Embed Size (px)
Citation preview
1
Inventors of the HeRO™ Vascular Access Device
The HeRO™ Vascular Access Device:The HeRO™ Vascular Access Device:A New Solution for the AV Access-Challenged PatientChallenged Patient
1
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

2
Learning ObjectivesLearning Objectives
Upon completion of this presentation, participants will p p p , p pbe able to:
Relate the significance of long-term catheter use to the i d t f b t i i d f di l i dincreased rate of bacteremia, inadequacy of dialysis and risk of mortality in the catheter patient population
2. Summarize key results from the HeRO™ Clinical Studyy y
3. Recognize a HeRO™ device implant patient
4. Describe the appropriate physical pp p p yassessment/cannulation technique of HeRO™ patients and additional management considerations
5 List characteristics of potential HeRO™ candidates
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
5. List characteristics of potential HeRO™ candidates

3
OutlineOutline
And I will do this by:
1. CPM data will be used to illustrate the growing prevalence of catheters and extrapolated to current HD data from 2008 USRDS data. KDOQI of 2006 goals will be reiterated.
2. Phase 3 clinical trial showing adequacy and infection data leading to FDA approval of this device as a graft
3 Th 3 i i i th t d fi H RO i l t ill b d ib d i3. The 3 incisions that define a HeRO implant will be described in detail along with history evidence
4. KDOQI 2006 graft cannulation guidelines will be reviewed along ith th btl h i l t diff t dwith the subtle physical assessment differences encountered
with HeRO
5.Clear inclusion and exclusion criteria will be given emphasizing th t thi i t ti f th ti t h h AVF
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
that this is not an access option for those patients who have AVF or AVG upper extremity options
4
The Catheter Problem
4
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

5
Patient StoryPatient Story
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

6
The Catheter Problem: Growing Catheter UtilizationGrowing Catheter Utilization
TimePeriod Incidence Prevalence
AVF AVG CVC AVF AVG CVC
Oct – Dec20051
AVF AVG CVC AVF AVG CVC
54% 10% 36% 44% 26% 27%
Oct – Dec20062 41% 13% 45% 45% 26% 29%
12006 ESRD CPM (Clinical Performance Measures) Project Table 922007 ESRD CPM (Clinical Performance Measures) Project Table 9
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
7
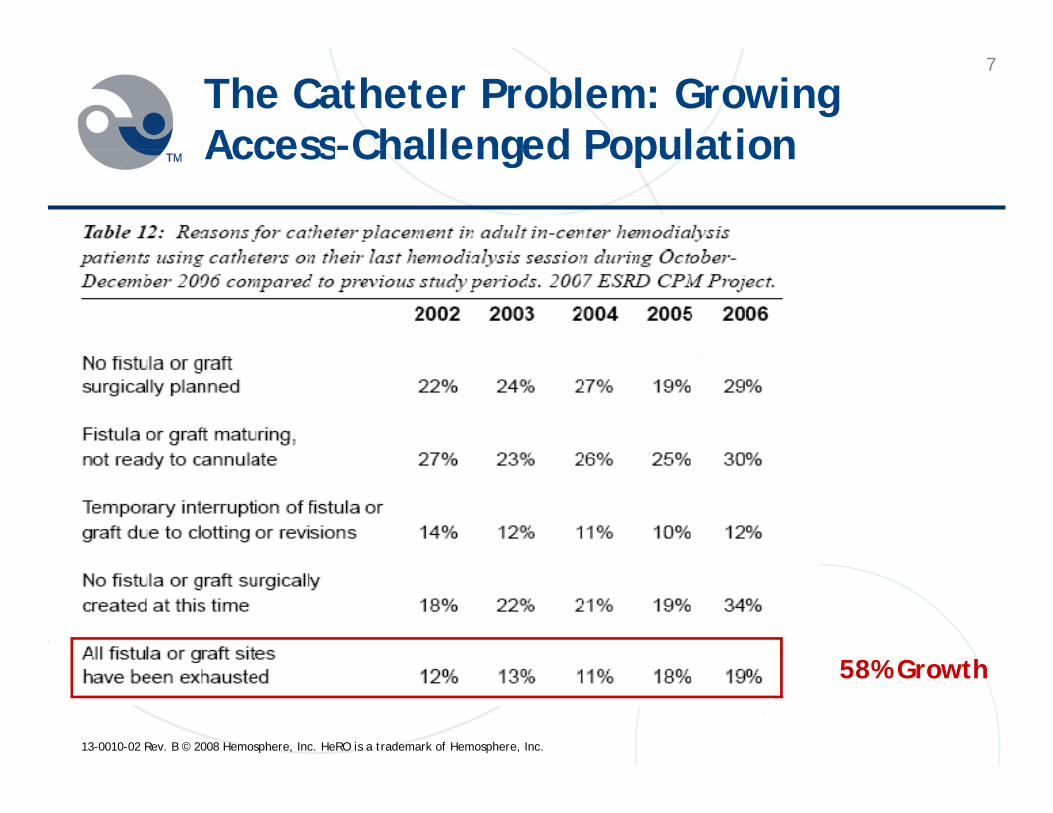
The Catheter Problem: Growing Access-Challenged PopulationAccess Challenged Population
58% G th
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
58% Growth
8
The Catheter Problem: BacteremiaThe Catheter Problem: Bacteremia
Bacteremia is the second leading cause ofBacteremia is the second leading cause ofhemodialysis patient death and catheters are the primary contributing factor
• KDOQI reports an IJ catheter-related overall bacteremia rate of 1.6-5.5 per 1,000 catheter days1
H RO™ li i l d d li l f 2 3 1 000 • HeRO™ clinical study used a literature control of 2.3 per 1,000 catheter days2
• Femoral catheter bacteremia rates are typically 2 times higher3e o al cat ete bacte e a ates a e typ cally t es g e1NKF K/DOQI Clinical Practice Guidelines and Clinical Practice Recommendations 2006 Updates2Oliver, M., Lynch, L. Estimate of the Risk and Rate of Hemodialysis Catheter-Related Bacteremia. 2006. Hemosphere, Inc. document. (Hemosphere
scientific literature review of prospective or randomized studies of tunneled IJ catheters (15 articles) with 20 patients or more).3Lynch, L. Dialysis Catheter Literature Summary. 2007. Hemosphere, Inc. document. (Hemosphere Scientific literature review of non-device related
IJ/SCV catheter infections and device-related femoral catheter infections (4 articles)).
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
9
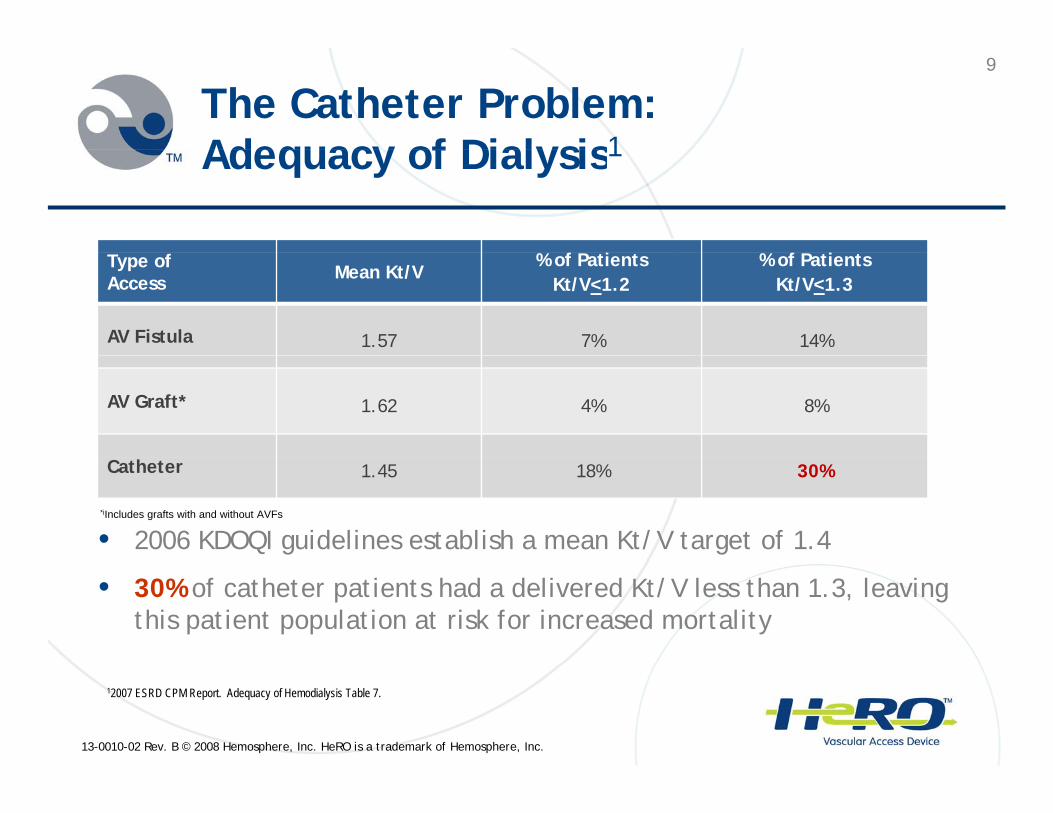
The Catheter Problem: Adequacy of Dialysis1Adequacy of Dialysis1
% f P i % f P iType of Access Mean Kt/V
% of PatientsKt/V<1.2
% of PatientsKt/V<1.3
AV Fistula 1.57 7% 14%
AV Graft* 1.62 4% 8%
Catheter 1.45 18% 30%
• 2006 KDOQI guidelines establish a mean Kt/V target of 1.4*iIncludes grafts with and without AVFs
• 30% of catheter patients had a delivered Kt/V less than 1.3, leaving this patient population at risk for increased mortality
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
12007 ESRD CPM Report. Adequacy of Hemodialysis Table 7.
10
The Catheter Problem: Increased Patient MortalityIncreased Patient Mortality
The mortality rate increases by 7% for each 0.1unit decrease in Kt/V1
There is a 40% higher mortality rate for catheter g ypatients compared to fistula patients2
1 Dhingra, R., Young, E., Hulbert-Shearon, T., Leavey, S., Port, F. Type of Vascular Access and Mortality in the U.S. Hemodialysis Patients. Kidney International.
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
g , , g, , , , y, , , yp y y y2001. Vol 60, pp. 1443-1451
2 Pastan, S., et. al. Vascular access and increased risk of death among hemodialysis patients. Kidney International. 2002: 620-626

11
The Catheter Problem: SummaryThe Catheter Problem: Summary
Catheter utilization is growing Catheter utilization is growing
Number of patients who have exhausted all fistula and graft sites is growing graft sites is growing
High incidence of bacteremia is associated with long-term catheter use
Measured Kt/V is lower in catheter patients
Mortality rates are significantly higher in catheter Mortality rates are significantly higher in catheter patients compared to fistula patients
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

12
The HeRO™ Vascular Access lDevice Solution
12
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

13
HeRO™ Device DescriptionHeRO Device Description
The HeRO™ device is the new long-term permanent The HeRO device is the new long term permanent access solution for access-challenged and catheter-dependent patients
• Fully subcutaneous surgical implant
• AV access with continuous outflow • AV access with continuous outflow into the central venous system
• Traverses central venous stenosis allowing for long term hemodialysis accessallowing for long-term hemodialysis access
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

14
HeRO™ Vascular Access Device
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

15
HeRO™ Vascular Access Device I t d d U & FDA Cl ifi tiIntended Use & FDA Classification
The HeRO™ is intended for use in maintaining long-term vascular access for chronic hemodialysis patients who have exhausted peripheral venous access sites suitable for fistulas or grafts
The FDA classified the HeRO™ device as a graft
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

16
HeRO™ Right-Sided Implant Visual
Graft Component
Dialysis Access
Area
Outflow Component
AreaRadiopaque Tip
Arterial Anastomosis
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
17
HeRO™ Implantation: Step 1p p
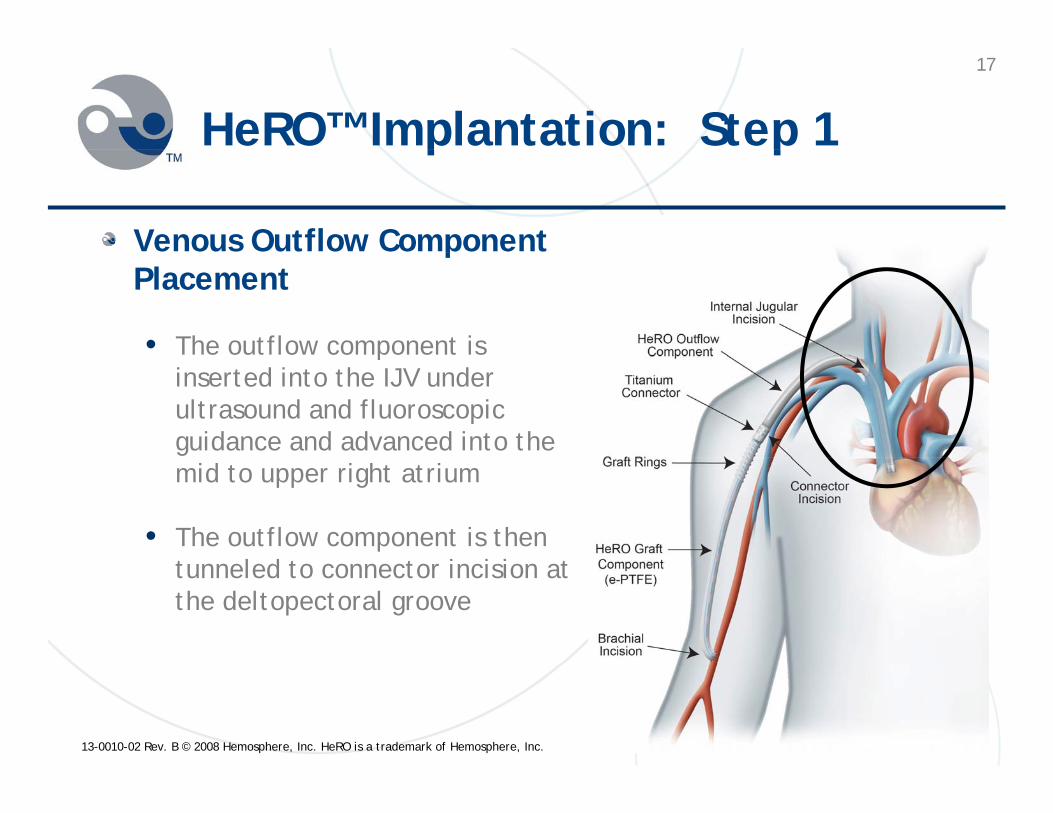
Venous Outflow Component pPlacement
• The outflow component is pinserted into the IJV under ultrasound and fluoroscopic guidance and advanced into the mid to upper right atrium
• The outflow component is then t l d t t i i i t tunneled to connector incision at the deltopectoral groove
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
18
HeRO™ Implantation: Step 2p p
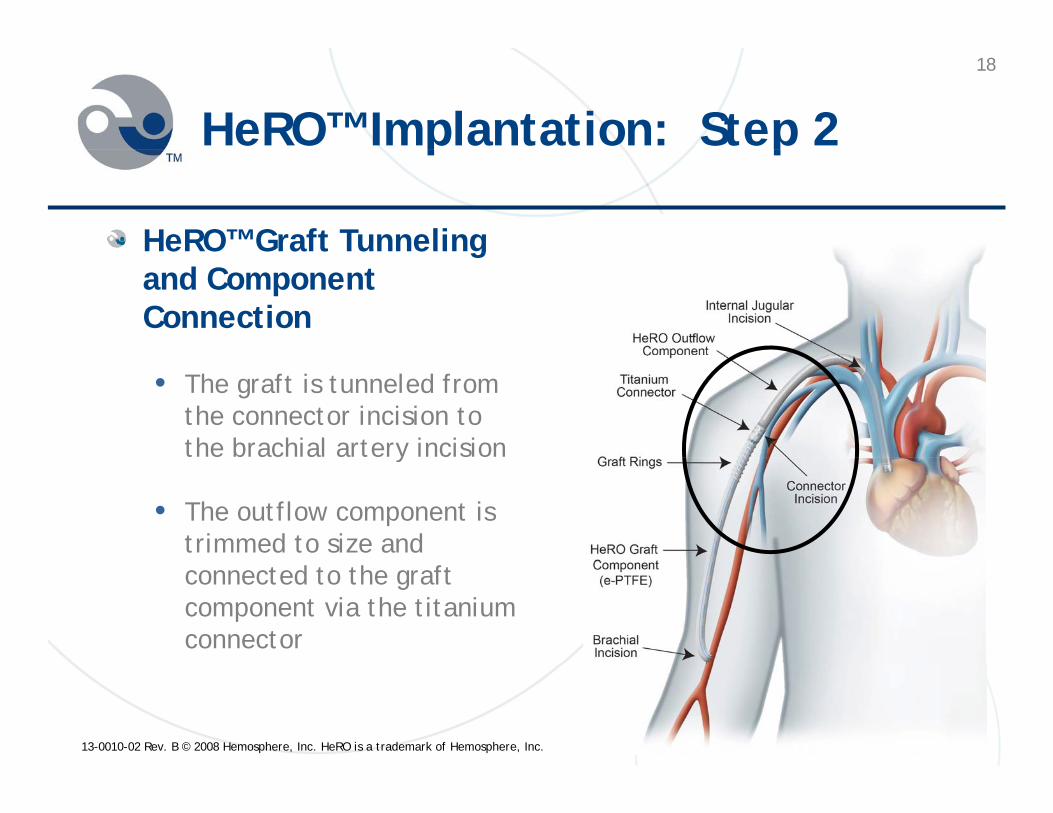
HeRO™ Graft Tunneling gand Component Connection
• The graft is tunneled from the connector incision to the brachial artery incision y
• The outflow component is trimmed to size and connected to the graft component via the titanium connector
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

19
HeRO™ Implantation: Step 3p p
Arterial Anastomosis
• The ePTFE graft component is trimmed to size and the arterial anastomosis is completed
A h d f h • At the end of the procedure, fluoroscopy is used to reconfirm proper outflow component tip outflow component tip placement and absence of kinking with arm movement
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
movement

20
HeRO™ Titanium Connector
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
21
HeRO™ Device Clinical Study
21
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
22
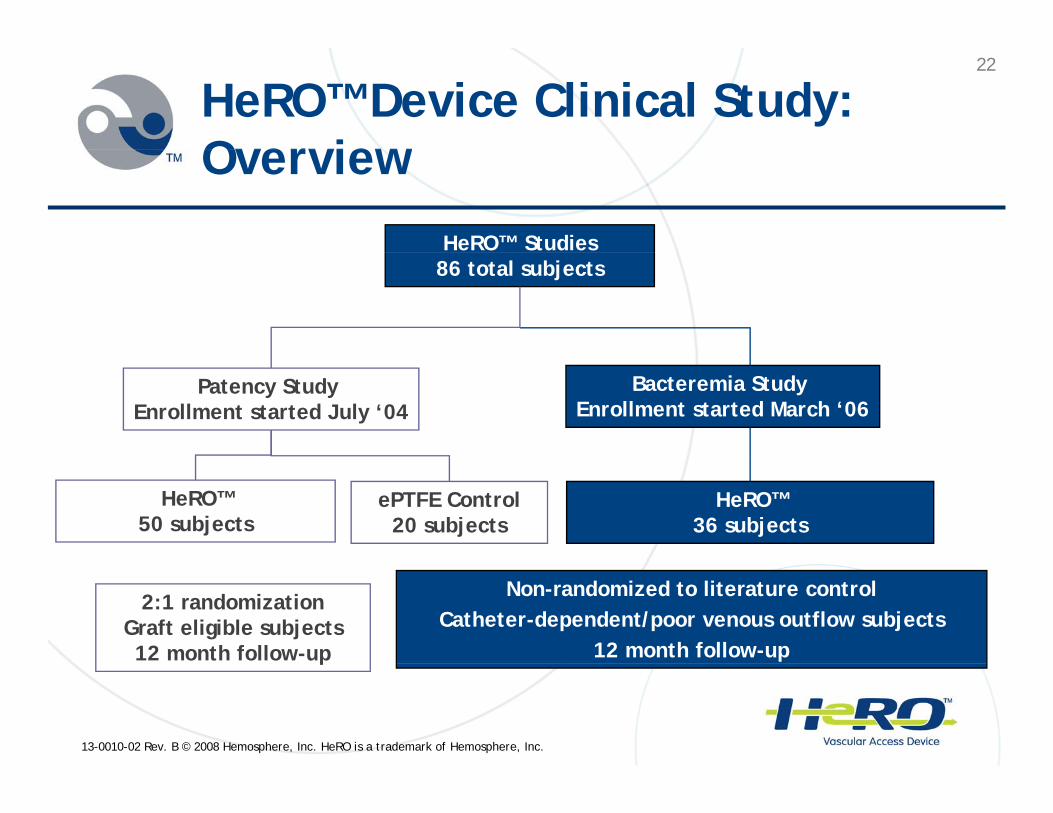
HeRO™ Device Clinical Study: OverviewOverview
HeRO™ Studies 86 total subjects
Bacteremia Study Enrollment started March ‘06
Patency Study Enrollment started July ‘04
HeRO™ 50 subjects
ePTFE Control20 subjects
HeRO™ 36 subjects
2:1 randomizationGraft eligible subjects12 month follow-up
Non-randomized to literature controlCatheter-dependent/poor venous outflow subjects
12 month follow-up
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
p
23
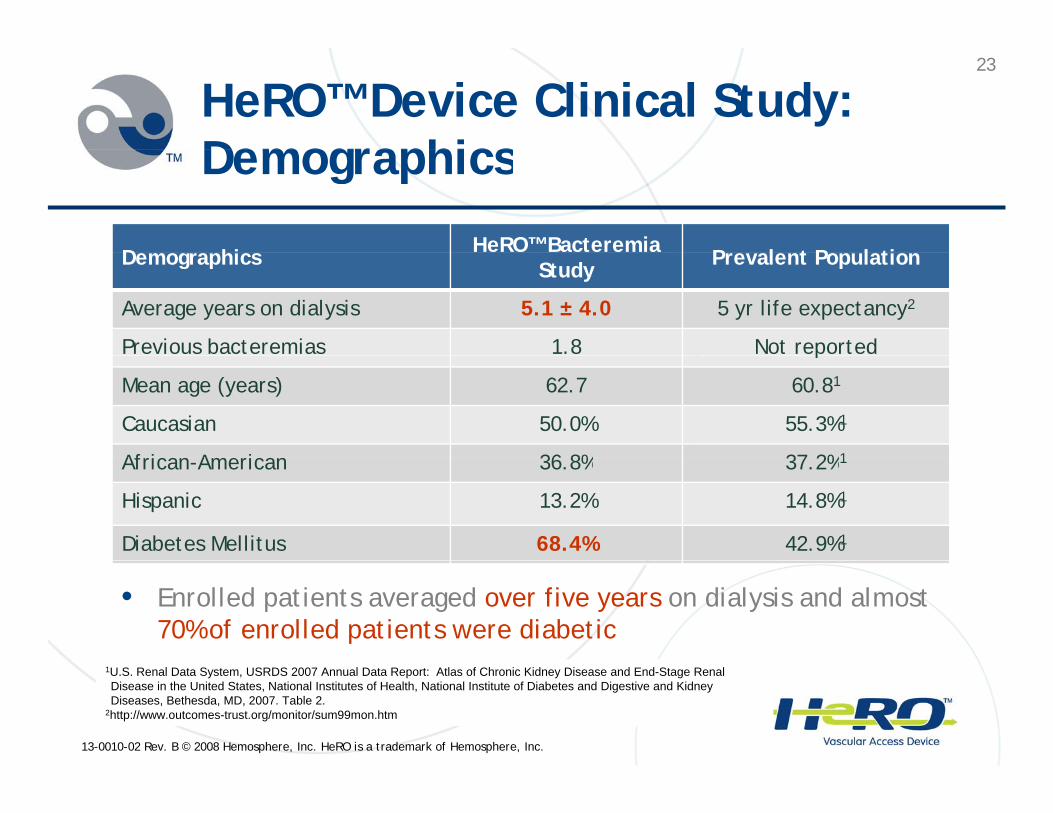
HeRO™ Device Clinical Study: DemographicsDemographics
D g hi HeRO™ Bacteremia P l t P l tiDemographics Study Prevalent Population
Average years on dialysis 5.1 ± 4.0 5 yr life expectancy2
Previous bacteremias 1.8 Not reportedp
Mean age (years) 62.7 60.81
Caucasian 50.0% 55.3%1
African American 36 8% 37 2%1African-American 36.8% 37.2%1
Hispanic 13.2% 14.8%1
Diabetes Mellitus 68.4% 42.9%1
• Enrolled patients averaged over five years on dialysis and almost 70% of enrolled patients were diabetic
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
1U.S. Renal Data System, USRDS 2007 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2007. Table 2.
2http://www.outcomes-trust.org/monitor/sum99mon.htm
24
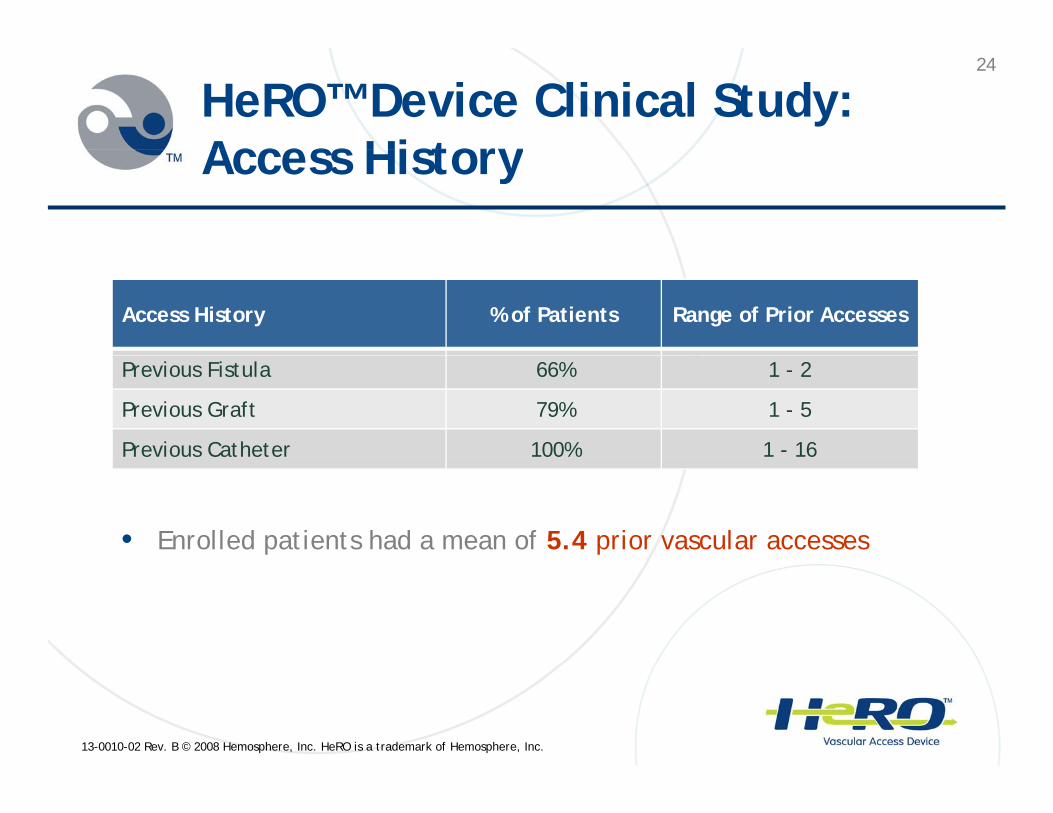
HeRO™ Device Clinical Study: Access HistoryAccess History
Access History % of Patients Range of Prior Accesses
Previous Fistula 66% 1 - 2
Previous Graft 79% 1 - 5
Previous Catheter 100% 1 - 16
• Enrolled patients had a mean of 5.4 prior vascular accesses
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

25
HeRO™ Device Clinical Study Results: 70% Reduction in Bacteremia Rates70% Reduction in Bacteremia Rates
A l d C h tHeRO™
B i HeRO™ Bacteremia Catheter LiteratureAnalyzed Cohorts BacteremiaEvents
HeRO BacteremiaRate/1,000 days
Catheter LiteratureControl/1,000 Days
HeRO™ w/Bridging TDC(1,373 days) 7 5.1 1.6 – 6.91
HeRO™ Alone(8,525 days) 0 0.0 2.34
HeRO™ Overall(9 931 d ) 7 0 7 2 32(9,931 days) 7 0.7 2.3
• 59% of patients with a bridging TDC had a femoral catheter
NO d i l t d b t i t t d ft b id i th t
1Combined bacteremia rate range for femoral and IJ TDCs; IJ TDC range from 2006 K/DOQI Guidelines and femoral TDC range from Lynch, L. Dialysis Catheter Literature Summary. 2007. Hemosphere, Inc. document
2Oliver M Lynch L Estimate of the Risk and Rate of Hemodialysis Catheter-Related Bacteremia 2006
• NO device-related bacteremia events were reported after bridging catheter was removed
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
Oliver, M., Lynch, L. Estimate of the Risk and Rate of Hemodialysis Catheter-Related Bacteremia. 2006. Hemosphere, Inc. document
26
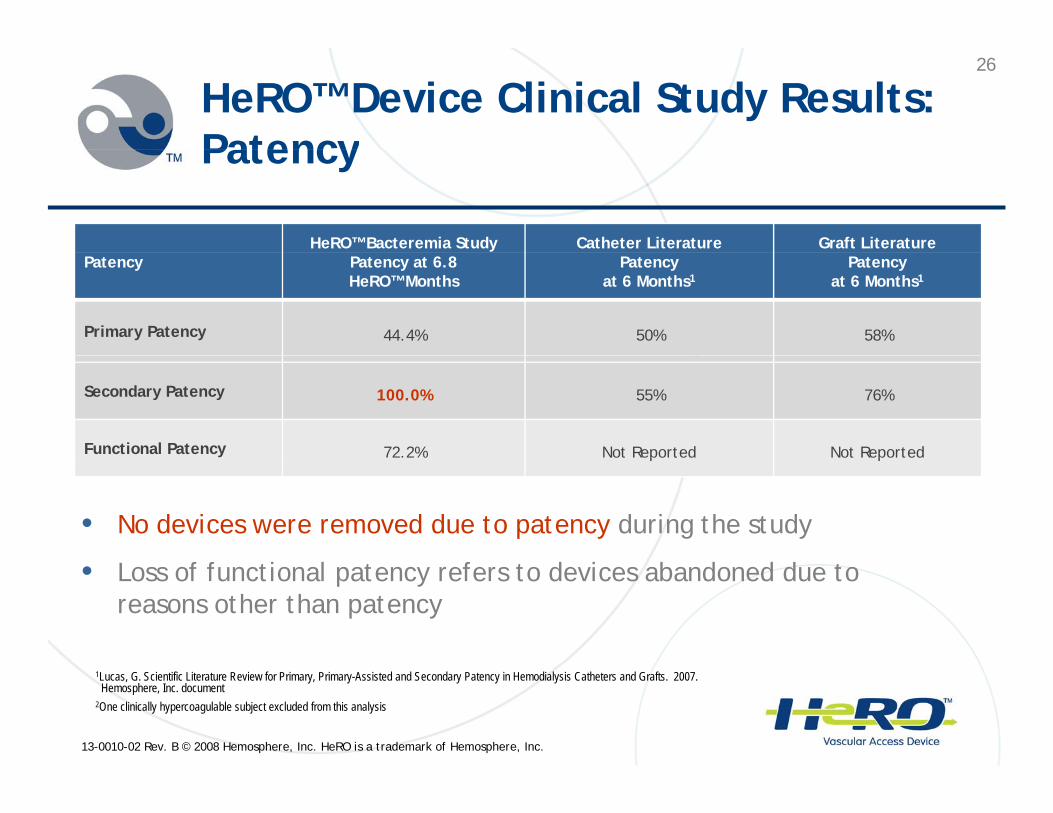
HeRO™ Device Clinical Study Results: PatencyPatency
HeRO™ Bacteremia Study Catheter Literature Graft LiteraturePatency Patency at 6.8
HeRO™ MonthsPatency
at 6 Months1Patency
at 6 Months1
Primary Patency 44.4% 50% 58%
Secondary Patency 100.0% 55% 76%
Functional Patency 72.2% Not Reported Not Reportedp p
• No devices were removed due to patency during the study
• Loss of functional patency refers to devices abandoned due to reasons other than patency
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
1Lucas, G. Scientific Literature Review for Primary, Primary-Assisted and Secondary Patency in Hemodialysis Catheters and Grafts. 2007. Hemosphere, Inc. document
2One clinically hypercoagulable subject excluded from this analysis
27
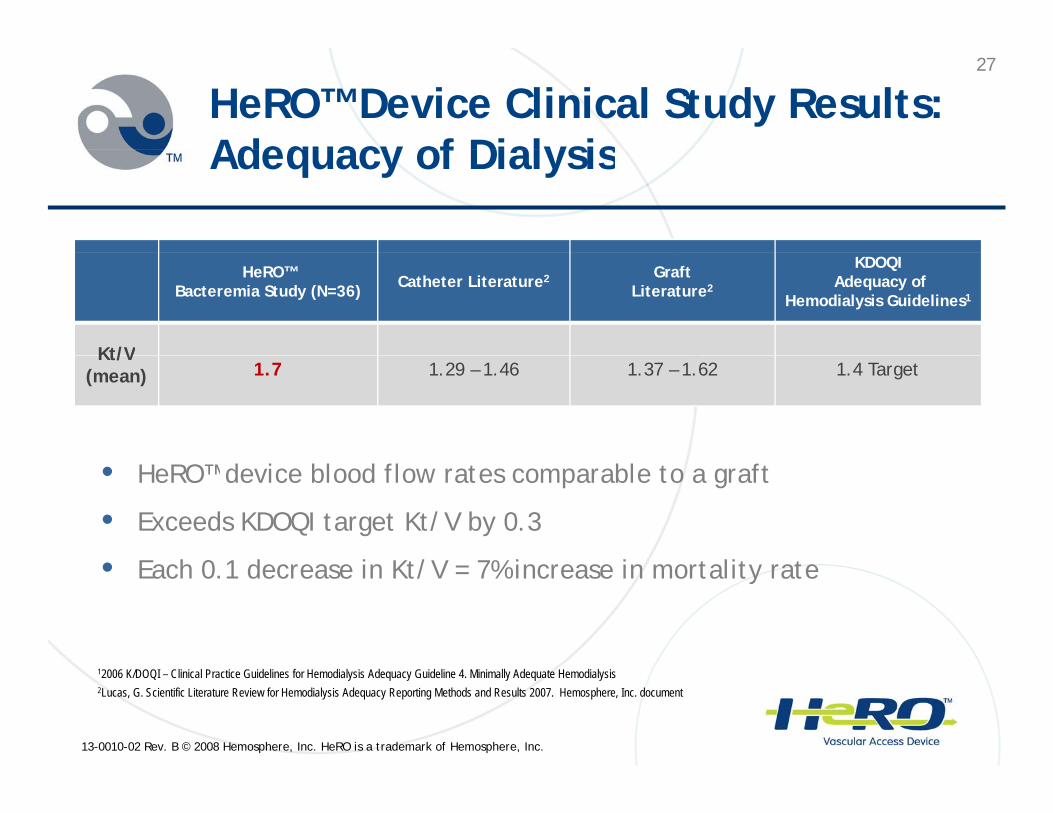
HeRO™ Device Clinical Study Results: Adequacy of DialysisAdequacy of Dialysis
HeRO™ Bacteremia Study (N=36) Catheter Literature2 Graft
Literature2
KDOQIAdequacy of
Hemodialysis Guidelines1
Kt/VKt/V(mean) 1.7 1.29 – 1.46 1.37 – 1.62 1.4 Target
• HeRO™ device blood flow rates comparable to a graft
• Exceeds KDOQI target Kt/V by 0.3
E h 0 1 d i K /V 7% i i li • Each 0.1 decrease in Kt/V = 7% increase in mortality rate
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
12006 K/DOQI – Clinical Practice Guidelines for Hemodialysis Adequacy Guideline 4. Minimally Adequate Hemodialysis2Lucas, G. Scientific Literature Review for Hemodialysis Adequacy Reporting Methods and Results 2007. Hemosphere, Inc. document
28
The HeRO™ Device Clinical Study: SSummary
Primary endpoint to reduce bacteremia was met!Primary endpoint to reduce bacteremia was met!
• 70% reduction in device/procedure-related bacteremia compared to catheter literature controlp
1.7 mean Kt/V exceeded the KDOQI target for adequate dialysis y
• Significantly improved vs. the catheter literature control
No devices were removed due to patency issuesNo devices were removed due to patency issues
• Although the HeRO™ device may require declot intervention similar to a graft
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
similar to a graft

29
Clinical Investigational Sites
I ti t Sit L ti
Clinical Investigational Sites
Investigators Sites Locations
Marc Glickman, MD (PI) Sentara Hospital Norfolk, VA
John Ross MD (PI) Bamberg County Hospital Bamberg SCJohn Ross, MD (PI) Bamberg County Hospital Bamberg, SC
Jeffrey Lawson, MD Duke University Medical Center Raleigh-Durham, NC
Howard Katzman, MD Univ. of Miami Hospital Miami, FL
Robert McLafferty, MD
Colleen Johnson, MDSouthern Illinois University Springfield, IL
Kevin Croston, MD North Memorial Medical Center Robbinsdale, MN
Jeffrey Martinez, MD Baptist Medical Center San Antonio, TX
Eric Peden, MD Baylor Medical Center Houston, TX
Joseph Zarge MD St Joseph’s Hospital Atlanta GA
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
Joseph Zarge, MD St. Joseph s Hospital Atlanta, GA
30
Recognizing HeRO™ Device Patients
30
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
31
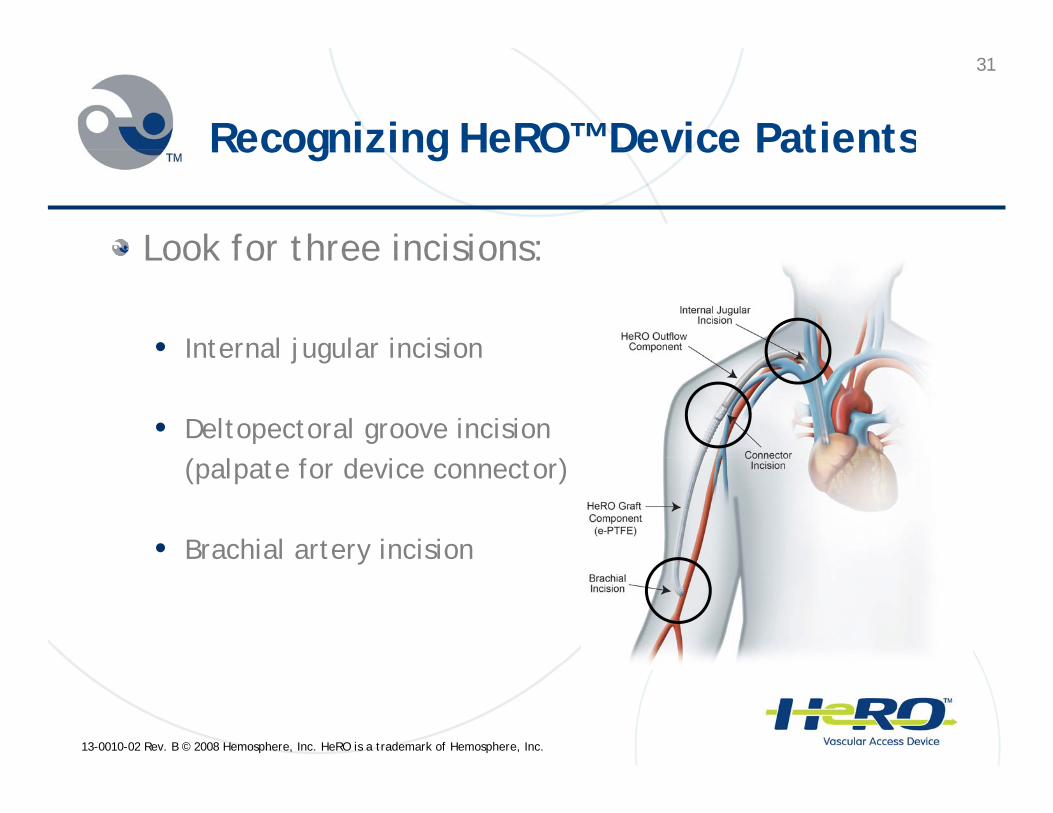
Recognizing HeRO™ Device PatientsRecognizing HeRO Device Patients
Look for three incisions:Look for three incisions:
• Internal jugular incisionInternal jugular incision
• Deltopectoral groove incision l f d(palpate for device connector)
• Brachial artery incisiony
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
32
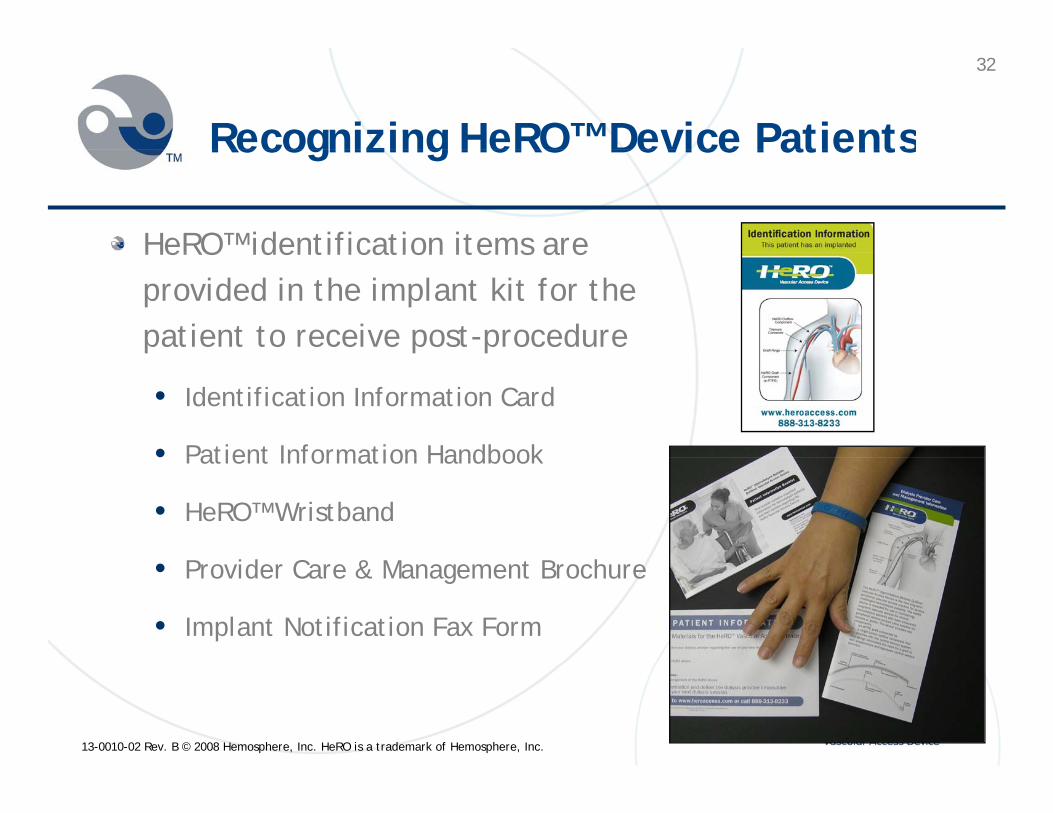
Recognizing HeRO™ Device PatientsRecognizing HeRO Device Patients
HeRO™ identification items are HeRO identification items are provided in the implant kit for the patient to receive post-procedure
• Identification Information Card
• Patient Information Handbook• Patient Information Handbook
• HeRO™ Wristband
P id C & M B h• Provider Care & Management Brochure
• Implant Notification Fax Form
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
33
HeRO™ Device Care & HeRO™ Device Care & Cannulation
33
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
34
AVG Physical Assessment:L k Li t & F lLook, Listen & Feel
LookLook• Uniform sized graft • No irregular areas or aneurysm formations• Organized cannulation site rotationOrganized cannulation site rotation
Listen• Low pitch continuous diastolic and systolic• HeRO™ bruit may be slightly softer due to absence HeRO bruit may be slightly softer due to absence
of venous anastomosis
Feel• Thrill and/or pulse strongest at the arterial Thrill and/or pulse strongest at the arterial
anastomosis, but should be felt over the course of the entire graft
• Easy to compress
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
• HeRO™ thrill may also be less prominent
35
HeRO™ Device CannulationHeRO Device Cannulation
Follow KDOQI Guidelines for cannulation:
• Wait until swelling has subsided so the course of the graft can be palpated (at least two weeks prior to first cannulation)
• Use standard fistula needles at a 45-degree angle• Use standard fistula needles at a 45-degree angle
• Rotate cannulation sites
• Stay 2-3 cm from the arterial anastomosisStay 2 3 cm from the arterial anastomosis
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

36
Techniques for AVG Cannulation
36
q
Technique RationaleTechnique Rationale
For routine AVGs:
• Advance the needle slowly with the beveled • Any manipulation may traumatize the vessel cutting edge up facing the top of the vessel
• Do not rotate the axis
intima
For deep, hard to palpate AVGs:
• Immediately rotate the axis of the needle 180o
• Advance needle slowly with the beveled
• Rotating the axis avoids traumatizing the top of the intima
• Prevents the needle tip from entering the backside of the graft materialy
cutting edge down facing the bottom of the vessel
• This should only be utilized when the graft back-wall location is difficult to determine and the risk of continuing needle advancement into the back-wall is high
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

37
AVG Cannulation Needle Handling
37
g
Technique Rationale
• Pressing the needle shaft flat against the skin moves the tip from the desired position within the vessel lumen• Tape the needle at the angle insertion
• Remove the needle at the angle of insertion
• Never apply pressure before the needle is
within the vessel lumen
• Any needle manipulation may traumatize the vessel intimaNever apply pressure before the needle is
completely removed
• Avoid pressing the cutting edge of the needle into the intima when applying pressure for hemodialysisy
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
38
Additional Considerations For H RO™ D i C l tiHeRO™ Device Cannulation
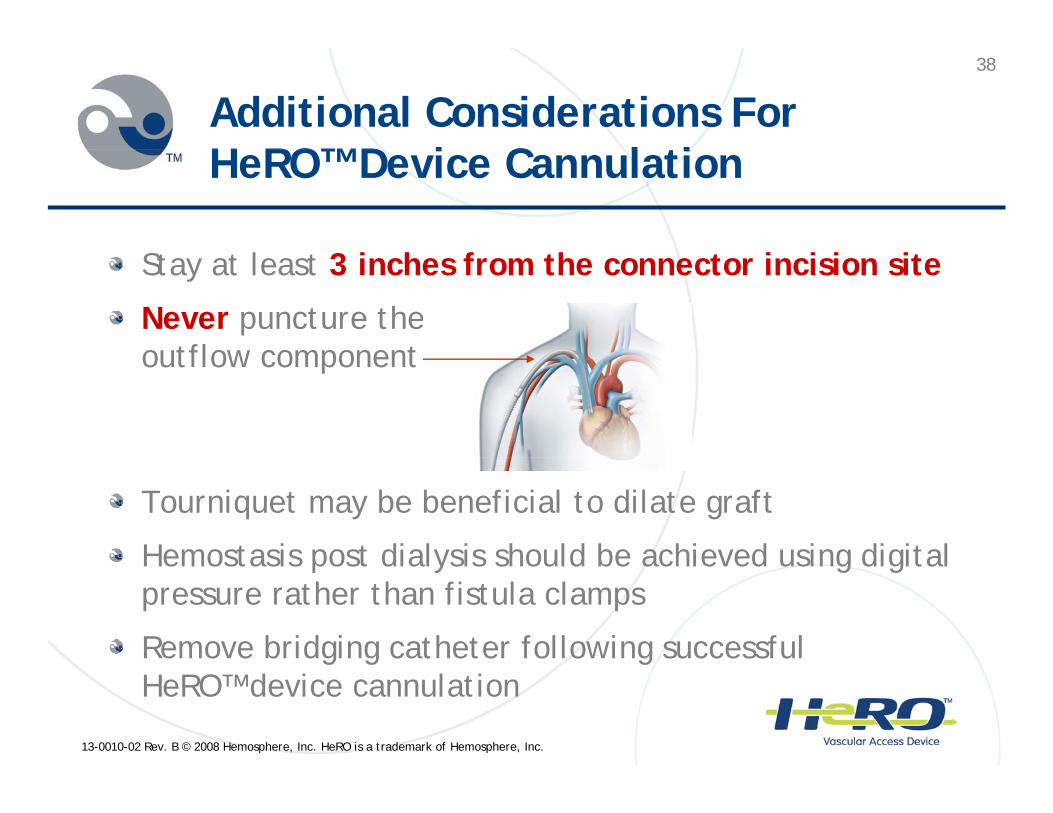
S l 3 i h f h i i i iStay at least 3 inches from the connector incision site
Never puncture the outflow componentoutflow component
Tourniquet may be beneficial to dilate graft
Hemostasis post dialysis should be achieved using digital Hemostasis post dialysis should be achieved using digital pressure rather than fistula clamps
Remove bridging catheter following successful
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
g g gHeRO™ device cannulation

39
HeRO™ Healthcare Economics
39
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
40
The Catheter Problem: Hi h C t t th H lth S t 1High Cost to the Healthcare System1
Bacteremia/septicemia is a significant complication Bacteremia/septicemia is a significant complication requiring hospital admission in hemodialysis patients
$23,451 is the mean cost of a catheter-related bacteremia hospitalization
• 17 day mean length of stay
• MRSA bacteremia associated with longer stays and higher costs
1Ramanathan V., Chiu, E.J., Thomas, J.T., Khan, A., Dolson, G.M., Darouicher, R.O. Healthcare Costs Associated with Hemodialysis
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
Catheter-Related Infections: A Single-Center Experience. Infection Control Hospital Epidemiology. 2007 May; 28(5):606-9.
41
Potential Healthcare Savingsg
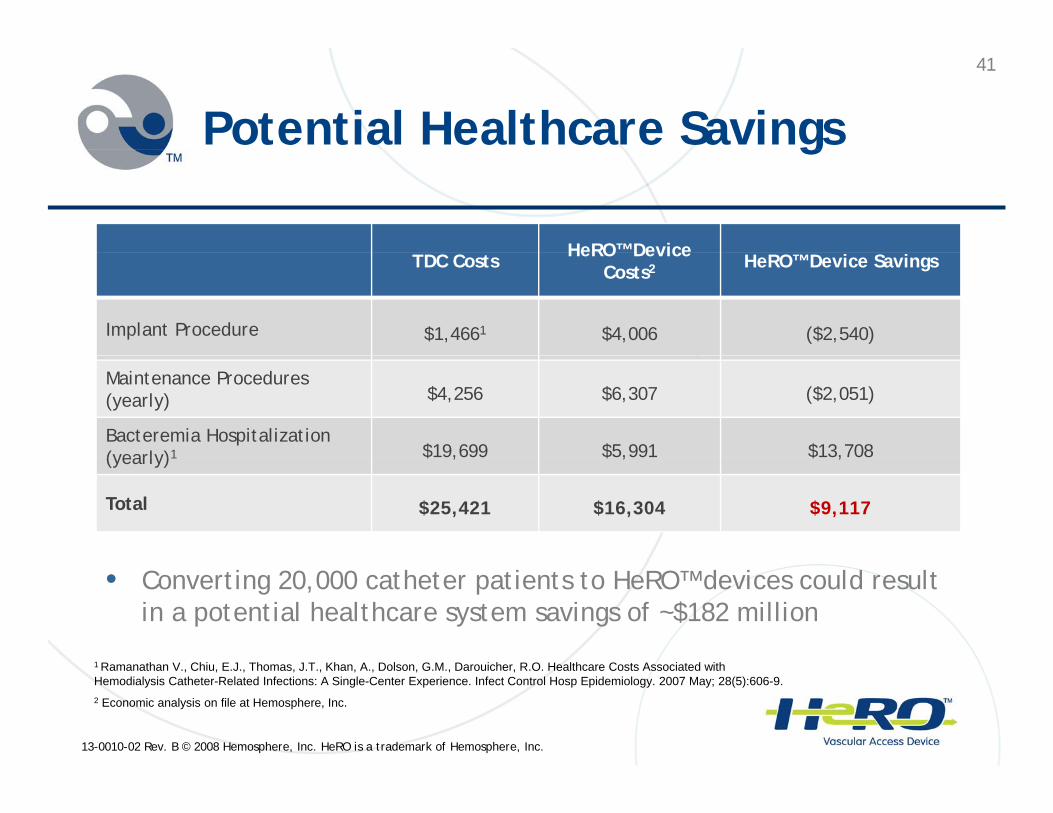
HeRO™ Device TDC Costs HeRO Device Costs2 HeRO™ Device Savings
Implant Procedure $1,4661 $4,006 ($2,540)
Maintenance Procedures (yearly) $4,256 $6,307 ($2,051)
Bacteremia Hospitalization (yearly)1 $19,699 $5,991 $13,708(yearly)1 $ , $ , $ ,
Total $25,421 $16,304 $9,117
1 R th V Chi E J Th J T Kh A D l G M D i h R O H lth C t A i t d ith
• Converting 20,000 catheter patients to HeRO™ devices could result in a potential healthcare system savings of ~$182 million
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
1 Ramanathan V., Chiu, E.J., Thomas, J.T., Khan, A., Dolson, G.M., Darouicher, R.O. Healthcare Costs Associated with Hemodialysis Catheter-Related Infections: A Single-Center Experience. Infect Control Hosp Epidemiology. 2007 May; 28(5):606-9.2 Economic analysis on file at Hemosphere, Inc.

42
Identifying HeRO™ Device Candidates
42
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
43
HeRO™ Device CandidatesHeRO Device Candidates
HeRO™ is ideally suited for the large and HeRO is ideally suited for the large and rapidly growing number of hemodialysis patients who are:p
• Catheter-dependent
A hi th t d d• Approaching catheter-dependency
• Failing an existing fistula or graft due to venous outflow obstruction or central venous stenosisoutflow obstruction or central venous stenosis
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

44
HeRO™ Candidate Selection Criteria HeRO Candidate Selection Criteria
Follow KDOQI guidelines for vessel mapping to evaluate Follow KDOQI guidelines for vessel mapping to evaluate patient qualifiers necessary for HeRO™ device placement
Necessary Patient Qualifiers:
> 3 mm brachial artery
Adequate cardiac function (ejection fraction > 20%)
Systolic BP > 100 mmHg
Infection free
Without ipsilateral PM/IADC
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
45
Introducing HeRO™ Into Your Access Programg
45
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

46
What Will HeRO™ Do For Your Patients d Y V l A P ? and Your Vascular Access Program?
Positively impact the overall health and quality of life Positively impact the overall health and quality of life for your access-challenged patients
• Significantly reduce catheter-related bacteremia
• Improve adequacy of dialysis over catheters
• Reduce complications experienced with a catheter
Lower your percentage of catheter-dependent patients
Simplify staffing patterns related to care of catheter p y g ppatients
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

47
What Happens Now?What Happens Now?
Review your current Review your current catheter-dependent patients to determine li ibilit
Access Coordinator/Hemodialysis
C t eligibility
Work with your HeRO™ representative to assist in
Coordinator/Nephrologist
Referral
Center Patients
representative to assist in educating the nephrologists and vascular surgeons
Vascular Access Surgeon
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

4848
Summary of HeRO™ Device MManagement
The HeRO™ device is the only long-term, peripheral AV access The HeRO device is the only long term, peripheral AV access
option for patients with venous outflow obstruction
Employ strict infection control procedures as per CDC dialysis Employ strict infection control procedures as per CDC dialysis
precautions to keep HeRO™ patients free from the risks of
infection
Keep in mind this patient population may require longer than 14
days for tissue to graft incorporation
Timely removal of the bridging TDC following successful HeRO™
device incorporation will likely decrease the risk of catheter-
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
related infections

49
The HeRO as I see it!The HeRO as I see it!
HeRO is not for everybody but it might be just the right HeRO is not for everybody but it might be just the right device for that patient who has:
• Good brachial flow
• Compromised venous outflow
• No other peripheral access options
AND …………………………………………………………
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.
50
R b Remember -It’s Always about what is best for the individualPatient!Patient!
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.

References and Resources
Dinwiddie, L.C. (2008). Vascular access for hemodialysis. In C.Dinwiddie, L.C. (2008). Vascular access for hemodialysis. In C. Counts (Ed.), Core Curriculum for Nephrology Nursing (5th ed). Pgs 735-764. ANNA, Pitman, NJ, PA.
National Kidney Foundation KDOQI Clinical Practice Guidelines forNational Kidney Foundation. KDOQI Clinical Practice Guidelines for Vascular Access: update 2006. (2006) American Journal of Kidney Diseases, 48(1), S176-S307.
Burrows Hudson S & Prowant B (2005) Nephrology nursingBurrows-Hudson S., & Prowant, B. (2005). Nephrology nursing standards of practice and guidelines for care. Pitman, NJ: American Nephrology Nurses Association.

52
Questions & AnswersQuestions & Answers
52
13-0010-02 Rev. B © 2008 Hemosphere, Inc. HeRO is a trademark of Hemosphere, Inc.