Embed Size (px)
Citation preview
1
The Family Perspective: Late Preterm Birth and
Short Stay NICU Families
Judith S. GoodingNational Director,
NICU Initiatives and
y
NICU Initiatives and Chapter Program Strategy
March of Dimes: Champion for All Babies
March of Dimes helps moms have full-term pregnancies and healthy babies. And if something goes wrong, we offer information and comfort to families. We research the problems that threaten our babies and
work on preventing them.

2
March of Dimes NICU Family Support®
O it NICU F il S t S i li tOn-site NICU Family Support SpecialistFamily-Staff Action Committee
Parent Care KitsProfessional Development2-3 Customized ProgramsDirect Service ActivitiesDirect Service ActivitiesParent-to-Parent Support
Evaluation
Shorter Stay Families• Pilot – history and
b k dbackground– 4 sites (Arkansas,
Montana, Illinois, Pennsylvania)
Importance of providing support to all families
3
DefinitionsDefinitions• Term Birth: birth at or after the 37 week of gestation• Premature Birth: birth before the end of the 36th week of
gestation• Late Preterm Birth (LPB): 340/7 to 366/7 weeks’ gestation (~240-
259 days after LMP)
• Birthweight– Average Birthweight: 2,500 to 4,000 grams at term– Low Birthweight (LBW): live born infants weighing less than g ( ) g g
2500 grams (5 pounds, 8 ounces)– Very Low Birthweight (VLBW): live born infants weighing 500
to 1,499 grams (1 pound, 1.5 ounces to 3 pounds, 5 ounces)
Transitional Later Neonatal Period
Medical Issues
Respiratory Distress (RDS)Temperature InstabilityHypoglycemiaFeeding difficulties
First WeekNeonatal jaundice
Poor feeding and dehydrationReadmission to hospital
Neonatal jaundiceApneaInfection rate
1 Late Preterm Birth: Every Week Matters, Medical Perspectives on Prematurity. Prepared by the Office of the Medical Director, March of Dimes. March 2006.2 Late Preterm Infant Assessment Guide, Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN)3 NICHD Workshop: Optimizing Care and Long-term Outcome of Near-termPregnancy and Near-term Newborn Infant. July 18-19. Bethesda, MD, 2005.
4
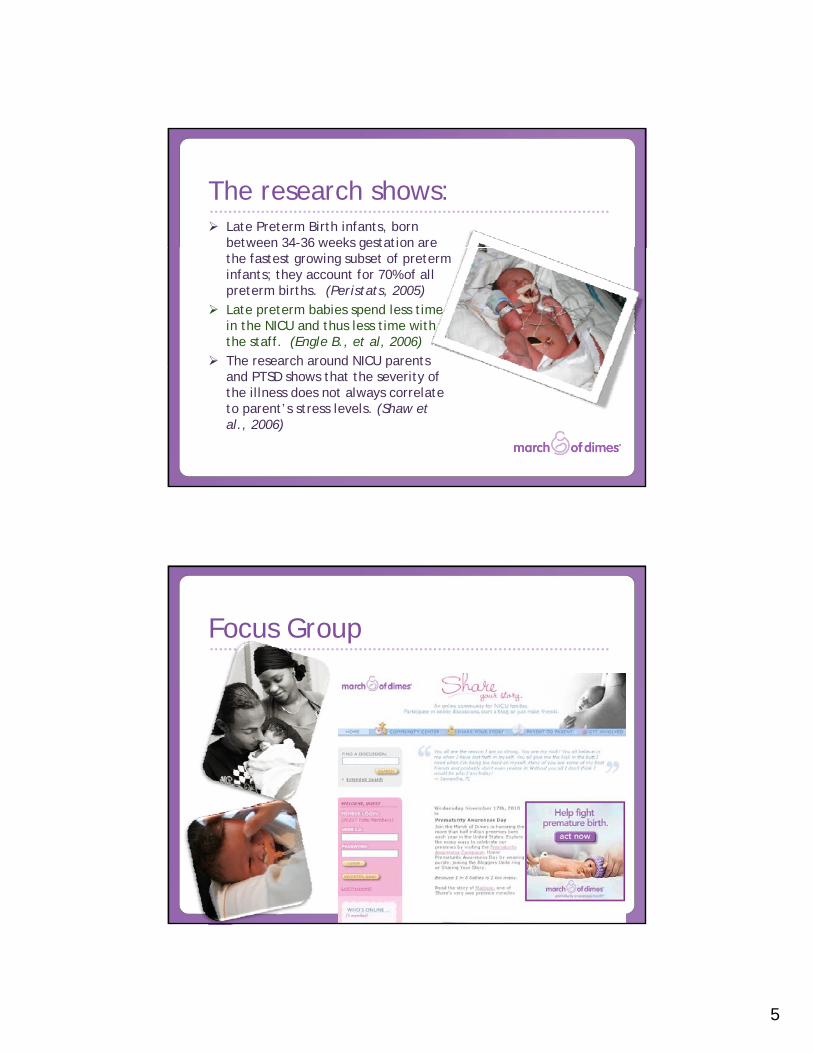
Distribution of Singleton Preterm Births, by Gestational Age
34-36 Weeks:• 74% of all
singleton PTB• 7.5% of all
births
March of Dimes Perinatal Data Center, 2005
births
“Near term infants had significantly di l bl d i d more medical problems and increased
hospital costs compared with contemporaneous full term infants. Near term infants may represent an
unrecognized at-risk neonatal population.”population.
Wang, et al. Clinical Outcomes of Near-Term Infants, Pediatrics (114) 372-6, 2004.
5
The research shows: Late Preterm Birth infants, born between 34-36 weeks gestation are gthe fastest growing subset of preterm infants; they account for 70% of all preterm births. (Peristats, 2005)Late preterm babies spend less time in the NICU and thus less time with the staff. (Engle B., et al, 2006)The research around NICU parents pand PTSD shows that the severity of the illness does not always correlate to parent’s stress levels. (Shaw et al., 2006)
Focus Group
6
Quotes from our Focus Group• “They just handed me the baby and walked away.
I had no idea how to hold a baby on oxygen In all I had no idea how to hold a baby on oxygen. In all the pictures I look so uncomfortable.”
• “They told me 33 weeks was good. But he didn’t look good to me. Good would be full term. I was horrified.”
• “Leaving my baby behind as I was discharged was one of the hardest things I have ever had to do. I felt like no one understood that.”
Parent Panel
7
Common Themes• What do we learn from families?
A th f ili id d “l i it ”?• Are these families considered “low priority”?• How do we reach them?
General Comments
• Constant comments from staff that “33 weeks is good. The baby is just a feeder/grower.”
• Not enough information for parents on outcomes or how to care for a late preterm birth baby.
• Discharge information was not specific to LPB.• Services are not the same (RSV shots, OT/PT).• Relationships with staff were challenging (time is
limited beca se sta is shorter) limited because stay is shorter). • Kangaroo care was not offered.
8
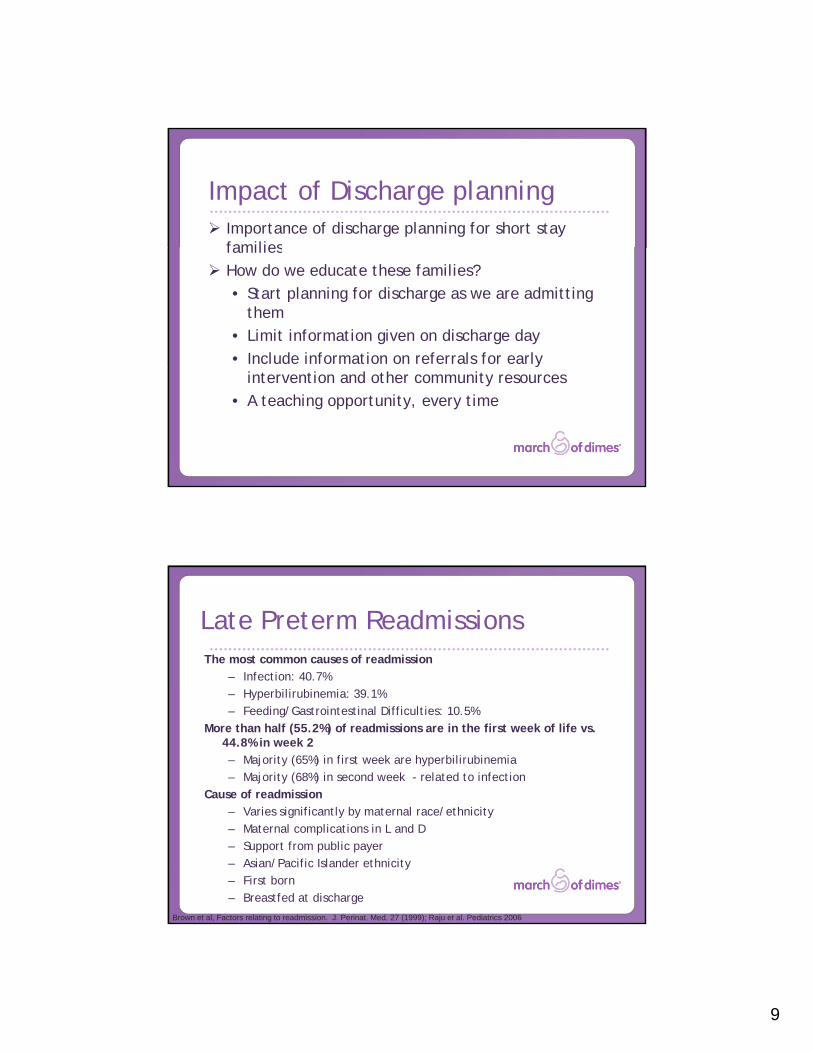
Intent vs. Impact
Leaving a baby in the NICU
“Any mother who leaves the hospital with her baby still in the hospital, understands a NICU experience.”
-Michelle Reeves, NICU Mom
9
Impact of Discharge planningImportance of discharge planning for short stay familiesfamiliesHow do we educate these families?• Start planning for discharge as we are admitting
them• Limit information given on discharge day • Include information on referrals for early
intervention and other community resources• A teaching opportunity, every time
Late Preterm ReadmissionsThe most common causes of readmission
– Infection: 40.7%– Hyperbilirubinemia: 39.1%– Feeding/Gastrointestinal Difficulties: 10.5%
More than half (55.2%) of readmissions are in the first week of life vs. 44.8% in week 2– Majority (65%) in first week are hyperbilirubinemia– Majority (68%) in second week - related to infection
Cause of readmission – Varies significantly by maternal race/ethnicity– Maternal complications in L and D– Support from public payer– Asian/Pacific Islander ethnicity– First born– Breastfed at discharge
Brown et al, Factors relating to readmission. J. Perinat. Med. 27 (1999); Raju et al. Pediatrics 2006
10
Late Preterm Infant Recommendations
• Identification of Late Preterm Infant
• Determining where baby goes• Feeding protocol• Car seat testing• Discharge criteria• AAP recommendation to NOT
discharge at < 48 hours• Provision for longer stay• Bilirubin screening• Parent support
Questions?
“Whether your baby is the
NICU for one day or 100 days –it’s traumatic!”
11
References• Engle B. A recommendation for the definition of “late preterm” (near-term)
and the birth weight-gestational age classification system. Semin-Perinatol2006;30:2-7 2006;30:2 7.
• Late Preterm Birth: Every Week Matters, Medical Perspectives on Prematurity. Prepared by the Office of the Medical Director, March of Dimes. March 2006.
• Late Preterm Infant Assessment Guide, Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN)
• National Center for Health Statistics. 2002 period linked birth/infant death data. Data prepared by the March of Dimes Perinatal Data Center, 2005.
• NICHD Workshop: Optimizing Care and Long-term Outcome of Near-term Pregnancy and Near-term Newborn Infant. July 18-19. Bethesda, MD, 2005.
• Shaw, R. J., et al. (2006). Acute Stress Disorder Among Parents of Infants in the Neonatal Intensive Care Nursery. Psychosomatics, 47#, May-June 2006, 206-211
• Wang, et al. Clinical Outcomes of Near-Term Infants, Pediatrics (114) 372-6, 2004.





























