Embed Size (px)
Citation preview

The Human Hepatic Asialoglycoprotein Receptor is a Target Antigen for Liver-infiltrating T Cells in Autoimmune Chronic
Active Hepatitis and Primary Biliary Cirrhosis
H A ” S LOHR, ULRICH TREICHEL, THOMAS PORALLA, MICHAEL M A ” S , KARL-HERMANN MEYER ZUM B~SCHENFELDE AND BERNHARD FLEISCHER
I . Department of Medicine, University of Mainz, 0 -6500 Mainz, FRG
Autoantibodies to the human hepatic asialoglyco- protein receptor have been found in nearly 50% of the sera of patients with autoimmune chronic active hep- atitis and in 15% of patients with primary biliary cirrhosis. In this study we demonstrate that the human hepatic asialoglycoprotein receptor is also a target antigen for T cell-mediated immune responses. Pe- ripheral blood lymphocytes of 37% (7 of 19) of patients with autoimmune chronic active hepatitis and 33% (2 of 6) of patients with primary biliary cirrhosis showed a proliferative response to highly purified human hepatic asialoglycoprotein receptor, whereas no pro- liferation was found with peripheral blood lympho- cytes of patients with chronic viral hepatitis (0 of 13) and healthy blood donors (0 of 4). Moreover, we isolated T-cell clones from liver biopsy samples of two patients with autoimmune chronic active hepatitis and two patients with peripheral blood lymphocytes. Be- tween 2.8% and 14.3% of these clones showed a specific proliferative response to purified human hepatic asia- loglycoprotein receptor. The response was restricted to autologous antigen-presenting cells and could be blocked by monoclonal antibodies against human leu- kocyte antigen-DR molecules. The response of T cells to the human hepatic asialoglycoprotein receptor did not require the lectinlike activity of the asialoglyco- protein receptor. Thus the human hepatic asialoglyco- protein receptor could be identified as a major target antigen of humoral and cellular immune reactions in autoimmune-mediated liver diseases. (HEPATOLOGY 1990; 12: 1314- 1320.)
Autoantibodies against a variety of cellular structures such as nucleus, smooth muscle membranes, soluble liver antigen and microsomes (ANA, SMA, SLA and LKM) have been found in sera as diagnostic markers for various types of autoimmune chronic active hepatitis (AI-CAH) (1-5). Their role in the pathogenesis of liver injury is unclear. The occurrence of autoantibodies to the human asialoglycoprotein receptor (anti-h-ASGPR)
Received November 6, 1989; accepted June 14, 1990. Address reprint requests to: Prof. Dr. Dr. Karl-Hermann Meyer zurn
Biischenfelde, 1. Medizinische Klinik und Poliklinik der Johannes Gutenberg- Universitat Mainz, Langenbeckstr. 1,6500 Mainz, Federal Republic of Germany.
31/1/24552
in sera of 50% of patients with AI-CAH and of 15% of patients with PBC has been recently documented. The anti-h-ASGPR titers showed a positive correlation with inflammatory activity (6-8). The ASGPR also called “hepatic lectin” is a well-characterized component of the liver-specific protein complex (LSP) expressed on the surface of the plasma membrane of hepatocytes and could therefore be a target antigen for an antibody- mediated immune reaction (5 ,6 ,9 , 10). In addition, the chronic liver injury in AI-CAH and PBC might be mediated by specific T cells that have cytotoxic activity or release lymphokines affecting the hepatocytes or the bile duct epithelia (11-13). Furthermore, helper T cells are required to induce autoantibody production in B lymphocytes. So far none of the autoantigens described above has been shown to induce a specific response of autoreactive T cells. To investigate the role of the h-ASGPR in cell-mediated immunity of AI-CAH and PBC we established T-cell lines and clones by limiting dilution from diagnostic liver biopsy and analyzed their antigen-specific proliferation. In this report we demon- strate that the h-ASGPR is a target antigen for a specific T-cell response. The T-cell clones recognizing the h- ASGPR appear to be restricted by HLA-DR antigens.
MATERIALS AND METHODS
Patients’ Characteristics. Two women patients (age 64 and 55 yr) with AI-CAH and two women patients (age 41 and 39 yr) with PBC gave informed consent for diagnostic liver biopsy. The histological examination of liver biopsy specimens re- vealed acute lymphohistiocytic infiltrations typical for an acute relapse of AI-CAH in Patients no. 1 and no. 2. Their sera contained ANA, but neither viral antigens nor antibodies to HBV, human immunodeficiency virus, cytomegalovirus or Epstein-Barr virus antigens were detectable. Both patients showed clinical symptoms of an acute relapse of AI-CAH with enhanced inflammatory activity and jaundice. The ALT level was 60 U/L (Patient no. 1) and 496 U/L (Patient no. 2) at the time biopsy specimens were taken. The histopathological examination of Patients no. 3 and no. 4 showed PBC grade IV (cirrhosis) and grade I1 (bile duct proliferation), respectively. They had high titers of antimitochondrial antibodies (AMA) in their sera. Serum of Patient No. 3 also contained ANA. High values of alkaline phosphatases indicated cholestasis and enhanced liver cell necrosis. All patients showed high-titer
1314

Vol. 12. No 6. 1990 T I l E AS(;PK AS 'I'AR(;ET AN'I'IGEN I N AI'TOIMMUNE (:AH 1315
TABLE 1. Patient's characteristics at time biopsy specimens were taken
Gammaglobulin Patient no. Age lhagnosib h-ASGPR ANA AMA ALT (UL) (gmn)
1 64 A1 ('AH 1 320 I 160 n d 60 21 02 2 55 A1 ('AH 1 320 1 320 n d 496 11 76 3 41 PIK IV 1 160 1 80 1 400 5 1 25 20 4 39 I'BC I1 1 640 n d 1 320 56 32 90
Biopsy specimens of these four patients were used for T-cell cloning. HLA types of the patients were A1,2, B53.73. Cw7, DR1,2 (Patient 1). A1,2, B7,8, Cw7, DR1,3 (Patient 2). A2.3. B35,44 Cw4.5. DRl .wl1 (Patient 3) . A25,w33, B8,18, Cw7, DR7,8 (Patient 4). CAH = chronicactive hepatitis; AMA = antirnitochondrial antibodies: ANA = antinuclear antibodies; PBC IV = cirrhosis, PBC I1 - ductal proliferation; ALT = alanine aminotransferase. n d . not detectable.
anti-h-ASGPR in their sera (Table 1) . The patients gave informed consent to this work, conformant to the Declaration of Helsinki ethical guidelines.
Liver-derived T Cells. The liver specimens were cut into several pieces of 2 mm and washed gently in medium IRPMI 1640 containing 1% glutamine. 1% gentamycin, 1 moliL HEPES buffer and 10% heat-inactivated FCS). The specimens were brought to the wells of a 96 flat-bottom well plate (Nunc GmBh, Roskilde, Denmark) with 200 ( ~ 1 medium supple- mented with recombinant interleukin 2 (IL-2) (Proleulun, Cetus Corp., Emeryville, CA) in a final concentration of 8.5 ng/ml(14-15). After 48 hr of incubation at 37" C and 10% CO, in a humidified atmosphere, the spontaneously outgrowing T cells were harvested, washed and further expanded in cultures or cloned as described below (fraction 1). The residual parts of the incubated liver biopsy specimens were transferred into fresh culture medium and disrupted mechanically by passage through a steel screen. The T cells from these biopsy specimens were then pooled and cloned in the same way (fraction 2).
Cloning and Expansion of Liver-derived T Cells. Cloning of T cells was performed as described (14-17). The liver-derived T cells were brought to 60-well Terasaki microtest-plate (Nunc) in a final concentration of 0.5 to 1 cells/well together with 1 x lo' irradiated allogenic feeder cells. The medium contained RPMI 1640 supplemented with 10% human serum. 8.5 ng/ml recombinant IL-2 and phytohemagglutinin (PHAb induced T-cell growth factor (PHA-TCGF). This medium contained PHA to allow growth of all resting or preactivated T cells present in the biopsy specimens. Because of the use of PHA, allogenic feeder cells could be used instead of autologous cells. It was shown previously that under these conditions ?' cells are stimulated to grow randomly without selection I 18). After 10 days of incubation in a humidified atmosphere at 37" C and 10% CO,, the proliferating T-cell clones were harvested, brought to a 96 round-bottom well plate and stimulated with 1 x 10" irradiated feeder cells and 0.5 pg/ml PHA. Growing cultures were further expanded by weekly splitting and restimulation with PHA and irradiated allogenic feeder cells. More than 95% of the T-cell clones derived from Patients 1 to 3 could be expanded to more than 5 x los cells.
Monoclonal Antibodies. The anti-CD4 monoclonal antibody ( d b ) OKT4, the antLCD8 mAb OKT8 and the anti-HLA-DR mAb L243 were obtained from the American Type Culture Collection (Rockville, MD) and were used as ascitic fluid. The mAb DA6.231 directed against monomorphic determinants of HLA-DR, HLA-DQ, HLA-DP molecules and the mAb B7121, specific for HLA-DP molecules, were also used as ascitic fluid.
Phenotyping of the T-cell Clones. The phenotypes of the T-cell clones were analyzed by using mAbs against the CD4 (OKT4) and CD8 (OKT8) molecules in a single cell ELISA (19); 3 x 10' cells were plated in a Terasaki microtest plate (Nunc)
pretreated with poly 1.-lysine. The cells were incubated with OKT4 or OKT8 antibodies, and after washing, the peroxidase- linked rabbit-anti-mouse immunoglobulin antibody was added (Dakopatts, Hamburg, FRG). The ELISA was developed with 670 mg of carbazole dissolved in 0.4 ml DMSO, 1 ~1 H,O, and 9.6 mlO.05 mol/L Tris HCl (pH 7.6). After staining for 30 min, the phenotypes could be determined by microscopy.
Antigen h p a r a t i o n . The h-ASGPR was prepared as de- scribed elsewhere (6, 8, 20, 21). Fresh frozen human liver tissue obtained from kidney donors whose livers were not suitable for transplantation for technical reasons was homog- enized and subsequently precipitated by acetone. Then s o h - bilization with triton X-100 and purification by two consec- utive affinity chromatography steps on a lactose-agarose column was performed. The eluted ASGPR preparation was characterized by SDS PAGE and Western blotting and showed no contaminants or degradation products. The biological function was proved by N-acetylgalactosamine (gal-NAc)- specific hemagglutination of desialinated erythrocytes (8). The protein was dialyzed three times against PBS and filtered through a 22-nm pore sterile filter. The concentration of protein was determined by the method of Lowry (22). The purity of this preparation was recently demonstrated. No human immunoglobulins were detectable with a polyvalent human immunoglobulin antibody (8).
Preparation of Peripheral Mononuclear Cells. Peripheral blood mononuclear cells (PBMNC) were separated from heparinized blood by centrifugation on Ficoll-Hypaque (Phar- macia AB, Uppsala, Sweden) density gradient at 400 g for 20 min (23). The cells at the interface were recovered and then washed two times in RPMI 1640.
Antigen-presenting Cells. Autologous or allogenic PBMNC ( 2 x 10') were resuspended and allowed to form rosettes with 1 ml of 2 4 neurarninidase-treated sheep erythrocytes for 30 min. The rosetted T-cell fraction was separated from non-T cells on a Ficoll density gradient a t 500g followed by hypotonic lysis of the sheep erythrocytes with sterile distilled water. The resulting nonrosette-forming lymphocytes (E-) were washed and resuspended in RPMI 1640 containing 1% gentamycin, 1% glutamine, 1 molL HEPES buffer and 10% heat-inactivated FCS. The E- cells were then incubated for 1 hr with the infectious supernatant of Epstein-Barr virus (EBV)-producing B95-8 cells. The EBV-transformed B lymphocytes (B-LCL) grew out within 2 wk and were cultured as a permanent cell line.
Assay for Proliferative Re8ponses. The proliferative re- sponse of T-cell clones to the purified ASGPR was analyzed as described by the rate of the "H-thymidine uptake (14). Clonal T cells (1 x 10') were incubated together with 3 x lo4 antigen-presenting cells (APC) t E- or mitomycin C-treated EBV-transformed B-LCL) and h-ASGPR at a final concen-

1316 LOHR ET AL. HEPATOLOGY
TABLE 2. Proliferative response of PBMNC reacting to h-ASGPR 'H-TdR incorporation (cpm) of PBL incubated with
mAb anti-HLA Patient no. Diagnosis M e d i U ASGPR ll t ASGPR PHA
~~~~~~~~~~~
1 AI-CAH 250 1,500 450 15,000 2 AI-CAH 450 2,600 n.d. 21,000 3 PBC IV 140 800 n.d. 1,300 4 PBC I1 200 220 n.d. 9,000 5 AI-CAH 12,000 28,000 10,000 26,000 6 AI-CAH 2,000 3,300 800 4,600 7 AI-CAH 200 1,100 n.d. 5,500 8 PBC I1 400 2,200 440 2,300 9 AI-CAH 500 3,600 n.d. 5,600
10 AI-CAH 400 2,200 n.d. 12,000
PBMNC were incubated with medium, h-ASGPR or PHA for 7 days. The MAb DA6.231 directed to monomorphic determinants on HLA class I1 molecules was added at a 11800 dilution. n.d. = not determined.
TABLE 3. Characteristics of patients suHering from AI-CAH or PBC Patient no. Diagnosis Stage ALT (UL) auto-ab anti-hASGPR pml.
1 AI-CAH Active 100 ANA 1: 160 1 : 320 + 2 AI-CAH Active 496 ANA 1 : 640 1 : 320 + 3 PBC Iv 77 AMA 1:400 1:160 + 4 PBC I1 56 AMA 1:320 1 : 640 5 AI-CAH 38 ANA 1:80 1 : 160 + 6 AI-CAH 83 ANA 1:80 1 : 320 + 7 AI-CAH Active 88 ANA 1 : 320 1 : 160 + 8 PBC I1 48 AMA 1 : 1,280 + 9 AI-CAH Mild 31 LKM + +
10 AI-CAH Active 92 LKM + + 11 AI-CAH Active 225 LKM + - 12 AI-CAH 75 ANA 1 : 8OlSLA + 1 : 160
AI-CAH 66 SMA 1 : 160 - 13 14 PBC 92 AMA 1:320 - 15 AI-CAH 96 ANA 1 : 320 - 16 AI-CAH 68 ANA 1 : 160
1: 160 - 17 AI-CAH 74 ANA 1 : 1601SMA + 18 AI-CAH Active 143 ANA 1 : 64OlSMA + 19 AI-CAH Active 63 SMA 1 : 640LMA + -
20 AI-CAH 112 ANA 1 : 160 1 : 160 -
21 AI-CAH 60 ANA 1 : 8OlSMA + - SLA + - 22 AI-CAH Mild 118
23 AI-CAH Mild 20 SMA 1:80 - 24 PBC 78 AMA 1:80 - 25 PBC 112 AMA 1:160 -
Stage = stage of disease according histopathological findings; auto-ab = titers of autoantibodies other than anti-h-ASGPR:
-
-
-
-
prol. = proliferative response of patient's PBMNC to h-ASGPR.
tration of 2.5 Clg/ml. Medium, PHA-induced T-cell clones and APC without T-cell clones served as controls. After 24 hr of incubation, the T cells were pulsed with 'H-thymidine, and another 24 hr later the cells were harvested, and the rate of incorporated radioactivity was determined by liquid scintil- lation.
The proliferation of PBMNC was measured in a similar way. PBMNC (1 x 107 were incubated with h-ASGPR for 6 days, then pulsed with 3H-thymidine for an additional 24 hr. Negative and positive controls were done with medium, PHA or tuberculin. To obtain lower background values the assay was performed in RPMI 1640 supplemented with 5% heat- inactivated human serum.
Data of proliferation assays are given as mean counts per minute (cpm) of triplicates or as mean stimulation index (test cpmhackground cpm) of triplicates.
RESULTS Proliferutiw Response of PBMNC. PBMNC of 42
patients with autoimmune CAH (n = 19), PBC (n = 61, chronic active viral hepatitis B and non-A, non-B hepatitis (n = 13) and PBMNC of healthy blood donors (n = 4) were tested for their proliferative response to h-ASGPR. Seven of 19 patients with AI-CAH (five ANA positive, two LKM positive AI-CAH) and two of six

Vol. 12, No. 6. 1990 ' r im ASGPK AS TARGET ANTIGEN IN ALYTOIMMUNE CAH 1317
TABLE 4. Phenotypes of liver-infiltrating T-cell clones Patient no. Diagnosis Clo. eff. No. clon. CD4' CD0 ' C D ~ ' i m a +
1 A1 CAH 9 76% 41 24 17 1 3 8
2 A I -( 'AH 18 33% 225 136 89 1 5 2
3 PRC IV 12 80% 77 41 :33 1 2 6
4 PIK' I I 9 83% 38 29 9 3 22
I 4 1/420l
r220'1,200)
I 7716001
j 591600)
Liver-derived T-cell clones were phenotyped by using mAbs to the CD4- and CD8-receptors with an ELISA-technique. All but Patient no.
Clo. eff. = cloning efficiency means the ratio of growing T-cell clones and maximal expected T-cell clones. No. clon. = number of growing 4 had comparable results in the CD4iCD8 ratio. Some T-cell clones of Patient no. 4 were lost before phenotyping.
T-cell clones.
TABLE 5. Proliferative reeponse of liver-derived T-cell clones to the h-ASGPR
'H-TdR incorporation (cpm) of clones to
Autologow B-LCL with Allogenic B-LCL with
Clone Medium ASGPR PHA Medium ASGPR
L7K1 600 3,000 2,500 2,000 600 L7K2 200 34.000 29,000 250 200 L7K3 100 17,000 14,000 250 100 L7K4 150 6,500 4,500 200 150 L7K5 100 2,500 3,500 150 200 L7K14 360 5.700 7,000 600 500 L49SK39 5 1 0 4.400 4,300 550 600 L49SK55 460 5,400 3,200 1,100 650 L49SK75 240 4,600 2,000 400 500 L49BK4 1.700 6,300 5,000 1,700 2,100 L49BK23 1 1,000 76,000 40,000 6,300 8,000 L49BK28 700 3,200 20,000 730 1,200 L57SK14 730 3,200 1,450 400 440 L57SK52 600 1,200 2,600 750 650 L57BK17 700 1,700 8,500 320 400 L86K3 620 3,730 12,000 750 550
The T-cell clones were incubated with autologous or completely HLA-mismatched B-LCL cells in the presence of the h-ASGPR (2.5 pg/ml) or PHA. All clones except L7K1 and L7K3 had the CD4 '-phenotype L7K = clones of Patient 1. L49K = clones of Patient 2, L57K = clones of Patient 3. L86K = clones of Patient 4 .
patients with PBC showed proliferative responses to the h-ASGPR. Monoclonal antibodies to HLA class I1 an- tigens were found to inhibit these responses. The stimulation indices were 5-fold (range = 1.6 to 6.0). The optimal antigen concentration was 2.5 Fg/ml (range = 0.5 to 3 Fg/ml). The histopathological exami- nations and the raised ALT levels of these patients a t the time PBMNC were taken indicated a chronic ac- tive inflammatory process. Table 2 shows the experi- mental data including Patients no. 1 to 4. Note that the PBMNC of Patient no. 4 did not respond to h-ASGPR (Table 2). The second group of PBMNC patients did not show a response to h-ASGPR. This group included 12 patients with AI-CAH (11 ANA and SMA positive, one LKM antibody-positive AJ-CAH) and four with PBC. None of five patients with viral non-A, non-B hepatitis; eight patients with hepatitis B; and four healthy blood donors had positively reacting PBMNC
(Table 3). The PBMNC were obtained from several patients on different occasions and were tested with identical results.
Prolifemtiw Response of Liuer-infiltrating T Lym- phocytes. Liver-derived T-cell clones were generated as described above to characterize infiltrating lymphocytes in AI-CAH and PBC. The cloning efficiency, defined as number of clones obtained divided by the number of seeded wells, ranged from 9.8% to 18.3% (Table 4).
Three hundred seventy-three T-cell clones from liver tissue were characterized phenotypically by using mAb to the CD4- and the CDS-receptor in the single-cell ELISA. Most clones of all patients showed the CD4- positive CDS-negative phenotype. Clones of Patients no. 1 to 3 showed a CD4/CD8 ratio between 1.2 and 1.6. Patient no. 4 had a ratio of 3.75, possibly because some clones had been lost for technical reasons before pheno- typing (Table 4). There was no significant difference in

1318 LOHR ET AL.
32MM 1
28000
2 m
12000
w Fa E w
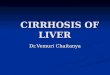
autologous B u I I a autologoua B + PHA autologoua B + hASGPR autologoua B + hASGPR + 50 mM galactoso
HEPATOLOCY
L7K2 L7K3 L7K4
FIG. 1. Effect of galactose on h-ASGPR-specific proliferative responses. T-cell clones were preincubated with autologous APC in the presence of medium, PHA, h-ASGPR or h-ASGPR together with 50 mmol/L galactose
L49BK23
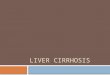
L49SK55
hASGPR + mAb HLA-DP 0 hASGPR + mAb HLA-DR
hASGPR + mAb HLA II
L49SK39
0 2000 4000 6000 8000
(CPm)
FIG. 2. Inhibition of h-ASGPR-specific proliferative response of T cells by mAb directed to HLA class I1 molecules. Liver-derived T-cell clones were stimulated with autologous B-LCL in the presence of medium, PHA, h-ASGPR and h-ASGPR with different mAb. mAb DA6.231 directed to monomorphic determinants on HLA class I1 molecules, mAb L243 directed to HLA-DR molecules or mAb B7/21 directed to HLA-DP molecules.
the CD4/CD8 ratio when phenotyping the clones of fraction 1 and 2 (Table 4).
Two hundred thirteen T-cell clones obtained from liver biopsy samples of Patients No. 1 to 4 could be examined for their proliferative response to h-ASGPR in an antigen-specific proliferation assay with autologous and allogenic APC. We used B-LCL as APC because autologous E- were not available in sufficient numbers from these patients. Such B-LCL cells have been shown to be potent APC for several different antigens in several different systems (24, 25). Six of 41 clones of Patient no. 1, six of 65 clones of
Patient no. 2, three of 77 clones of Patient no. 3 and one of 38 clones of Patient no. 4 showed a dose-dependent proliferative response to h-ASGPR using autologous
APC, reaching a maximum of 3H-thymidine uptake when cultured in the presence of 2.5 pg/ml h-ASGPR. In Patient no. 1 two proliferating clones showed the CD8-positive phenotype. This phenotype was deter- mined twice. No significant antigen-induced prolifer- ative response was found if h-ASGPR was presented by allogenic APC (Table 5). Many of these clones were tested again after several weeks in culture with identical results.
To exclude an unspecific stimulation by binding of the h-ASGPR to cell-surface glycoproteins, we examined the rate of proliferation after addition of 50 mmoVL D- galactose to the cultures. As shown in Figure 1, there was no influence of D-galactose on response to the h-ASGPR.

Restriction o f Proliferative Response by HLA-DR Antigens. The h-ASGPR-induced proliferation of the clones was inhibited by a mAb-directed against mono- morphic determinants on HLA class I1 molecules (DA6.231) and on HLA-DR molecule tL243) but not by a mAb against HLA-DP antigens tB71211. This shows that recognition of the h-ASGPR by cloned liver-derived T cells is restricted by HLA-DR gene products expressed on the surface of autologous APC (Fig. 2).
DISCUSSION
Various types of AI-CAH can he characterized by the occurrence of several diagnostic marker autoantibodies like ANA, SMA, LKM and SLA in serum ( 1-5). However. their antigens have so far not been shown to be expressed on the cell surface and lack organ specificity ( 1, 3-5). In recent studies autoantibodies to the liver- specific protein (LSP) complex were thought to be involved in the pathogenesis of AI-CAH (6, 11, 26-29). Rabbits immunized with human LSP complex showed typical necrosis in liver (9) . This LSP complex, how- ever, was shown to contain heterogeneous cytoplasmic proteins carrying different antigenic determinants (6, 7, 9, 30, 31). In addition the LSP autoantibodies showed immunohistochemically cross-reactions with various tissues, especially with the kidney (31-33). One well-characterized constituent of the LSP fraction is the ASGPR that is expressed on the surface of hepatocytes (6, 7, 21, 34, 35). The ASGPR, also called "hepatic lectin," functions as a receptor for desialinated glyco- proteins and is expressed homogeneously on the hepa- tocyte plasma membrane (21, 34. 36). The occurrence of anti-h-ASGPR in 50% of patients with AI-CAH has recently been reported ( 8 , 27). Additionally, 15% of patients with PBC showed anti-h-ASGPR ( 8 ) . The anti-h-ASGPR were predominantly found (88% in patients with severe inflammatory activity proven by histopathologcal findings ( 8 , 27). Furthermore, the occurrence of anti-h-ASGPR did not correlate with distinct subtypes of AI-CAH or PBC, other autoanti- bodies or rheumatoid factors ( 8 ) .
The chronic liver injury in AI-CAH and in PBC is thought to be mediated by T lymphocytes infiltrating the liver tissue either by cytotoxic activity against hepatic tissue or bile duct epithelia or by releasing lymphokines that attract bystander T cells or damage hepatocytes directly (11, 13, 16, 32, 37-39). Immunohistological examinations showed a predominance of CD8-positive T cells in the liver infiltrations of AI-CAH and PBC. Among the infiltrating T cells, however, there appear to be more activated CD4-positive than CD8-positive T cells (13, 16, 32, 37). In this study, cloning T cells from liver biopsy specimens of three of four patients revealed a slight increase in CD8-positive T cells in comparison with the normal CD4ICDR ratio in PBMNC. Our protocol of cloning selects for preactivated T cells because IL-2 receptor-positive T cells are allowed to expand in the medium supplemented with recombinant IL-2. After addition of PHA during the cloning pro- cedure, no further selection of subpopulations occurred and all cultures had the same growth conditions. This
cloning protocol allows growth of all T lymphocytes regardless of their phenotype and antigen specificity ( 14, 15, 18). There was no significant difference in the CD4iCD8 ratio of spontaneously outgrowing T cells (fraction 1) and 'r cells collected after mechanical disruption of liver tissue (fraction 2 I . These data indicate that both fractions represent liver-infiltrating-activated T cells (16).
Our data demonstrate the existence of activated, IL-2-receptive T cells in the liver infiltration of AI-CAH and PBC that specifically proliferate to the h-ASGPR in the presence of autologous but not allogenic APC. We used B-LCL as AFT because the supply of PBMNC of our patients was limited. B-LCL cells are potent APC for a variety of antigens. It has been reported that some T-cell clones recognize their antigen only presented by macro- phages and monocytes but not B-LCL cells (24, 25). Thus there might be additional h-ASGPR-specific T cells among our clones that we did not detect. Fur- thermore, the recognition could be blocked by mAb against HLA-DR molecules. This indicates that these cells are HLA-restricted T cells. The fact that two of these h-ASGPR-specific clones of Patient no. 1 had the CD8-positive phenotype is surprising because exogenous antigens are thought to be recognized only by CD4- positive T cells in the context of HLA class I1 molecules (40,41). There are, however, exceptions to this rule (42).
The blocking of h-ASGPR by galactose has no in- fluence on recognition of h-ASGPR by T cells. These data strongly suggest that h-ASGPR acts as an antigen and not as a nonspecific lectinlike stimulant. It is difficult to envision a proper control antigen for h-ASGPR. However, since the assays were performed in medium supplemented with 10% FCS, abundant glycoproteins are around.
Taken together, our data clearly show the presence of a significant number of h-ASGPR-specific T cells among the liver-infiltrating T cells in four patients with AI-CAH or PBC.
Furthermore, our data also show that PBMNC of some additional patients with AI-CAH and PBC but not of patients suffering from chronic viral hepatitis had positive proliferative responses to the h-ASGPR. This indicates that autoreactive T cells recognizing this self-antigen may be a common finding in these diseases. The negative response of peripheral T cells in Patient no. 4, despite the presence of h-ASGPR-specific T cells in the liver, indicates an enrichment of autoreactive T cells at the site of inflammation. The finding that PBMNC of only 37% of AI-CAH and 33% of PBC showed a proliferative response to h-ASGPR correlate with the data on anti-h-ASGPR antibodies. No correlation of T-cell response could be found to inflammatory activity because only four patients were examined by diagnostic liver biopsy. Furthermore, the ALT levels cannot predict the inflammatory activity exactly.
Finally, most autoantigens are characterized by anti- bodies, but it is not known whether the autoantibodies are directed against cross-reacting epitopes on different proteins (e. g., viral antigens) or whether the immune response is initiated and directed against the autoan-

LOHR ET AL. HEPATOLOGY 1320
tigen itself. For the first time we present evidence that in an autoimmune chronic liver disease some T-cell epitopes are located on the same autoantigen as the B-cell epitopes. These data suggest that the ASGPR is a target antigen for both humoral and cellular immune reactions and that the h-ASGPR might be involved in the pathogenesis of AI-CAH and PBC.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Mackay IR, Taft LI, Cowling DC. Lupoid hepatitis. Lancet
Manns M, Meyer zum Biischenfelde K-H, Slusarczyk J, Dienes HP. Detection of liver-kidney microsomal autoantibodies by radioimmunoassay and their relation to antimitochondrial anti- bodies in inflammatory liver diseases. Clin Exp Immunol 1984;
Manns M, Gerken G, Kyriatsoulis A, Staritz M, Meyer zum Biischenfelde K-H. Characterization of a new subgroup of au- toimmune chronic active hepatitis by autoantibodies against a soluble liver antigen. Lancet 1987;1:292-294. Hopf U, Meyer zum Biischenfelde K-H, Arnold W. Detection of a liver membrane autoantibody in HBsAg-negative chronic active hepatitis. N Engl J Med 1976;294:578-582. Manns M, Meyer zum Biischenfelde K-H, Hess G. Autoantibodies against liver-specific membrane lipoprotein in acute and chronic liver diseases: studies on organ-, species- and disease-specificity.
McFarlane IG, McFarlane BM, Major GN, Tolley P, Williams R. Identification of the hepatic asialoglycoprotein receptor (hepatic lectin) as a component of liver specific membrane lipoprotein (LSP). Clin Exp Immunol 1984;55:347-354. McFarlane BM, McSorley CG, Vergani D, McFarlane IG, Williams R. Serum autoantibodies reacting with the hepatic asialoglyco- protein receptor (hepatic lectin) in acute and chronic liver disorders. J Hepatol 1986;3: 196-205. Treichel U, Poralla T, Hess G, Manns M, Meyer zum Biischenfeldt K-H. Autoantibodies to human asialoglycoprotein receptor (ASGPR) in autoimmune-type chronic hepatitis. HEPATOLOGY 1990;
Helin H, Uibo R, Paronen I, Krohn K. Immunohistochemical localization of human liver specific protein using rabbit antisera and the avidin-biotin complex technique. Clin Exp Immunol
Manns M, Meyer zum Biischenfelde. Fractionation of the liver membrane lipoprotein (LSP) and characterisation of its antigenic determinants by autoantibodies and a heterologous anti-serum.
Vento S, Eddleston AL. Immunological aspects of chronic active hepatitis. Clin Exp Immunol 1987;68:225-232. Mackay IR, Gershwin ME. Molecular basis of mitochondria1 autoreactivity in primary biliary cirrhosis. Immunology Today
Lobo-Yeo A, Alviggi L, Mieli-Vergani G, Portmann B, Mowat A, Vergani D. Preferential activation of helperhnducer T lympho- cytes in autoimmune chronic active heptitis. Clin Exp Immunol
Fleischer B, Kreth HW. Clonal analysis of HLA-restricted virus specific T lymphocytes from cerebrospinal fluid in mumps men- ingitis. J Immunol 1983;130:2187-2192. Vallbracht A, Maier K, Stierhof Y-D, Wiedmann KH, Flehmig B, Fleischer B. Liver-derived cytotoxic T cells in hepatitis A virus infection. J Infect Dis 1989;160:209-217. Meuer SC, Moebius U, Manns M, Dienes HP, Ramadori G, Hess G, Hercend T, et al. Clonal analysis of human T lymphocytes infiltrating the liver in chronic active hepatitis B and primary biliary cirrhosis. Eur J Immunol 1988;18:1447-1452. Fleischer B, Becht H, Rott R. Recognition of viral antigens by human influenza virus-specific T lymphocyte clones. J Immunol
Moretta A, Pantaleo G, Moretta L, Mingari MC, Cerottini JC. Quantitative assessment of the pool size and subset distribution of
1956;1323-1326.
57:600-608.
Gut 1980;21:955-961.
11:606-612.
1985;59:371-376.
Gut 1982;23:14-20.
1989;10:315-318.
1987;67:95-104.
1985; 135~2800-2804.
cytolytic T lymphocytes within human resting or alloactivated peripheral blood T cell populations. J Exp Med 1983; 158:571-560.
19. Holzmann B, Johnson J . A P-galactosidase-linked immunoassay for the analysis of antigens on individual cells. J Immunol Methods 1983;60:359-365.
20. Hudgin RL, Pricer WE, Ashwell G, Stockert RJ, Morel1 AG. The isolation and properties of a rabbit liver binding protein specific for asialoglycoproteins. J Biol Chem 1974;249:5536-5544.
21. Tanabe T, Pricer WE, Ashwell G. Subcellular membrane topology and turnover of a rat hepatic binding protein specific for asialoglycoproteins. J Biol Chem 1979;254:1038-1043.
22. Lowry DH, Rosebrough MJ, Farr AL, Randall KI. Protein mea- surement with the folin reagent. J Biol Chem 1951;193:265-275.
23. Boyum A. Separation of leukocytes from blood and bone marrow. S a n d J Clin Lab Invest 1968;21: 1-5.
24. Lanzavecchia A. Antigen-specific interaction between T and B cells. Nature 1985;314:537-539.
25. Van der Pouw Kraan TT, Stiekema FE, Teunissen MB, Bos JD, Kapsenberg L. The selective antigen-presenting cell capacity of activated B lymphocytes in HLA-11-restricted responses of CD4 + T lymphocytes. Immunology 1989;69:147-153.
26. Meyer zum Biischenfelde K-H, Alberti A, Arnold W, Freudenberg J . Organ-specificity and diagnostic value of liver-specific mem-
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39. 40.
41.
42.
brane-protein: studies in hepatic and non-hepatic diseases. Klin Wochenschr 1975;53: 1061-1067. McFarlane IG, Hegarty JE, McSorley CG, McFarlane BM, Williams R. Antibodies to liver- specific protein predict outcome of treatment withdrawal in autoimmune chronic active hepatitis. Lancet 1984;2:954-956. Poralla T, Manns M, Dienes HP, Dippold W, Hiitteroth TH, Meyer zum Biischenfelde K-H. Analysis of liver-specific protein LSP using murine monoclonal antibodies. Eur J Clin Invest 1987;17:
Poralla T, Ramadori G, Dienes HP, Manns M, Gerken G, Dippold W, Hiitteroth TH, et al. Liver cell damage caused by monoclonal antibody against an organ specific membrane antigen in vivo and in vitro. J Hepatol 1987;4:373-380. Feher J , Filipp G, Kocsar L, Mohari K, Toncsev H, Feher E, Biro G. Inhibition of autoimmune hepatitis with hot labelled liver specific antigen. Clin Exp Immunol 1984;55:360-368. Chisari FV. Liver-specific protein in perspective. Gastroenterology
Paronetto F, Vernace S. Immunological studies in patients with chronic active hepatitis: cytotoxic activity of lymphocytes to autochthonous liver cells grown in tissue culture. Clin Exp Immunol 1975;19:99-104. Behrens UJ, Paronetto F. Studies on liver specific antigens: evaluation of the liver specificity of LSP and LP-2. Gastroenter-
Harford J , Ashwell G. Immunological evidence for the transmem- brane nature of the rat liver receptor for asialoglycoproteins. Proc Natl Acad Sci USA 1981;78:1557-1561. Spiess M, Schwartz AL, Lodish H. Sequence of human asialogly- coproteinreceptor cDNA. J Biol Chem 1985;260: 1979-1982. Mizuno M, Brown WR, Vierling JM. Ultrastructural immunocy- tochemical localization of the asialoglycoprotein receptor in rat hepatocytes. Gastroenterology 1984;87:763-769. Vento S, O’Brien CJ, McFarlane BM, McFarlane IG, Eddleston A, Williams R. T-lymphocyte sensitization to hepatocyte antigens in autoimmune chronic active hepatitis and primary biliary cirrhosis. Gastroenterology 1986;9 1 :8 10-8 17. Hoffmann RM, Pape GR, Spengler U, Rieber EP, Eisenburg J, Dohrmann J , Paumgartner G, et al. Clonal analysis of liver- derived T cells of patients with primary biliary cirrhosis. Clin Exp Immunol 1989;76:210-215. Duke RC. Self recognition by T cells. J Exp Med 1989;170:59-71. Long EO, Jacobson S. Pathways of viral antigen processing and presentation to CTL. Immunology Today 1989;10:45-48. Long EO. Intracellular traflic and antigen processing. Immu- nology Today 1989;10:232-234. Jin Y, Shih JW, Berkower J. Human T cell response to the surface antigen of hepatitis B virus (HBsAg). J Exp Med 1988;168:293- 306.
360-367.
1980;78: 168- 172.
ology 1979;77:1045-1053.