Embed Size (px)
Citation preview

The interface of various glasses and glass ceramics with a bony implantation bed
U. Gross lnstitute of Pathology, Klinikum Steglitz, Freie Universitat Berlin, 1000 Berlin 45, Federal Republic of Germany V. Strum Department of Maxillo-Facial and Plastic Surgery, Klinikum Steglitz, Freie Universitat Berlin, 1000 Berlin 45, Federal Republic of Germany
Basing on histomorphological evaluations and morphometrical quantifications in a standardized model experiment, a com- parison is made between the reactions of skeletal tissues to various glasses, glass- ceramics and enamels. On the surface of these so-called reactive biomaterials either a direct bonding to mineralized bone or also different amounts of osteoid or chon- droid tissue formation can be observed, depending on the composition of the mate- rial. It is shown that (1) the solubility of the glasses cannot directly be related to the reactivity and the resulting bone bonding; (2) bone binds only to glasses with a con-
trolled release of constituents and which exhibit a seam of extracellular matrix on their surface, in which normal primary mineralization can occur; (3) the release of constituents such as A1203, Ta205, Zr02, or phosphates from the material can inhibit this normal mineralization and the trans- formation of chondroid tissue to bone; (4) if connective tissue instead of bone is present at the interface (either primarily or after bone remodelling), the dissolution (or cor- rosion) of the material may be no longer controllable, and the tissue reacts with a continuous inflammatory response to the corrosion products.
INTRODUCTION
Biomaterials for bone implants can be subdivided into categories according to their relative surface reactivity' (1) nearly inert with smooth or, (2) (micro) porous surface, (3) controlled reactive surface, (4) resorbable materials.
Most of the biomaterials in clinical use for bone or tooth replacement are of types 1 and 2. They should be non-toxic, non-irritant, non-tumor- inducing, biomechanically stable, adapted or adaptable to function, and should also display additional properties requisite for lifetime durability. The interfacial tissue response is mainly fibrous; under certain conditions, how- ever, contact to bone, osteoid or cartilage is possible. The type 4 resorbable materials are totally replaced by regenerating tissues, the most important being bone. The potential for bone regeneration is rather high even in hu- mans; the limitation for the applicability of these resorbable materials seems to lie in the difficulty of attaining the right equilibrium between resorbability of the material and bone development, the external and internal porous structure of the material affecting the mechanical stability, and other factors
Journal of Biomedical Materials Research, Vol. 19,251-271 (1985) 0 1985 John Wiley & Sons, Inc. CCC 0021 -9304/85/030251-21$04.00

252 GROSS AND STRUNZ
as well. Therefore, only a limited application range can be expected in hu- mans for porous materials of this type, e.g., Ca0-A1203 ceramic (Z), hydroxy- apatite and/or tricalcium phosphate (reviewed by de Groot ref. (3)).
The type 3 surface reactive biomaterials provoke tissue reactions which can result in osteoid or bone-bonding mechanisms. This was shown for bioglass and other glass- ceramic^.^
1. BONE BONDING
Hench4 was first to systematically investigate a class of so- called bio- reactive glass ceramics (Bioglass) and to formulate a theory on the bone bonding mechanism. At the interface of implanted bioglass he found a Ca- P-rich layer and, under this layer, a second Si-rich layer covering the bulk g l a ~ s . ~ - ~ The Si-rich layer is assumed to protect the glass from further attack even at pH > 9 and almost indefinitely at pH < 9.6 The analysis of system- atic variations in the contents of Si02, CaO, NazO and constant 6.0 wt% P205 showed bone bonding and non-bonding bioglass compositions, which can be visualized in a triaxial plotting. The implications of this study are discussed by Ducheyne (this issue; the plotting is depicted in his Figure 2). Further- more, Hench and Paschal15 found the behavior of the bioglasses 45 S5 (Table I) and 45 S 0.75 to be independent of whether the implants were as-cast glass, partially crystallized or fully crystallized.
Light microscopy (LM) and transmission electron microscopy (TEM) showed that the direct bonding of bone to bioglasses or other glass ceramics was due to the deposition and subsequent mineralization of organic bone matrix- mainly composed of collagen and mucopolysaccharides - at the outer layer of the implant.6 Between the collagen fibers and the glass, there is an amorphous 800-1000 A thick zone6 which can be mineralized and which seems to play a special role, as will be shown later.
The reactivity of these bioglasses is the result of their solubility and the leaching of ions into the surrounding intercellular m a t r i ~ . ~ This can be dem- onstrated with two basic compositional modifications: the addition of CaF2 (in place of CaO) resulted in a composition (45 S5 F) with slower reactivity
TABLE I Composition of Silicon-Based Glasses and Glass Ceramics? Bonded to Bone
Compositions (wt%)
Compound UF45S5 KG Z1 Cera* KG S' KG Si 20/1+
SiOl 45.0 46.7 46.2 46.0 46.0 Ca(P03)~ - 16.2 25.5 16.0 16.0 Na20 24.5 3.5 4.8 5.0 KzO MgO CaO P205 6.0
- - - - 0.4 -
- - 2.9 - 5.0 24.5 33.5 20.2 33.0 33.0
- - - -

GLASSES IN BONY IMPLANTATION BED 253
and reduced bone bonding after insertion into the femur or tibia of male Sprague Dawley rats. The addition of B203 (for SiOz) resulted in a more reactive composition (45 B5 S5) with rapid resorption of the implant.'r6
Another attempt to reduce the solubility while maintaining the reactivity of glasses and glass ceramics was made by Bromer and co-workers.g By lowering the NazO content and the addition of K 2 0 and MgO to the glass or glass ceramic compositions Ceravital (R) was manufactured (Table I) .9 The bone tissue response to these materials was evaluated by employing more advanced histological techniques which provided a more reliable insight into the basic mechanisms of bone bonding of glasses and glass ceramics. This progress was gained by the adoption of morphometrical methods for the evaluation of serial sections after superficial staining.'O Furthermore, this morphometrical quantification of the main tissue components - bone, oste- oid, chondroid and soft tissue - as a percentage of the implant interface" provided a reasonable basis for the comparison of different implant materi- als. Finally, also the animal model was standardized for this comparison, using always the same implantation site in the diaphysis of the femur of male Sprague-Dawley rats. Consecutively, however, the results obtained with this model proved to be principally transferable to other models with the follow- ing implantation sites: the maxilla or mandible of pigs,I2 the femur of dogs,13 the metatarsus of chickens,I4 the femur of rabbits,15 the middle ear of rabbitsl6 and the lower jaw of humans.17 Nevertheless, in the following we refer to the rat femur model (Fig. 1) that has been described in detail."
It seems reasonable to discriminate between the early effects of an implant material on the processes during wound healing, i.e., bone healing, which exert an influence on the development of immature tissue, and the late effects, which modify the turnover of a more mature tissue, as, in the case of bone, the remodeling.
In studying the reactions mainly 14,30, and 60 days postoperatively, as we did in the rat model, the late effects cannot be analysed appropriately. The early effects, however, seem to be more important for the assessment of an implant material and for the question of whether an implant material should also be studied in special implantation sites and with certain conditions, e.g., load, design, in a long-term trial, as we did in the above-mentioned models.
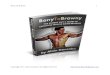
The different silicon-based glasses and glass ceramics to which bone bond- ing occurs (Table I) display a characteristic time-dependent tissue reaction at the interface. An example is given for KG Si20/1 (Fig. 2), whose solubility is very low compared with that of the bioglass 45 S5.9 Soft tissue is rapidly replaced by bone; a low percentage of chondroid tissue is found. Osteoid is practically absent, indicating that the mineralization takes place without delay. When the percentage of bone at the interface of some glasses and glass ceramics is plotted against implantation time (Fig. 3) the best results are shown for the glasses 45 S5 and KG Z1, less favorable results for KG S and Ceravital OF (the latter was etched by an acid prior to implantation), and intermediate results for KG Si20/1. This result is astonishing, because the solubility of the composition KG Si20/1, which does not contain NazO

254
100-
90-
80-
70-
60 - 50 - 40 -
30 - 20 - 10 -
GROSS AND STRUNZ
Figure 1 Square-shaped glassy implant within a sagittal hole midshaft in the rat femur. (Macrophotograph 3.5 X.)
bone
soft t issue
.-a - chondroid I I 1 I I
0 14 30 60 90 1 2 0 DAYS
Figure 2 Percentage of bone, chondroid, and soft tissue at the interface of glass ceramic KG Si20/1. Mean, *SE. No osteoid was found in this case.

255
1007
90 -
80 -
70 -
60 -
50 -
40 -
30 -
20 -
10-
0 -r 0
GLASSES IN BONY IMPLANTATION BED
~
KG Z1 U F 4 5 S 5 KG SI 20/1 KG CERA OF KG S
I I I I I 14 30 60 90 120 days
Figure 3 Percentage of bone at the interface of glass ceramics KG S, A; KG Cera OF, m; KG Si20/1,0; and glasses UF 45 S 5 , O ; KG Z1,o. Mean values (SE has been calculated, but is not given in this plot.)
(Table I), is very low in comparison with the high solubility of the glasses 45 S5 and KG Z1 and the intermediate solubility of KG S and KG Cera OF. Therefore, the solubility of a composition cannot be directly related to the reactivity of a glass or glass ceramic and to bone bonding, as suggested in the triaxial plotting18 (see also the paper by Ducheyne, this issue). Those glassy materials which contain modifying compounds such as K 2 0 and MgO in Ceravital or the metal oxides listed in Table I1 are not comprised in this triaxial plot.18 Besides, the composition Kg Si20/1 does not fit into the triaxial plot, because it lacks Na20 and contains MgO. This composition, however, is comparable with that of the glass ceramic 1 + 0.5 F of Kokubo et al.I9
There is evidence for a certain surface structure for each glass ceramic after exposure to an aqueous solution in vitro and in vivo. For example, after treatment with heated water (90°C) for 24 h (Fig. 4), the composition KG S (Table I) displays a considerable number of small pores between promi- nences that are possibly crystals. Controls, without treatment, not depicted, show a more smooth surface with furrows only originating from cutting with the saw. The in vivo conditions for the corrosion of KG S are different. In vivo corrosion produces interconnecting pores by the dissolution of crystals prior to the glassy phase." Cell processes of macrophages, lamellopodia, invade the pores, and debris-mainly of the glassy phase of the ceramic- can be phagocytosed and dissolved by these cells." Later on, however, TEM reveals an extracellular seam of fine granular material at the interface. This seam has a thickness of approximately 0.5-0.7 pm (Fig. 5), and can be min- eralized.20 A corresponding seam with a thickness of 0.7 pm or less can also be seen at the interface of bioglass 45 S5 (Fig. lo), which-as a glass-does

TABL
E I1
C
ompo
sitio
n of
Sili
con-
Bas
ed G
lass
es a
nd G
lass
Cer
amic
s w
ith
Red
uced
Sol
ubili
ty a
nd Im
pair
ed B
indi
ng M
echa
nism
s
Com
posi
tion
(wt%
)
Com
poun
d K
GZ
rl
KG
ZR
z K
GE
10
KG
E4
KG
X
KG
X1/
4 KG
Y
KG
Y17
K
GY
22
KG
Y23
KG
Si1
2/1
~ ~~
~
41.0
45
.0
41.0
38
.5
34.0
34
.0
38.0
38
.0
16.0
16
.0
16.0
16
.0
12.0
12
.0
13.5
13
.5
3.5
3.5
3.5
3.5
3.5
3.5
4.0
4.0
34.0
34
.0
34.0
34
.0
23.0
23
.0
31.0
31
.0
-
-
-
-
15.0
15
.0
7.0
9.5
-
-
-
2.5
12.5
12
.5
5.5
2.5
-
-
2.5
2.5
-
-
1.0
1.5
-
-
-
-
-
-
-
0.00
1 5.
0 1.
0 2.
5 2.
5 -
-
-
-
38.6
13
.7
4.1
31.5
9.
7 2.
5
0.00
1 -
-
38.6
38
.5
13.7
16
.0
4.0
5.0
31.5
33
.0
9.7
7.5
2.5
0.00
1 -
-

GLASSES IN BONY IMPLANTATION BED
Figure 4 Porous surface structure of glass ceramic KG Cera after treatment with heated water (SEM).
Figure 5 Seam of fine granular material at the surface of KG S (top) (cracks as artifacts), 14 days postoperatively, Collagen fibrils and globular deposits of mineral between the seam and part of an osteoblast (bottom). (TEM, bar 1 Pm.)
257

258 GROSS AND STRUNZ
not show the corrosion-induced porous structure and thus displays a smoother surface. On the surface of the glass ceramic KG Si20/1 this seam with a thickness of 0.4-0.6 pm can also be found (Fig. 12). It can be specu- lated that the seam consists of extracellular ground-substance material, which possibly contains nectins, e.g., fibronectin, and provides a basis for the attachment of the collagen. The mineralization of the seam was demon- strated. Up to now, we have not been able to find the seam at the interface of materials which are not bonded primarily to bone (Fig. 15).
Therefore the seam could be a characteristic of and prerequisite for bone bonding, We assume that this is the phenomenon that has already been described6j7 and designated as the surface layer of bioglass or amorphous cementing substance.
The further steps in bone development and bonding are governed by osteoblasts in the implant area after macrophages have disappeared. Osteo- blasts provide collagen, ground substance and matrix vesicles for primary mineralization. This could be shown in TEM for glass ceramic KG S (Figs. 5, 6), KG Si20/1 (Fig. 12, 13) and for the other compositions, given in Table I. The events are consistent with the present concepts of primary bone
Also here, within the extracellular matrix and between small bundles of fibrils, matrix vesicles appear and display small, electron-dense, needle-like crystallites (Fig. 13), assumed to be apatite. After rupture of the vesicle membrane, first calcifying globules, then conglomerations of cal- cospheritic structures, and finally calcifying fronts are formed (Figs. 12, 5). Often this process begins and is therefore more pronounced in the sur- roundings of the implant and the adjacent osteoblast (Fig. 6), but may also start in the area around the osteoblast and then involve the surroundings of the already mineralized seam of amorphous cementing substance at the interface (Fig. 5). Later on, the whole area is mineralized (Fig. ll), the osteo- cytes being rather evenly distributed and often arranged with their long axis parallel to the surface of the implant (Figs. 8, 14). This feature is found in different species-rats, dogs, pigs (Fig. 9), chickens (Fig. 7), and humans- and provides the morphologic basis for the biomechanical quality of the bone bonding. According to our understanding and definition, one can only diag- nose bone bonding or bone connection if bone adheres to the implant mate- rial as shown, and if a tensile strength of the bonding can be measured in such cases.
For KG Ceravital (R), pure tensile strength to rupture, without interfering shear forces, was determined with mean values of 2.2 N/mm2 in pigs27 and 3.9 N/mm2 in chickens28; single values, however, were much higher by a factor of 2 to 3. Measurements of shear strength yielded even higher values up to 17 N/mm2 for KG Ceravital, 384 days after implantation into the pig jaw.” The stresses to which bulk bioglass-ceramic implants were resistant 210-350 days after implantation in monkey femurs averaged about 880 k g f / ~ m ~ . ~ ’ The bonding strength of the implants is dependent on the percentage of bone connection at the interface, and this parameter is dependent on time after implantation, as shown by data from different

GLASSES IN BONY IMPLANTATION BED
Figure 6 Patchy mineralization and calcifying front between an osteoblast (bottom) and KG S (top), 15 days postoperatively. Note indentations of the glass ceramic indicating remainders of pores. (TEM, bar 1 pm.)
Figure 7 Interface of KG Cera (top) with bone bonding (middle), 60 days after implantation into the metatarsus of a cock. Rather even distribution of osteocytes. Haversian canal at the interface (middle right) producing lacunar corrosion of the implant. (Giemsa, bar 50 pm.)
259

260 GROSS AND STRUNZ
Figure 8 Bone bonding at the surface of KG S (top), 60 days after im- plantation into the rat femur. Axis of osteocytes parallel to the implant sur- face. Haversian canal (middle right and bottom left) with empty vessels after perfusion. (Giemsa, bar 25 pm.)
specie^.'^-^^ A minor contribution to mechanical resistance of the interface is assumed for other types of tissue: osteoid, chondroid, and soft tissue.
Chondroid is defined as a tissue with rounded cells producing meta- chromatically staining ground substance with fibrils different from type l collagen but TEM features of type 2 collagen. Whereas the amount of chon- droid at the interface is low in early stages after implantation of bioglass 45 S5 (in the range of 1% of the implant surface after 14 days, 0.5% after 30 days, and 0 thereafter) and KG Si20/1 (1% after 14 days, 3% after 30 days, 0 there-
Figure 9 Bone bonding to KG Cera (top), 101 days after implantation into the left lower jaw of a pig. Even distribution of osteocytes parallel to the implant surface (middle). Haversian canal with seam of osteoblasts (bottom). (Giemsa, bar 50 pm.)

GLASSES IN BONY IMPLANTATION BED 261
Figure 10 Seam of mineralized material at the surface of bioglass 45 S 5 (top), 14 days postoperatively. Below this seam, chondroid showing rather patchy mineralization with a dense calcifying front (middle). Ground sub- stance with fibrillar and globular material (bottom left) in the territory of a chrondroid cell (bottom right). (TEM, bar 0.5 pm.)
after), KG S implants display a much higher amount (23% after 14 days, 2% after 30 days and 1% after 60 days).
The sequence of events suggests that the chondroid is transformed into bone, the chondroid cells being transformed into osteoblasts, chondroid
Figure 11 Fully mineralized bone with two osteocytes (middle and bottom) bonding to bioglass 45 S 5 (top) with fine cracks as artifacts, 30 days post- operatively. (TEM, unstained, bar 2.5 pm.)

262 GROSS AND STRUNZ
Figure 12 Seam of mineralizing substance at the surface of KG Si20/1 (top) with cracks as artifacts, 8 days after implantation. Below this seam calcifying front, globular calcification and patchy mineralization. Collagen fibrils outside the lacuna of an osteoblast (middle right). (TEM, bar 1 pm.)
bone I.31 Other investigations confirm this d e v e l ~ p m e n t . ~ ~ In our experi- ments we did not find any signs of resorption of chondroid cells and their territories, and no replacement by osteoblasts. This is in contrast to en- chondral bone d e ~ e l o p m e n t , ~ ~ in which cartilage is resorbed and replaced by bone as shown by Reddi (this issue). The significance of chondroid at an implant interface points to the possibility that the release of substances from the implant can affect the differentiation of young cells in the surroundings of the interface. Therefore, we assume that biomaterials which do not induce chondroid development at the interface are superior to those which do. This assumption is based on the conception that primary bone development is
Figure 13 Surroundings of an implant KG Si20/1: adjacent to cells, newly formed bundles of transversely cut collagen fibrils, fine granular ground substance and matrix vesicles (middle), 14 days after implantation. Some matrix vesicles contain fine needle-like crystals (TEM, bar 0.5 pm.)

GLASSES IN BONY IMPLANTATION BED 263
Figure 14 Bone bonding at the interface (middle) of glass ceramic KG Si20/1 (top), 60 days postoperatively. Note crystal structure of the implant (top) and leaching zone (middle) with persisting crystals. Osteocytes 'parallel to the implant surface and evenly distributed. Bone marrow with blood forming cells (bottom left). (Giemsa, bar 50 pm.)
better for the anchorage, i.e., the biomechanical quality of the interface, than the development of chondroid.
Another problem to be kept in mind is the lacunar corrosion of glass or glass ceramic at sites where Haversian systems reach the interface. Long- term studies (up to 3 years in pigs) have shown that these lacunae can gain considerable depth in the bulk material and can contribute to the deterio- riation of the implant and to implant fai1ure.l'
Some of these lacunae are secondarily filled with bone, and bone bonding can be restored. This process was also observed in long-term studies and is thought to be due to physiological bone remodeling extending into the im- plant interface. Formally the corrosion is bound to areas with soft tissue of Haversian canals, in which the leaching of the material by interstitial fluid is increased and macrophages can move in to phagocytose the remainders of the implant material." Since the lacunar corrosion of glasses and glass ce- ramics which principally exhibit bone bonding is dependent to some extent on the solubility of these substances, the search began for additives to the silicon-based glasses and their ceramised counterparts.
2. INHIBITED BONE BONDING
In vifro studies revealed that the solubility of glasses and glass ceramics decreased considerably if metal oxides were added.'," Some of the com- positions tested also in vivo, are listed in Table 11. The in vivo tests can be summarized with the observation of more or less pronounced inhibition of bone bonding mechanisms at the interface."^^^ Bone bonding if it occurred at all, was considerably decreased, delayed or absent." Often there was a seam

264 GROSS AND STRUNZ
Figure 15 Seam of osteoid with some electron-dense mineralized borders of canaliculi (middle to top) and masked fibrils at the interface of glass KG E4 (top), 14 days postoperatively. Osteoblast (bottom right) surrounded by col- lagen fibrils and a zone with globular mineralization. (TEM, bar 1.25 pm.)
of unmineralized osteoid tissue (Fig. 15). Within this seam the collagen cross- striation was usually masked, but the canaliculi of osteoblasts were discern- ible, their surroundings in TEM being electron-dense and apparently to some extent mineralized. But mineralization was lacking in the seam between the implant surface and the already mineralized surroundings of the osteoblasts (Fig. 15).*' The fact that this defective mineralization only occurs at the im- plant interface indicates that the implant releases substances which influence steps in the mineralization process. The most potent inhibition of mineral- ization was observed with the compositions KG y 17, KG y 22, and KG X %. Up to 50% of the implant interface (KG y 17) was covered only by osteoid 60 days postoperatively. From the composition of these materials (Table 11), it could be concluded that a combination of the compounds A1203 and Ta205 may be responsible for this inhibitory effect. Besides, aluminum can inhibit the growth of calcium phosphate crystals in and induces osteo- malacia, as is well-known in patients with long-term hemodialysis.
Morphometric measurements also showed a persistence of chondroid in a seam at the implant interface of the compositions listed in Table 11. Once again, the highest values were found at the interface of KG y 17 with 28% chondroid 60 days postoperatively. (The percentages given here are mor- phometric data and therefore differ slightly from the estimated values pub- lished previously.11).

GLASSES IN BONY IMPLANTATION BED 265
Chondroid can be transformed into bone, as shown above. The persistence of chondroid therefore suggests that this differentiation is inhibited. The inhibited cells do not switch from production of metachromatic ground sub- stance and type 2 collagen to production of type 1 collagen and organelles for mineralization. 'I
The best values for bone bonding in this group of materials (Table 11) were found for the compositions KG Zr 1 and KG Zr 2. Since these compositions exhibited also a slight persistence of osteoid and chondroid at the inter- face, they were classified among those materials with principally inhibitory effects and should thus no longer be considered as suitable for bone or tooth substitutes.
Apart from silicon-based glasses, some phosphate-based glasses (Table 111) have been also tested in the rat femur model. The compositions PK 2 and PK G12 displayed rather extensive corrosion and some cracks. They induced a considerable inflammatory tissue response, which increased with time. High corrosion rates and an inflammatory tissue response was reported after implantation of phosphate glass into the tibia of rabbits.36 Only the com- position PK 1 showed a less adverse tissue response and a seam of osteoid or chondroid at the interface (Fig. 16). In view of the above considerations, this type of materials must be also discarded.
Since bulk bioglass or glass ceramic is biomechanically too weak to fulfill the requirements of a load-bearing bone or tooth substitute, enameled coating- as described by Ducheyne, this issue, and shown schematically in his Fig. 6- was developed and tested in vivo. 15,37 Here we refer only to the tissue reaction at the interface of some enamels whose composition (Table IV) similar to the above-described glasses or glass ceramics with re- duced solubility (Table 11). For example, the enamel El6 K7 gives rise to soft tissue formation in the rat femur model after 14 days (Fig. 17), and to in- creasing amounts of osteoid or chondroid later on (Fig. 18). Once more the inhibitory effect on mineralization and differentiation is obvious. It could be shown, however, that inclusion of glass ceramic particles (Ceravital) in the enamel counteracts these inhibitory effects to a certain e~ ten t ,~ ' i.e., to in- crease mineralization at the enamel moiety of the interface.
TABLE111 Composition of Phosphate-Based Glasses
Compositions (wt%)
Compound PK 1 PK 2 PK G12

266 GROSS AND STRUNZ
Figure 16 Seam of osteoid and chondroid (middle, grey) at the surface of phosphate glass PK 1 (top), 60 days postoperatively. New (bottom right) and old bone (bottom left) outside the seam. (Giemsa, bar 50 pm.)
Substances released from the surface of the glass ceramic KG S (Table I) have been demonstrated to counteract the inhibitory effects of the di- phosphonate EHDP (ethane-1-hydroxy-1, 1-diphosphonic acid) at the implant interfa~e,~' whereas the EHDP-induced osteoid persisted in more remote areas of the bony implantation bed.
3. HYPOTHESIS FOR THE BONE BONDING MECHANISM
How can these data be interpreted? The theory for primary bone mineral- ization attributes a decisive role to matrix vesicles, which are thought to act
TABLE IV Composition of Some Enamels for Metal Coating with Glass Ceramic Particles
Compositions (wt%)
Compound BU 9 BAY WR El6 K7 Wendel
S i 0 2 - 40.2 49.0 49.0 8 2 0 3 17.0 18.1 5.9 5.9 Al(P03)3 41.0 Li20 4.0 - 2.6 2.6 Na20 12.0 10.1 9.3 18.5 KzO 4.0 5.1 9.2 - A1203 16.0 1.2 2.7 2.7 Ti02 6.0 18.5 7.7 7.7
2.9 p205
- 0.7 3.2 3.2 - 3.2
MgO F
- 2.6 2.6 CaO - CeO - - 2.5 -
- 5.3 5.3 Na3AIF6 - 2.5 Biz03 - - -
- - -
- - -
- -

GLASSES IN BONY IMPLANTATION BED 267
Figure 17 Enamel El6 K7 (top) surrounded by a layer of soft tissue (middle), 14 days postoperatively. Young bone (bottom) adjacent to soft tissue. (Giemsa, bar 50 pm.)
as primary sites of apatite f o r m a t i ~ n . ~ ~ , ~ ~ It is assumed that, within these matrix vesicles, calcium is bound to phospholipids and PO4 ions released from pyrophosphate or other polyphosphates. Amorphous calcium phos- phates and apatite crystals thus form within the matrix vesicles at their membrane.** This theory attributes to pyrophosphate and/or polyphosphates an inhibitory effect on minerali~ation.~' Inhibition of phosphatases - enzymes which play a key role in matrix vesicles-would also have an inhibitory influence on apatite nucleation. On the other hand, monophos- phate could be required to stimulate apatite development and growth out- side the matrix vesicles in the interstitial space and in collagen.42
These reflections led to another experiment in which the release of phos- phates from some glasses and a glass ceramic was tested in vifro. Two grams of the pulverized materials (Table V) were shaken in 10 ml water for 24 h,
Figure 18 Enamel El6 K7 (top) encased in osteoid and chondroid (middle and top left), 60 days postoperatively. New bone (bottom, middle and right) and old bone (bottom left). (Giemsa, bar 50 pm.)

268 GROSS AND STRUNZ
TABLE V Release of Monophosphate and/or polyphosphates at the Surfaces
of Glass or Glass Ceramics" and Relation to Bone Bonding
Tri- and tetraphosphate Bone bonding to Composition Monophosphate or polyphosphate the implant
- +++ +++ +++
- PKI (+I PK2 (+I PIG KG St +++ KG Si 20/1 glass +++ KG Si 20/1 ceramic +++
+ +
-
- -
Note: +, positive; + + +, strongly positive; -, negative.
and the supernatant was analyzed for monophosphate and polyphosphates by paper~hromatography.~~ The findings (Table V) indicate that mono- phosphate is released from compositions which display bone bonding at the interface in vivo, whereas tri- and tetraphosphate and polyphosphates were released from compositions which inhibit mineralization and differentiation in vivo, as discussed above. Although these results must be reaffirmed and other materials should be analyzed as well, they support the hypothesis: Glasses and glass ceramics as well as other materials should not release polyphosphates or other substances which can lead to a decompensation of physiological mineralization processes at the implant interface in a bony implantation bed.
It seems to us that this hypothesis, although negatively formulated, pro- vides essential points for the description of biomaterials with a controlled reactive surface or so-called bioactive materials. The activity would thus be the absence of inhibition of mineralization. Besides, osteoinductive properties have not yet been conclusively demonstrated for any glass based material."
Moreover, the adsorption of blood proteins and noncollagenous bone pro- teins to glass-based materials may be of importance for bone bonding. Ad- sorption properties were shown for poly-L-alanine on L-quartz and a glass ceramic.44 Calcium phosphate compounds (CaHP04, Ca3 (PO&, hydroxy- apatite) adsorb complement factor C3, alpha-2-HS-glycoprotein, albumin and IgG.45 The adsorption of blood fibronectin to bioglass (01 52 S 4.6) and an effect of precoated bioglass (01 52 S 4.6) on adhesion and spreading be- havior of hamster fibroblasts was demonstrated in vifro. 46 In accordance with these studies, we found the expression of fibronectin at the surface of rat fibroblasts and osteoblasts adhering to the surface of KG S.47 Further studies are needed, however, to clarify the significance of adsorption of bone matrix noncollagenous proteins48 for the bone bonding to implant materials.
CONCLUSIONS
Progress in the understanding of bone bonding mechanisms to glasses, glass ceramics and related materials was made by systematic quantitative

GLASSES IN BONY IMPLANTATION BED 269
analysis of tissue response in short-term experiments with a standardized rat femur model as well as by light-microscopic, TEM, and SEM analyses which revealed the basic similarity of long-term implantation in other species (hu- mans, monkeys, pigs, dogs, rabbits, chickens) at other implantation sites. On the other hand, it proved necessary to analyze more thoroughly the release of substances from the materials and their biological effect on cells and cellular products, which can be done partially in vitro. Bone bonding to certain glassy compositions does occur, and the most important prerequisite is the controlled release of substances which do not inhibit bone-cell function and the extracellular processes associated with mineralization. Furthermore, it seems that the adsorption of not yet determined cellular and/or blood- derived products to the implant surface provides the basis for the devel- opment of a biomechanically stable integration of the material in bone.
References 1.
2.
3.
4.
5.
6.
7.
8. 9.
10.
11.
12.
13.
14.
15.
L. L. Hench and E. C. Ethridge, Biomuteriuls, An lnterfuciul Approach, Aca- demic Press, New York, 1982. J. J. Klawitter and S. F. Hulbert, "Application of porous ceramics for the attachment of load bearing internal orthopedic applications," ]. Biomed. Muter. Res. Symp., 2, 161-229 (1972). K. de Groot, (ed.) Biocerumicsof Calcium Phosphate, CRC Press, Boca Raton, Fla., 1982. L. L. Hench, R. J. Splinter, W. C. Allen, and T. K. Greenlee, "Bonding mechanisms at the interface of ceramic prosthetic materials," J. Biomed. Muter. Res. Symp., 2, 117-141 (1971). L. L. Hench and H. A. Paschall, "Direct chemical bond of bioactive glass- ceramic materials to bone and muscle," J. Biomed. Muter. Res. Symp., 4,
L.L. Hench and H.A. Paschall, "Histochemical responses at a bio- materials interface," J. Biomed. Muter. Res. Symp., 5, 49-64 (1974). A. E. Clark, L. L. Hench, and H. A. Paschall, "The influence of surface chemistry on implant interface histology: A theoretical basis for implant materials selection," ]. Biomed. Muter. Res., 10, 161-174 (1976). H. Bromer, E. Pfeil, and H. H. Kas, German Patent 2.326.100, 1973. B. A. Blencke, H. Bromer, and K. K. Deutscher, "Compatibility and long- term stability of glass ceramic implants," ]. Biomed. Muter. Res., 12,
U. M. Gross and V. Strunz, "Surface staining of sawed sections of un- decalcified bone containing alloplastic implants," Stain Techn., 52, 217-219 (1977). U. M. Gross and V. Strunz, "The anchoring of glass-ceramics of different solubility in the femur of the rat," J. Biomed. Muter. Res., 14,
V. Strunz, U. Gross, H. Bromer, and K. Deutscher, "Glaskeramiken fur kieferchirurgische und zahnarztliche Zwecke," Bundesministerium fur Forschung und Technologie Forschungsbericht BMFT-FB MT 0267, Abschlupbericht, 1982. K. Deutscher, B. Blencke and H. Bromer, "Bioaktive Glaskeramik als Implantatwerkstoff" Biotechnische Umschuu, 2, 288-293, (1978). D. Schumacher, V. Strunz and U. Gross, "Does piezoceramic influence avian bone formation in the early postoperative phase?" Biomuteriuls, 4,
G. A. Fuchs and K. Deutscher, "Glass-ceramic coated implants," Arch. orthop. truumut. Surg., 98, 121-126 (1981).
25-42 (1973).
307-316 (1978).
607-618 (1980).
215-217 (1983).

270 GROSS AND STRUNZ
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
R. Reck, ”Tissue reactions to glass ceramics in the middle ear,” Clin. Otolaryngol., 6 , 63-65 (1981). M. Bunte and V. Strunz, “Ceramic augmentation of the lower jaw,”
M. M. Walker, ”Master’s Thesis,” University of Florida, Gainesville, 1977, cited according 1. T. Kokubo, M. Shigematsu, Y. Nagashima, M. Tashiro, T. Nakamura, T. Yamamuro, and S. Higashi, “Apatite- and wollastonite-containing glass- ceramics for prosthetic application,” Bull. fnsf. Ckem. Res., Kyoto Univ., 60,260-268 (1982). U. Gross, J. Brandes, V. Strunz, I. Bab, and J. Sela, ”The ultrastructure of the interface between a glass ceramic and bone,” J. Biomed. Muter. Res.,
H. C. Anderson, ”Matrix vesicles of cartilage and bone,” in The Biochem- istry and Physiology of Bone, Vol. 4, G. H. Bourne, Ed., Academic Press, New York, 1976, pp. 135-157. A. Boyde and M. H. Hobdell, “Scanning electron microscopy of primary membrane bone,” Z . Zellforsch., 99, 98-108 (1969). M. Owen, ”Cellular dynamics of bone,” in The Biochemistry and Physiology of Bone, Vol. 3, G. H. Bourne, Ed., Academic Press, New York, 1971,
D. J. Simmons, ”Comparative physiology of bone,“ in The Biochemistry and Physiology of Bone, Vol. 4, G. H. Bourne, Ed., Academic Press, New York, 1976, pp. 446-516. J. Sela, I. A. Bab and A. Muhlrad, ”Ultrastructural and biochemical char- acterization of extracellular matrix vesicles in healing alveolar bone sock- ets: preliminary indications for the presence of contractile proteins,” Metab. Bone Dis. Rel. Res., 1, 185-191 (1978). J. Sela, J. Brandes, V. Strunz, I. Bab, and U. Gross, “Primary mineral- ization and extracellular matrix vesicles in rat bone after administration
J. ~ u x . - ~ u c . Surg., 5, 303-309 (1977).
15, 291-305 (1981).
pp. 271-298.
of glass-ceramic implants,” Arch. Orthop. Traumat. Surg., 98, 237-240 (1981). M. Bunte, V. Strunz, U. M. Gross, H. Bromer, and K. Deutscher, “Ver- gleichende Untersuchungen uber die Haftung verschiedener Implantat- materialien im Knochen,” Dtsch. zahnurztl. Z . , 32, 825-828 (1977). U. Gross, D. Schumacher, and V. Strunz, ”Comparative studies on the tissue reaction after implantation of glass ceramic into human, pig, rat and chicken bone,” in Ceramics in Surgery, P. Vincenzini, Ed., Materials Science Monographs 17, Elsevier, Amsterdam, 1983, pp. 161-168. A. Hirsch, ”Struktur und Belastbarkeit von Zwischenschicht und Kno- chen nach Implantation von Glaskeramik in den Schweinekiefer,” Dis- sertation, Freie Universitat Berlin, 1979. G. Piotrowski, L. L. Hench, W. C. Allen, and G. L. Miller, “Mechanical studies of the bone bioglass interfacial bond,“ 1. Biomed. Muter. Res.
W. A. Beresford, Chondroid Bone, Secondary Cartilage and Metaplasia, Ur- ban & Schwarzenberg, Baltimore, 1981. M.E. Holtrop, ”The origin of bone cells in enchondral ossification,” Third Europ. Symp. Calc. Tiss., 32-36 (1966). A. H. Reddi, ”The growth and development of cartilage and bone,” in Biochemical Development of the Fetus and Neonate, C . T. Jones, Ed., Elsevier Biomedical Press, Amsterdam, 1982, pp. 163-183. U. Gross and V. Strunz, “Bone connection, a principle for biomaterials engineering in bone and tooth replacement,” in Clinical Applications of Biomaterials, A. J. C. Lee, T. Albrektsson, and P.-I. Branemark, Eds., Wiley, New York, 1982, pp. 237- 244. J . L. Meyer and E. E. Angino, ”The role of trace metals in calcium uro- lithiasis,” Invest. Urol., 14,347-350 (1977).
Symp., 6, 47-61 (1975).

GLASSES IN BONY IMPLANTATION BED 271
36.
37.
38.
39.
40.
41.
42.
43. 44.
45.
46.
47.
48.
F. Pernot, J. Zarzycki, F. Bonnel, P. Rabischong, and P. Baldet, ”New glass-ceramic materials for prosthetic applications,” I. Mater. Sci., 14, 1694-1706 (1979). U. Gross, F. Schmelzer, and V. Strunz, “Tissue reactions to enamel with glass ceramic particles for coating of metals,” presented at the Eighth Annual Meeting of the Society for Biomaterials, Orlando, Florida, April 24-27, 1982. U. M. Gross and V. Strunz, ”Effects of EHDP on the development of bone connection to a glass ceramic implant in the femur of rats,” in Current Advances in Skeletogenesis, M. Silbermann and H. C. Slavkin, Eds., Excerpta Medica, Amsterdam, 1982, pp. 239-246. H. C. Anderson, “Vesicles associated with calcification in the matrix of epiphyseal cartilage,” I. Cell Biol., 41, 59-72 (1969). E. Bonucci, “Fine structure and histochemistry of ’calcifying globules’ in epiphyseal cartilage,” Z . Zellforsch., 103, 192-217 (1970). R. G. G. Russell and H. Fleisch, ”Pyrophosphate and diphosphonates,” in The Biochemistry and Physiology of Bone, 2nd ed., Vol. 4, G. H. Bourne, Ed., Academic Press, New York, 1976, pp. 61-104. H. J. Hohling, R. Kreilos, G. Neubauer, and A. Boyde, ”Electron micros- copy and electron microscopical measurements of collagen mineral- ization in hard tissues,” Z. Zellforsch., 122, 36-52 (1971). E. Pfeil, personal communication, 1982. B. A. Harhvig and L. L. Hench, “The epitaxy of poly-L-alanine on L- quartz and a glass-ceramic,” I. Biomed. Mater. Res., 6, 413-423 (1972). Ch., P. A. T. Klein, G. J. van Kamp, and K. de Groot, ”A possible signifi- cance of immunoproteins in the phagocytic recognition of the implant material hydroxylapatite,” presented at the Seventh Annual Meeting of the Society for Biomaterials, Troy, N.Y., May 28-31, 1981. T.L. Seitz, K.D. Noonan, L.L. Hench, and N.E. Noonan, ”Effect of fibronectin on the adhesion of an established cell line to a surface reac- tive biomaterial,” I. Biomed. Mater. Res., 16, 195-207 (1982). U. Gross, Th. Rudiger, and V. Strunz, ”Adsorption of fibronectin at the surface of implants,” poster, presented at the Symposium on Implant Stimulated Interface Reactions, Berlin, February 18-19, 1983. J. Termine, ”Phenotypic proteins of calf lamellar bone,” in Current Ad- vances in Skeletogenesis, M. Silbermann and H. C. Slavkin, Eds., Internat. Congress Series 589, Excerpta Medica, Amsterdam, 1982, pp. 3-7.
Received May 1, 1983 Accepted July 1, 1984