays an important role in normal cellular physiology
• Met (c Met HGFR) is a cell
Rac1 Cdc42 Ras
Grb2
Sos
Shp2
Gab1
Crk PI3K
Met(HGFR)
HGF• Met (c-Met, HGFR) is a cell surface RTK that functions as a dimer1
• Binding of HGF (scatter factor) causes receptor dimerisation1–3
Di i ti ti t lti l
Pak
Rac1 Cdc42 Ras
Raf
Shp2
ERK/MAPK
Ets1 AP1
Rap1
Crk
C36
PI3K
AKT
Motility Proliferation Migration/Invasion Survival
• Dimerisation activates multiple cell signalling cascades leading to
– Cell proliferation, survival, motility, invasion and migration4,5
HGFR= hepatocyte growth factor receptor; RTK = receptor tyrosine kinase; HGF = hepatocyte growth factor 1. Kong-Beltran M, et al. Cancer Cell 2004;6:75–84; 2. Schmidt C, et al. Nature 1995;373:699–702;
3. Uehara Y, et al. Nature 1995;373:702–5; 4. Bladt F, et al. Nature 1995;376:768–71; 5. Birchmeier C, et al. Nat Rev Mol Cell Biol 2003;4:915–25
Adapted from Birchmeier C, et al. Nat Rev Mol Cell Biol 2003;4:915–25

2013-11-21
75
I ll ll l (NSCLC) t di 1 6
The Met Pathway in Lung Cancer• In non–small cell lung cancer (NSCLC) studies1–6
– Met overexpression was detected in up to 67% of patient samples
– MET gene amplification has been observed in 1–7% of NSCLC patients samples surveyed
– Mutations in MET have been identified in patient samples and NSCLC cell lines
• Met activation has been reported in up to 5–20% of patients with EGFR tyrosine kinase inhibitor (TKI)-resistant NSCLC1,7–9
– In preclinical studies, inhibition of Met signaling was capable of restoring sensitivity to treatment in EGFR TKI-resistant NSCLC cells
1. Lawrence R, Salgia R. Cell Adh Migr 2010; 4:146–152. 2. Christensen J, et al. Cancer Lett 2005; 225:1–26.
3. Cappuzzo F, et al. J Clin Oncol 2009; 27:1667–1674. 4. Toschi L, Cappuzzo F. Future Oncol 2010; 6:239–247.
5. Kris M, et al. J Clin Oncol 2011; 29(18 suppl.): Abstract CRA7506. 6. Kong-Beltran M, et al. Cancer Res 2006; 66:283–289.
7. Engelman J, et al. Science 2007; 316:1039–1043. 8. Sequist L, et al. J Clin Oncol 2008; 26:2442–2449.
9. Sequist L, et al. Sci Transl Med 2011; 3:75ra26.

2013-11-21
76
Prognostic value of MetHigh Met expression is linked with lower OS in NSCLC
• Retrospective study; 885-year survival
rate(%) †• Retrospective study; 88 NSCLC tumours assessed by IHC*– Adenocarcinoma (n=46)
– Squamous cell carcinoma (n=29)
%)
rate(%) †
Met negative 63.2
Met positive 33.8
Intratumoural Met negative
60
80
100
– Large-cell carcinoma (n=13)
• 36/88 were intratumoural Met positive (40.9%)
• Intratumoural Met expression
OS
rat
e (%
p=0.0095
Intratumoural Met positive
0
20
40
60
Intratumoural Met expression was a significant prognostic factor– RR=2.642; p=0.0029OS = overall survival; NSCLC = non-small-cell lung cancer *IHC: rabbit polyclonal anti-Met antibody (sc10), Santa Cruz
Biotechnology†5-year survival rate, based on 52 Met negative tumours and 36 Met positive tumours
Masuya D, et al. Br J Cancer 2004;90:1555–62
Months after surgery
0 20 40 60 80 100 120

2013-11-21
77
MET IHC as a companion diagnostic in NSCLC
• ‘MET Positive’ was defined as majority (≥50%) of tumor cells with moderate or strong staining intensity
10
100
1000N
A (
2-D
ct)
M dM d SS
NegativeNegative WeakWeak MET NegativeMET Negative MET PositiveMET Positive
MET IHC score 1 2 30
1
10
0
ME
T m
R
Ventana’s CONFIRM (SP44 mAb clone)
ModerateModerate StrongStrong
• MET diagnostic status was assessed after randomization and prior to unblinding
• 93% of patients had adequate tissue for evaluation of MET by IHC
• 52% patients with evaluable tissue were “MET Positive”
IHC: immunohistochemistryRoche data on file
2013-11-21
78
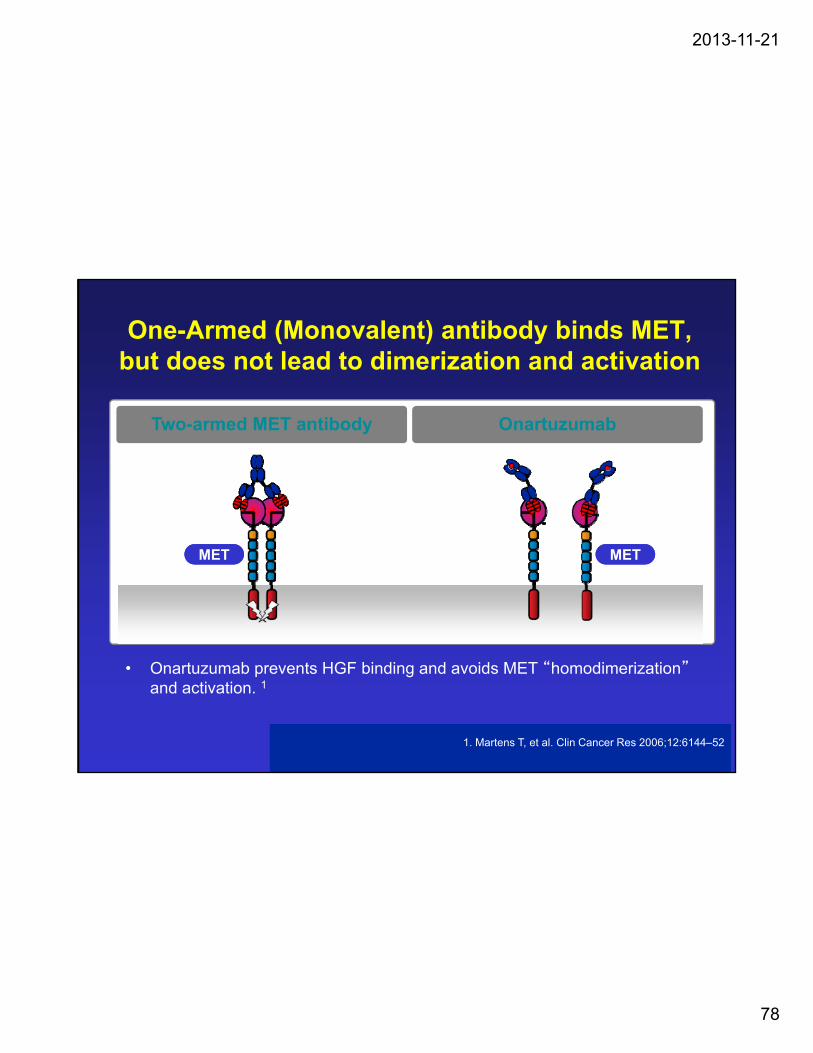
One-Armed (Monovalent) antibody binds MET, but does not lead to dimerization and activation
OnartuzumabTwo-armed MET antibody
METMET METMET
1. Martens T, et al. Clin Cancer Res 2006;12:6144–52
• Onartuzumab prevents HGF binding and avoids MET “homodimerization”and activation. 1
2013-11-21
79
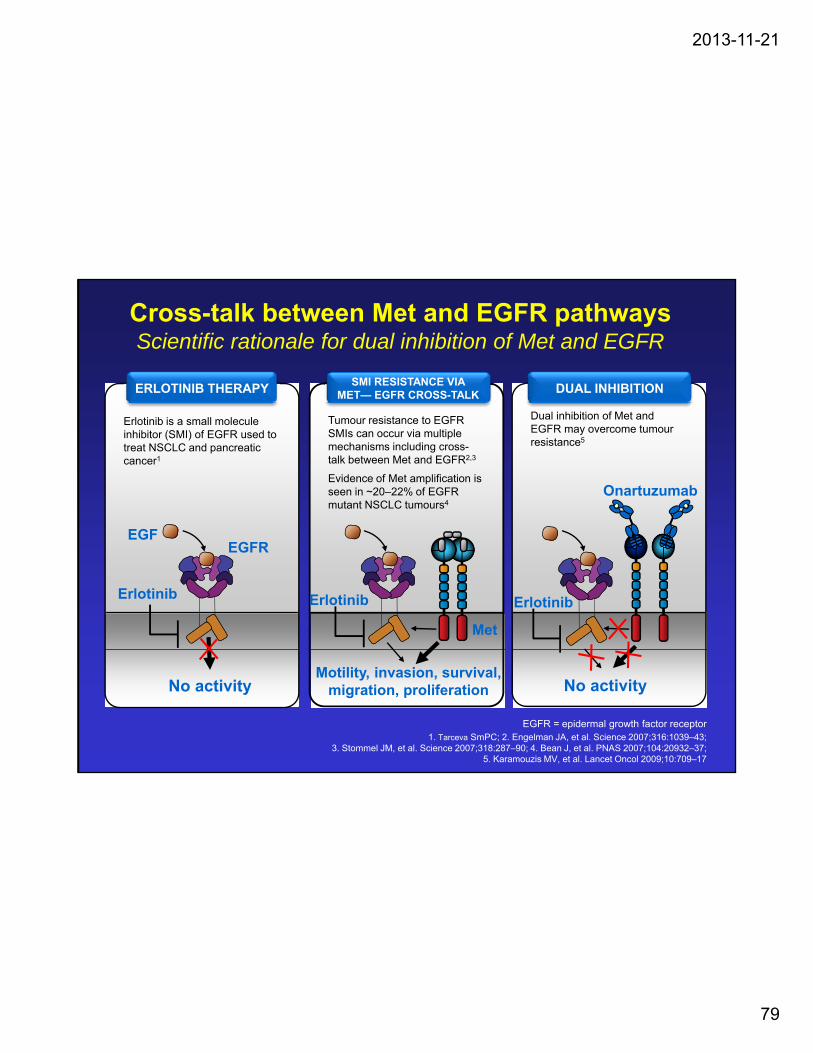
Cross-talk between Met and EGFR pathwaysScientific rationale for dual inhibition of Met and EGFR
ERLOTINIB THERAPYSMI RESISTANCE VIA
MET— EGFR CROSS-TALK DUAL INHIBITION
Erlotinib is a small molecule inhibitor (SMI) of EGFR used to treat NSCLC and pancreatic cancer1
Dual inhibition of Met and EGFR may overcome tumour resistance5
Tumour resistance to EGFR SMIs can occur via multiple mechanisms including cross-talk between Met and EGFR2,3
Evidence of Met amplification is seen in ~20–22% of EGFR mutant NSCLC tumours4
Onartuzumab
EGFEGFR
Erlotinib Erlotinib Erlotinib
Met
EGFR = epidermal growth factor receptor1. Tarceva SmPC; 2. Engelman JA, et al. Science 2007;316:1039–43;
3. Stommel JM, et al. Science 2007;318:287–90; 4. Bean J, et al. PNAS 2007;104:20932–37; 5. Karamouzis MV, et al. Lancet Oncol 2009;10:709–17
No activity No activityMotility, invasion, survival,
migration, proliferation
2013-11-21
80
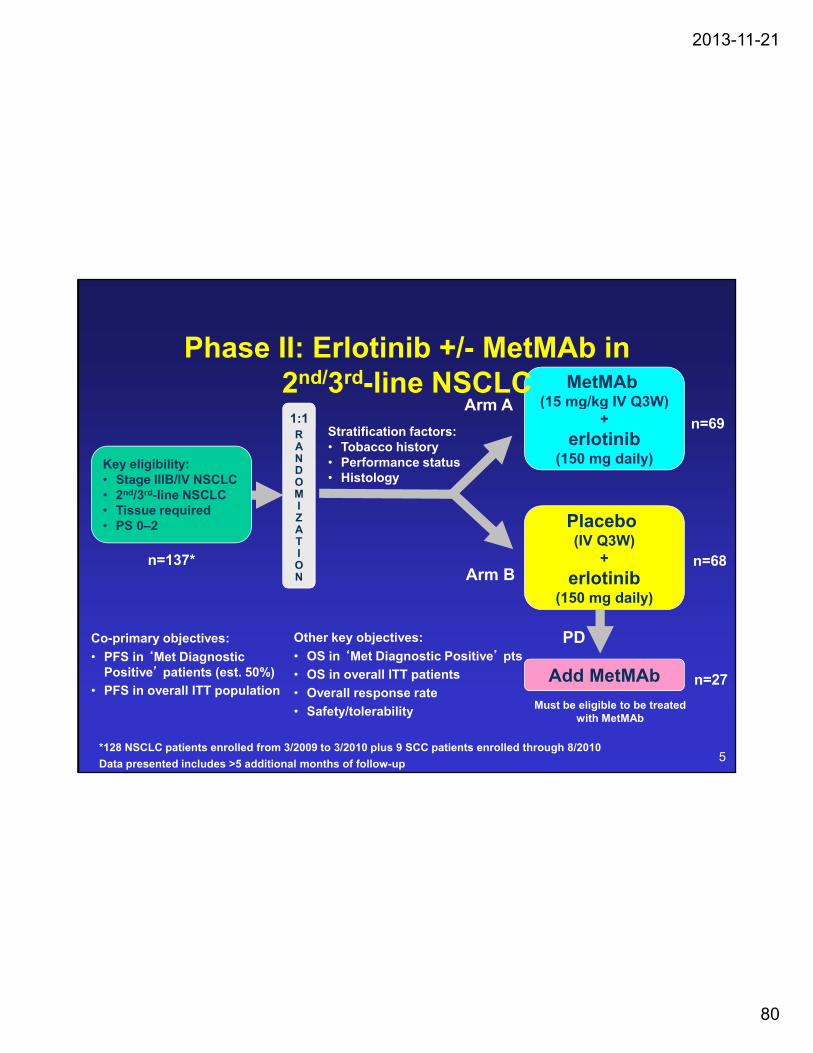
MetMAb(15 mg/kg IV Q3W)
Phase II: Erlotinib +/- MetMAb in2nd/3rd-line NSCLC
Arm A (15 mg/kg IV Q3W)+
erlotinib(150 mg daily)
RANDOMIZA
1:1 n=69Arm A
Key eligibility:• Stage IIIB/IV NSCLC• 2nd/3rd-line NSCLC• Tissue required• PS 0–2
Stratification factors:• Tobacco history • Performance status • Histology
PlaceboATION
n=137* n=68Arm B
PD
• PS 0–2 Placebo (IV Q3W)
+
erlotinib(150 mg daily)
Co-primary objectives: Other key objectives:
*128 NSCLC patients enrolled from 3/2009 to 3/2010 plus 9 SCC patients enrolled through 8/2010
Data presented includes >5 additional months of follow-up
n=27
Must be eligible to be treated with MetMAb
Add MetMAb• PFS in ‘Met Diagnostic
Positive’ patients (est. 50%)
• PFS in overall ITT population
• OS in ‘Met Diagnostic Positive’ pts
• OS in overall ITT patients
• Overall response rate
• Safety/tolerability
5

2013-11-21
81
MetMAb plus erlotinib in Met Dx+ patients
PFS: HR=0.53 OS: HR=0.37
sio
n f
ree
0.8
1.0
Placebo +erlotinib
3.8
26
MetMAb +erlotinib
12.6
16
Median (mo)HR
(95% CI)Log-rank p-value
No. of events
viva
l 0.8
1.0
Placebo +erlotinib
1.5
27
Median (mo)HR
(95% CI)Log-rank p-value
No. of events
MetMAb +erlotinib
2.9
20
0.53(0.28–0.99)
0.04
0.37(0.19–0.72)
0.002
rob
abili
ty o
f p
rog
ress
0.2
0.4
0.6
Pro
bab
ility
of
surv
0.2
0.4
0.6
Time to progression (months)
0 3 6 9 12 15 18
Pr
0.0
Overall survival (months)
0 3 6 9 12 15 18 21
0.0
9

2013-11-21
82
MetLung(OAM4971g): A RANDOMIZED, PHASE III, MULTICENTER, DOUBLE-BLIND, PLACEBO-CONTROLLED STUDY EVALUATING
ONARTUZUMAB IN COMBINATION WITH ERLOTINIB IN PATIENTS WITH MET DIAGNOSTIC−POSITIVE mNSCLC WHO AFTER
STANDARD CHEMOTHERAPY
Treat until PD
Erlotinib + onartuzumab
Randomise 1:1
2L/3L NSCLC
Met-positive
(1 prior platinum-based line of therapy)
Central testing for:
• Met status
• EGFR mutation
Survivalfollow-up
Erlotinib + placebo
status
(N=490)
Primary endpoint:• OSSecondary endpoints:• PFS
Erlotinib: 150mg p.o. qdOnartuzumab/placebo: 15mg/kg i.v. q3w
No crossover tx
Stratification criteria
• EGFR mutation status
Key eligibility criteria
• Stage IIIb or IV Met+ NSCLC
ECOG = Eastern Cooperative Oncology Group; PFS = progression-free survival; ITT = intent-to-treat; OS = overall survival; ORR = overall response rate; PD = progressive disease
PFS• ORR• Quality of life• Safety
• EGFR mutation status
• Met 2+ or 3+ score
• Number of prior lines of therapy
• Histology
• Stage IIIb or IV Met+ NSCLC
• 1–2 prior lines of treatment
• No prior EGFR inhibitor
• ECOG PS 0 or 1

2013-11-21
83
SMALL CELL LUNG CANCER :
Limited Disease Extensive Disease
1L Cisplatin/Etoposide Carboplatin/Etoposide
S C U G C CALGORITHM
1L Cisplatin/Etoposide x 4-6 cycles
Concurrent thoracic RTProphylactic Cranial RT
Carboplatin/Etoposidex 4-6 cycles
± Palliative RTProphylactic Cranial RT
1LM Surveillance Surveillance
2L Re-challenge with Carboplatin/Etoposideor
Topotecan single-agent

2013-11-21
84
Group No. of trials
Comparison Survival HR
G 1 1 ± Ci l ti ( t id ) 0 70Group 1 1 ± Cisplatin (no etoposide) 0.70
Group 2 17 ± Etoposide (no cisplatin) 0.72
Group 3 9 Cis/Etop vs Other 0.57
Group 4 9 Cis/Etop vs Etop/other 0.74

2013-11-21
85
“It was decided to remove the reference thatEtoposide-carboplatin was biologically equivalent to etoposide-cisplatin..and to discuss the limitedamount of data on this issue.”

2013-11-21
86

2013-11-21
87

2013-11-21
88
Compared to patients in arm III patients treated in arms I and II survived longer with median survivals of 336 days (95% CI 275-397), 340 days (95% CI 290-390), and 293 days (95% a 266-320), respectively. The overall survival difference between the three arms was statistically significant (P = 0.04, Figure 1). P i i i b thPairwise comparison by the logrank test showed that the difference in survival betweenarm II and III was statistically significant (P - 0.02, logranktest), while the P-value of the difference betweendifference betweenarm I and arm III was 0.07.

2013-11-21
89

2013-11-21
90
J Clin Oncol 1999
Similar survival, superior symptom , p y prelief, slightly better response rates;but more anemia,thrombocytopenia on topotecan.

2013-11-21
91
15 pts re-challenged;10 responses (67%)MST 5 months
However, we have identified seven studies (192patients altogether) employing so-called non-cross-resistantchemotherapy in clearly distinguishable relapsed patients
Their response rates (CR + PR) range from 6%.... Their response rates (CR + PR) ...range from 6%to 31%, and the median survival of responding patientswas usually only 3-4 months. Thus, results with re-challenge chemotherapy, although poor, appear to be no worse than with alternative second-line chemotherapy.
THERE IS NO STANDARD 2ND LINE:CAV OR TOPOTECAN PROBABLY NOTSUPERIOR TO RE-CHALLENGE WITHPLATINUM AND ETOPOSIDECONSIDER G-CSF TO PREVENT FN & MAINTAIN DOSE INTENSITY

2013-11-21
92
PCI in ED-SCLC:Cumulative Incidence of Symptomatic Brain Metastases
Slotman B et al. N Engl J Med 2007;357:664-672

2013-11-21
93
Overall Survival
PCI in ED-SCLC:
Slotman B et al. N Engl J Med 2007;357:664-672

2013-11-21
94
Bone Metastases:
Zoledronate vs Placebo

2013-11-21
95
2013-11-21
96

2013-11-21
97

2013-11-21
98

2013-11-21
99

2013-11-21
100

2013-11-21
101

2013-11-21
102
2013-11-21
103

2013-11-21
104

2013-11-21
105

2013-11-21
106
EXPERIMENTAL TARGETS IN SMAL CEL LUNG CANCER
Teicher B. Biochemical Pharmacology 2013

2013-11-21
107

2013-11-21
108
Home page

2013-11-21
109
Signing up

2013-11-21
110
Logging in

2013-11-21
111
Premise behind the website

2013-11-21
112
Resources – available to view without signing in or logging in

2013-11-21
113
Resources include a link to the actual trial, granted the computer you are working from has access ie. hospital

2013-11-21
114
User Guide tab

2013-11-21
115
New patient (can be saved) vs sample patient (teaching or review opportunity)

2013-11-21
116
Overview field

2013-11-21
117
Overview

2013-11-21
118
Entering patient characteristics allows for a personalized treatment guide

2013-11-21
119
Patient Characteristics

2013-11-21
120
Medical details

2013-11-21
121
Prior therapy considerations
2013-11-21
122
Specific notes that pertain to patient characteristics

2013-11-21
123
Drug details

2013-11-21
124
Warning symbols

2013-11-21
125
Choosing a drug eliminates subsequent choices in later lines

2013-11-21
126
Comment Boxes

2013-11-21
127
CASE REPORT (1)
An overview: Current systemic th i f d d ll lltherapies for advanced non-small cell lung cancer
Ong M and Vincent M. Lung Cancer, In Press

2013-11-21
128
CASE REPORT (cont) … (2)
• 54 yr Caucasian male• 54 yr Caucasian male
• Never-smoker
• Dyspnea, large pleural effusion
• FNA: “adenocarcinoma lung”
• Chest tube drainage pleurodhesis• Chest tube drainage, pleurodhesis
• EGFR “inconclusive” (scant 6x material)
• 6 cycles carbo/paclitaxel – minor response
• Relapsed within 3/12
Refractor to 3 c cles pemetre ed• Refractory to 3 cycles pemetrexed
• Multiple brain mets, 02 dependent
• Whole brain RT

2013-11-21
129
CASE REPORT (cont) … (3)
• Rx erlotinib 150 mg po od

2013-11-21
130
Disease burden before (Panels A, B, C) and 8 months after (Panels D, E, F) initiation of third-line erlotinib for metastatic A-NSCLC.

2013-11-21
131
CASE REPORT (cont) … (4)
• Eventual PD on erlotinib (± 1 year• Eventual PD on erlotinib (± 1 year remission)
• Unresponsive to trial of afatinib• Unresponsive to trial of afatinib
• Dies rapidly of respiratory failure
• EGFR ? But almost certainly M+

2013-11-21
132
THE END

2013-11-21
133
2013-11-21
134

2013-11-21
135

2013-11-21
136
2013-11-21
137









![HOMEOPATHY IN ADVANCED LUNG CANCER.ppt - Ningapi.ning.com/.../HomeopathyinAdvancedLungCancer.pdfMicrosoft PowerPoint - HOMEOPATHY IN ADVANCED LUNG CANCER.ppt [Compatibility Mode] Author:](https://img.pdfslide.net/doc/110x75/5af339257f8b9a8b4c9132b6/homeopathy-in-advanced-lung-ningapiningcomhomeopathyinadvancedlungcancerpdfmicrosoft.jpg)