Embed Size (px)
Citation preview

Review article
The histopathology of grey matterdemyelination in multiple sclerosis
Introduction
Multiple sclerosis (MS) is a disease of the humancentral nervous system characterized by multifocalareas of demyelination, called MS lesions orplaques (1). MS lesions are macroscopically visiblein white matter (WM), leading to the previousdescription of MS as a WM disease. Already earlyMS pathology studies detected lesions also in greymatter (GM), however, when staining autopsytissue with histochemical stains for myelin (2–5). Inthe last few years, it has been recognized that GMdemyelination in MS is extensive and is similar inextent to the WM lesions (6–9). Studies usingquantitative magnetic resonance imaging (MRI)techniques indicate that GM MS pathology has asignificant impact on clinical symptoms and dis-ability in MS, and may occur independently ofWM pathology (10–18). GM lesions may contrib-ute to the so-called clinico-radiological paradox,the weak correlation between the extent of WMpathology by MRI and the extent of disability (19).MS in GM lesions may be important for cognitive
dysfunction in MS, which occurs in 40–60% of thepatients (20–23). MS GM pathology could alsolead to an increased risk of epileptic seizures;approximately 2% of MS patients have epilepsy(24–26). In this review, we will give an update onthe pathology of GM lesions in MS, with anemphasis on histopathological changes.
Extent and distribution of GM demyelination
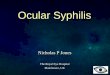
Purely cortical lesions are largely undetectable in aclinical setting, because of the low sensitivity ofconventional MRI techniques (3–5%) for purelyGM plaques, while the sensitivity for mixedGM ⁄WM lesions is higher (27). Extensive corticalpathology is not associated with increased focal ordiffuse WM pathology on MRI, indicating that theextent or distribution of WM abnormalities cannotbe used to identify patients with extensive GMdemyelination (Fig. 1) (28). Sensitivity for corticallesions is improved by novel techniques, such asthree-dimensional double inversion recovery(3D-DIR), and a T1-weigthed 3D spoiled gradi-
Acta Neurol Scand 2009: 120 (Suppl. 189): 51–57 � 2009 John Wiley & Sons A ⁄ SACTA NEUROLOGICA
SCANDINAVICA
Bø L. The histopathology of grey matter demyelination in multiplesclerosis.Acta Neurol Scand 2009: 120 (Suppl. 189): 51–57.� 2009 John Wiley & Sons A ⁄S.
Multiple sclerosis (MS) is characterized by focal demyelinating lesionsin white matter (WM) and grey matter (GM) of the central nervoussystem. Results of studies using quantitative magnetic resonanceimaging techniques indicate that GM MS pathology has a significantimpact on clinical symptoms and disability in MS, and may occurpartly independently of WM pathology. Subpial cerebral andcerebellar cortexes are predilection sites for demyelination in MS.Significant neuronal and axonal pathology has been detected in GMMS lesions. The pathology of MS lesions is location-dependent; thereis less pronounced inflammation in GM lesion areas than in WMlesions. The presence and extent of GM lesions has recently beencorrelated to meningeal inflammation, and cells infected with theEpstein–Barr virus have been detected in meningeal infiltrates,suggesting a role of meningeal inflammation in cortical lesionpathogenesis.
L. BøNational Competence Center for Multiple Sclerosis,Department of Neurology, Haukeland UniversityHospital, Bergen, Norway, and Department of ClinicalMedicine, University of Bergen, Bergen, Norway
Key words: cerebral cortex; grey matter; multiplesclerosispathology
Lars Bø, National Competence Center for MultipleSclerosis, Department of Neurology, HaukelandUniversity Hospital, N-5021 Bergen, NorwayTel.: +47 559 75045 ⁄ 5044Fax: +47 559 75901e-mail: [email protected]
Conflicts of interest: The author declares no conflicts ofinterest.
51

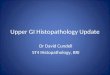
ent-recalled-echo sequence (29, 30). Extensive sub-pial demyelination, which is the most commonlesion pattern in chronic MS, has not beendescribed in MRI studies. However, this indicatesthat the majority of these lesions are not detectedeven with advanced MRI techniques. Also histo-chemical staining methods for cortical myelin andcortical demyelination have a low sensitivity forsuperficial layers of cortical myelin, which mayexplain why the extent of subpial demyelination inMS was not fully appreciated earlier (Fig. 2) (6).Histochemical studies found that the majority ofcortical MS lesions were located at the GM ⁄WMborder. Brownell and Hughes (31) found that 26%of the lesions affected GM in a material of 22 MSpatients and 77% of the cortical lesions involvedsubcortical WM. Kidd et al. (32) detected 478cortical lesions in a material of 2–6 coronalsections from 12 MS brains and 76% of the lesionsinvolved subcortical WM. In later immunohisto-chemical studies, purely cortical lesions have beenshown to represent the majority of the cortical
demyelinated area, with subpial lesions being themost frequent lesion type (6, 8, 9). In an autopsymaterial from 20 patients with chronic MS, 84% ofthe cortical lesions were purely cortical, accountingfor 86% of the cortical demyelinated area. Themean proportion of the GM demyelinated areawas 25%, while the mean percentage demyelina-tion in WM in the same tissue block was 5% (6). Ina study of large coronal sections of the brain of sixMS patients, more than 90% of the lesions wererestricted to the superficial layers of the cerebralcortex. A mean of 14.8% of the cerebral cortex wasdemyelinated and 21.8% of the WM was demye-linated (9). In a study of 14 MS cases, 96% ofcortical lesions were restricted to the cerebralcortex (7).There is significant regional variation in the
extent of GM demyelination. In different studies,the most extensive cortical demyelination has beendetected in the cingulate gyrus (17%–44%), andtemporal and frontal cortexes (17–28%) with alower proportion of demyelinated area in other
A
C
B
D
Figure 1. Paraffin sections immunohistochemically stained with antiproteolipid protein antibody (A and C) and correspondingT2-weighted magnetic resonance (MR) images from a patient with extensive cortical subpial demyelination (A and B) and from apatient with a low extent of cortical demyelination (C and D). Demyelinated cortical areas are visible by immunohistochemistry(A and C, blue outline) but not by MR imaging (B and D). Sparse white matter demyelination is detected in both patients (A and C,red outline) and is detectable by MR imaging (B and D, arrows). Source: With permission from Archives of Neurology 2007;64:76–80.
Bø
52

cortical areas studied, including the paracentrallobule (11.5%), occipital lobe (8%) and primarymotor cortex (3.5%) (6, 7, 9, 33). In two studies,23–25% of the patients had a pattern of subpialdemyelination in all cortical regions studied. Thispattern of demyelination, termed �general subpialdemyelination� may represent the extreme end of aspectrum of cortical demyelination (Fig. 2) (6, 33).The percentage of demyelinated area is very high inthe cerebellar cortex of MS patients with progres-sive disease (39–44%). This may be a cause of
cerebellar dysfunction in MS (7, 34). In thecerebellum, approximately half of the corticallesions are purely cortical (7). Episodic memory isfrequently affected in MS, which could be due inpart to hippocampal MS pathology (35). Extensivedemyelination has been detected in the hippo-campus of MS patients (36, 37). In a study ofhippocampi from 45 progressive MS cases, themean percentage hippocampal demyelinated areawas 30.4% (37).In the spinal cord, the percentage of demyeli-
nated area in GM (33%) was significantly higherthan the percentage of demyelinated area in WM(20%) (38). The extent of GM demyelination wassimilar in all cord levels; the majority of spinal cordlesions were combined WM ⁄GM lesions (38).Extent of cortical demyelination in the cerebel-
lum and cerebrum, and in different cerebralcortical regions is significantly correlated, suggest-ing a common pathogenesis (6–8). In severalstudies, extent of cerebral GM and WM demye-lination was not correlated or weakly correlated,indicating that GM demyelination may occur atleast partly independent of demyelination in theWM in the brain (6, 8, 9). In one study, corticaldemyelination was largely restricted to progressiveforms of MS (8). In another study, however,extensive cortical demyelination was detected alsoin early lesion stages (39). Remyelination isfrequently detected in WM MS lesions and isalso observed in the GM. In a direct comparisonof remyelination of WM and GM MS lesions ofthe same patients, GM remyelination was consis-tently more extensive (33).Cortical demyelinated lesions are not specific for
MS, intracortical and leucocortical lesions werealso detected in progressive multifocal leucoence-phalopathy (PML). Subpial lesions were notobserved in PML, however (40).
Lesion classification
A classification system of cortical lesions has beenused based on lesion location: (i) combinedWM ⁄GM lesions; (ii) lesions entirely within thecerebral cortex, not making contact with subcor-tical WM or pia mater and (iii) subpial lesions (41).In some studies, an additional lesion category,type 4, is used, which are lesions that extend to theentire width of the cortex without entering thesubcortical WM (6, 42). The largest lesions aretype 3 or 4, which may extend as large sheaths overseveral gyri or the whole brain. Type 2 lesions arein general small and perivascular (6). Spinal cordlesions may also be classified into purely GMlesions and combined WM ⁄GM lesions (38). In
WM
CTX
WM
CTX
WM
CTX
WM
CTX
WM
CTX
WM
CTX
A
B
Figure 2. Adjacent paraffin sections from a multiple sclerosis(MS) patient with general cortical subpial demyelinationhistochemically stained for myelin using the Luxol fast blue(LFB) technique (A) and immunohistochemically stained forproteolipid protein (PLP) (B). With LFB staining, demyelina-tion of periventricular white matter (WM), including thecorpus callosum, is readily detectable (A, white arrows). Cor-tical myelin is largely unstained (A, black arrows). Periven-tricular lesions are also well delineated by PLPimmunohistochemistry (B, white arrows). In cerebral cortex(CTX), all areas have a superficial subpial loss of myelin (B,black arrows); an area of myelin loss is also detected in theputamen (B, arrowhead). At higher magnification, a sharplydefined cortical lesion border is visible by PLP immunohisto-chemistry (B, inset, black arrow); the border is not detectableby LFB staining in an adjacent section (A, inset, black arrow).Source: With permission from Archives of Neurology2007;64:76–80.
Histopathology of grey matter demyelination in MS
53

general, purely cortical lesions may not be classi-fied on the basis of inflammatory activity or thepresence of myelin proteins within macrophagesbecause of the very low extent of inflammation inthese lesions, and because of technical difficulties indetecting the much lower amount of phagocytosedmyelin within the macrophages (42). In type 1lesions, the WM part of the lesion has been used toclassify the age and demyelinating activity of theGM part of the lesion (41).
Pathology of GM lesions
The pathology of GM MS lesions is similar to thatof WM lesions in that there are well-demarcatedareas of demyelination, oligodendrocyte andaxonal loss (33, 41). In several other aspects, MSlesion pathology is location-dependent.In purely cortical lesions with leucocytes, there
is a very low extent of inflammation (9, 32, 41–43). Perivascular infiltrates are rare; the density ofinfiltrating lymphocytes was not increased inpurely cortical lesions when compared with thenormal control GM or normal-appearing GM inMS patients. This was also the case when com-paring lymphocyte subsets (CD4, CD8, CD20)(42). In the cortical part of type 1 lesions thedensity of the infiltrating lymphocytes is interme-diate between that of the WM lesions and in thecontrol cortex (41, 42). Extent of lymphocyteinfiltration in cortical lesions may depend onpatient population, as lymphocyte infiltration hasbeen reported in purely cortical lesions of biop-sied MS patients (44). This may signify either thatthe pathogenesis of cortical demyelination isdifferent in the subgroup of MS patients that isbiopsied, or that cortical inflammation is transientand therefore rarely observed in chronic MSpatients. In purely GM lesions, the majority ofphagocytic cells have the morphology of activatedmicroglia, with a minority having a phagocyticmacrophage appearance (41). Activated microgliawithin cortical lesions contain elevated levels ofmyeloperoxidase, indicating that reactive oxygenspecies may contribute to GM lesion pathogenesis(45).In purely GM MS lesions, no significant leakage
of plasma proteins into brain parenchyma wasdetected, suggesting a patent blood–brain barrier(46). Purely GM lesions contained occasionaldeposits of C4d on myelin and oligodendrocytes.Apart from this, there were no significant signs ofcomplement activation (47). The pathogenesis ofGM demyelination may be studied in the animalmodels of experimental autoimmune encephalo-myelitis (EAE) and in the cuprizone model (48–52).
In the EAE model in rat, the extent of corticaldemyelination was dependent on major histo-compatibility complex haplotypes (51). In thecuprizone model, cortical demyelination was veryextensive and complete demyelination was detectedat the disease peak (49).
Neuronal pathology
A significant increase of TUNEL-positive apopto-tic neurons have been detected in cortical lesions.The majority of apoptotic neurons were largepyramidal cells in cortical layers 3 and 5 (41). Incortical lesion areas, immunopositivity for non-phosphorylated neurofilament was decreased (41),and immunopositivity for phosphorylated proteinwas increased in cortical neurons (45). Specificsubpopulations of neurons are vulnerable in MS;in primary motor cortex, parvalbumin interneu-rons within layer 2 were significantly reduced, withno concurrent change in the number of calretinin-positive neurons (53). The extent of neuronal lossseems to vary depending on the lesion location andpossibly patient population. Neuronal numbers inthe hippocampus of MS patients were decreased by27–30% (37). In the cerebral cortex of patientswith extensive cortical demyelination, 18–23% ofthe neurons were lost, while in patients with alower extent of cortical demyelination the extent ofneuronal loss was lower (9). In patients withcombined WM ⁄GM lesions in the frontal lobe,the density of neurons within the GM part of thelesions was reduced by approximately 10% whencompared with the adjacent normal-appearing MSneocortex. The synaptic density was substantiallyreduced within lesions and the mean synaptophysinsignal was reduced by 47% (54). In the thalamus,the proportion of neurons lost was calculated to be35% based on cell density and atrophy measure-ments (55). In cervical and thoracic GM in thespinal cord, 24% and 30% of the neurons werelost, respectively, while no significant neuronal losswas detected in lumbar spinal cord (56). In thelateral geniculate nucleus, the extent of pathologyin parvocellular neurons correlated with the extentof axonal loss, suggesting that neuronal damagemay occur secondary to axonal damage (57).Neurons within cortical lesions containedincreased levels of matrix metalloproteinase 9,which may mediate pathology of the corticalextracellular matrix, manifesting as a decrease inthe number of cortical perineuronal nets (58).Neuronal pathology in MS lesions is not restrictedto demyelinated lesions. In non-demyelinated MS,neocortex gene expression was reduced for 26nuclear-encoded mitochondrial genes. The reduc-
Bø
54

tion of mitochondrial mRNA was demonstrated tooccur predominantly in neurons (59). Chronicinsults in MS cortex may activate protectivemechanisms. Both ciliary neurotrophic factor(CNTF) and CNTF–receptor complex memberswere increased in the MS cortex. CNTF wasincreased and also expressed by neurons, suggest-ing that the pathogenesis of MS in cerebral cortexelicits neuroprotective signalling pathways (59).
Meningeal inflammation
The leptomeninges of MS patients is known tocontain inflammatory infiltrates (60). Ectopic B-cellfollicles are present in the meninges of a proportionof secondary progressive MS (SPMS) patients. Thiswas detected in 41% of the SPMS cases, but not inprimary progressive MS (PPMS) cases (43, 61). Thepresence of ectopic B-cell follicles correlated signif-icantly with the extent of GM demyelination, butnot with that of WM demyelination (43). Allectopic B-cell follicles were found adjacent to thesubpial cortical lesions, suggesting a role for men-ingeal B-cell follicles in the pathogenesis of subpialdemyelination. The number of neurofilament–pro-tein immunopositive neurites was significantlylower in follicle-positive cases, when comparedwith the MS cases without B-cell follicles. Follicle-positive cases had a more rapid disease progressionwith an earlier onset of irreversible disability anddeath (43). B cells and plasma cells in meningealinfiltrates and ectopic follicles were enriched formarkers of Epstein–Barr virus (EBV) infection inMS, but not in other central nervous systeminflammatory disease, indicating a role of EBVinfection in cortical lesion pathogenesis (62). Cor-tical demyelination may be mediated throughmechanisms of bystander demyelination, as acti-vated CD8+ T cells with signs of cytotoxicreactivity to plasma cells were detected in MSbrain, and were correlated to the number of EBV-infected cells, both in WM and meninges (62).
Conclusion
The use of immunohistochemical methods todetect cortical myelin has recognized that corticaland other GM demyelination is extensive in MS.The results of MRI studies indicate that corticaldemyelination contributes significantly to disabil-ity in MS. The pathology of GM MS lesionsdiffers from that of the WM lesions in severalimportant aspects. Information about location-dependent and -independent features of MSpathology may thus give important informationabout the pathogenesis of MS. Recent studies have
indicated an important role of meningeal inflam-mation and EBV infection in cortical lesionpathogenesis and possibly MS immunopathologyin general.
References
1. Holmøy T. Immunopathogenesis of multiple sclerosis:concepts and controversies. Acta Neurol Scand Suppl2007;187:39–45.
2. Dawson JW. The histology of disseminated sclerosis. TransR Soc Edin 1916;L:517–774.
3. Dinkler M. Zur Kasuistik der multiplen Herdsklerose desGehirns und Ruckenmarks. Deuts Zeits f Nervenheilk1904;26:233–47.
4. Sander M. Hirnrindenbefunde bei multipler Sklerose.Monatschrift fur Psychiatrie und Neurologie 1898;IV:427–36.
5. Schob F. Ein Beitrag zur patologischen Anatomie dermultiplen Sklerose. Monatschrift fur Psychiatrie undNeurologie 1907;22:62–87.
6. Bø L, Vedeler CA, Nyland HI, Trapp BD, Mørk SJ.Subpial demyelination in the cerebral cortex of multiplesclerosis patients. J Neuropathol Exp Neurol 2003;62:723–32.
7. Gilmore CP, Donaldson I, Bø L, Owens T, Lowe JS,Evangelou N. Regional variations in the extent and patternof grey matter demyelination in multiple sclerosis: a com-parison between the cerebral cortex, cerebellar cortex, deepgrey matter nuclei and the spinal cord. J Neurol NeurosurgPsychiatry 2008;80:182–7.
8. Kutzelnigg A, Lucchinetti CF, Stadelmann C et al. Corti-cal demyelination and diffuse white matter injury inmultiple sclerosis. Brain 2005;128:2705–12.
9. Vercellino M, Plano F, Votta B, Mutani R, Giordana MT,Cavalla P. Grey matter pathology in multiple sclerosis.J Neuropathol Exp Neurol 2005;64:1101–07.
10. Agosta F, Rovaris M, Pagani E, Sormani MP, Comi G,Filippi M. Magnetization transfer MRI metrics predict theaccumulation of disability 8 years later in patients withmultiple sclerosis. Brain 2006;129:2620–7.
11. Oreja-Guevara C, Charil A, Caputo D, Cavarretta R,Sormani MP, Filippi M. Magnetization transfer magneticresonance imaging and clinical changes in patients withrelapsing–remitting multiple sclerosis. Arch Neurol2006;63:736–40.
12. Khaleeli Z, Cercignani M, Audoin B, Ciccarelli O, Miller
DH, Thompson AJ. Localized grey matter damage in earlyprimary progressive multiple sclerosis contributes to dis-ability. Neuroimage 2007;37:253–61.
13. Rovaris M, Judica E, Gallo A et al. Grey matter damagepredicts the evolution of primary progressive multiplesclerosis at 5 years. Brain 2006;129:2628–34.
14. Vrenken H, Geurts JJ, Knol DL et al. Whole-brain T1mapping in multiple sclerosis: global changes of normal-appearing gray and white matter. Radiology 2006;240:811–20.
15. Vrenken H, Pouwels PJ, Geurts JJ et al. Altered diffusiontensor in multiple sclerosis normal-appearing brain tissue:cortical diffusion changes seem related to clinical deterio-ration. J Magn Reson Imaging 2006;23:628–36.
16. Charil A, Dagher A, Lerch JP, Zijdenbos AP, Worsley KJ,Evans AC. Focal cortical atrophy in multiple sclerosis:relation to lesion load and disability. Neuroimage2007;34:509–17.
Histopathology of grey matter demyelination in MS
55

17. Bakshi R, Benedict RH, Bermel RA et al. T2 hypointensityin the deep gray matter of patients with multiple sclerosis:a quantitative magnetic resonance imaging study. ArchNeurol 2002;59:62–8.
18. Pulizzi A, Rovaris M, Judica E et al. Determinants ofdisability in multiple sclerosis at various disease stages: amultiparametric magnetic resonance study. Arch Neurol2007;64:1163–8.
19. Barkhof F. The clinico-radilogical paradox in multiplesclerosis revisited. Curr Opin Neurol 2003;15:239–45.
20. Amato MP, Bartolozzi ML, Zipoli V et al. Neocorticalvolume decrease in relapsing–remitting MS patients withmild cognitive impairment. Neurology 2004;63:89–93.
21. Sanfilipo MP, Benedict RH, Weinstock-Guttman B, Bakshi
R. Gray and white matter brain atrophy and neuro-psychological impairment in multiple sclerosis. Neurology2006;66:685–92.
22. Lazeron RH, Langdon DW, Filippi M et al. Neuro-psychological impairment in multiple sclerosis patients: therole of (juxta)cortical lesion on FLAIR. Mult Scler2000;6:280–5.
23. Hoffmann S, Tittgemeyer M, Von Cramon DY. Cognitiveimpairment in multiple sclerosis. Curr Opin Neurol2007;20:275–80.
24. Moreau T, Sochurkova D, Lemesle M et al. Epilepsy inpatients with multiple sclerosis: radiological–clinical cor-relations. Epilepsia 1998;39:893–6.
25. Calabrese M, De SN, Atzori M et al. Extensive corticalinflammation is associated with epilepsy in multiplesclerosis. J Neurol 2008;255:581–6.
26. Engelsen BA, Gronning M. Epileptic seizures in patientswith multiple sclerosis. Is the prognosis of epilepsyunderestimated? Seizure 1997;6:377–82.
27. Geurts JJ, Bø L, Pouwels PJ, Castelijns JA, Polman CH,Barkhof F. Cortical lesions in multiple sclerosis: combinedpostmortem MR imaging and histopathology. AJNR AmJ Neuroradiol 2005;26:572–7.
28. Bø L, Geurts JJ, Van DV, Polman C, Barkhof F. Lack ofcorrelation between cortical demyelination and whitematter pathologic changes in multiple sclerosis. ArchNeurol 2007;64:76–80.
29. Bagnato F, Butman JA, Gupta S et al. In vivo detectionof cortical plaques by MR imaging in patients withmultiple sclerosis. AJNR Am J Neuroradiol 2006;27:2161–7.
30. Geurts JJ, Pouwels PJ, Uitdehaag BM, Polman CH,Barkhof F, Castelijns JA. Intracortical lesions in multiplesclerosis: improved detection with 3D double inversion-recovery MR imaging. Radiology 2005;236:254–60.
31. Brownell B, Hughes JT. The distribution of plaques in thecerebrum in multiple sclerosis. J Neurol NeurosurgPsychiatry 1962;25:315–21.
32. Kidd D, Barkhof F, Mcconnell R, Algra PR, Allen IV,Revesz T. Cortical lesions in multiple sclerosis. Brain1999;122(Pt 1):17–26.
33. Albert M, Antel J, Bruck W, Stadelmann C. Extensivecortical remyelination in patients with chronic multiplesclerosis. Brain Pathol 2007;17:129–38.
34. Kutzelnigg A, Faber-Rod JC, Bauer J et al. Widespreaddemyelination in the cerebellar cortex in multiple sclerosis.Brain Pathol 2007;17:38–44.
35. Benedict RH, Ramasamy D, Munschauer F, Weinstock-Guttman B, Zivadinov R. Memory impairment in multiplesclerosis: correlation with deep grey matter and mesialtemporal atrophy. J Neurol Neurosurg Psychiatry2009;80:201–6.
36. Geurts JJ, Bø L, Roosendaal SD et al. Extensive hippo-campal demyelination in multiple sclerosis. J NeuropatholExp Neurol 2007;66:819–27.
37. Papadopoulos D, Dukes S, Patel R, Nicholas R, Vora A,Reynolds R. Substantial archaeocortical atrophy andneuronal loss in multiple sclerosis. Brain Pathol2009;19:238–53.
38. GilmoreCP,BøL,OwensT,Lowe J, EsiriMM,EvangelouN.Spinal cord graymatter demyelination inmultiple sclerosis –a novel pattern of residual plaquemorphology. Brain Pathol2006;16:202–8.
39. Roemer S, Stadelmann C, Bruck W, Morales Y, Parisi JE,Lucchinetti CF. Cortical demyelination is present in earlymultiple sclerosis. Neurology 2009;66:A93–4.
40. Moll NM, Rietsch AM, Ransohoff AJ et al. Corticaldemyelination in PML and MS: similarities and differ-ences. Neurology 2008;70:336–43.
41. Peterson JW, Bø L, Mork SJ, Chang A, Trapp BD.Transected neurites, apoptotic neurons, and reducedinflammation in cortical multiple sclerosis lesions. AnnNeurol 2001;50:389–400.
42. Bø L, Vedeler CA, Nyland H, Trapp BD, Mork SJ. In-tracortical multiple sclerosis lesions are not associated withincreased lymphocyte infiltration. Mult Scler 2003;9:323–31.
43. Magliozzi R, Howell O, Vora A et al. Meningeal B-cellfollicles in secondary progressive multiple sclerosis associ-ate with early onset of disease and severe cortical pathol-ogy. Brain 2007;130:1089–1104.
44. Pirko I, Lucchinetti CF, Sriram S, Bakshi R. Gray matterinvolvement in multiple sclerosis. Neurology 2007;68:634–42.
45. Gray E, Thomas TL, Betmouni S, Scolding N, Love S.Elevated activity and microglial expression of myeloper-oxidase in demyelinated cerebral cortex in multiplesclerosis. Brain Pathol 2008;18:86–95.
46. Van Horssen J, Brink BP, De Vries HE, Van DV, Bø L. Theblood–brain barrier in cortical multiple sclerosis lesions.J Neuropathol Exp Neurol 2007;66:321–8.
47. Brink BP, Veerhuis R, Breij ECW, Van Der Valk P,Dijkstra CD, Bø L. The pathology of multiple sclerosis islocation-dependent: no significant complement activationis detected in purely cortical lesions. J Neuropathol ExpNeurol 2005;64:147–55.
48. Pomeroy IM, Matthews PM, Frank JA, Jordan EK, Esiri
MM. Demyelinated neocortical lesions in marmosetautoimmune encephalomyelitis mimic those in multiplesclerosis. Brain 2005;128:2713–21.
49. Skripuletz T, Lindner M, Kotsiari A et al. Corticaldemyelination is prominent in the murine cuprizone modeland is strain-dependent. Am J Pathol 2008;172:1053–61.
50. Torkildsen O, Brunborg LA, Myhr KM, Bø L. Thecuprizone model for demyelination. Acta Neurol ScandSuppl 2008;188:72–6.
51. Storch MK, Bauer J, Linington C, Olsson T, Weissert R,Lassmann H. Cortical demyelination can be modeled inspecific rat models of autoimmune encephalomyelitis andis major histocompatability complex (MHC) haplotype-related. J Neuropathol Exp Neurol 2006;65:1137–42.
52. Merkler D, Ernsting T, Kerschensteiner M, Bruck W,Stadelmann C. A new focal EAE model of cortical demy-elination: multiple sclerosis-like lesions with rapid resolu-tion of inflammation and extensive remyelination. Brain2006;129:1972–83.
53. Clements RJ, McDonough J, Freeman EJ. Distribution ofparvalbumin and calretinin immunoreactive interneurons
Bø
56

in motor cortex from multiple sclerosis post-mortem tissue.Exp Brain Res 2008;187:459–65.
54. Wegner C, Esiri MM, Chance SA, Palace J, Matthews PM.Neocortical neuronal, synaptic, and glial loss in multiplesclerosis. Neurology 2006;67:960–7.
55. Cifelli A, Arridge M, Jezzard P, Esiri MM, Palace J,Matthews PM. Thalamic neurodegeneration in multiplesclerosis. Ann Neurol 2002;52:650–3.
56. Gilmore C, Deluca GC, Bø L et al. Spinal cord neuronalpathology in multiple sclerosis. Brain Pathol 2009;in press[Epub ahead of print, 19 December 2008].
57. Evangelou N, Konz D, Esiri MM, Smith S, Palace J,Matthews PM. Size-selective neuronal changes in theanterior optic pathways suggest a differential susceptibilityto injury in multiple sclerosis. Brain 2001;124:1813–20.
58. Gray E, Thomas TL, Betmouni S, Scolding N, Love S.Elevated matrix metalloproteinase-9 and degradation of
perineuronal nets in cerebrocortical multiple sclerosisplaques. J Neuropathol Exp Neurol 2008;67:888–99.
59. Dutta R, McDonough J, Yin X et al. Mitochondrial dys-function as a cause of axonal degeneration in multiplesclerosis patients. Ann Neurol 2006;59:478–89.
60. Gay FW, Drye TJ, Dick GW, Esiri MM. The applicationof multifactorial cluster analysis in the staging of plaquesin early multiple sclerosis. Identification and character-ization of the primary demyelinating lesion. Brain1997;120(Pt 8):1461–83.
61. Serafini B, Rosicarelli B,Magliozzi R, Stigliano E, Aloisi F.Detection of ectopic B-cell follicles with germinal centers inthe meninges of patients with secondary progressive multi-ple sclerosis. Brain Pathol 2004;14:164–74.
62. Serafini B, Rosicarelli B, Franciotta D et al. DysregulatedEpstein–Barr virus infection in the multiple sclerosis brain.J Exp Med 2007;204:2899–912.
Histopathology of grey matter demyelination in MS
57