Embed Size (px)
Citation preview

Flexner Centenary
The Increasing Complexities ofProfessionalismFrederic W. Hafferty, PhD, and Brian Castellani, PhD
AbstractOrganized medicine’s modern-dayprofessionalism movement has reachedthe quarter-century mark. In this article,the authors travel to an earlier time toexamine the concept of profession withinthe work of Abraham Flexner. AlthoughFlexner used the concept sparingly,it is clear that much of his writingon reforming medical education isgrounded in his views on physicians asprofessionals and medicine as aprofession.
In the first half, the authors exploreFlexner’s views of profession, whichwere (1) empirically (as opposed tophilosophically) grounded, (2) casebased and comparatively framed, (3)
sociological in orientation, and (4)systems based, with professionalismconceptualized as dynamic, evolving, andmultidimensional.
In the second half, the authors build onFlexner’s systems perspective tointroduce a complexity scienceunderstanding of professionalism. Theydefine professionalism as a complexsystem, introduce a seven-part typologyof professionalism, and explore how theorganization of physician work andvarious flash points within medicinetoday reveal not one but severalcompeting forms of professionalism atwork. The authors then develop atripartite model of professionalism with
analysis at the micro, meso, and macrolevels. They conclude with observationson how best to frame professionalism asa force for change in 21st-centurymedical education.
Flexner’s reforms were grounded in hisvision of two particular types ofprofessional—the physician clinicianand the full-time academic physician–scientist. The authors propose reformgrounded in professionalism as acomplex system composed of competingtypes.
Acad Med. 2010; 85:288–301.
Medicine in the United States today isawash in a sea of complexities. Millionslack access to basic medical services.1,2
Health disparities abound.3,4 Efforts toimprove patient safety are labyrinthine.5
Quality in patient care remains elusive,and quality initiatives are oftencontradictory.6 – 8 Health expenditureshave surged into the trillion-dollarstratosphere.9 Medical school graduatescourt lifestyle specialties and areabandoning primary care in recordnumbers.10 –13 Mandated limits onresident duty hours have upendedtraditional teaching practices, andquestions about the commitments ofnewer physicians to traditionalprofessional values have become part ofthe national educational dialogue.14 –17
Reports of economic opportunism andconflicts-of-interest (COIs) within
researcher, educator, and clinician rankshave become a media staple.18 –21
Within this maelstrom of work andidentity, organized medicine has calledfor change along a number of fronts,including quality of care, patient safety,evidence-based medicine, physicianworkforce, and, in the face of a self-perceived loss of public trust, a call forphysicians to recommit themselves to theprinciples of medical professionalism. Insum, medicine currently struggles withwhat it means to practice high-qualityscientifically grounded medicine, howone best trains physicians for an ever-changing work environment, and what itmeans to be a professional.
One hundred years ago, medicine andmedical education faced a similar crisis ofidentity and identification. An emergingscience of clinical medicine was beingheld hostage by the practice patterns ofclinicians trained in another era andunder a different value system—muchlike today’s controversies over evidence-based medicine, the nature of scientificevidence, and the “necessary”restructuring of physician practicepatterns.7,22,23 Commercialism, which atthat time was emblematized by a gaggleof proprietary medical schools, cast a very
long and stifling shadow. Meanwhile, arapidly expanding (numbers andgeographic) population lacked access towell-trained physicians. Into this vortexstepped a number of change agents,including Abraham Flexner, Frederick T.Gates, Franklin Mall, Henry Pritchett,and William H. Welch. They representeda new vision of medical education andmedical practice and the emerging powerof philanthropic organizations. Flexner’sBulletin No. 4 (the “Flexner Report”)24
was one important blueprint in thatreform.
As visionaries conceived andphilanthropies conspired, change beganto bubble. In this article, we focus on oneparticular percolate—professionalism.Flexner’s efforts to reform medicaleducation and medical practice were verymuch grounded in his views of physiciansas professionals (or at least “potentialprofessionals”) and of medicine as aprofession.* Flexner’s approach to
Dr. Hafferty is professor, Department ofBehavioral Sciences, University of Minnesota MedicalSchool–Duluth, Duluth, Minnesota.
Dr. Castellani is associate professor, Departmentof Sociology, Kent State University, Kent, Ohio.
Correspondence should be addressed to Dr.Hafferty, Department of Behavioral Sciences,University of Minnesota Medical School–Duluth,1035 University Drive, Duluth, MN 55812;telephone: (218) 726-7144; e-mail:[email protected].
*Throughout this article, we alternate between theterm profession (as a conceptual referent, similar tohow one might use the terms bureaucracy and freemarket) and the term professions (a descriptive labeland more fitting when speaking about severalprofessions and/or professions in general). For themost part, Flexner used the term descriptively.
Academic Medicine, Vol. 85, No. 2 / February 2010288

professionalism is notable in severalrespects.
• His approach was empirically (asopposed to philosophically) grounded.
• His approach was case based andcomparative. Flexner drew on otheroccupations and other educationalsystems in crafting his analysis.
• Flexner’s orientation was philosophical,with society and social forces playing adetermining role in the evolution ofprofessionalism.
• Flexner took a systems approach,treating professionalism as an evolvingand dynamic force.
• Flexner’s view of professionalism wasmultidimensional: He conceptualizedprofessionalism at both the individualand organizational levels.
• Flexner saw professionalism embodiedin two somewhat countervailing types:the full-time academicphysician–scientist versus thepracticing clinician.
Of additional interest is the similarity ofFlexner’s approach to current educationalreform and the new science of complexity,an approach being adopted by a growingnetwork of faculty within academicmedicine. Like Flexner, these scholarsconceptualize many of the challengesfacing medicine today in systems terms,ranging from disease etiology25,26 tocommunity health,27 primary care,28 andmedical professionalism.29 –31 Key to theseinitiatives is the promise of improvedhealth policy27—which leads to yetanother way these complexity sciencescholars are similar to Flexner. AlthoughFlexner did not write extensively aboutprofessionalism, it is clear that hismethodological approach to change castprofessionalism as an engine of reform.More specifically, he grounded his reformof medical education in a particular typeof professional, the full-time academicphysician–scientist. In sum, the success ofFlexner’s reforms was, in part, a functionof the method he adopted, which often isthe case with results seeped in complexityanalysis as well.
We believe that these previouslyunexplored linkages between Flexner’ssystems-like view of professionalism andhis visions for medical education reformhave considerable import for morecontemporary calls for change. We also
believe that further insights can be gainedby revisiting Flexner’s original vision forchange, his underlying methodologicalapproach, and the role of professionalismin that change, and, in turn, placing allthree within a more formal complexsystems framework. We wrote this articleto demonstrate why we hold these beliefs.
Overview
We organized this article into two majorsections. In the first section, “Flexner andProfessionalism,” we review what Flexnerhad to say about the nature of professionsand professionalism, paying particularattention to Flexner’s view ofprofessionalism as a dynamic andfundamentally social process and thetransformative role Flexner envisionedfor altruism in the growth of medicine asa true profession. Also core to Flexner’svisions of educational reform was hisview that commercialism is antithetical toprofessionalism and his identification ofa new type of medical educator—thefull-time academic physician–scientist.We highlight Flexner’s relativelysophisticated systems view ofprofessionalism, his sensitivity to context,his views of how different models ofmedical education have evolved out ofdifferent social and culturalenvironments, and his penchant for usingcomparative case studies to develop anideal, yet nuanced, model of medicaleducation in the United States.
The second section, “A TheoreticalModel for Researching Professionalism,”outlines an agenda for investigatingprofessionalism as a complex system.This section is divided into three parts.First, we begin with a basic definition ofprofessionalism as a complex system.From this standpoint, we argue that thecurrent conception of professionalismbeing advanced within organizedmedicine, something we label nostalgicprofessionalism29 (a label tied to organizedmedicine’s explicit and repeated calls forphysicians to rediscover and recommitthemselves to traditional professionalprinciples), is an overly restricted andultimately unproductive way to leverageprofessionalism as a tool in thetransformation of 21st-century medicine.In contrast, we present a systems-basedapproach to medical professionalism.We trace the evolution of medicine’smodern-day (mid-1980s to present)professionalism movement, and in doing
so we explore how sociohistorical datareveal not one, but rather multiple, formsof professionalism (e.g., entrepreneurial,lifestyle, nostalgic, activist) at work.Second, we explore the web of relationsamong these types, and we propose amultipronged and complexity-drivenresearch agenda to both study andunderstand the structure and dynamicsof medical professionalism. Third,we explore how best to frameprofessionalism as a force for change inthe evolution of 21st-century medicaleducation, and we seek to do so in a spiritsimilar to Flexner’s. Flexner proposededucational reform based on his vision ofthe physician educator. We proposeeducational reform based on ourunderstanding of professionalism as acomplex system composed of competingtypes.
Flexner and Professionalism
Despite his wealth of writings on medicaleducation and its reform, it is importantto note from the outset that Flexner didnot often use the concept of profession asa core element in his analytical armament.This should not be surprising, given thatconcept’s relatively undeveloped presencein the early decades of the 20th centuryboth within sociology and medicine.Nonetheless, what Flexner had to sayabout medicine as a profession, bothdirectly and indirectly, is essential tounderstanding his overarching agenda ofeducational reform.
Flexner’s six-part definition andcase-based comparative approachto profession
Flexner’s most detailed statement aboutprofessions did not appear in Bulletin No.4, nor in any of his other writings onmedical education, but rather in aninvited 1915 address (“Is social work aprofession?”) to the National Conferenceof Charities and Correction.32 In hispresentation, Flexner advanced a six-partdefinition of profession, along with a hostof other comments that reflected a highlycontextual, dynamic, relational, andsystems-oriented view of professions.
For Flexner,
professions involve essentially intellectualoperations with large individualresponsibility; they derive their rawmaterial from science and learning; thismaterial they work up to a practical anddefinite end; they possess an educationally
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010 289

communicable technique; they tend to self-organization; they are becoming increasinglyaltruistic in motivation.32(p156)
Fundamental to understanding Flexner’sapproach to professions is how heemployed each of his six definitionalelements within a case-based,comparative analysis. In his 1915 address,Flexner used each criterion to assess theprofessional prospects of severaloccupational groups, social work beingonly one of many occupations hereviewed. In doing so, Flexnerunderscored what would become asignature element in his approach topolicy and reform initiatives—the use ofdata from multiple sources (be theynation-states, occupational groups, or auniverse of medical schools) to drive ananalysis constantly grounded in acomparative method. His address alsoreflected another signature proclivity, histendency to be disconcertingly candid inhis assessments—which included, in thisinstance, the unapologetic conclusionthat social work fell short in its claim tobe a profession.
Using his definitional template,Flexner walked his audience through astep-by-step analysis of pharmacy,banking, plumbing, journalism, andsocial work—rejecting each, in turn, as aprofession. In other comments, Flexnerrepeatedly identified medicine andengineering as professions, closelyfollowed (in frequency of mention) bythe clergy, law, and architecture. He alsorepeatedly characterized business as anonprofession. In one isolated burst, butwithout any further explanation, Flexneridentified literature, painting, and musicas professions.32(p158) Finally, and in afascinating and uncharacteristicallyequivocal aside, Flexner labeled theprofessional prospects of nursing as a“live wire” and nursing itself a “twilight[i.e., betwixt and between] case.”32(p158)
Flexner’s sociological approach toprofessions
Along with being empirically grounded,Flexner’s approach was resolutelysociological—in that he sought to depictprofessionalism in its wider socialcontext. For example, although Flexnerconsistently referred to professionalismas “a calling,” he also recognizedprofessionalism as a social status and onethat is tied to public recognition. Flexneridentified professionalism as a shared
occupational identity tied to a “strongclass consciousness,” something heviewed as both “aristocratic in form” yet“highly democratic,” with the trainingprocess based on individual achievementsrather than an ascribed socialstatus.32(p153) Moreover, Flexner wascognizant that even by 1915, the labelprofessional had been culturally hijacked/expropriated by a large number ofoccupational groups, thus undercuttingat least some of its cultural capital.Finally, and anticipating a key issue in thecontemporary professionalism debate,Flexner addressed the balance betweenfamily and work, concluding that “thesocial and personal lives of professionalmen and their families thus tend toorganize around a professionalnucleus.”32(p156)
Flexner’s systems approach toprofessions
The third distinction of Flexner’sapproach is its systems orientation.Simply put, Flexner believedprofessionalism to be a dynamic andevolutionary force. Nonetheless, whendiscussing medicine, he did limit hisfocus exclusively to physicians’attainment of professionalism and didnot explore the possibility that medicineitself might lose its status as a professionat some point in the future.
Flexner also recognized (shades of the1980s) that occupational groups maystrategically embark on their ownprofessionalism initiatives and that anydeliberate striving for professional statuscould spark “battles” and “trenchwarfare.”32(p164) Here, Flexner’s concernsforeshadow Abbott’s33 famous 1980swork (at least within sociology) onprofessions as a system of countervailinginterests.
Key to understanding Flexner’s visionof professions as dynamic and evolvingare his views on the role of altruism in theevolution of professionalism as atransformative social force (see the last ofFlexner’s six criteria in the quote above).Flexner was unequivocal in insisting thatthis “professional spirit” had yet to berealized across professional groups ingeneral and within medicine inparticular. For Flexner, altruism wassomething that “may . . . come to be amark of professional character” and issomething where the “pecuniary interestof the individual practitioner . . . [is] apt
to yield gradually before an increasingrealization of responsibility to a largerend” (italics ours).32(p156) For Flexner,medicine and other professions werenot yet “fully socialized” and currently“fall short” in this regard.32(p161) Eversociological in his framing, Flexner wasconvinced that any move to a serviceorientation would be as much (or more)driven by the “pressures of publicopinion”32(p156) than by internalmotivations.
Flexner was not alone in this vision of anevolving and altruistically drivenprofessionalism. In his introduction tothe Carnegie Foundation’s Bulletin No. 6,foundation president Henry S. Pritchettnoted,
As the commercial medical schooldisappears, and the profession comes tobe composed of educated men alive to theideal of service to their communities andto humanity, the opportunity to exploitmedicine for gain will disappear. Theyouth who is looking for a fortune, or theparent who seeks for his son aremunerative occupation, should lookelsewhere.34(p xvii)
Another element in Flexner’s views onprofessionalism as a dynamic andtransformative force is his vision of thefull-time academic physician–scientistas a key element in engineeringorganizational change. In his 1924 JAMAappraisal of historical changes in U.S. andEuropean medical education between1909 and 1924, Flexner explicitly labeledthe move to full-time clinical faculty as“professional” in nature.35(p834) He alsocharacterized schools that had movedonly somewhat in this direction as being“partly professionalized.”35(p836) Flexner’smain biographer, Thomas NevilleBonner,36(p1068) concurs, noting thatFlexner’s drive to “create institutionsthat were as free as possible from thecommercial spirit that had dominated somuch of America’s experience in medicaleducation” was, in fact, “taking a strongstand for professionalism and againstgreed in the teaching of medicine.”
Micro-level versus macro-level typesof professionalism
Fourth, and a key element in Flexner’ssystems thinking, was his tendency todifferentiate between the professionalismmanifested by individual practitionersand the professionalism exhibited byorganizations. The latter, for Flexner, hadseparate and distinctive public service
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010290

responsibilities and could just as easilylose sight of those responsibilities ascould individual clinicians.
Professionalism versus commercialism
Finally, in his 1915 talk on social work asa profession, and throughout his writingsas a whole, Flexner maintained thatthere was a sharp cleavage betweencommercialism and professionalism.In terms of his systems thinking,commercialism functions as anenvironmental force, having a negativeimpact on the system of professionalism.
For Flexner, an emphasis on “financialprofit” is antithetical to the spirit ofprofessionalism (“professions may not becultivated for mere profit”).32(p163)
Moreover, the motive of service (in termsof professional status) is a “spiritualstriving from within,” where the rewardsof work are devoted to “impersonalends.”32(p162) Professions strive tominimize “selfish and mercenarymotives” and to “minimize personalprofit” as a motive.32(p159) For Flexner,the two occupations best reflecting anethos of altruism were teaching and socialwork. Medicine, interestingly, was notmentioned in this context, nor was theclergy. Flexner perceived altruism(“unselfish devotion”/“a genuine regardfor the public interest as against itsown”)32(p159) as core to professionalstatus— even as he concluded, based on aconstellation of other criteria, that socialwork was not a profession. For Flexner(this time quoting from his bookUniversities: American, English,German37), “professions have primarilyobjective, intellectual, and altruisticpurposes,” and while they are “not alwaysin fact free from selfish purposes,” theydo hold the “ideal” of being “devoted tothe promotion of larger and nobler endsthan the satisfaction of individualambitions.”37(p30) Professions have “acode of honour.”37(p30) Flexner’sdenouncements of commercialism andits corruptive influences had a frequentpresence both in his writings onproprietary medical education (see, forexample, Bulletin No. 4 or his later“Medical education 1909 –1924”35) andwithin the context of his views on theneed to establish clinical teaching as afull-time academic enterprise, a themethat began to appear more fully in hisfollow-up Bulletin No. 6 for the CarnegieFoundation, Medical Education inEurope.34
Flexner’s conclusion that neitherphysicians nor organized medicine hadbecome fully professional (as of the1920s) brings us to an interestingconundrum. Today, the consensus,within both sociology and organizedmedicine, is that medicine has lost itsservice ethos and/or violated its socialcontract with society and therefore needsto make explicit efforts to regain thattrust and related social status.38 – 42 IfFlexner was correct in identifyingmedicine’s professionalism as nascentand as a force driven by incipientaltruism, then the more contemporaryobservation of loss requires a corollaryconclusion that medicine did, in fact,attain such an ethos of selfless servicesomewhere between Flexner’s time andtoday. If this indeed is the case, then weshould be able to locate this “golden age”somewhere between the 1920s and 1980s.Alternatively, we would have to concludethat any such attainment of altruisticgrace (thus allowing for a fall) has beenmore hyperbole than historical fact—with both sociology and medicine guiltyof attributing more to medicine’s past (interms of some overall service ethic) thanis historically warranted.
Flexner, medical education, and the riseof a new type of professional
As stated in our introduction, a keyelement in Flexner’s plans to reformmedical education was his vision to havemedical schools adopt a new type ofclinical faculty position, the full-timeacademic physician–scientist. Flexnerconsidered this type of physician to bedistinct from the practicing physician—primarily because this type of physicianwould not have to generate an “outside”income by seeing private patients andwould play out the role of altruism in hisor her daily work.
Flexner’s primary connection betweenprofessionalism and medical educationwas through his vision of medicine as asocial good and his fundamental belief inwhat we refer to today as medicine’s “socialcontract” with society.43 For Flexner,physicians were “social instruments,”42(p154)
and medical schools were “public servicecorporations.”24(p ix; 154),44(p49) Given thisstatus, neither had the right, accordingto Flexner, to “exploit” the publicfor personal/organizationalgain.24(p127),42(p49) Correspondingly, andonce again because of medicaleducation’s “social function,”24(p127)
Flexner saw society as being obliged tounderwrite the cost of educating newphysicians. Flexner took this position, inpart, to minimize the possibility thatschools would become dependent ontuition and thus subject to furthercorruption. Flexner also saw tuition as aninsufficient source of revenue to supporta university-based educational mission.Furthermore, and because medicine was“an organ differentiated by society for itsown highest purposes,”24(p19) Flexnerbelieved that society had the right andobligation to set standards for whoshould become physicians. In turn,Flexner believed that no one had thepreordained right to become a physician,nor was this limitation to be viewed asan infringement on individualliberties.24(p155)
Flexner’s professional ideal
A related cornerstone in Flexner’s overallvision of medical education reform washis belief that the clinical faculty membermust become a full-time academicposition. Once again, while this theme ismentioned in Bulletin No. 4, it is morefully developed in Flexner’s later writing.He envisioned this shift in faculty statusmore as a third wave of reform—after theclosing of proprietary medical schools(wave one) and the geographic andadministrative relocation of thoseremaining schools to a university setting(wave two). Thus, it would not beuntil Flexner joined the RockefellerFoundation’s General Education Boardthat he would begin to push for fundingspecific to such positions, first at JohnsHopkins, then at Washington Universityin St. Louis, and then at Yale.45 Onceagain, commercialism was the mainculprit, with then-current clinicaleducators needing to be freed from the“handicap” of having to “make theirliving by practice”45(p176) and of having to“snatch what time they could to devote toclinical research and teaching.”45(p176)
(For further details, see chapters 12and 17 in Flexner’s autobiography, IRemember45). Although Flexner rarelyused the term profession in this context,the full-time clinical faculty memberwas Flexner’s epitome of theprofessional educator. This was theeducator–researcher Flexner envisionedwhen he differentiated betweengraduate/professional education andundergraduate (college) education, thelatter, for Flexner, having a fracturedfocus (trying to be too many things for
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010 291

too many people) and being awash withwhat Flexner saw as strong commercial(e.g., correspondence schools)pressures.37 In addition to pouringmillions of foundation dollars intoencouraging medical schools to adoptthis model, Flexner eventually wouldbuild an educational monument to housethis ideal—the Institute for AdvancedStudy at Princeton, where Flexner wouldbe the first president and where initialfaculty were paid the same salary as thepresident of Princeton University.46
Medical education as a system
Finally, it is important to note thatFlexner was, at root, a systems thinkerwhose work and writings emblemize hiscommitment to analysis that was datadriven, contextually grounded, andcomparatively framed. Although BulletinNo.4 may have been his legacy, itsvoluminous state-by-state listing ofschool-specific data renders it more areport card than an analytic inquiry. Amore complete, comparatively focused,and contextually nuanced presentation ofhis views on medical education thus hadto wait until his underappreciated 1912examination of medical education inEurope,34 his 1925 work on medicaleducation (Medical Education: AComparative Study),47 which heconsidered to be his magnum opus, andhis highly reflective yet analyticallydetailed 1940 autobiography, IRemember.45 In all three of those works,and in a bevy of related publications,Flexner was explicit in recognizing theimportance of both context (e.g., theimportant role of environmental forces)and comparison (e.g., linking reforms inthe United States to models derived fromother countries). In his 60-plus-yearcareer as an educator, Flexner not onlycrisscrossed the United States andCanada but also made multiple visits tomedical schools across Germany, France,England, Austria, Switzerland, Belgium,Holland, Denmark, Norway, andSweden—all in search of a better (i.e.,more comparative) understanding of therelative strengths and weaknesses ofdifferent culturally bound approaches tomedical education. Flexner may have hadhis favorites (e.g., Germany), but he wasnever a sycophant, and rarely would heever sing praises without enumeratingcountervailing weaknesses.
An additional window into Flexner’ssystems-based thinking about medical
education is reflected in his emphasis onconnectedness and his understandingthat changes in one part of medicaleducation would generate (sometimes forthe better and sometimes for the worse)changes in other parts of that system. ForFlexner, a medical school was much likethe human body: “an organic whole[where] to comprehend or remove adisturbance in any part of which requires,first of all, a comprehension of its entirestructure and function: for no part is,strictly speaking, separable from thewhole.”34(p11) Flexner held a similar“organic whole” and interconnected viewof the university. Universities, forFlexner, were dynamic entities,influenced by “the social evolution ofwhich they are part,”34(p4) and thus verymuch a part of the “social fabric of agiven era.”34(p3) Thus, while Flexnersought to create a university system thatwould be more focused than what heviewed as a more chaotic collegeenvironment, Flexner was not an enemyof internal differentiation (on a structurallevel). Complexity was to be embraced solong as this diversity of function wasunified/connected around some commonvision or “unity of purpose.”37(p178 –179)
Nonetheless, Flexner’s obvious distaste ofthe polymorphous undergraduatecampus rendered him vulnerable tocriticisms by later educational leaders,such as Clark Kerr,48 for not seeing “thecreative tensions of divergent forces.”
Flexner’s overall strategy of educationalreform also was relational and decisivelyinteractive in nature. Although he wouldeventually direct several hundred milliondollars toward his reform efforts,46 hewas decisively strategic in disbursingthese funds. In network terms, Flexnersought to create “hubs,” or centers ofinfluence, from which successive waves ofreform would, in his view, spontaneouslyspread. Thus, when Flexner, workingwith the Rockefeller Foundation’sGeneral Education Board, sought totransform the culture of clinical teachingby funding full-time clinical facultypositions, he targeted specific schools,beginning with Johns Hopkins, beforeeventually extending support to 25 of thenation’s then 66 four-year schools.Furthermore, and in search of leveraginghis dollars, Flexner was quite attentive toother relational variables such asgeographic location and the necessity tofund public as well as private institutions.
Finally, even though Flexner was aproponent of strategic planning and order,he was no determinist. Flexner’s tripartitetypology of medical schools(clinical—France and England, university—Germany, and proprietary—America) wasunderscored by his belief that each nationaltype was the product of “circumstances,”whose starting point was a “matter ofchance.”47(p14) Flexner saw no “evidence ofinitial planning” across his major types ofmedical education and no “proof thatnational genius originally selected one typerather than another.”47(p14)
A Theoretical Model forResearching Professionalism
As we have noted, Flexner offered a uniqueapproach to professionalism. He saw it as acomplex system comprising competingtypes, taking place at multiple levels, andthreatened by the environmental forces ofcommercialism, particularly within theorganization and practice of medicaleducation. Drawing on the uniquenessof this approach and its importance forthe reforms he suggested, we seek hereto outline an agenda for studyingprofessionalism in complex systemsterms. We begin with a definition ofprofessionalism as a complex system.
Professionalism as a complex system
Those familiar with complexity sciencehave encountered the almoststereotypical litany of characteristicssometimes used when scholars define orredefine a topic as a complex system. Thislitany includes terms such as emergent,self-organizing, agent-based, operating-far-from-equilibrium, chaotic, dynamic,nonlinear, sensitive to initial conditions,stochastic, autopoietic, network-based, andso forth.49,50 This proliferation ofdescriptors, however, often results fromthe quick or uncritical application ofcomplexity science to a topic, as if themere evocation of these termsautomatically made that topic applicableto a complex systems analysis.51 AsCilliers50 and others (e.g., Byrne52;Capra49,53) explain, science is stillstruggling to articulate what makessomething a complex system, the generalargument being that the only real answerwill come slowly and methodologicallyas researchers roll up their sleeves andengage in the nose-to-the-grindstonelabor of real empirical inquiry.
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010292
Our definition of professionalism as acomplex system comes from several yearsof empirical sleeve-rolling-up. As such, itseeks to avoid a normative, or a this-is-what-it-should-be, approach to adefinition. Instead, our definition isgrounded in the examination of twoprimary sets of data: (1) the fact thatphysicians carry out their work based onhow physicians as a group define whatthey do as professionals, and (2) theevolution of modern-day medicine’s ownprofessionalism movement and howorganized medicine has sought to advancea certain normative framework within thatmovement, along with an analysis ofconsequential system reactions to thatframing.
For us, there are several major ways inwhich professionalism acts like a complexsystem.
• Medical professionalism comprisesseveral competing types.
• As we will explain below,professionalism seems to havesplintered into a system of severalcompeting types. Understandingthese types requires a case-based,comparative approach to the analysisof professionalism.
• The differing types of professionalismseem to form an emergent system.Without any external guidance orinternal oversight, the different types ofprofessionalism have been self-organized, without the organizers’awareness, into an emergent system.What is particularly interesting aboutthis system is that those individualswho organize specific types ofprofessionalism often are constrainedby local knowledge, an example being alimited awareness of the other types orthe conflicting aspects of those types.
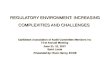
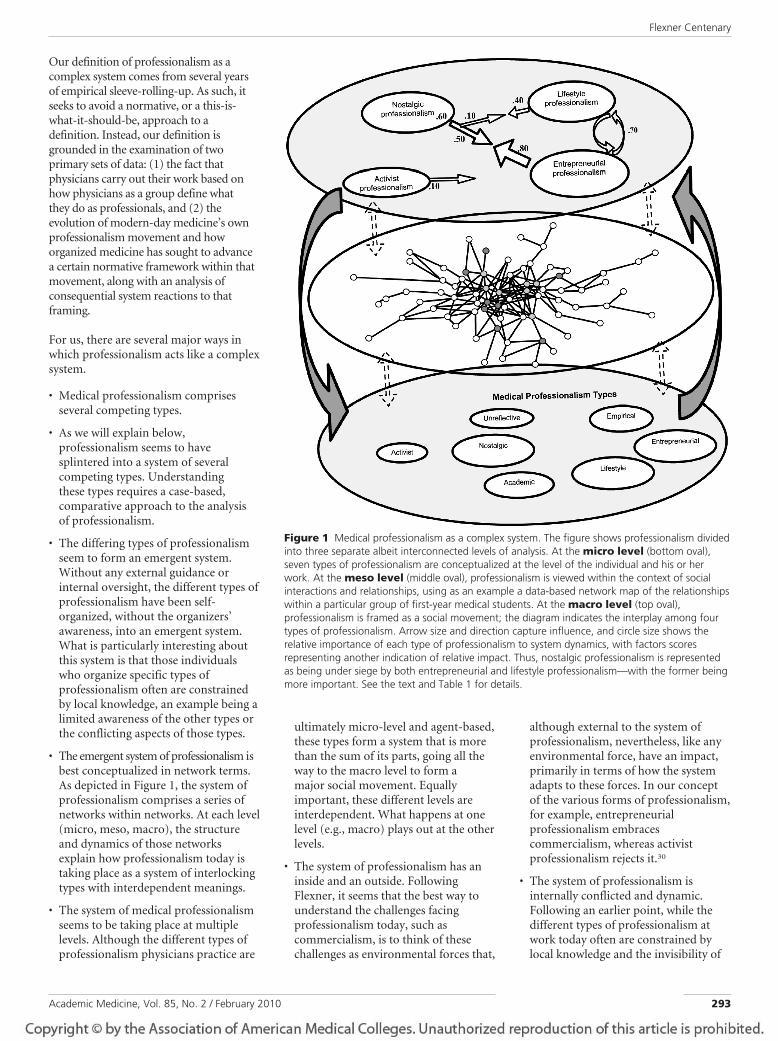
• The emergent system of professionalism isbest conceptualized in network terms.As depicted in Figure 1, the system ofprofessionalism comprises a series ofnetworks within networks. At each level(micro, meso, macro), the structureand dynamics of those networksexplain how professionalism today istaking place as a system of interlockingtypes with interdependent meanings.
• The system of medical professionalismseems to be taking place at multiplelevels. Although the different types ofprofessionalism physicians practice are
ultimately micro-level and agent-based,these types form a system that is morethan the sum of its parts, going all theway to the macro level to form amajor social movement. Equallyimportant, these different levels areinterdependent. What happens at onelevel (e.g., macro) plays out at the otherlevels.
• The system of professionalism has aninside and an outside. FollowingFlexner, it seems that the best way tounderstand the challenges facingprofessionalism today, such ascommercialism, is to think of thesechallenges as environmental forces that,
although external to the system ofprofessionalism, nevertheless, like anyenvironmental force, have an impact,primarily in terms of how the systemadapts to these forces. In our conceptof the various forms of professionalism,for example, entrepreneurialprofessionalism embracescommercialism, whereas activistprofessionalism rejects it.30
• The system of professionalism isinternally conflicted and dynamic.Following an earlier point, while thedifferent types of professionalism atwork today often are constrained bylocal knowledge and the invisibility of
Figure 1 Medical professionalism as a complex system. The figure shows professionalism dividedinto three separate albeit interconnected levels of analysis. At the micro level (bottom oval),seven types of professionalism are conceptualized at the level of the individual and his or herwork. At the meso level (middle oval), professionalism is viewed within the context of socialinteractions and relationships, using as an example a data-based network map of the relationshipswithin a particular group of first-year medical students. At the macro level (top oval),professionalism is framed as a social movement; the diagram indicates the interplay among fourtypes of professionalism. Arrow size and direction capture influence, and circle size shows therelative importance of each type of professionalism to system dynamics, with factors scoresrepresenting another indication of relative impact. Thus, nostalgic professionalism is representedas being under siege by both entrepreneurial and lifestyle professionalism—with the former beingmore important. See the text and Table 1 for details.
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010 293

other types at work, these types are,nonetheless, in competition with oneanother. For example, one of thebiggest challenges facing nostalgicprofessionalism today (see below) isits adherents’ almost completeignorance that there are other types ofprofessionalism at work—some ofwhich are diametrically opposed to thereforms these true believers are tryingto ensure.
• Finally, the system of professionalism issituated within a larger series ofsystems. Medical professionalism doesnot take place in a vacuum. FollowingFlexner, it is situated within a widersocial context, which can beconceptualized as a series of largersystems. Such systems include medicaleducation, clinical practice, the healthcare system, Wall Street and the U.S.economy, the federal government, andvarious other sociopolitical institutions.
A tripartite model for studying thecomplexities of professionalism
Given this complexity-grounded view ofprofessionalism, how does one study it?As shown in Figure 1, we have found thatthe best approach is to conceptualizeprofessionalism as a complex systemdivided into three separate albeitinterconnected levels of analysis.
At the micro level, we conceptualizeprofessionalism at the level of theindividual and his or her work. At themeso level, we view professionalismwithin the context of social interactionsand relationships. At the macro level, weframe professionalism as a socialmovement. In turn, differentmethodological tools are employedwithin each of these levels: historicalanalysis being one such possibility at themacro level, the new science of networksat the meso level, and cluster and factoranalysis at the micro level. Whereasinvestigators may focus on elementsparticular to a given level, these elementsultimately function within an overall,interdependent, and dynamic “field ofrelations.”54 At the same time, and asshown in Figure 1, factors and forcestaking place at one level haveimplications for factors and forces atother levels. In short, an overall system ofprofessionalism exists across all threelevels. This system, in turn, functions as asub- or corollary system within stillbroader complexes such as medical
education or the health care deliverysystem.
In the following subsections, we brieflyreview some of these interrelationships,first by examining issues of physicianwork at the individual (micro) level and,second, by scrutinizing the dynamics oforganized medicine’s modern-dayprofessionalism movement at the societal(macro) level. At the micro/individuallevel, we explore how variations in theway physicians organize their workprovide us with insights into a framing ofprofessionalism far more complex thanFlexner’s dual interplay of altruistic andcommercial forces. Similarly, anexamination of organized medicine’snow 25-year professionalism movement31
yields similar complexities. Across thesetwo levels, we highlight how theemergence of a particular type ofprofessionalism (“nostalgic”),30 alongwith the rise of two flash points (COIs18–21,55
and duty hours14 –17), capture the host ofpressures facing the traditional renderingof professionalism. Although we will notfully develop any of these three dynamics,we do lay out how their intersectionscapture the complexities underscoringprofessionalism as a modern social force.Finally, and to round out our micro,meso, and macro schema, we offer a briefrationale for how professionalism mightbe explored at the meso level usingnetwork analysis.
We end our article withrecommendations showing whyprofessionalism must be treated as acomplex system if professionalism is tofunction as a positive force for change in21st-century medicine.
Micro-level professionalism
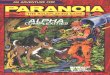
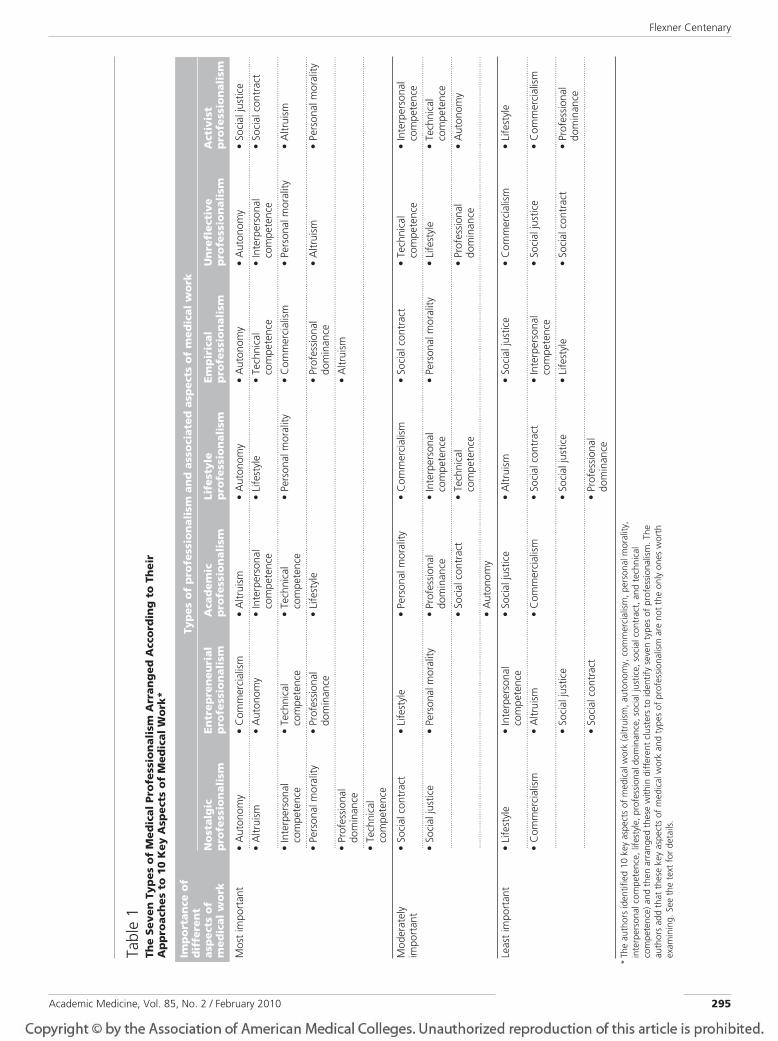
When contemporary physicians organizetheir work, they do so within an array offorces far more tangled than the simplealtruism– commercialism dichotomy sooften embedded within contemporarydiscussions of medical professionalismand its discontents. So what does thismore complex dynamic look like? In oneexercise,30 we identified 10 key aspects ofmedical work (altruism, autonomy,commercialism, personal morality,interpersonal competence, lifestyle,professional dominance, social justice,social contract, and technicalcompetence) and then arranged theseapproaches to work within differentclusters to identify seven types of
professionalism (entrepreneurial,empirical, lifestyle, unreflective,academic, activist, and nostalgic—seeTable 1 for more details about thesetypes). We make no claim that these keyaspects of medical work are the only onesworth examining. Nor do we insist thatthese seven types of professionalism (ortheir labels) are similarly sacrosanct.Indeed, since our original inquiries intothe nature of professionalism,30 we havefound three of these types (nostalgic,entrepreneurial, lifestyle) to be far moresocially active and visible than theremaining four. At the same time, andsince delving into Flexner’s writings, wealso have discovered parallels betweenFlexner’s conceptualization of the full-time academic physician–scientist andtwo (academic and empirical) of ourremaining four types of professionalism.Likewise, it has been affirming to studymedicine’s modern-day professionalismmovement at the macro level and findtypes of professionalism at work similarto those uncovered during micro-levelanalysis.
Finally, it has been gratifying to observehow a particular type of professionalismat the macro level—for example, theembedding of nostalgic professionalismwithin institutionalized statements ofprofessional ideals— can also be foundwithin coursework or accreditationstandards at the meso level and/or withinstudent identities at the micro level. Andthen, reversing direction and starting atthe micro level, it is fascinating toexplore how concepts of nostalgicprofessionalism at that level cancombine with countervailing conceptsof professionalism such as lifestyleprofessionalism and thus beginto evolve into new forms ofprofessionalism within studentinteractions (meso), ultimately toappear at the macro level within a givenflash point such as duty hours.14 –17 Inshort, we have a two-way street, withvarious types of professionalismtrickling down and bubbling up at thesame time (dual influence), and we seesimilar concepts (e.g., of nostalgic orlifestyle professionalism) behaving verydynamically at each of the levels.
It also has been fascinating to see hownotions of balance, lifestyle, andresponsibilities to self and family arebeing reframed within the context ofprovider fatigue, patient safety, quality
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010294
Tabl
e1
The
Seve
nTy
pes
of
Med
ical
Pro
fess
ion
alis
mA
rran
ged
Acc
ord
ing
toTh
eir
Ap
pro
ach
esto
10K
eyA
spec
tso
fM
edic
alW
ork
*
Imp
ort
ance
of
dif
fere
nt
asp
ects
of
med
ical
wo
rk
Typ
eso
fp
rofe
ssio
nal
ism
and
asso
ciat
edas
pec
tso
fm
edic
alw
ork
No
stal
gic
pro
fess
ion
alis
mEn
trep
ren
euri
alp
rofe
ssio
nal
ism
Aca
dem
icp
rofe
ssio
nal
ism
Life
styl
ep
rofe
ssio
nal
ism
Emp
iric
alp
rofe
ssio
nal
ism
Un
refl
ecti
vep
rofe
ssio
nal
ism
Act
ivis
tp
rofe
ssio
nal
ism
Mos
tim
port
ant
•A
uton
omy
•C
omm
erci
alism
•A
ltrui
sm•
Aut
onom
y•
Aut
onom
y•
Aut
onom
y•
Soci
alju
stic
e...
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
•A
ltrui
sm•
Aut
onom
y•
Inte
rper
sona
lco
mpe
tenc
e•
Life
styl
e•
Tech
nica
lco
mpe
tenc
e•
Inte
rper
sona
lco
mpe
tenc
e•
Soci
alco
ntra
ct
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Inte
rper
sona
lco
mpe
tenc
e•
Tech
nica
lco
mpe
tenc
e•
Tech
nica
lco
mpe
tenc
e•
Pers
onal
mor
ality
•C
omm
erci
alism
•Pe
rson
alm
oral
ity•
Altr
uism
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Pers
onal
mor
ality
•Pr
ofes
siona
ldo
min
ance
•Li
fest
yle
•Pr
ofes
siona
ldo
min
ance
•A
ltrui
sm•
Pers
onal
mor
ality
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Prof
essio
nal
dom
inan
ce•
Altr
uism
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Tech
nica
lco
mpe
tenc
e
Mod
erat
ely
impo
rtan
t•
Soci
alco
ntra
ct•
Life
styl
e•
Pers
onal
mor
ality
•C
omm
erci
alism
•So
cial
cont
ract
•Te
chni
cal
com
pete
nce
•In
terp
erso
nal
com
pete
nce
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Soci
alju
stic
e•
Pers
onal
mor
ality
•Pr
ofes
siona
ldo
min
ance
•In
terp
erso
nal
com
pete
nce
•Pe
rson
alm
oral
ity•
Life
styl
e•
Tech
nica
lco
mpe
tenc
e...
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
•So
cial
cont
ract
•Te
chni
cal
com
pete
nce
•Pr
ofes
siona
ldo
min
ance
•A
uton
omy
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Aut
onom
y
Leas
tim
port
ant
•Li
fest
yle
•In
terp
erso
nal
com
pete
nce
•So
cial
just
ice
•A
ltrui
sm•
Soci
alju
stic
e•
Com
mer
cial
ism•
Life
styl
e
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Com
mer
cial
ism•
Altr
uism
•C
omm
erci
alism
•So
cial
cont
ract
•In
terp
erso
nal
com
pete
nce
•So
cial
just
ice
•C
omm
erci
alism
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...•
Soci
alju
stic
e•
Soci
alju
stic
e•
Life
styl
e•
Soci
alco
ntra
ct•
Prof
essio
nal
dom
inan
ce...
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
•So
cial
cont
ract
•Pr
ofes
siona
ldo
min
ance
*Th
eau
thor
sid
entif
ied
10ke
yas
pect
sof
med
ical
wor
k(a
ltrui
sm,a
uton
omy,
com
mer
cial
ism,p
erso
nalm
oral
ity,
inte
rper
sona
lcom
pete
nce,
lifes
tyle
,pro
fess
iona
ldom
inan
ce,s
ocia
ljus
tice,
soci
alco
ntra
ct,a
ndte
chni
cal
com
pete
nce)
and
then
arra
nged
thes
ew
ithin
diff
eren
tclu
ster
sto
iden
tify
seve
nty
pes
ofpr
ofes
siona
lism
.The
auth
ors
add
that
thes
eke
yas
pect
sof
med
ical
wor
kan
dty
pes
ofpr
ofes
siona
lism
are
nott
heon
lyon
esw
orth
exam
inin
g.Se
eth
ete
xtfo
rdet
ails.
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010 295

of care, and better models of medicaleducation (see below). Taken as a whole,professionalism is a fluid and evolvingpicture, and the presence of thesealternative dynamics sometimes is lostwhen a dominant stakeholder, such asorganized medicine, seeks to advance aparticular and privileged representationof professionalism (e.g., nostalgic) thatlimits alternative framings. As we willillustrate below, some of the bestevidence of competing types can befound at the margins of medicine’smodern-day professionalism movementwhen flash points such as COIs or dutyhours appear on the scene.
In Table 1, we depict how differentways of organizing work lead to differenttypes of professionalism at the micro(individual) level. The underlyingmethodology and data sources aredetailed elsewhere.30
In this table, we summarize seven typesof professionalism (academic, activist,empirical, entrepreneurial, lifestyle,nostalgic, unreflective) along with howthey prioritize their respective workarrangements. For example, nostalgicprofessionals highly value autonomy andaltruism in their work, with lifestyle andcommercialism viewed as less important.Conversely, activist professionals highlyvalue social justice and the socialcontract, with commercialism andprofessional dominance occupying lessimportant positions. Parenthetically, itwas only after developing all seven typesthat we discovered how the relativerankings of activist professionals seemedmore faithful to the overall ideals ofprofessionalism than what actually wasbeing promulgated under the guiseof nostalgic professionalism. For example,note the difference in rankings fornostalgic versus activist professionalismaround the issues of professionaldominance versus social justice.Meanwhile, the kind of professionalismoften reflected in the career decisions oftrainees and younger physicians (e.g.,lifestyle) represents a differentconfiguration from that of nostalgicprofessionalism, even though both sharea ranking of autonomy (something wesee as changing with a diminishment inthe value of autonomy for lifestyleprofessionals). Finally, we includeempirical professionalism (ournomenclature for the physician–scientistresearcher) in Table 1 to highlight the
place of commercialism in this particularconstellation of work orientations.Flexner would not be pleased to seecommercialism ranked so highly.
Figure 1 presents these seven types atthe micro level. Although we did notreproduce the relationships that existacross these types, it is important to notethat these seven types do not exist asisolated domains of influence. Rather,they interact in a flurry of competinginterests as different configurations ofprofessionalism jockey for the hearts,minds, and professional identities ofphysicians.30 We provide examples ofthese interactions when we move to ouranalysis of medicine’s professionalismmovement at the macro level.
Macro-level professionalism
Although there was no “crisis ofprofessionalism” during Flexner’slifetime, there were organized efforts bymedicine to secure its boundaries againstcompeting occupations via restrictivelicensing laws and medical practice actswithin the hallways of state legislaturesand the conference rooms of statemedical boards.38 For Larson,56 thiswas medicine’s early-20th-century“professionalism project.” Medicine’smodern-day professionalism movementdiffers from those earlier efforts in thatthe motive-of-record then (“protect thepublic”), although possibly self-serving,was something quite different from the“recapturing of public trust” motives/language defining medicine’s more recentand ongoing professionalism efforts.Furthermore, the initiatives of Flexner’sera sought to establish the profession’sautonomy (e.g., by limiting the influenceof “outsiders”) and to secure dominanceover other health occupations—all quitedifferent from the current rhetoric ofhaving medicine become more “patient-centered,” “team-based,” and“interprofessional.”57–59
Aside from an occasional journalreference to the threat of commercialcorruption, medicine’s own sense of itsstatus as a profession during the middlehalf of the 20th century was moreassumed than questioned. Physicianswere professional by virtue of theirtraining. There were no professionalismcourses, nor were there any formallylabeled professionalism initiatives. Nonewere needed. That was a different timeand a different professionalism.
All that began to change in the late 1980sas journal editors and other opinionleaders such as George Lundberg,60,61
Arnold Relman,62,63 and JeromeKassirer64 began to publish a phalanx ofeditorials and commentaries concludingthat medicine had violated its socialcontract with society, lost public trust,and jettisoned its professional moorings,and that therefore it was necessary forphysicians to rediscover and recommitthemselves to the traditional principles ofmedical professionalism.31,65 These criesof concern were followed, in successivewaves, by calls to define and assessprofessionalism, to develop andimplement professionalism curriculawithin medical schools, and toinstitutionalize core principles withincodes, charters, and accreditationstandards. Scholarly journals, particularlyAcademic Medicine, and medicalorganizations such as the AmericanBoard of Internal Medicine and theAssociation of American MedicalColleges took the lead in organizingspecial conferences and other initiatives.
A key element in this movement was theemergence of a particular and highlyprivileged type of professionalism, a typewe have labeled elsewhere as “nostalgicprofessionalism.”30 As mentioned earlier,the call for providers to “rediscover” and“reconnect” themselves to “traditionalmedical values” was very Flexnerian inthat all of these calls identified altruism ascore to professionalism while tagging“commercialism” as the single overridingthreat to that call. Key players in this riseinclude Herbert Swick’s66 highlyinfluential definitions of professionalism,along with the emergence of variousprofessionalism codes, the most widelycited being the physician charter, aproduct of an organizational consortiumled by the American Board of InternalMedicine.67 Altruism was the first ofSwick’s “nine behaviors ofprofessionalism,” and Swick’s definition(“physicians subordinate their owninterests to the interest of others”)proved as popular with the medicalestablishment (Swick’s definitions werekey in the wordings of many codes andstatements of professionalism principles,including the charter) as it wasunpopular with students (who did notlike the notion of subordinating theirown interests).68 Similarly, the charter ledwith its own altruism statement(“primacy of patient welfare”) as well as
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010296

warnings about “market forces” in bothits preface and summary. Thesenostalgically oriented depictions ofprofessionalism also began to appear inmedical schools and residencycoursework, professionalism assessmenttools,69 –71 core competencies at theresidency level,72 and accreditationstandards (e.g., MS-31-A) forundergraduate training.73
All these traditionally focusedprofessionalism activities were viewed asquite rational and necessary—to insiders.After all, the very identification of theproblem (a loss of professionalism), thecause of this threat (commercialismand market forces), and the necessarysolution (having physicians rediscoverand recommit) practically demandedthat organized medicine perceiveprofessionalism as something groundedin the practices and principles of anearlier (and structurally less chaotic) era.In turn, when problems or schismsappeared, this logic also required that“causes” be located on the micro levelwithin individuals and their practices,such as those in the rank and file wholacked nostalgic professionalism’s corevalues; not-yet-fully socialized students;inadequate teaching tools; incompleteassessment practices; and/or inadequateenforcement of “professional standards.”That there might be other ways ofthinking about professionalism did notfit into this overall mindset. Instead, arather narrow and almost trenchantconception of professionalism battled on.
Within a decade of its launching,undeniable schisms began to appear,particularly as these tradition-ladenconceptions of what it meant to be aprofessional began to clash withalternative renderings. Medical students,for example, were uncomfortable withthe emphasis on altruism or withprofessionalism codes that applied totrainees but not to faculty. Students didnot like the idea that they might have tosubordinate themselves to the needs ofothers. They viewed calls to “selflessservice” as a prescription for burnout, asjust another way for higher-ups to getthem to work harder or for manipulativepatients to take advantage of them.68
As coursework about professionalismbecame more formalized, students foundthemselves trapped within a hiddencurriculum, as lessons taught in the
“classroom” proved to be inconsistent orcontradictory to the more tacit lessonsthey were learning in clinic and on thewards.74 –76 Cynicism oozed and angerbubbled.77–79 Students began to pushback, treat their professionalismcurriculum as “just another course” (i.e.,“just pass the test”), evince strategies ofevasion or duplicity, and/or adopt thefacade of chameleon socialization.80
Students accused faculty of hiding behindthe power of hierarchy and (rightly insome instances) of generating studentcodes while they refused to apply thesame standards and principles tothemselves. Faculty, feeling bewildered,defensive, and angered, began to labelstudents as self-centered slackers.81– 83
Generational rifts widened.82
Meanwhile, and somewhat outside themedical school gates, additional points oftension began to erupt. The first wasCOIs.18 –21 Although COIs have alwaysbeen a sentinel issue within medicine—after all, Flexner’s concerns aboutproprietary medical schools and thegeneral issue of commercialism were, atheart, COI issues—it was not until thebeginning of the 21st century that issuesmoved beyond the particulars ofphysician referrals and ownership ofmedical facilities to a broader call bymedical leaders for academic healthcenters and other organizational entitiesto divest themselves from a litany ofindustry gifts and inducements that hadbegun to engulf medical work.19 Afirestorm ensued. Some insiders urged aban.84,85 Others argued that relations withindustry should be “managed.”86 Ofparticular interest within this ongoingdebate was the infusion of an organizedstudent presence when the AmericanMedical Student Association decided toissue a “report card” to grade (A throughF) medical schools on the basis of theirCOI policies.55 There has beenconsiderable organizational squirming(driven by press coverage) since manyschools received an initial grade of F.
Although COI is not the onlyprofessionalism issue, it is a signatureone, given the altruism-infused issue ofwho is being served, provider or patient.In turn, the debate between calls to banversus to manage COIs is, at root,a debate about the meaning ofprofessionalism and how medicine’sprofessionalism movement shouldcontinue to evolve. A similar debate
(although one we will not explore here)focuses on continuing medical education(CME) and its long-standing reliance onindustry funding. Here, too, calls to banversus to manage industry funding ofCME are, in fact, a debate over themeaning of professionalism. Within all ofthese conflicts, Flexner’s warnings about“proprietary” medical education seemwell founded and prophetic.
A second flash point is resident dutyhours.14 –17,87 Once again, the historyand particulars will not be reviewed here,but where COI captures the tensionbetween commercial and nostalgicprofessionalism, duty hours reflects thetension between nostalgic and lifestyleprofessionalism—the former builtaround the issue of physician autonomyand the “right to make a living” andthe latter around the issues of patientsafety, student supervision, and the“appropriate” pace and structure ofmedical work.88 Both duty hours andCOIs continue to receive extensive mediacoverage, with COI reports highlightingphysician “greed,”89 while duty hourscoverage depicts sleep-addled andunsupervised residents who placedpatients at risk.90 Across all, medicine’sinsistence that it is a profession in theservice of others is placed under adisbelieving lens.
In Figure 1, we provide a brief renderingof the interplay among four types ofprofessionalism (activist, entrepreneurial,lifestyle, and nostalgic) at the macro level.Arrow size and direction captureinfluence, and circle size shows therelative importance of each type ofprofessionalism to system dynamics, withfactor scores representing anotherindication of relative impact. Thus,nostalgic professionalism is representedas being under siege by bothentrepreneurial and lifestyleprofessionalism—with entrepreneurialprofessionalism more important thanlifestyle professionalism. After all, thevariety of work/lifestyle options availableto physicians is facilitated, in part, by theincrease in the types of employmentstructures (e.g., part-time, job sharing,locum tenens) generated byentrepreneurial forces. Meanwhile, therole of activist professionalism is moreperipheral (at least to date) to the clashesbetween nostalgic professionalism,entrepreneurial professionalism, andlifestyle professionalism. Furthermore,
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010 297

and when exerted, we see it occurringmore in entrepreneurial professionalismthan in lifestyle professionalism.
Meso-level professionalism
Although the oral culture of medicaleducation is rife with stories aboutstudents who managed to “sail through”their training without attending classand/or were able to “game” their way bymanipulating faculty during theirclerkship and residency experiences,becoming a physician is a highly socialactivity marked by considerableinteraction among and between trainees,faculty, and patients. Efforts to create aformal curriculum of professionalismmay be a pedagogical initiative-de-jour,but students have always “augmented”these faculty-centric efforts with a host ofinformal, tacit, and often idiosyncraticlearning experiences (the informal,hidden, null, etc., curricula), which formthe cultural backbone of medical practiceand of the medical school as a socialsystem.91
To date, efforts to untangle the structure,process, context, and impact of theseinformal/hidden types of learning and, inturn, how they interact with the formalcurriculum, have been hampered by thelack of conceptual and methodologicaltools that would allow researchers toanalyze the various components ofstudent learning and their interactions.Part of the problem has been thetendency within medical educationresearch to frame problems and theiranalysis in terms of individuals and theircharacteristics. Thus, although anynumber of social factors (e.g., age, race,sex, social status, popularity) mayfunction as key explanatory variables insome investigations of medical education,they remain “attached” to individuals. Asa consequence, we may learn somethingabout factors that predict career choice,the delivery of quality of care, or evenprofessionalism— but with theunderlying model treating students asdiscrete, and fundamentally isolated,entities.
The new science of social networks92–94
challenges this particular depiction andasks that we consider models that are notonly dynamic but also grounded inrelationships/interactions. Thus,although we might want to learn whattypes of students trigger professionalismwarning flags during training or in
practice, we also want to know wherethese students “fit” within the socialnetworks of their peers. After all, we willhave completely different sociologicalpictures depending on whether these“unprofessional few” (e.g., studies ofstudent “lapses” almost always identifysuch students as a “small minority”)function as key nodes, or hubs, withintheir webs of relations or whether,instead, they are peripheral (e.g., fringe)members of their communities. Similarly,we could map how national medicalorganizations (specialty groups,associations, etc.) work together (or not)to influence the overall direction ofmedicine’s modern-day professionalismmovement. To do so, however, wouldrequire that we locate our explanationswithin the interactions of systemelements rather than within thecharacteristics of system pieces. Anotherexample focuses on students and theirrole models. Although it would be wrongto minimize the importance of rolemodels and mentors as a key element inprofessional development, the factremains that neither students nor rolemodels function within isolated dyads.A more robust understanding ofprofessionalism requires that we movebeyond these couplets of influence andinto the networks of influence that engulfthem.
Another example of how networkanalysis can be employed to betterunderstand the overall learningenvironment of medical students is themove within medical schools to formlearning communities and academicsocieties.95 Learning communities areformal structures designed to linkstudents, usually across years of training,and to facilitate the education andsocialization processes. That Student Xhas been assigned to LearningCommunity Y, and that this cohort isformally brought together in certainways, are all structural conditions of thesituation. But to what import? Dostudents “stay” within these groups?Perhaps these formal communities existon paper but have very little functionalpresence otherwise? Perhaps studentsform “outside” and more informalnetworks of peers for the purposes ofstudy and/or social interactions? Socialnetwork analysis can begin to addressthese issues and, in turn, build bridges ofunderstanding between what takes placeat the interface between the formal and
the informal/hidden curricula.96 As notedby Haidet and Stein, “there is littleempirical work in the medical literaturethat explores the development andmeaning of relationships in medicaleducation.” For those authors, and for us,“relationships are a critical mediatingfactor in the hidden curriculum.”97(pS16)
To date, network analysis has not beenemployed to examine medical education.Nonetheless, this conceptual frameworkand related empirical tools are being usedto understand a variety of clinical andbasic science research questions includingcolorectal cancer screening,98 healthinequalities,99 obesity,100 and smoking.101
The network map superimposed inFigure 1 at the meso level is data basedand depicts the relationships that existwithin a particular group of first-yearmedical students. Although the scale usedhere makes particulars difficult to discernand renders impossible the inclusion ofunderlying statistics of connectednessand node centrality, there are certainobvious patterns worth noting. Somestudents, for example, are more linkedthan others (either through their actionsor the actions initiated by classmates),with a few being highly linked “hubs”whose absence—if removed from thenetwork—would threaten the structuralintegrity of the group. How this networkchanges over time as students continuetheir training would make for afascinating study and a more texturedunderstanding of medical education andits effects.
In sum, social networks matter, andmedical students operate within webs ofinterrelationships whether the issue athand is learning pathophysiology, clinicalskills, or professionalism.102 The structureand dynamics of these networks need tobe better understood.
Conclusions
Flexner’s universe contained two types ofprofessionals. The first, incomplete andevolving, was his physician clinician. Thesecond was his full-time academicphysician–scientist. Flexner viewed thisfirst type as the product of changingsocial forces. He viewed the second as aforce for social change, as core to therestructuring of medical education, andtherefore something that needed to beinserted—with financial inducements if
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010298

necessary—into the structure of themedical school.
Since Flexner’s heyday, the practice ofclinical medicine, the content andorganization of medical education,and even how we conceptualizeprofessionalism have become morenuanced and complex. For Flexner andhis contemporaries, professionalism wassomething that emerged within therollback of commercial influences.Although there were other elements inFlexner’s six-part definition of profession(see his statement quoted earlier), theprofessionalism– commercialismconundrum was his crucible. Issues oflifestyle, or professional dominance (inthe way we think about these now), werenot a part of his conceptual equation.
Today, medical practice, medicalprofessionalism, and medicine’srelationship with society are morecomplex. Conceptions that servedFlexner well have lost their robustness.What remains relevant, however, isFlexner’s systems-oriented approach tothe interplay of social forces and socialchange, including professionalism. Thetension between professionalism andcommercialism continues, but it is notthe same (structural) tension as it was inFlexner’s era (after all, medicine has yetto adequately define what is and what isnot “unprofessional commercialism”).65
Nor is this the only tension. We havereviewed issues of lifestyle andentrepreneurial professionalism (in thecontext of duty hours and COIs), and inclosing we offer readers yet one moretype for their reflection—professionaldominance. Although not yet at the levelof a flash point (like duty hours andCOIs), calls to bridge relations amonghealth professions, to create a true team-based practice (no “captain of the ship”here), and to construct interdisciplinarytraining across the health occupationshave surged in recent years.57,103
Nonetheless, these calls, particularly for ateam-based approach to patient care,have been around for decades. So what isdifferent today? Complexity. The healthcare workforce has become more highlydifferentiated. Physicians truly are “oneof many.” Traditional definitions ofprofessionalism, within both medicineand sociology, have identifiedprofessional dominance as key tomedicine’s professional status (althoughmedicine’s definitions have been more
normative, with sociology’s being moredescriptive). Nonetheless, a top-downhierarchical model of work (as reflectedin the professional dominance model)no longer seems to capture thesecomplexities— even as the underlyingcomplexity of medical work, theuncertainties of knowledge and itsapplication to patient care, and thetremendous variabilities that exist withthe patient population continue todemand some measure of individualexpertise and discretionary decisionmaking. What remains an underlyingtruism within all this is that the debatesover workforce issues, like those ofpatient safety, COIs, duty hours, andothers are debates about the nature andmeaning of medical professionalism.How organized medicine responds to theproblems of internal integration (e.g.,increasing subspecialization) and to thechallenges of external adaptation (e.g.,the buyer’s revolt) will have a great dealto say about the nature and sustainabilityof medical professionalism in the future.Traditional conceptions of what it meansto be a professional—as a stand-aloneentity—are neither systematically realisticnor ultimately sustainable. Like it or not,we remain awash in a sea of complexities.
Funding/Support: None.
Other disclosures: None.
Ethical approval: Not applicable.
References1 Epstein AM. Health care in America—Still
too separate, not yet equal. N Engl J Med.2004;351:603– 605.
2 Fiscella K, Franks P, Gold MR, Clancy CM.Inequality in quality addressingsocioeconomic, racial, and ethnic disparitiesin health care. JAMA. 2000;283:2579 –2584.
3 Marmot M. Inequalities in health. N EnglJ Med. 2001;345:134 –136.
4 Smedley BD, Stith AY, Nelson AR. UnequalTreatment: Confronting Racial and EthnicDisparities in Health Care. Washington, DC:The National Academies Press; 2003.
5 Longo DR, Hewett JE, Ge B, Schubert S. Thelong road to patient safety: A status reporton patient safety systems. JAMA. 2005;294:2858 –2865.
6 Moussa ID. The practice of interventionalcardiovascular medicine: “Evidence-based”or “judgment-based?” Catheter CardiovascInterv. 2008;72:134 –136.
7 Rosenstock L, Lee LJ. Attacks on science:The risks to evidence-based policy. Am JPublic Health. 2002;92:14 –18.
8 Traynor M. Indeterminacy and technicalityrevisited: How medicine and nursing haveresponded to the evidence based movement.Sociol Health Illn. 2009;31:494 –507.
9 Blumenthal D. Controlling health careexpenditures. N Engl J Med. 2001;344:766 –769.
10 Hauer KE, Durning SJ, Kernan WN, et al.Factors associated with medical students’career choices regarding internal medicine.JAMA. 2008;300:1154 –1164.
11 Morrison G. Mortgaging our future—Thecost of medical education. N Engl J Med.2005;352:117–119.
12 DeAngelis CD. Commitment to care for thecommunity. JAMA. 2009;301:1929 –1930.
13 Rosenblatt RA, Andrilla HA. The impact ofU.S. medical students’ debt on their choiceof primary care careers: An analysis of datafrom the 2002 medical school graduationquestionnaire. Acad Med. 2005;80:815– 819.
14 Fletcher KE, Underwood W III, Davis SQ,Mangrulkar RS, McMahon LF, Saint S.Effects of work hour reduction on residents’lives: A systematic review. JAMA. 2005;294:1088 –1100.
15 Nuthalapaty FS, Carver AR, Nuthalapaty ES,Ramsey PS. The perceived impact of dutyhour restrictions on the residencyenvironment: A survey of residency programdirectors. Am J Obstet Gynecol. 2006;194:1556 –1562.
16 Ratanawongsa N, Bolen S, Howell EE, KernDE, Sisson SD, Larriviere D. Residents’perceptions of professionalism in trainingand practice: Barriers, promoters, and dutyhour requirements. J Gen Intern Med. 2006;21:758 –763.
17 Reed DA, Levine RB, Miller RG, et al.Impact of duty hour regulations on medicalstudents’ education: Views of key clinicalfaculty. J Gen Intern Med. 2008;23:1084 –1089.
18 Angell M. The Truth About the DrugCompanies: How They Deceive Us andWhat to Do About It. New York, NY:Random House Trade Paperbacks; 2005.
19 Brennan TA, Rothman DJ, Blank LL, et al.Health industry practices that createconflicts of interest: A policy proposal foracademic medical centers. JAMA. 2006;295:429 – 433.
20 Kassirer JP. Commercialism and medicine:An overview. Camb Q Healthc Ethics. 2007;14:377–386.
21 Kuttner R. The American health caresystem: Wall Street and health care. N EnglJ Med. 1999;340:664 – 668.
22 De Simone J. Reductionist inference-basedmedicine, i.e., EBM. J Eval Clin Pract. 2006;12:445– 449.
23 Timmermans S, Berg M. The GoldStandard: The Challenge of Evidence-BasedMedicine and Standardization in HealthCare. Philadelphia, Pa: Temple UniversityPress; 2003.
24 Flexner A. Medical Education in the UnitedStates and Canada: A Report to the CarnegieFoundation for the Advancement ofTeaching. Bulletin No. 4. Boston, Mass:Updyke; 1910.
25 Barabasi AL. Network medicine—Fromobesity to the ‘diseasome.’ N Engl J Med.2007;357:404 – 407.
26 Goldberger AL, Amaral LAN, Hausdorff JM,Ivanov PC, Peng CK, Stanley HE. Fractaldynamics in physiology: Alterations withdisease and aging. Proc Natl Acad Sci. 2002;99:2466 –2472.
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010 299
27 Dunn JR, Cummins S. Placing health incontext. Soc Sci Med. 2007;65:1821–1824.
28 Miller WL, McDaniel RRJ, Crabtree BF,Stange KC. Practice jazz: Understandingvariation in family practices usingcomplexity science. J Fam Pract. 2001;50:872– 878.
29 Anderson RA, McDaniel RRJ. Managinghealth care organizations: Whereprofessionalism meets complexity science.Health Care Manage Rev. 2000;25:83–92.
30 Castellani B, Hafferty FW. The complexitiesof professionalism: A preliminaryinvestigation. In: Wear D, Aultman JM, eds.Professionalism in Medicine: CriticalPerspectives. New York, NY: SpringerVerlag; 2006:3–23.
31 Hafferty FW, Levinson D. Professionalismperspective: Moving beyond nostalgia andmotives towards a complexity science viewof medical professionalism. Perspect BiolMed. 2008;51:599 – 614.
32 Flexner A. Is social work a profession? ResSoc Work Pract. 1915;11:152–165.
33 Abbott A. The System of Professions: AnEssay on the Division of Expert Labor.Chicago, Ill: University of Chicago Press;1988.
34 Flexner A. Medical Education in Europe: AReport to the Carnegie Foundation for theAdvancement of Teaching. Bulletin No. 6.New York, NY: Carnegie Foundation for theAdvancement of Teaching; 1912.
35 Flexner A. Medical education: 1909 –1924.JAMA. 1924;82:833– 838.
36 Bonner TN. Crushing the commercial spiritin academic medicine: A crusade that failed.Acad Med. 1999;74:1067–1071.
37 Flexner A. Universities: American, English,German. New Brunswick, NJ: Transaction;1930.
38 Starr PE. The Social Transformation ofAmerican Medicine: The Rise of a SovereignProfession and the Making of a VastIndustry. New York, NY: Basic Books; 1982.
39 Wynia MK. The short history and tenuousfuture of medical professionalism: Theerosion of medicine’s social contract.Perspect Biol Med. 2008;51:565–578.
40 Cohen JJ, Cruess S, Davidson C. Alliancebetween society and medicine: The public’sstake in medical professionalism. JAMA.2007;298:670 – 673.
41 Sullivan WM. What is left of professionalismafter managed care? Hastings Cent Rep.1999;29:8 –13.
42 Cooke M, Irby DM, Sullivan WM,Ludmerer KM. American medical education100 years after the Flexner Report. N EnglJ Med. 2006;355:1339 –1344.
43 Cruess SR, Cruess RL. The role ofprofessionalism in the social contract. In:Parsi K, Sheehan M, eds. Educating forProfessionalism. Lanham, Md: Rowan andLittlefield; 2006:9 –23.
44 Flexner A. Medical education in the UnitedStates and Canada. Science. 1910;32:41–50.
45 Flexner A. I Remember: The Autobiographyof Abraham Flexner. New York, NY: Simonand Schuster; 1940.
46 Bonner TN. Iconoclast: Abraham Flexnerand a Life in Learning. Baltimore, Md: JohnsHopkins University Press; 2002.
47 Flexner A. Medical Education: AComparative Study. New York: TheMacmillan Company; 1925.
48 Kerr C. Introduction to the Transactionedition: Remembering Flexner. In: FlexnerA, ed. Universities: American, English,German. Piscataway, NJ: Transaction; 1994.
49 Capra F. The Web of Life. New York, NY:Anchor Books Doubleday; 1996.
50 Cilliers P. Complexity and Postmodernism.New York, NY: The Free Press; 1998.
51 Hafferty FW, Castellani B. The two culturesof professionalism: Sociology and medicine.In: Pescosolido B, Martin J, McLeod J,Rogers A, eds. The Handbook of Health,Illness and Healing: Blueprint for the 21stCentury. New York, NY: Springer; 2010.
52 Byrne D. Complexity Theory and the SocialSciences. London, UK: Routledge; 1998.
53 Capra F. The Hidden Connections:Integrating the Biological, Cognitive, andSocial Dimensions of Life Into a Science ofSustainability. New York, NY: Doubleday;2002.
54 Castellani B, Hafferty FW. Sociology andcomplexity science: A new field of science.New York, NY: Springer; 2009.
55 American Medical Student Association.AMSA PharmFree Scorecard 2009. Availableat: http://amsascorecard.org. Accessed May19, 2009.
56 Larson MS. The Rise of Professionalism: ASociological Analysis. Berkeley, Calif:University of California Press; 1977.
57 Baldwin DWC. Some historical notes oninterdisciplinary and interprofessionaleducation and practice in health care in theUSA. J Interprof Care. 2007;21:23–37.
58 Herbert CP. Changing the culture:Interprofessional education for collaborativepatient-centered practice in Canada.J Interprof Care. 2005;19:1– 4.
59 Irvine DH. Time for hard decisions onpatient-centered professionalism. Med JAust. 2004;181:271–274.
60 Lundberg GD. Medicine—A profession introuble? JAMA. 1985;253:2879 –2880.
61 Lundberg GD. Countdown to millennium:Balancing the professionalism and businessof medicine: Medicine’s rocking horse.JAMA. 1990;263:86 – 87.
62 Relman AS. Practicing medicine in the newbusiness climate. N Engl J Med. 1987;316:1150 –1151.
63 Relman AS. Shattuck lecture: The healthcare industry: Where is it taking us? N EnglJ Med. 1991;325:854 – 859.
64 Kassirer JP. Medicine at center stage. N EnglJ Med. 1993;328:1268.
65 Hafferty FW. Professionalism andcommercialism as antitheticals: A search for‘unprofessional commercialism’ within thewritings and work of American medicine.In: Parsi K, Sheehan M, eds. Healing asVocation: A Medical ProfessionalismPrimer. New York, NY: Rowen andLittlefield; 2006:35–59.
66 Swick HM. Toward a normative definitionof medical professionalism. Acad Med. 2000;75:612– 616.
67 ABIM Foundation. American Board ofInternal Medicine; ACP–ASIM Foundation.American College of Physicians–AmericanSociety of Internal Medicine; EuropeanFederation of Internal Medicine. Medical
professionalism in the new millennium: Aphysician charter. Ann Intern Med. 2002;136:243–246.
68 Hafferty FW. What medical students knowabout professionalism. Mt Sinai J Med.2002;69:385–397.
69 Arnold L. Assessing professional behavior:Yesterday, today, and tomorrow. Acad Med.2002;77:502–515.
70 Kao A, Lim M, Spevick J, et al. Teaching andevaluating students’ professionalism in U.S.medical schools, 2002–2003. JAMA. 2003;290:1151–1152.
71 Stern DT, ed. Measuring MedicalProfessionalism. New York, NY: OxfordUniversity Press; 2006.
72 Accreditation Council for Graduate MedicalEducation. Outcome Project. Availableat: http://www.acgme.org/outcome.Accessed October 18, 2009.
73 Liaison Committee on Medical Education.LCME Accreditation Standards.Available at: http://www.lcme.org/functionslist.htm#learning%20environment. AccessedMay 19, 2009.
74 Coulehan J, Williams PC. Vanquishingvirtue: The impact of medical education.Acad Med. 2001;76:598 – 605.
75 Hafferty FW. In search of a lost cord:Professionalism and medical education’shidden curriculum. In: Wear D, Bickel J,eds. Educating for Professionalism: Creatinga Culture of Humanism in MedicalEducation. Iowa City, Iowa: University ofIowa Press; 2000:11–34.
76 Lempp H, Swale C. The hidden curriculumin undergraduate medical education:Qualitative study of medical students’perceptions of teaching. BMJ.2004;329:770 –773.
77 Brainard AH, Brislen HC. Viewpoint:Learning professionalism: A view from thetrenches. Acad Med. 2007;82:1010 –1014.
78 Leo T, Eagen K. Professionalism education:The medical student response. Perspect BiolMed. 2008;51:508 –516.
79 Reddy ST, Farnan JM, Yoon JD, UpadhyayGA, Humphrey HJ, Arora VM. Third-yearmedical students’ participation in andperceptions of unprofessional behaviors.Acad Med. 2007;82(10 suppl):S35–S39.
80 Hafferty FW, Hafler JP. The hiddencurriculum, structural disconnects, and thesocialization of new professionals. In: HaflerJP, ed. Exemplary Learning in theWorkplace. New York, NY: Springer; 2010.
81 Henningsen JA. Why the numbers aredropping in general surgery: The answer noone wants to hear—lifestyle! Arch Surg.2002;137:255–256.
82 Smith LG. Medical professionalism and thegeneration gap. Am J Med. 2005;118:439–442.
83 Van Eaton EG, Horvath KD, Pellegrini CA.Professionalism and the shift mentality—How to reconcile patient ownership withlimited work hours. Arch Surg. 2005;140:230 –235.
84 Chimonas S, Brennan TA, Rothman DJ.Physicians and drug representatives:Exploring the dynamics of the relationship.J Gen Intern Med. 2007;22:184 –190.
85 Pollack A. Stanford to ban drug makers’gifts to doctors, even pens. New York Times.September 12, 2006:C2.
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010300
86 Huddle TS. Drug reps and the academicmedical center: A case for managementrather than prohibition. Perspect Biol Med.2008;51:251–260.
87 Lin GA, Beck DC, Stewart AL, Garbutt JM.Resident perceptions of the impact of workhour limitations. J Gen Intern Med. 2007;22:969 –975.
88 Gaba DM, Howard SK. Fatigue amongclinicians and the safety of patients. N EnglJ Med. 2002;347:1249 –1255.
89 Warner J. Diagnosis: Greed. Available at:http://warner.blogs.nytimes.com/2008/10/09/diagnosis-greed. Accessed May 19, 2009.
90 USA Today Opinion. Our view on medicalcare: Sleep-deprived residents still pose risksfor patients: ‘Culture of expectation’ and laxenforcement thwart changes. Available at:http://blogs.usatoday.com/oped/2008/12/our-view-on-med.html. Accessed May 19,2009.
91 Bloom SW. The medical school as a socialsystem: A case study of faculty–studentrelations. Milbank Mem Fund Q Health Soc.1971;49:1–196.
92 Barabasi AL. Linked: The New Science ofNetworks. Cambridge, Mass: Perseus; 2002.
93 Crandall RE. Linked: The new science ofnetworks [book review]. Am J Phys. 2003;71:409 – 410.
94 Watts DJ. The “new” science of networks.Annu Rev Sociol. 2004;30:243–270.
95 Hafferty FW, Watson KV. The rise oflearning communities in medical education:A socio-structural analysis. J Cancer Educ.2006;22:6 –9.
96 King S, Greidanus E, Carbonaro M,Drummond J, Patterson S. Merging socialnetworking environments and formal learningenvironments to support and facilitateinterprofessional instruction. Med EducOnline [serial online]. 2009;14:5. Available at:http://www.med-ed-online.org/volume14.php#T0000132. Accessed May 19, 2009.
97 Haidet P, Stein HF. The role of the student–teacher relationship in the formation ofphysicians: The hidden curriculum asprocess. J Gen Intern Med. 2006;21(1suppl):S16 –S20.
98 Ye J, Williams SD, Xu Z. The associationbetween social networks and colorectal
cancer screening in American males andfemales: Data from the 2005 healthinformation national trends survey. CancerCauses Control. 2009;20:1227–1233.Available at: http://www.springerlink.com/content/w475187287467663/fulltext.html.Accessed May 19, 2009.
99 Mackereth C, Appleton J. Social networksand health inequalities: Evidence forworking with disadvantaged groups.Community Pract. 2008;81:23–26.
100 Christakis NA, Fowler JH. The spread ofobesity in a large social network over 32years. N Engl J Med. 2007;357:370 –379.
101 Christakis NA, Fowler GA. The collectivedynamics of smoking in a large socialnetwork. N Engl J Med. 2008;358:2249 –2258.
102 Lurie SJ, Fogg TT, Dozier AM. Socialnetwork analysis as a method of assessinginstitutional culture: Three case studies.Acad Med. 2009;84:1024 –1035.
103 Baldwin DCJ. Territoriality and power inthe health professions. J Interprof Care.2007;21:97–107.
Flexner Centenary
Academic Medicine, Vol. 85, No. 2 / February 2010 301