Embed Size (px)
Citation preview

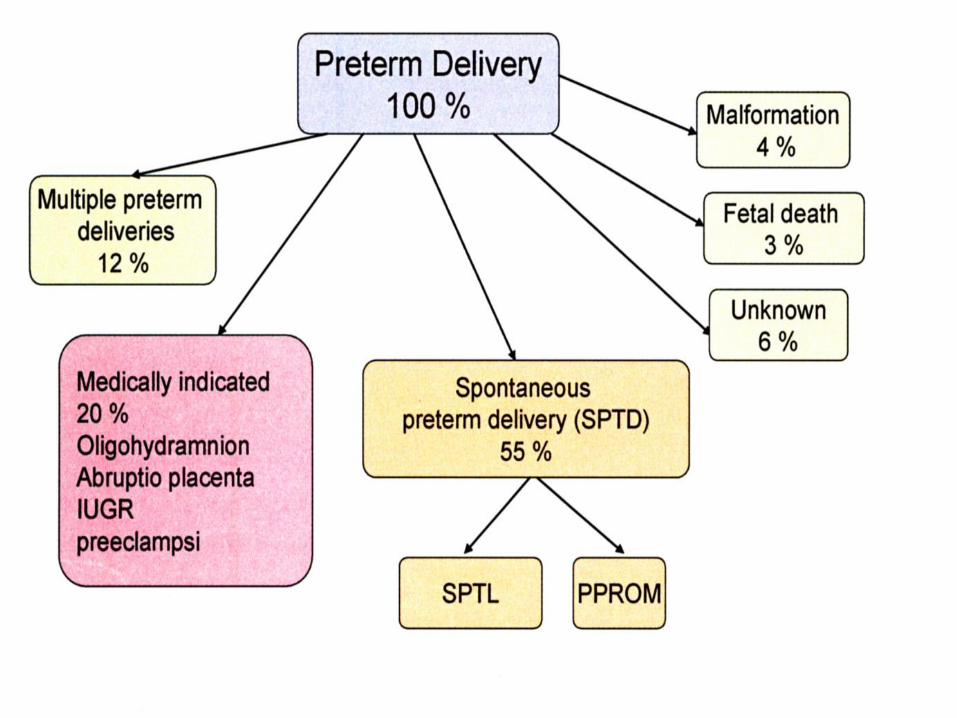
Preterm födsel
Underburenhet
=
För tidig födsel
=
Prematur förlossning
=
Preterm birth
English abbreviations
• PTB - preterm birth (för tidig födsel)
• PTD - preterm delivery (för tidig födsel)
• PTL - preterm labour (hotande för tidig födsel)
– In labour - contractions - (not delivered)
• PPROM - preterm prelabour rupture of
membranes (för tidig vattenavgang)
• SROM - spontaneous rupture of
membranes
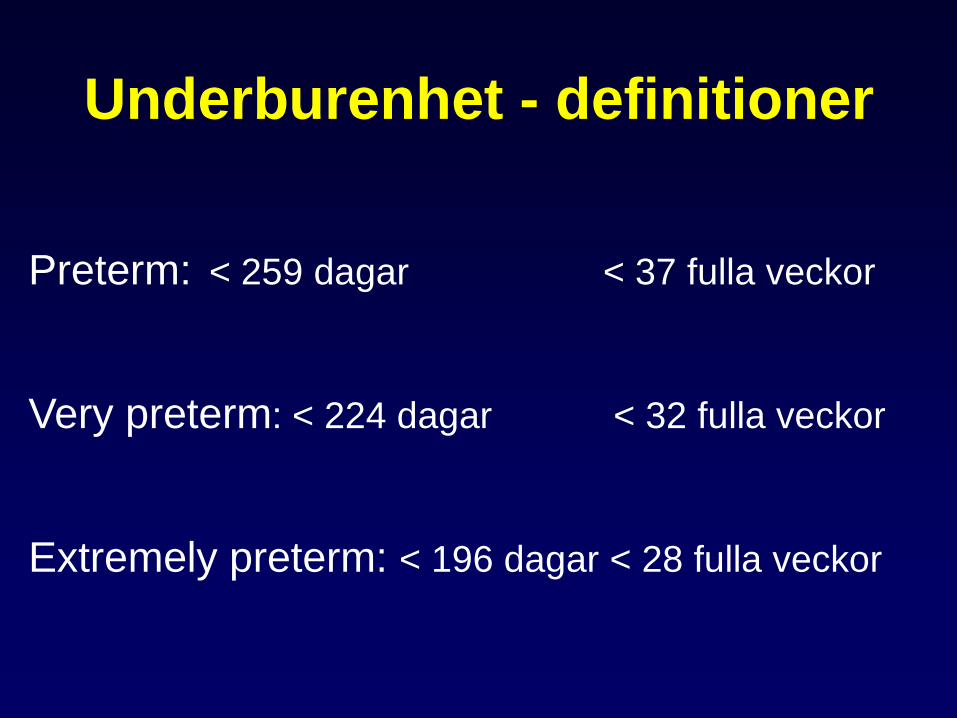
Underburenhet - definitioner
Preterm: < 259 dagar < 37 fulla veckor
Very preterm: < 224 dagar < 32 fulla veckor
Extremely preterm: < 196 dagar < 28 fulla veckor
Underburenhet - prevalens
- mellan 5 och 11 % av alla födslar
i industrialiserade länder
I Sverige:
< 37 veckor – 5.5 %
< 32 veckor - 1.0 %
< 28 veckor - 0.3-0.6 %
0
2
4
6
8
10
12
Latin
America
Africa Asia North
America
Europe Oceania
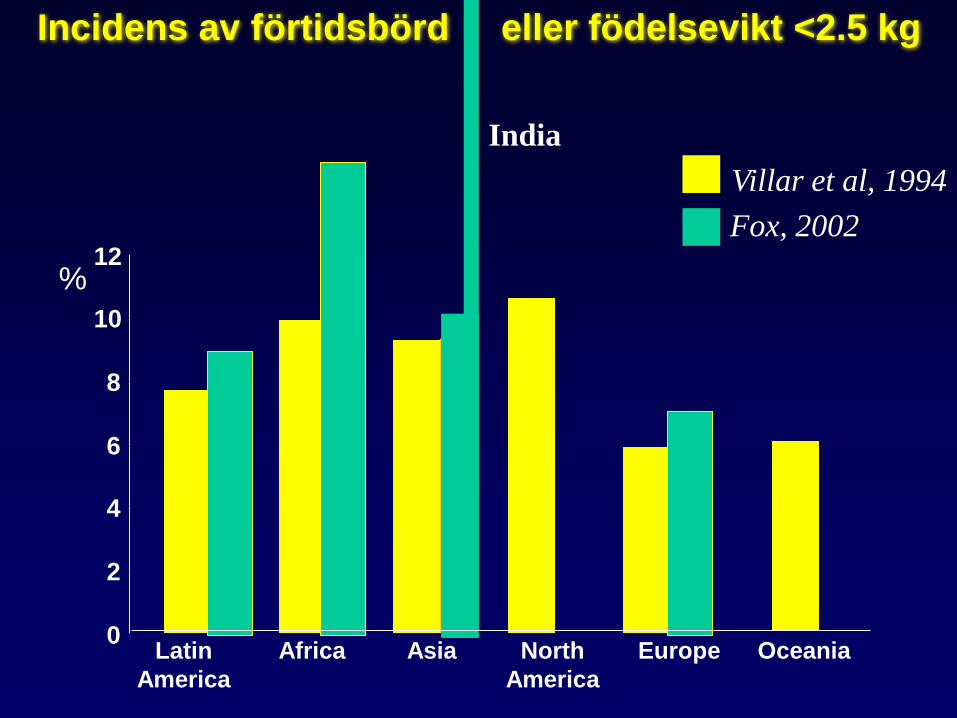
Villar et al, 1994
Incidens av förtidsbörd eller födelsevikt <2.5 kg
%
Fox, 2002
India
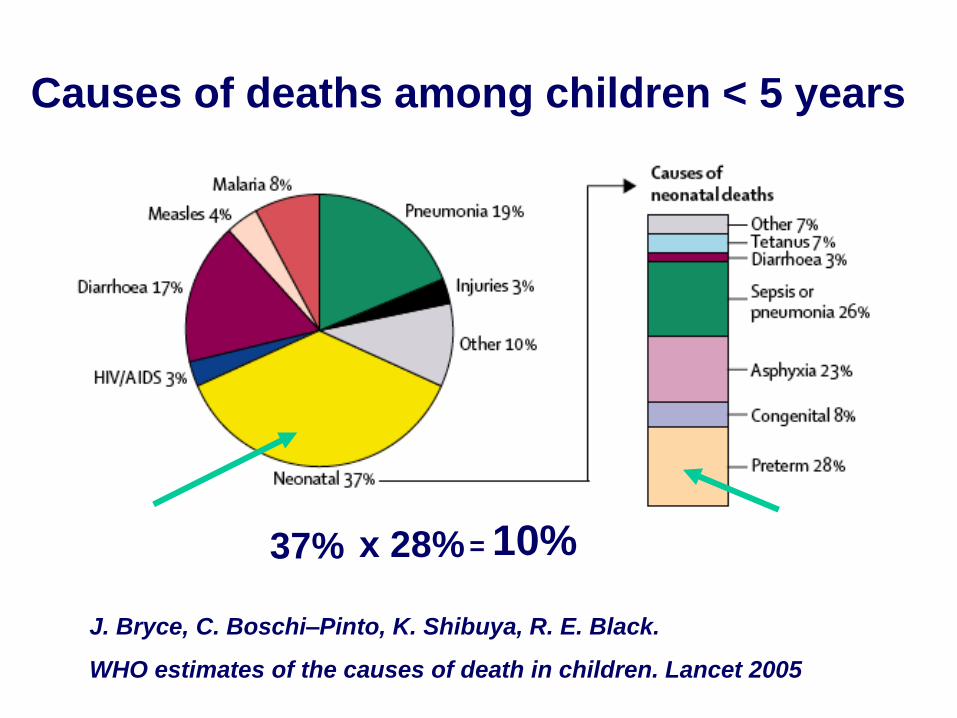
Causes of deaths among children < 5 years
37% x 28% = 10%
J. Bryce, C. Boschi–Pinto, K. Shibuya, R. E. Black.
WHO estimates of the causes of death in children. Lancet 2005
0
10
20
30
40
50
60
70
80
90
100
85-
86
87-
88
89-
90
91-
92
93-
94
95-
96
97-
98
99-
00
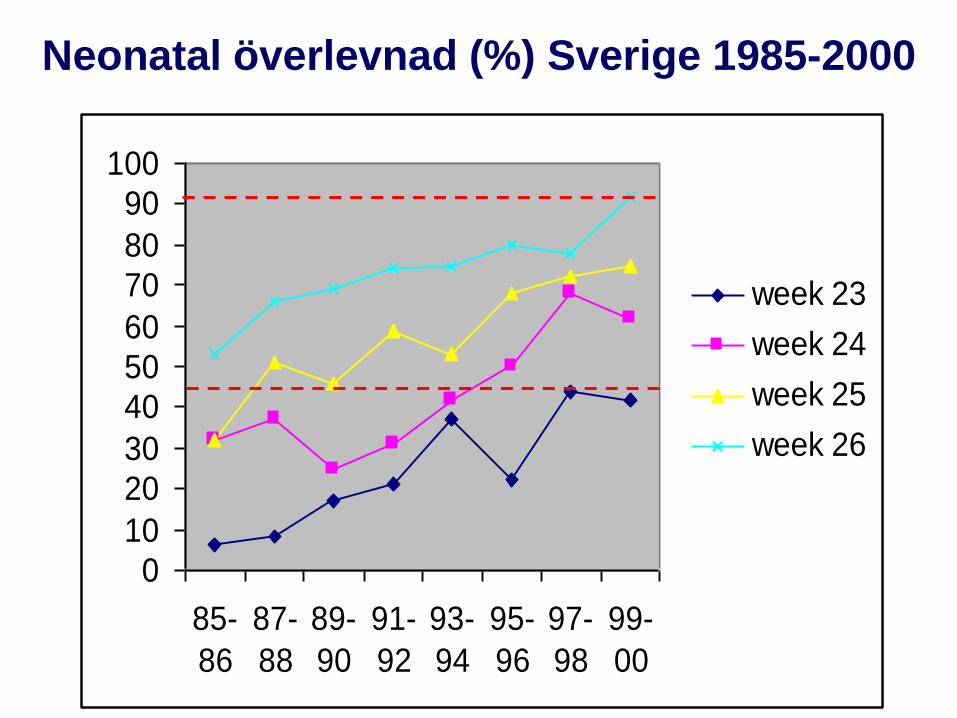
week 23
week 24
week 25
week 26
Neonatal överlevnad (%) Sverige 1985-2000
Perinatalt omhändertagande vid extrem underburenhet
”27-veckors studie” i Sverige 2004-2007
EXPRESS
Extreme Preterm Infants in Sweden Study
JAMA, June 3, 2009, Vol. 301, No. 21, pp. 2225-2233
Antal registrerade barn 1011 !!
Incidens 3,3 per 1000 barn
- levande födda 707 (70 %)
- dödfödda 304 (30 %)
Perinatalt omhändertagande vid extrem underburenhet
”27-veckors studie” i Sverige 2004-2007
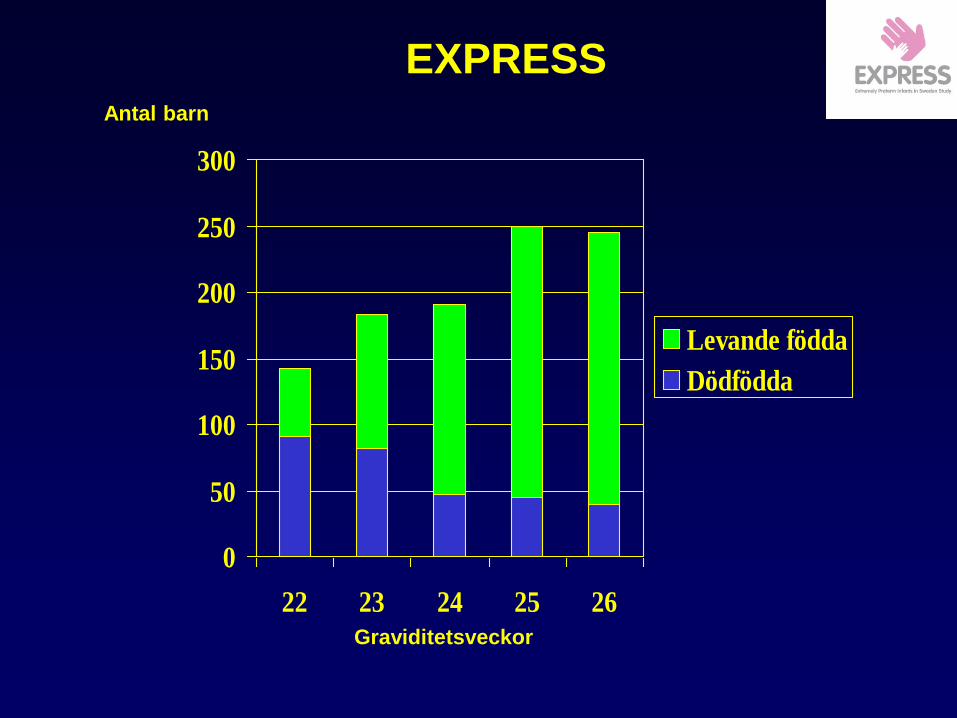
0
50
100
150
200
250
300
22 23 24 25 26
Levande födda
Dödfödda
Graviditetsveckor
Antal barn
EXPRESS
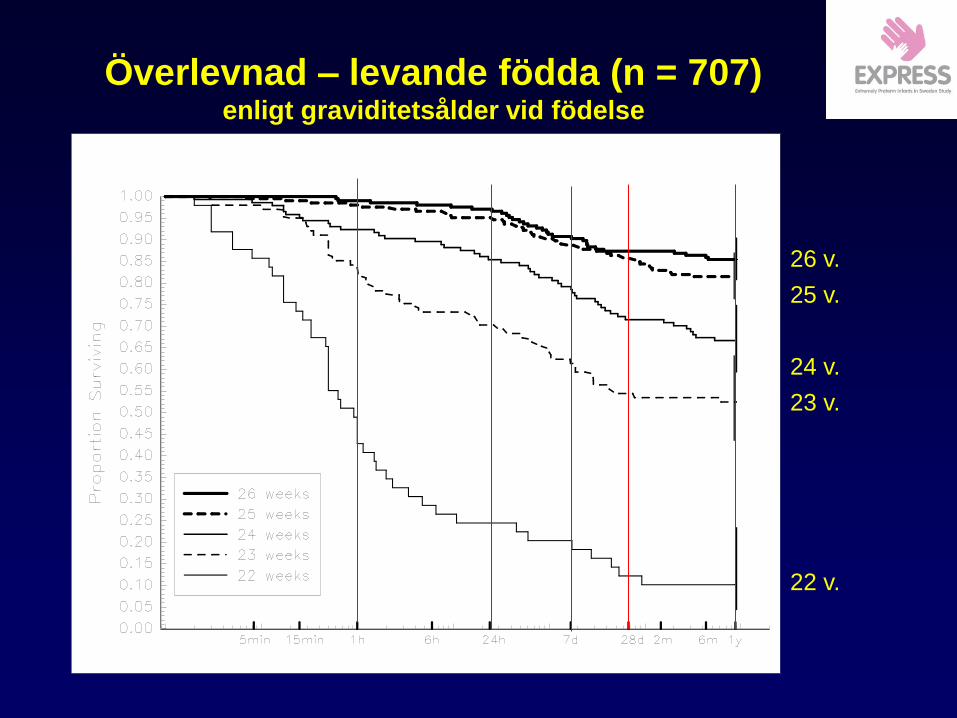
26 v.
25 v.
24 v.
23 v.
22 v.
Överlevnad – levande födda (n = 707) enligt graviditetsålder vid födelse
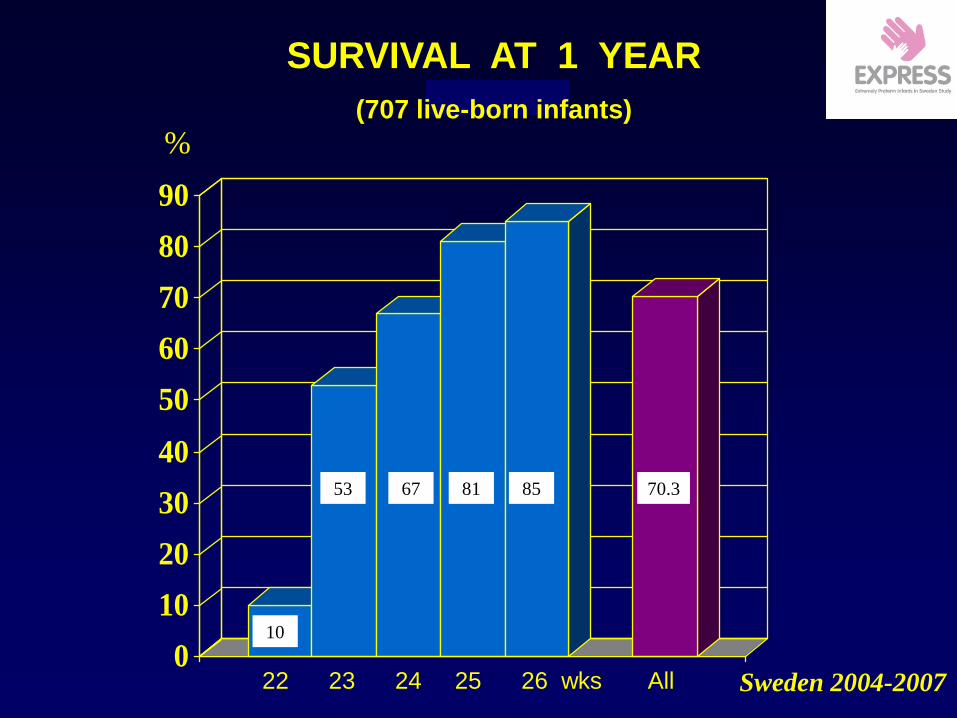
%
0
10
20
30
40
50
60
70
80
90
10
53 67 81 85 70.3
SURVIVAL AT 1 YEAR
(707 live-born infants)
22 23 24 25 26 wks All Sweden 2004-2007
0
10
20
30
40
50
60
70
80
90
Percent
22 23 24 25 26
GA
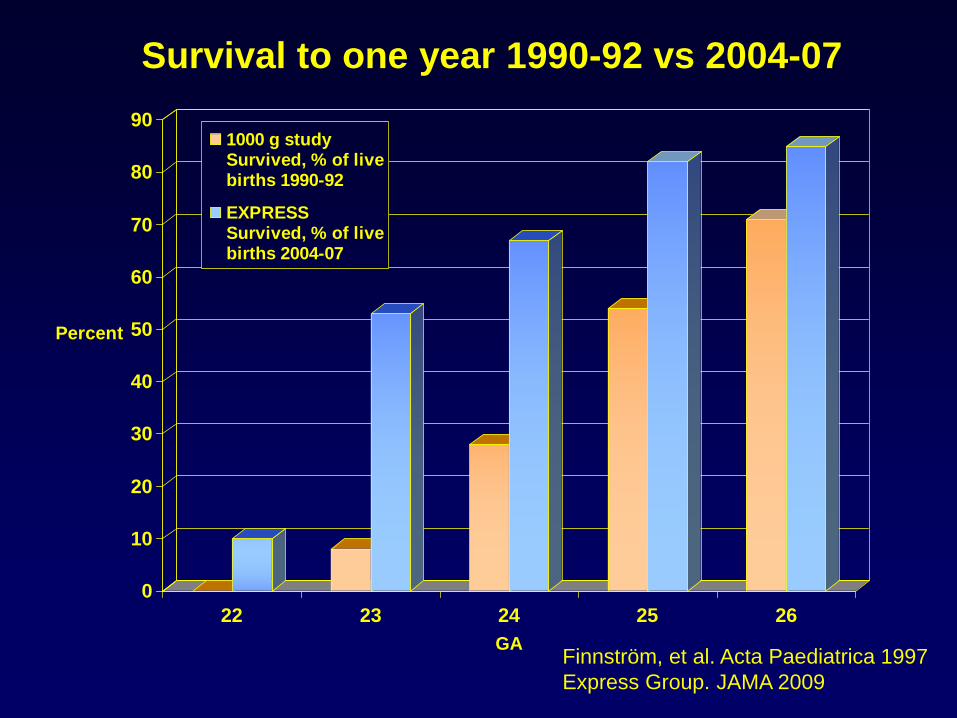
1000 g studySurvived, % of livebirths 1990-92
EXPRESSSurvived, % of livebirths 2004-07
Survival to one year 1990-92 vs 2004-07
Finnström, et al. Acta Paediatrica 1997
Express Group. JAMA 2009
0
10
20
30
40
50
60
70
80
90
Percent
22 23 24 25 26
GA
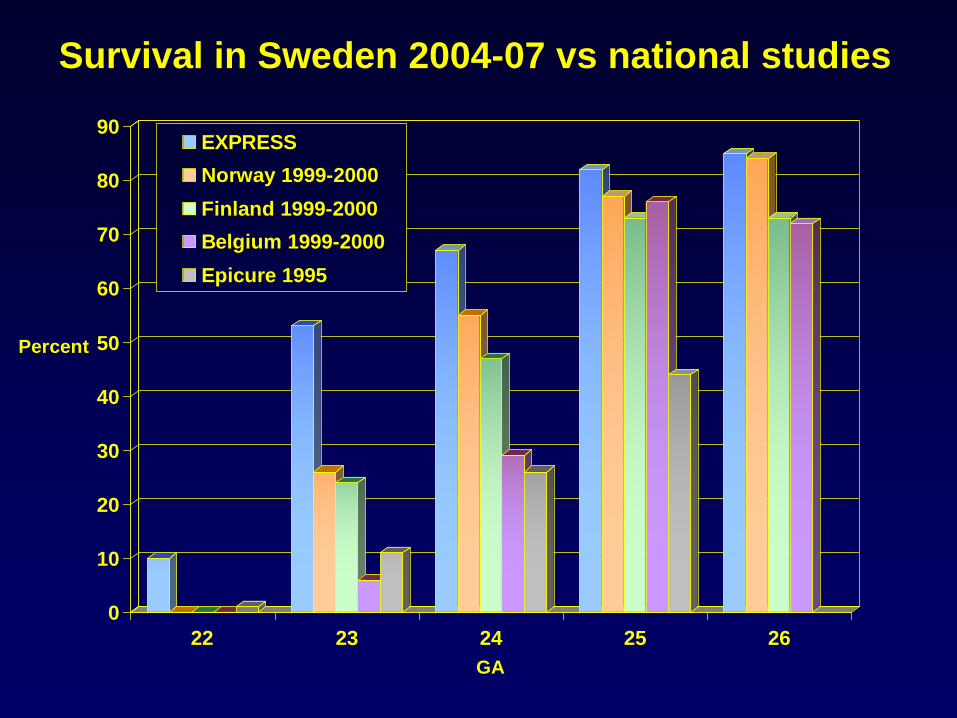
EXPRESS
Norway 1999-2000
Finland 1999-2000
Belgium 1999-2000
Epicure 1995
Survival in Sweden 2004-07 vs national studies
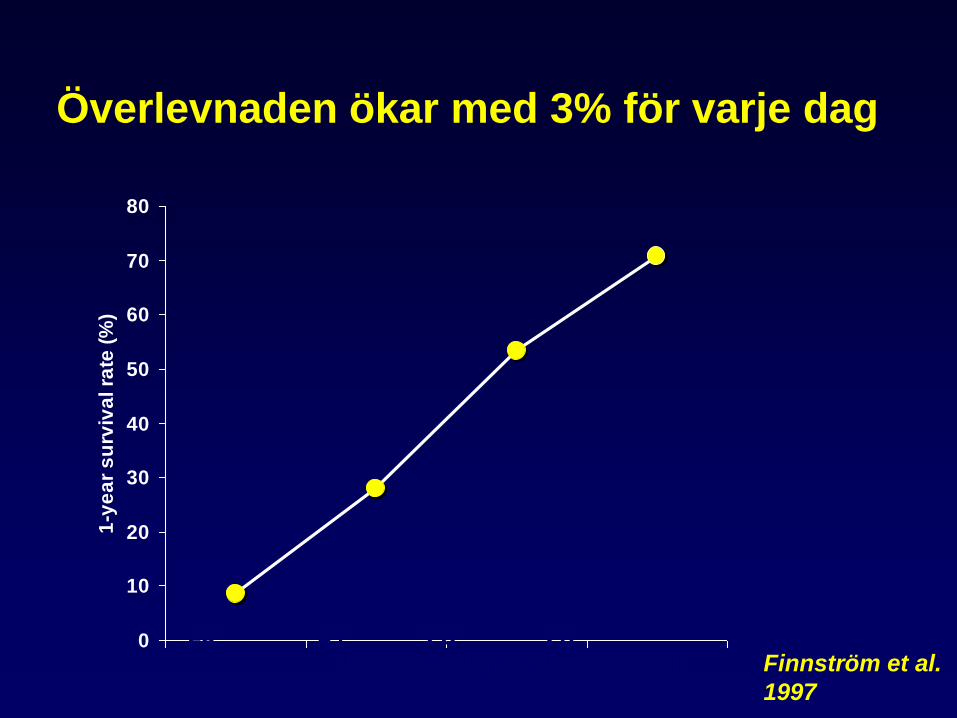
Överlevnaden ökar med 3% för varje dag
0
10
20
30
40
50
60
70
80
1-y
ea
r s
urv
iva
l ra
te (
%)
24
Completed gestation (weeks) Finnström et al.
1997
23 25 26
0
10
20
30
40
50
60
70
80
90
Percent
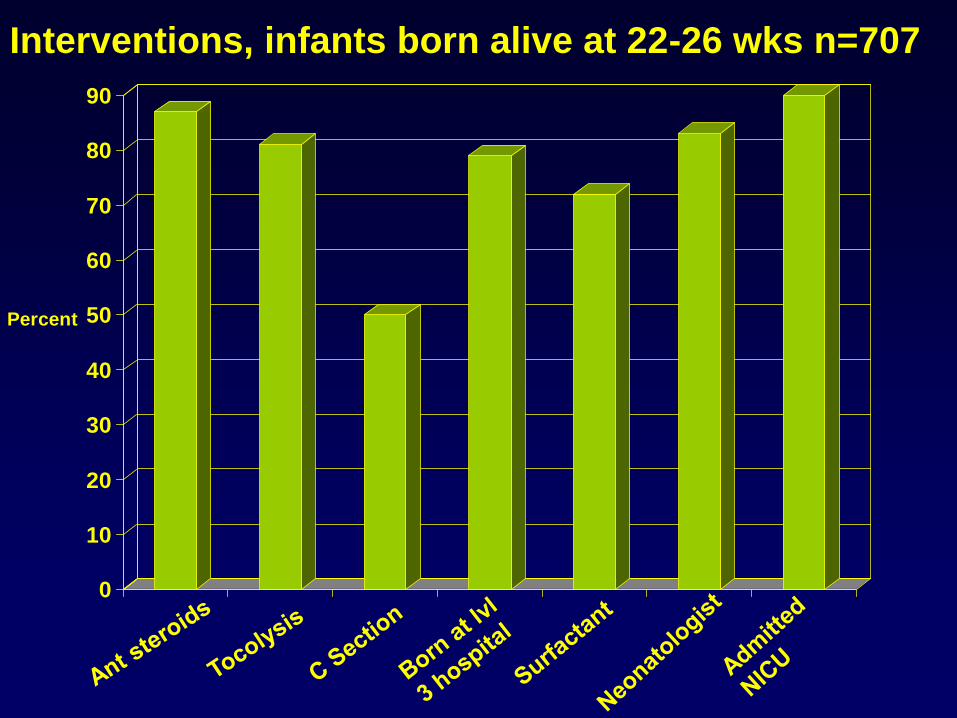
Interventions, infants born alive at 22-26 wks n=707
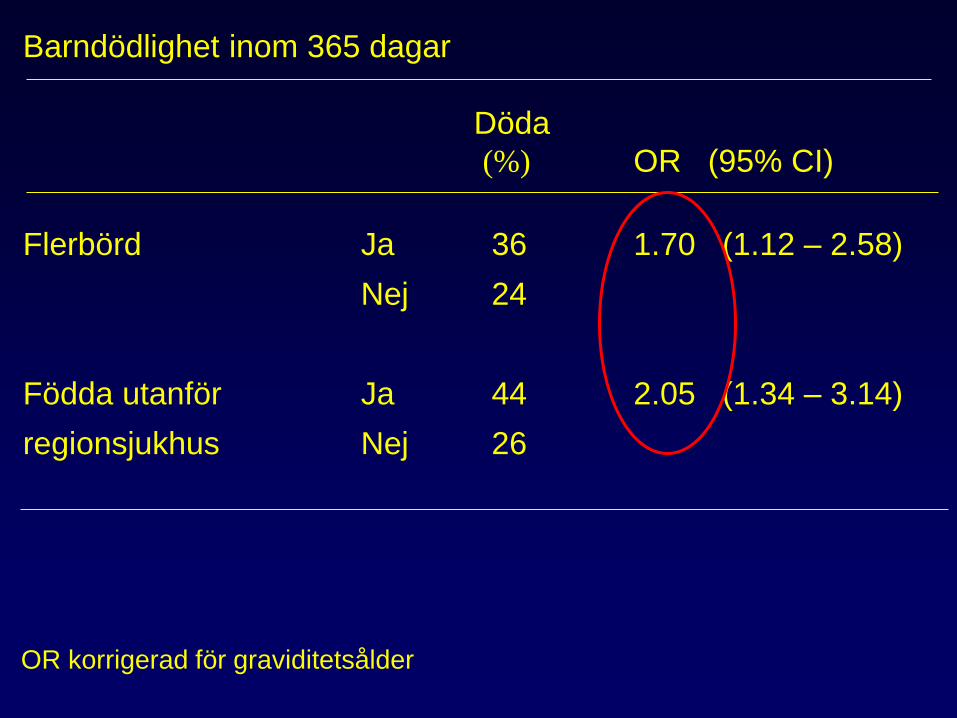
Barndödlighet inom 365 dagar
Döda
(%) OR (95% CI)
Flerbörd Ja 36 1.70 (1.12 – 2.58)
Nej 24
Födda utanför Ja 44 2.05 (1.34 – 3.14)
regionsjukhus Nej 26
OR korrigerad för graviditetsålder
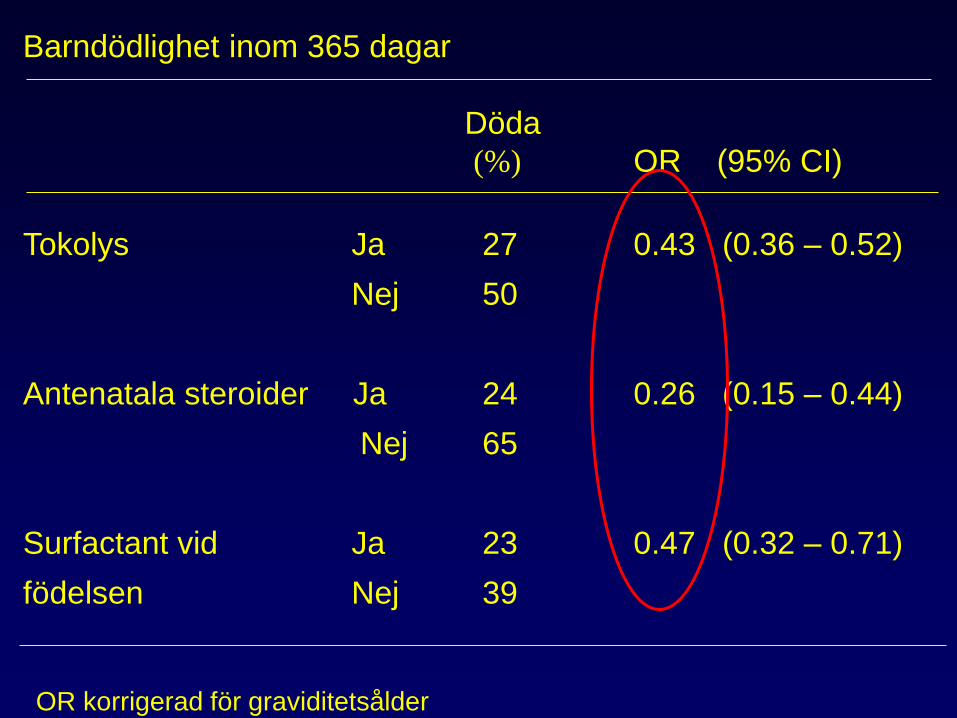
Barndödlighet inom 365 dagar
Döda
(%) OR (95% CI)
Tokolys Ja 27 0.43 (0.36 – 0.52)
Nej 50
Antenatala steroider Ja 24 0.26 (0.15 – 0.44)
Nej 65
Surfactant vid Ja 23 0.47 (0.32 – 0.71)
födelsen Nej 39
OR korrigerad för graviditetsålder
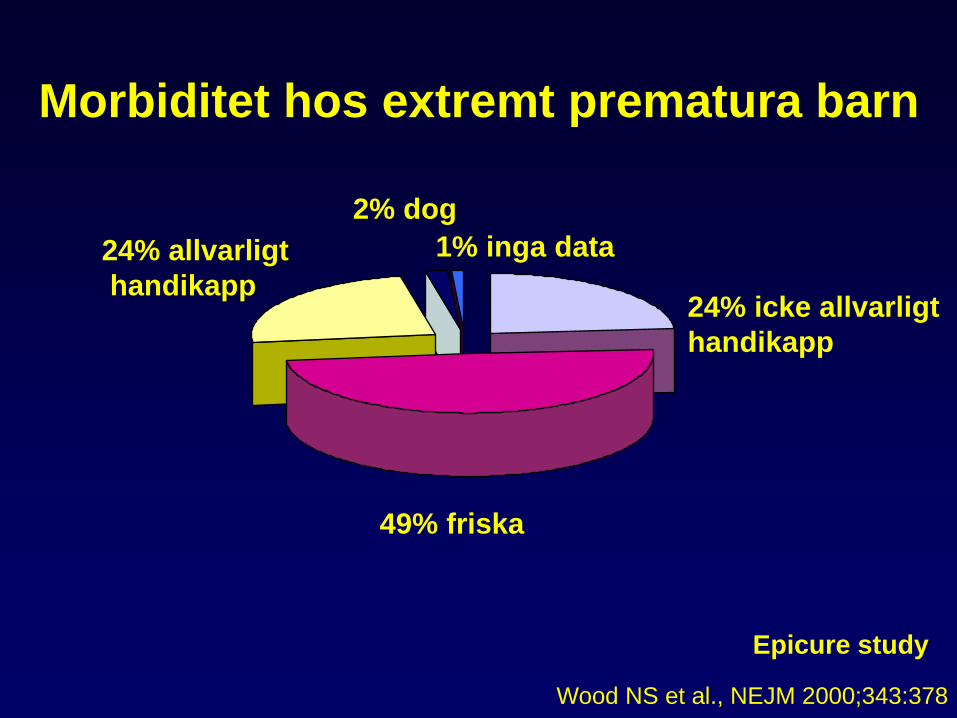
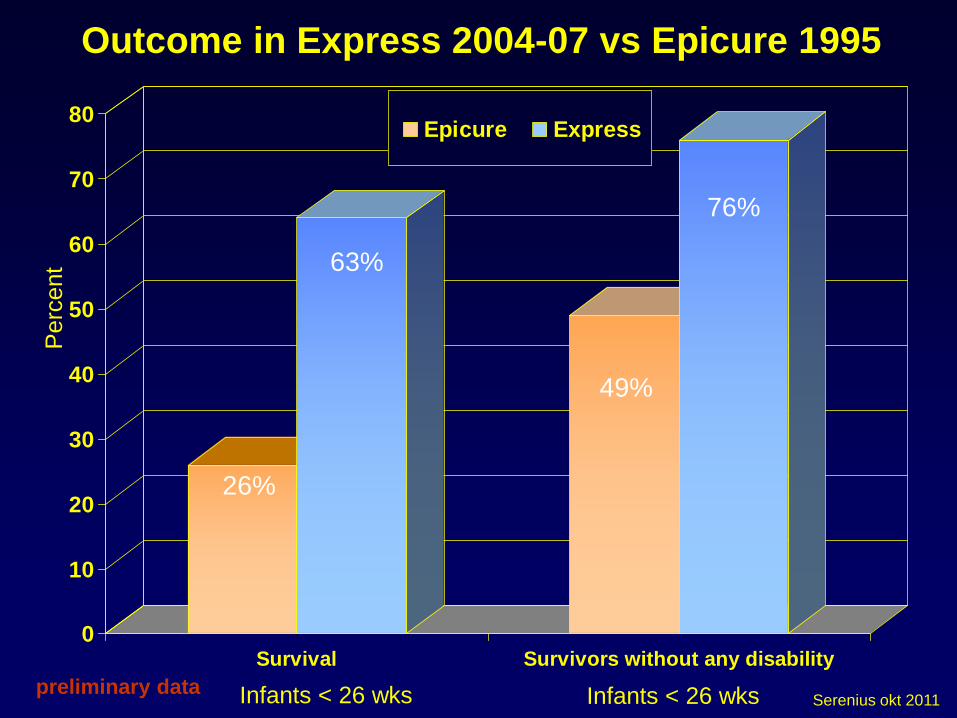
Morbiditet hos extremt prematura barn
49% friska
24% icke allvarligt
handikapp
24% allvarligt
handikapp
2% dog
1% inga data
Epicure study
Wood NS et al., NEJM 2000;343:378
0
10
20
30
40
50
60
70
80
Survival Survivors without any disability
Epicure Express
Perc
ent
Outcome in Express 2004-07 vs Epicure 1995
Infants < 26 wks Infants < 26 wks preliminary data
76%
49%
63%
26%
Serenius okt 2011
0
10
20
30
40
50
60
70
80
90
. 22 23 24 25 26 . All .
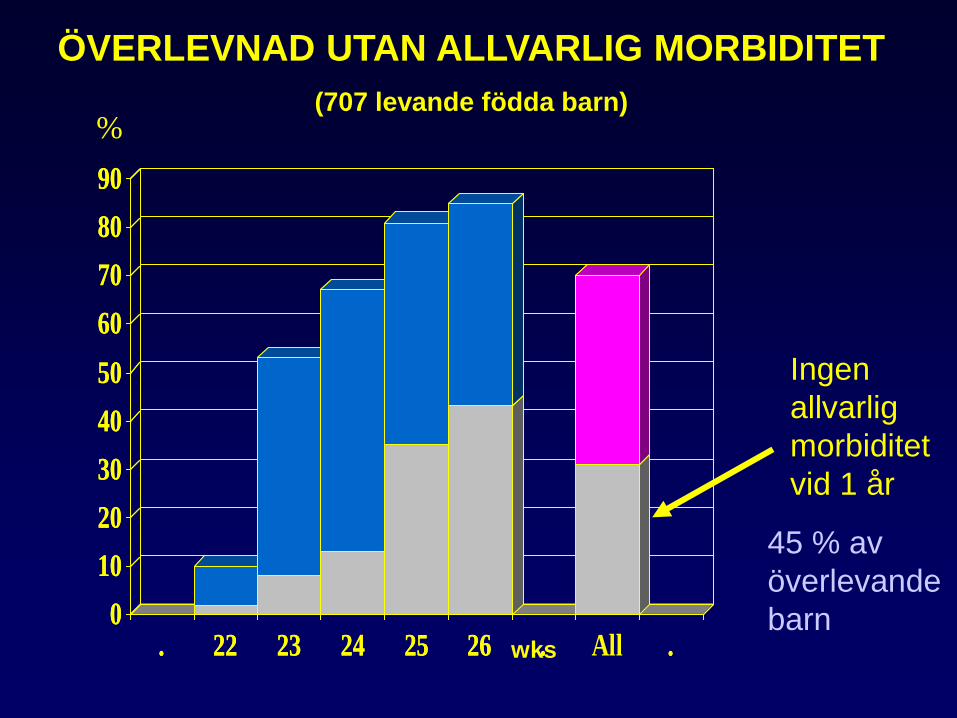
ÖVERLEVNAD UTAN ALLVARLIG MORBIDITET
(707 levande födda barn)
wks
Ingen
allvarlig
morbiditet
vid 1 år
%
0
10
20
30
40
50
60
70
80
90
. 22 23 24 25 26 . .
45 % av
överlevande
barn
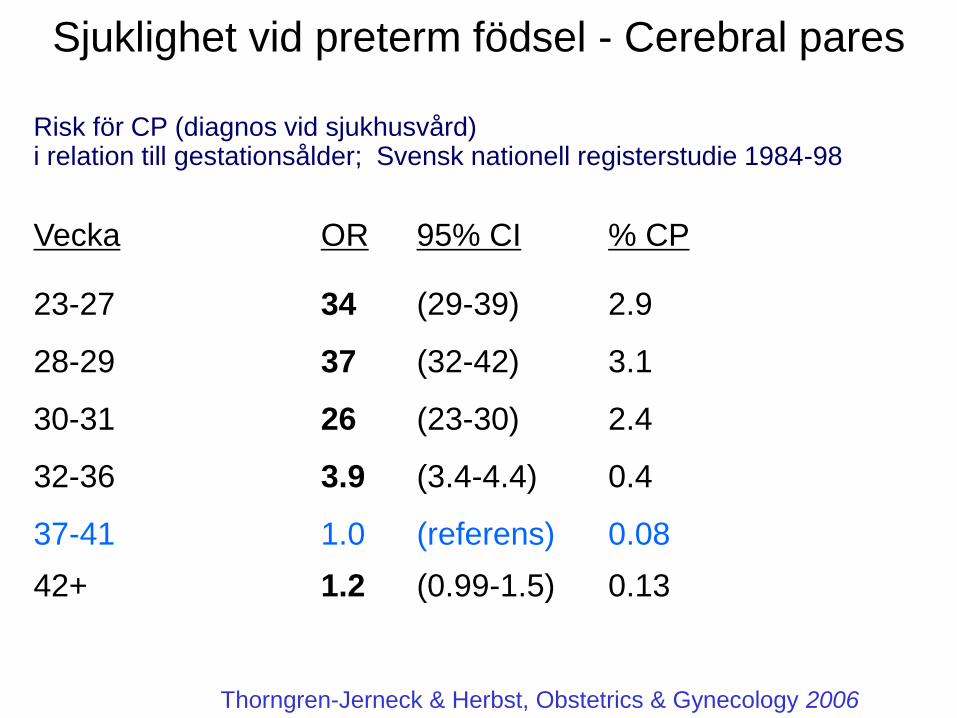
Sjuklighet vid preterm födsel - Cerebral pares
Risk för CP (diagnos vid sjukhusvård) i relation till gestationsålder; Svensk nationell registerstudie 1984-98
Vecka OR 95% CI % CP
23-27 34 (29-39) 2.9
28-29 37 (32-42) 3.1
30-31 26 (23-30) 2.4
32-36 3.9 (3.4-4.4) 0.4
37-41 1.0 (referens) 0.08
42+ 1.2 (0.99-1.5) 0.13
Thorngren-Jerneck & Herbst, Obstetrics & Gynecology 2006
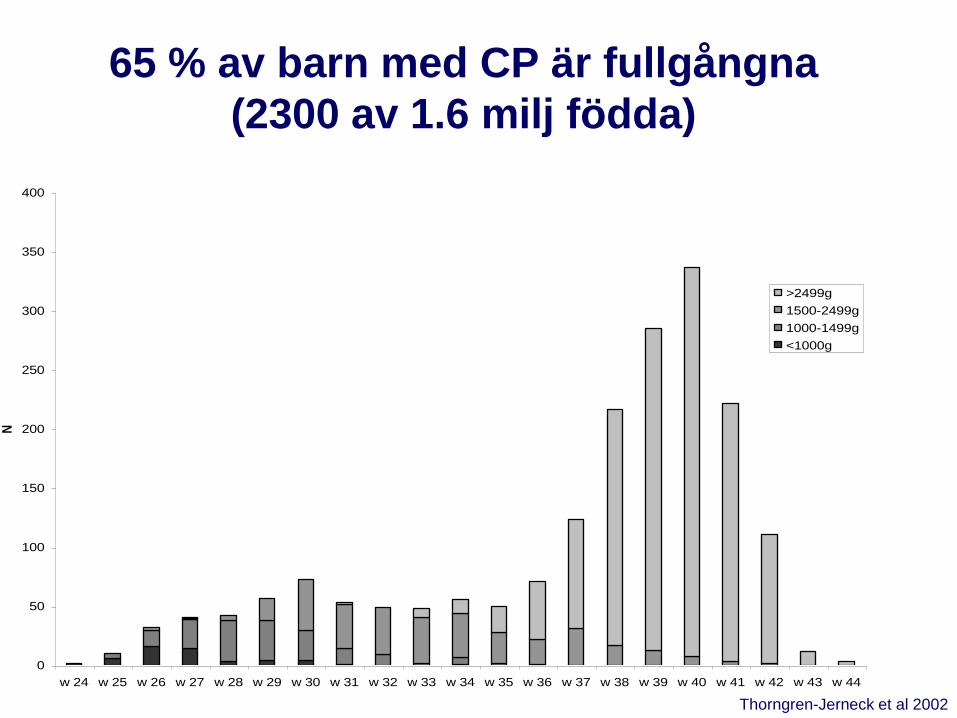
65 % av barn med CP är fullgångna
(2300 av 1.6 milj födda)
0
50
100
150
200
250
300
350
400
w 24 w 25 w 26 w 27 w 28 w 29 w 30 w 31 w 32 w 33 w 34 w 35 w 36 w 37 w 38 w 39 w 40 w 41 w 42 w 43 w 44
N
>2499g
1500-2499g
1000-1499g
<1000g
Thorngren-Jerneck et al 2002
Risk factors
Medical history
• Prior PTB
• Maternal age
• Low SES
• Race
• Uterine anomalies
• Trauma
Current Pregnancy
• Maternal infections – bacteriuria
– pyelonephritis
– genital tract (BV)
– pneumonia
• PPROM
• Uterine distention – twins, polyhydramnios
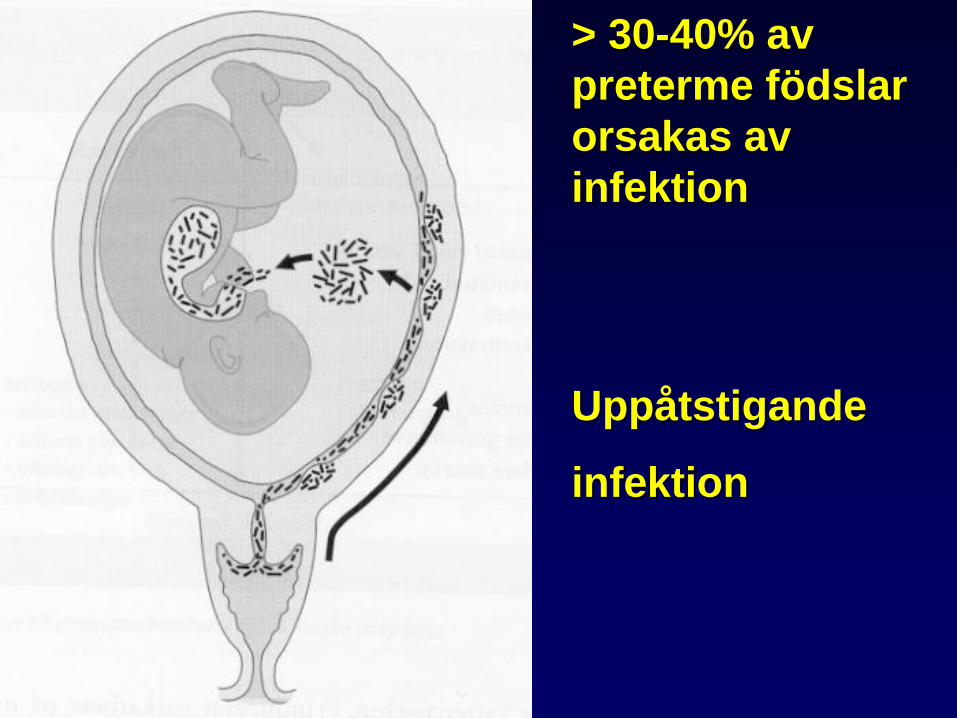
Uppåtstigande
infektion
> 30-40% av
preterme födslar
orsakas av
infektion
Can PTB be predicted?
Prediction of PTL
• Contractions
• Rupture of membranes
• Gestational length
• Cervical length
• Biochemical markers
Diagnosen av hotande
preterm födsel er svår
• Vad er skilnaden mellom värkar
(contractions) och förvärkar
(Braxton Hicks contractions)?
• Cervix ändringar er viktigt at
vardera
– Inspektion ?
– Fingror ?
– Ultraljud ?
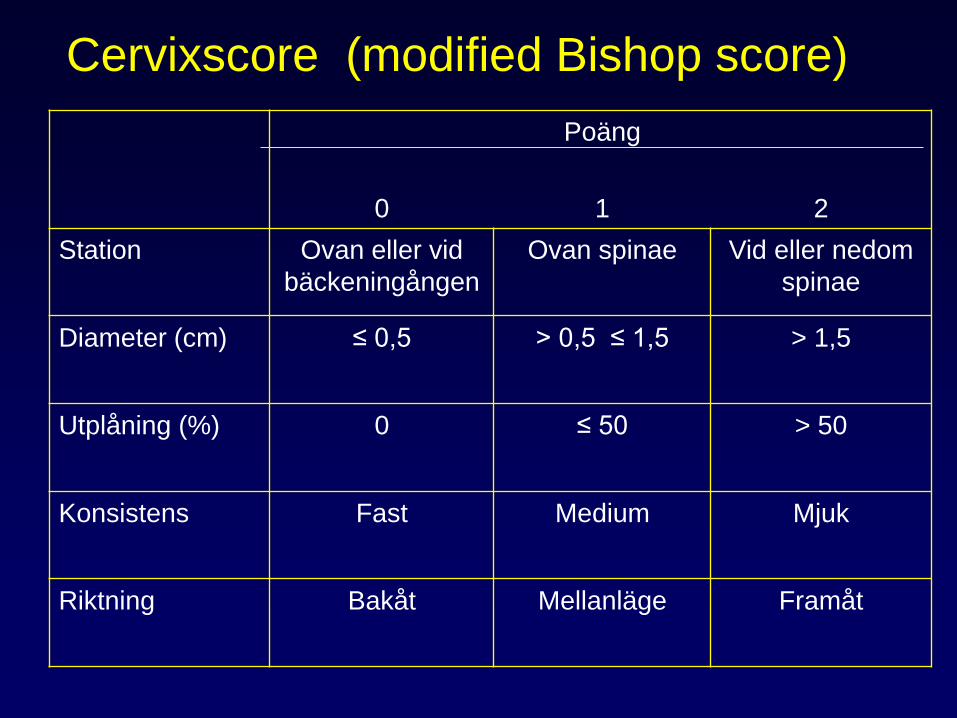
0
Poäng
1
2
Station Ovan eller vid
bäckeningången
Ovan spinae Vid eller nedom
spinae
Diameter (cm) ≤ 0,5 > 0,5 ≤ 1,5 > 1,5
Utplåning (%) 0 ≤ 50
> 50
Konsistens Fast Medium Mjuk
Riktning Bakåt Mellanläge Framåt
Cervixscore (modified Bishop score)
Oracle II clinical trial
• RCT, N= 6295 - no PPROM - no clinical
signs of infection
• Included if a doctor decided that she
needed treatment for preterm labour
• Untreated controls, n = 1556
• Undelivered after 7 days, 1323 (85%)
Kenyon et al. Lancet 2001;357: 989-94
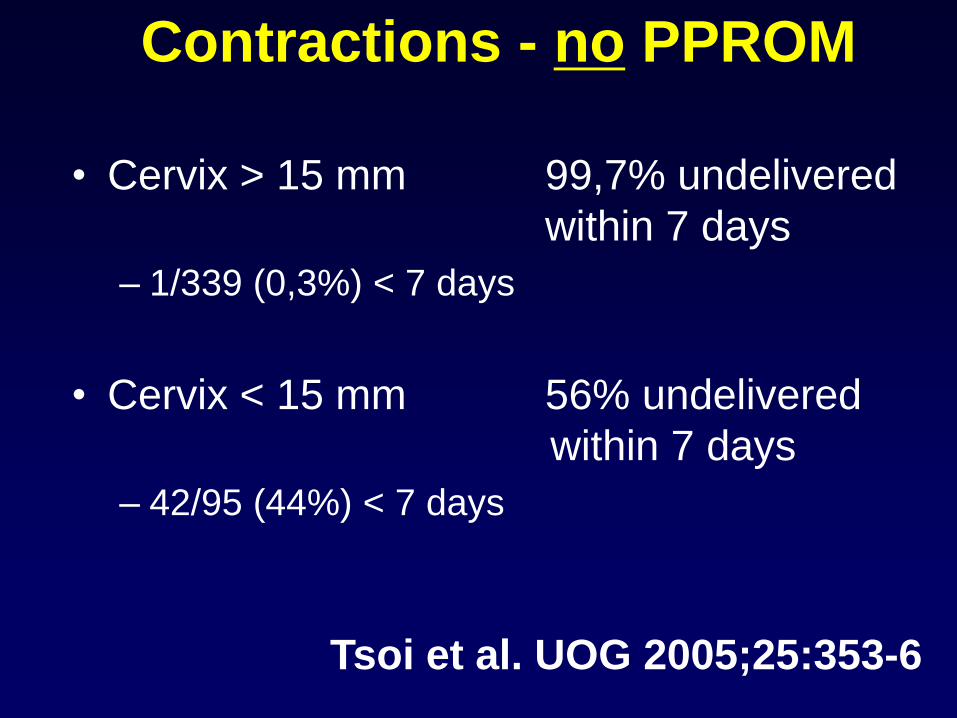
Contractions - no PPROM
• Cervix > 15 mm 99,7% undelivered
within 7 days
– 1/339 (0,3%) < 7 days
• Cervix < 15 mm 56% undelivered
within 7 days
– 42/95 (44%) < 7 days
Tsoi et al. UOG 2005;25:353-6
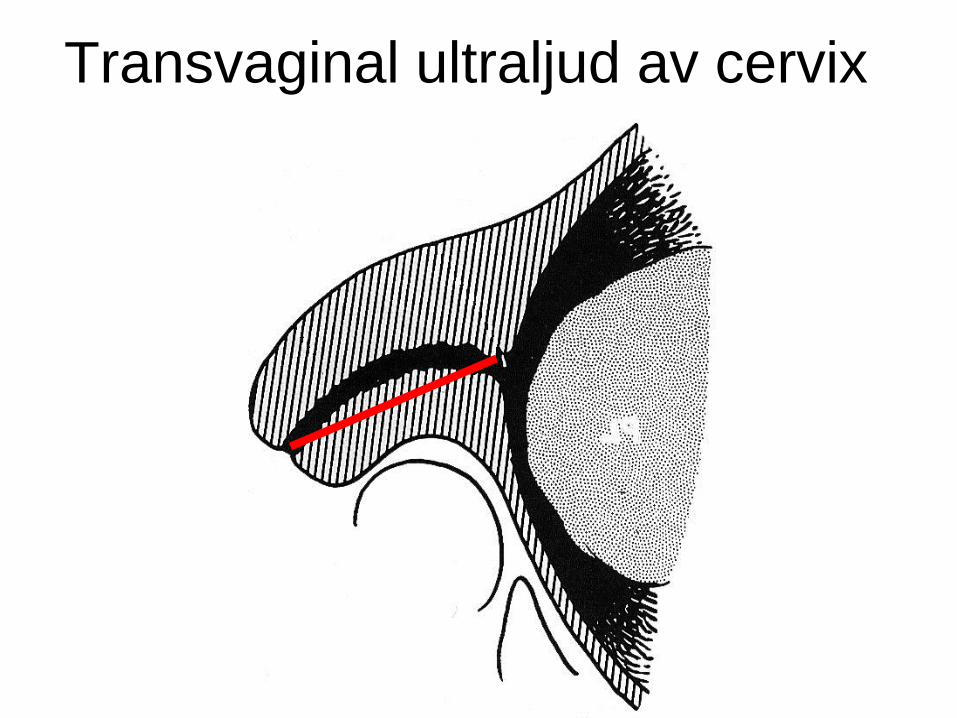
Transvaginal ultraljud av cervix
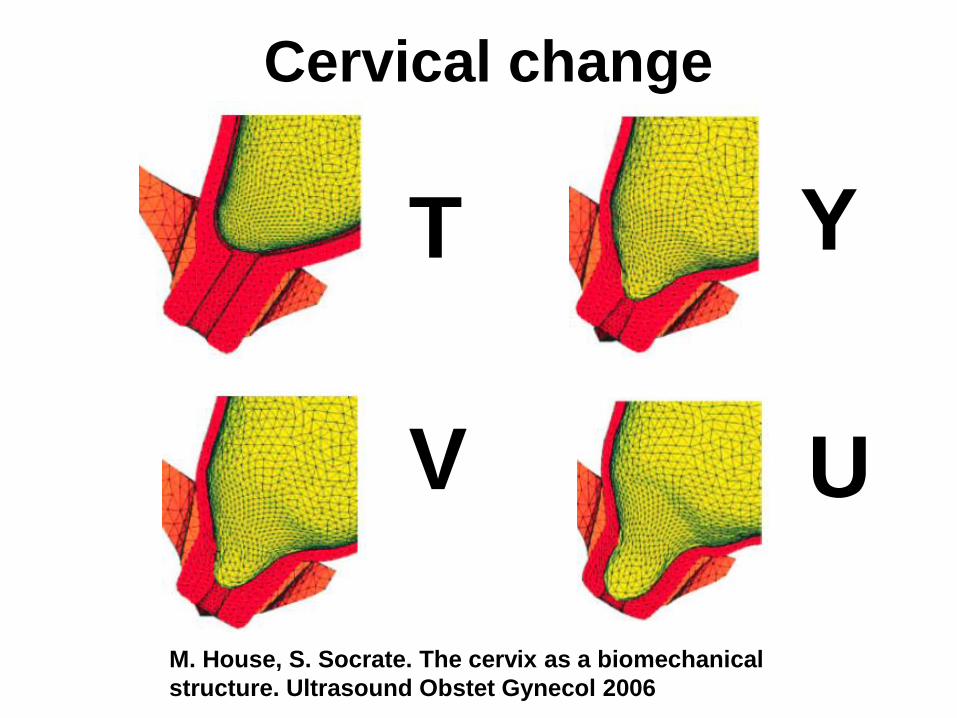
Cervical change
M. House, S. Socrate. The cervix as a biomechanical
structure. Ultrasound Obstet Gynecol 2006
T Y
V U
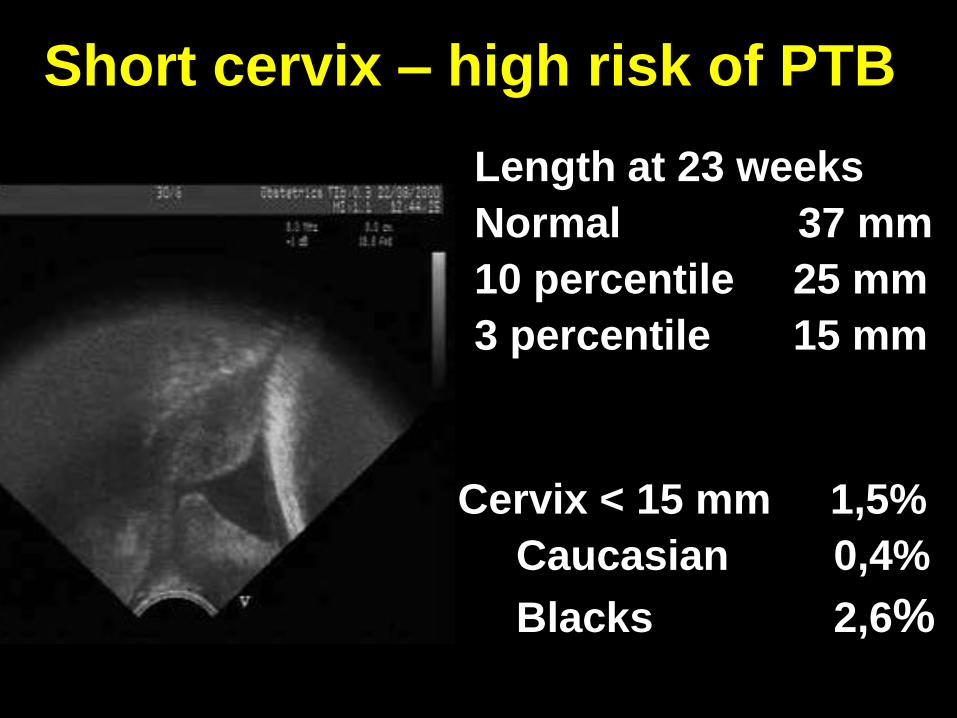
Short cervix – high risk of PTB
Cervix < 15 mm 1,5%
Caucasian 0,4%
Blacks 2,6%
Length at 23 weeks
Normal 37 mm
10 percentile 25 mm
3 percentile 15 mm
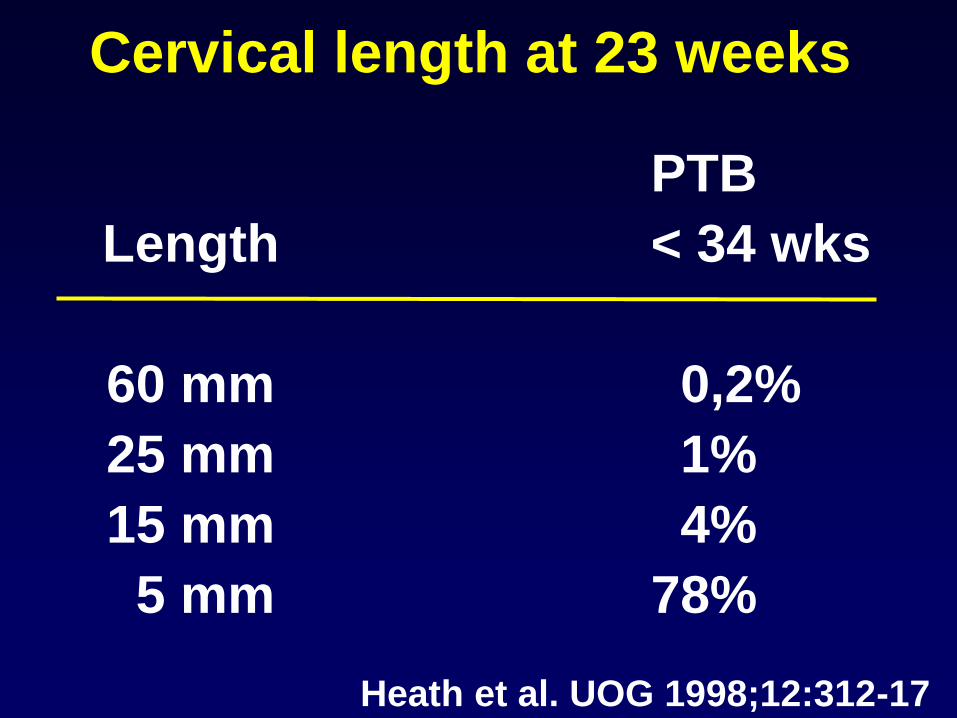
Cervical length at 23 weeks
PTB
Length < 34 wks
60 mm 0,2%
25 mm 1%
15 mm 4%
5 mm 78%
Heath et al. UOG 1998;12:312-17
Fibronectin and PTD
• Best prediction – short
term in clinical situations
• Even better when
combined with ultrasound
• Useful test in symptomatic
women on one condition:
• The test must be negative
H. Leitich et al. Cervicovaginal fetal fibronectin as a marker for
preterm delivery: a meta–analysis. Am J Obstet Gynecol 1999
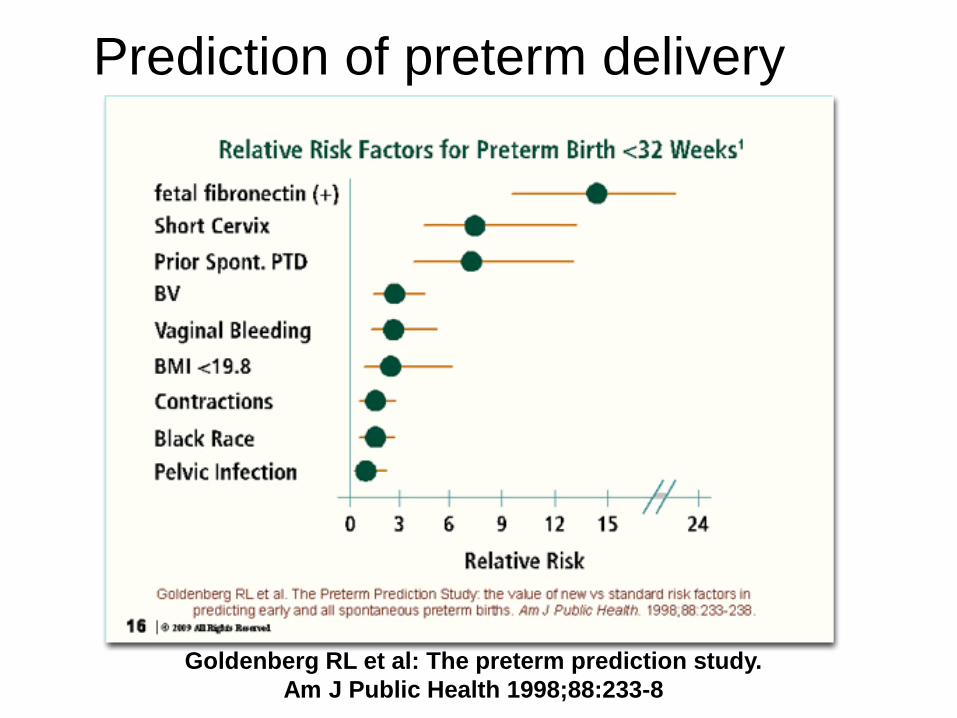
Prediction of preterm delivery
Goldenberg RL et al: The preterm prediction study.
Am J Public Health 1998;88:233-8
Can we prevent PTD?
• Bed rest?
• Tocolysis?
• Life style changes?
• Cerclage?
• Progesterone?
Tocolysis - remove contractions
• Oxytocin antagonist (Tractocile®)
• Calsium antagonist (Adalat®)
• Betamimetics (Bricanyl®)
• Prostaglandin synthesis inhibitor
(Indometacin®, cox-2 antagonists)
• Smooth muscle relaxation
(Nitroglycerin)
Moderate effect of tocolysis
• Postpone delivery up to 48 hours,
but the prognosis is not improved
• Principle: Give tocolysis to get
effect of steroids and to secure the
time and place of a preterm
delivery
Vinster med tokolys
– Transport in utero till perinatalt centrum
– Administration av steroider
• Lungmognad
• Minskning av risken för
• RDS (respiratory distress disease)
• IVH (intraventricular hemorrhage)
• NEC (necrotisizing enterocolitis)
Preterm vattenavgång (PPROM)
Diagnos:
- anamnes
- steril speculumundersökning (inspektion)
- bromthymol test (pinnprov)
- (arborisation test)
- observation
Behandling:
- antibiotika
- i øvrigt som vid PTL
Handläggning enligt grav. åldern:
<20+0 v. överväg avbrytande av graviditet
20+0–23+6 individual handläggning, ev. poliklinisk
24+0 v. Undvik palpation (inspektion + ultraljud är OK)
Ultraljudsutvärdering av fostret
Cervixodling – upprepade ggr
Kontroller – kroppstemperatur, CRP, vita, CTG
Antibiotika
Preterm vattenavgång (PPROM)
• erfaren obstetriker
• erfaren neonatolog
• sectio vs. vaginal förlossning ? (bjudning? duplex?)
• försiktig användning av oxytocin
• CTG, scalp pH
• analgesi (EDA)
• episiotomi (klipp)
• om möjligt behålla hinnsäcken
• tång vs. vacuum extraktion ?
• operationsteknik vid kejsarsnitt
Preterm förlossning
Underburenhet
Individuell handläggning !
Can we prevent PTD?
• Bed rest?
• Tocolysis?
• Life style changes?
• Cerclage?
• Progesterone?
Cervical insufficiency
• Causes of cervical insufficiency
–Uterine anomalies (bicorn uterus,
septum)
– (Late) surgical abortions
–Conisation
–Unknown
Causes < 10% of PTB
Cervical insufficiency is a
clinical diagnosis
• Medical history of 2nd trimester
abortion or PTB (several times)
with opening of the cervix
without contractions
• PPROM +/-
• The treatment is cerclage
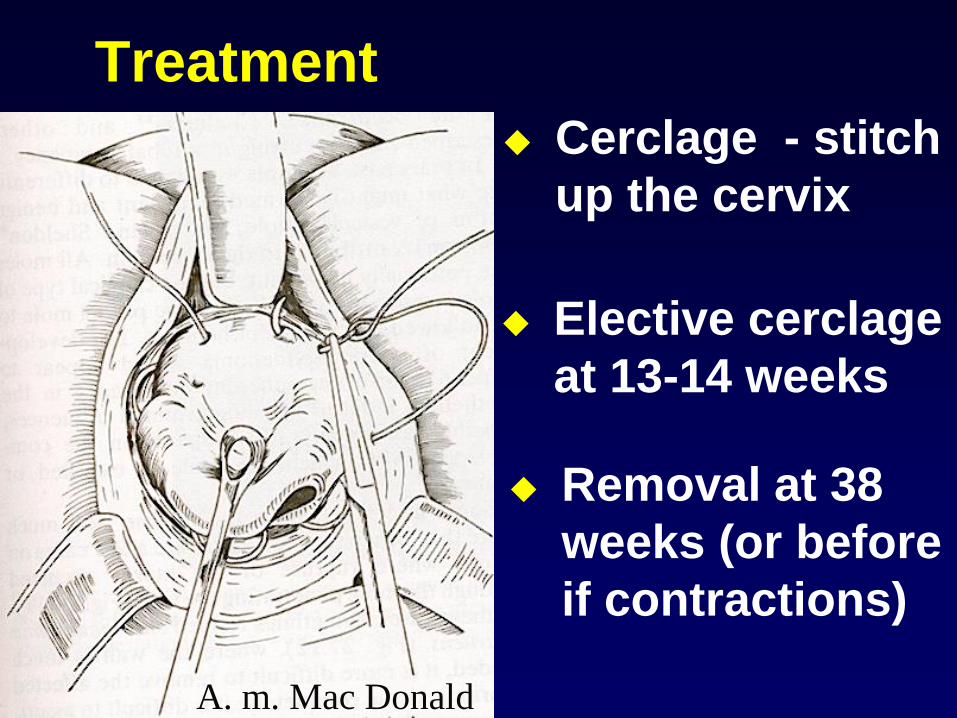
Treatment
Elective cerclage
at 13-14 weeks
A. m. Mac Donald
Removal at 38
weeks (or before
if contractions)
Cerclage - stitch
up the cervix
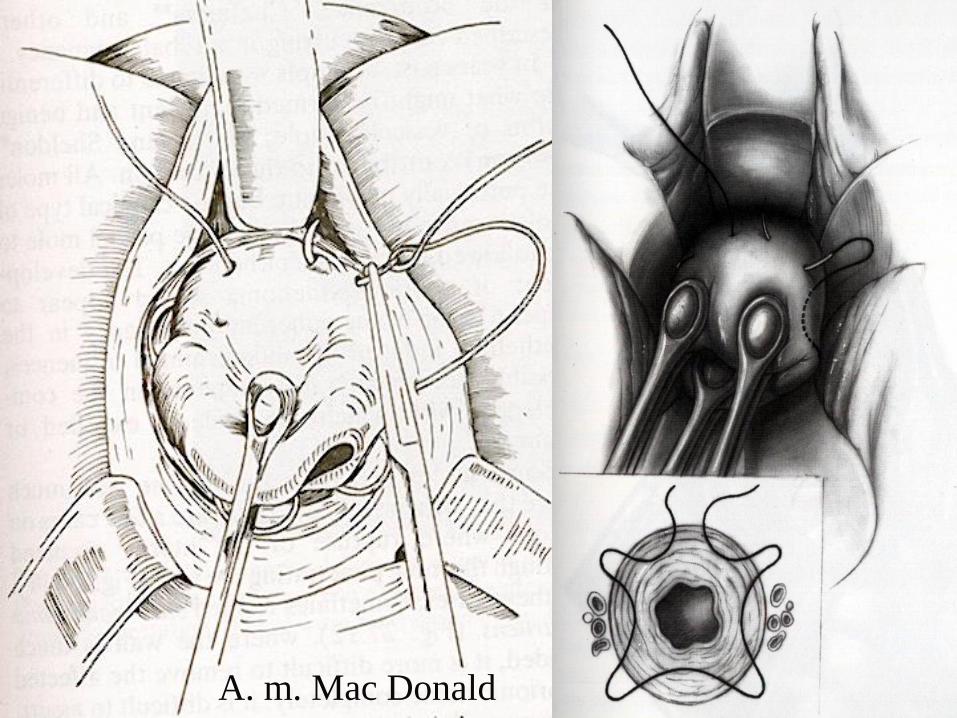
A. m. Mac Donald
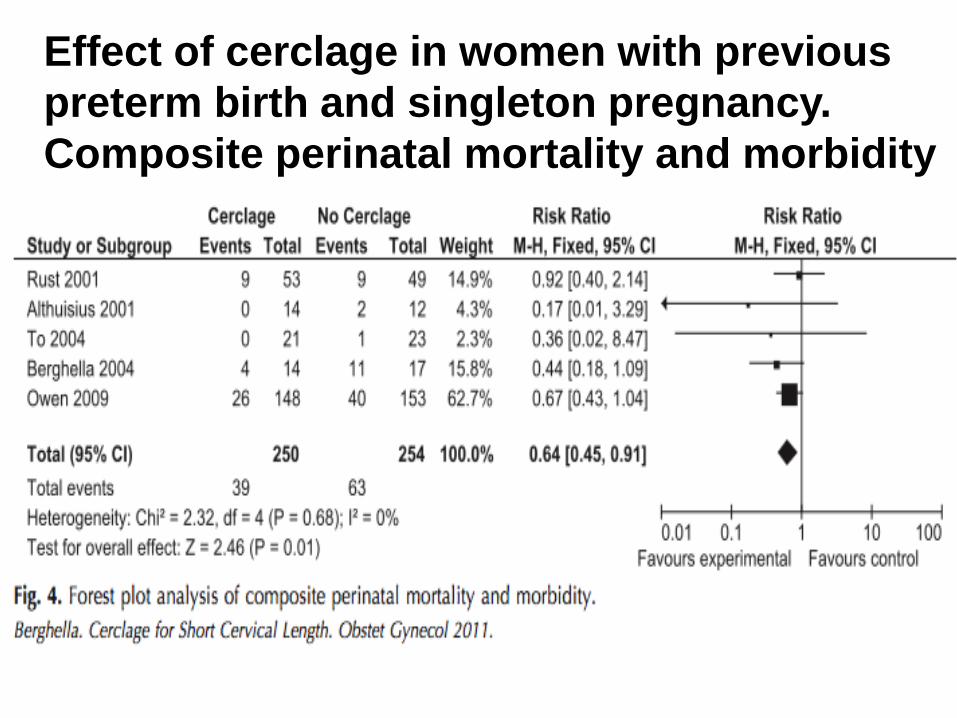
Effect of cerclage in women with previous
preterm birth and singleton pregnancy.
Composite perinatal mortality and morbidity
Progesterone
• Key hormone - start of labour (animals)
• Smooth muscle insensitive to stretch
• Placenta produces large amounts
• RCTs have found that progesterone
reduces the risk of recurrent preterm
delivery in high risk women
Progesterone - singletons
• N = 24 620 screened with TVS at 22 weeks
• Cervical length < 15 mm in n = 413 (1,7%)
• RCT - Vaginal progesterone 200 mg x 1
• Delivery < 34 weeks
– Progesterone group 19%
– Placebo group 34% p = 0.007
Fonseca EB et al. N Engl J Med 2007; 375: 462-9
Progesterone - singletons
• N = 32 091 screened with TVS 19-24 weeks
• Cervix length 10-20 mm in n = 733 (2,3%)
• 16% previous history, 9% cervical surgery
• RCT - Vaginal progesterone 90 mg x 1
– Acute Cerclage 10 vs 6 (p = 0,46), - 16 (3%) in total
• PTD < 33 weeks
– Progesterone 9%
– Placebo 16% p = 0.02
Hassan SS et al. Ultrasound Ob Gyn 2011; 38: 18-31
Progesterone - singletons
• “Doing nothing is no longer an
option”
• Cervix length cut-off at 20 weeks? Cervix < 25 mm
– 50% of all births < 34 weeks and 10% of all
women
Cervix < 5 mm
– No effect of progesterone (– too late?)
Campbell S. Ultrasound Obstet Gynecol 2011; 38: 1-9
Progesterone - twins
• N = 1526 twins, n = 661 randomised
• RCT: 17 - progesterone - 250 mg im daily
from 16 to 35 weeks
• PTB or IUFD < 35 weeks
– Progesterone 42%
– Placebo 37% ns.
• No data on cervical length
Rouse DJ et al. N Engl J Med 2007; 375: 454-61