Embed Size (px)
Citation preview
11/18/20
1
The Mental and Behavioral Health Implications of HIV and COVID-19
Debbie Cestaro-Seifer, MS, RN, NC-BC, CTPUniversity of Florida Department of Medicine
1
1
Disclosures§ The activity planners and speaker do not have any financial relationships
with commercial entities to disclose. § The speaker will not discuss any off-label use or investigational product
during the program.
This slide set has been peer-reviewed to ensure that there are no conflicts of interest represented in the presentation.
2
2
11/18/20
2
Learning ObjectivesBy the end of the session participants will be able to:
§ Identify three mental/behavioral health conditions that can be experienced by people with HIV (PWH).
§ Describe a few of the psychological effects of COVID-19 described in the literature.
§ Identify three interventions that support an integrated person-centered approach to HIV care during virtual care visits.
§ Discuss strategies that support the emotional wellbeing and resilience of both patients and healthcare professionals.
3
3
Presentation Topics
§ Psychological impact of HIV and COVID-19
§ Screening tools to identify mental/behavioral health needs
§ Promoting emotional wellness virtually and in person
4Image accessed on 11/16/2020 at www.pixabay.com
4
11/18/20
3
HIV Mental and Behavioral Health Concerns
5
5
HIV Chronic Disease Management
1. Cope with intense, sometimes debilitating emotions
2. Change behaviors to minimize the impact of HIV and maximize antiretroviral (ARV) treatment
3. Manage the disruptions HIV may cause for work, school, social, spiritual and family life
6Stanton AL, Revenson TA, Tennen H. Health psychology: psychological adjustment to chronic disease. Annu Rev Psychol. 2007; 58: 565-92.
6
11/18/20
4
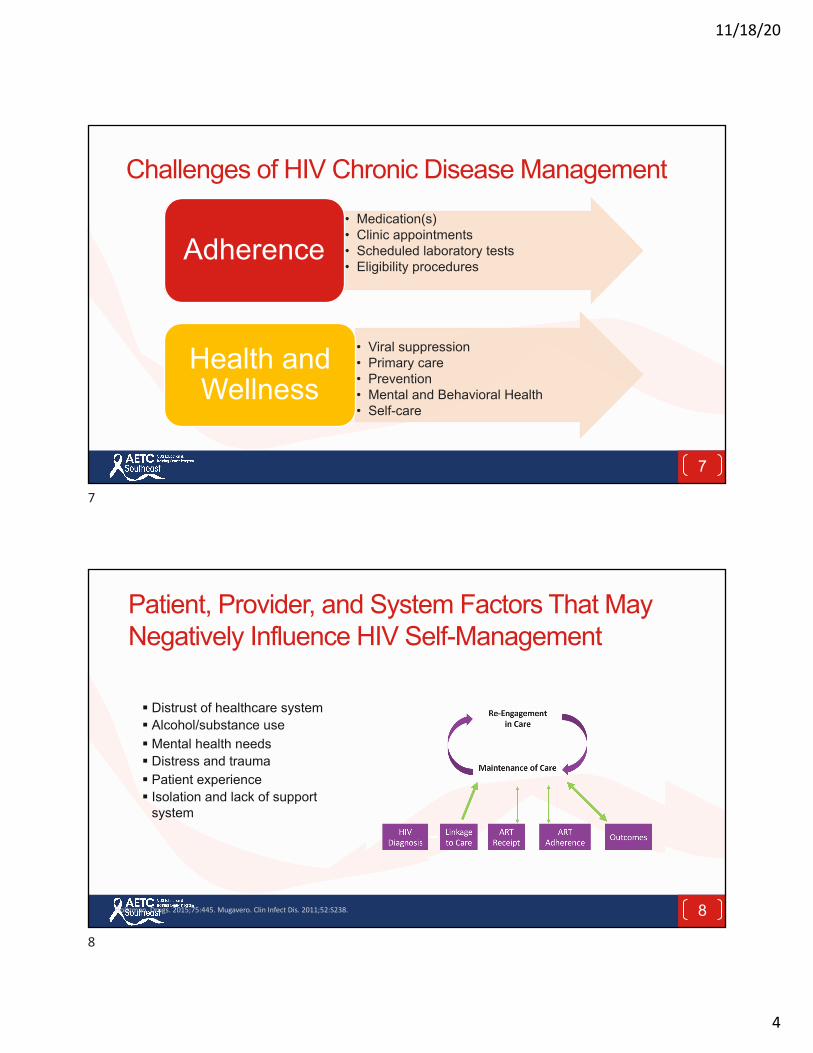
Challenges of HIV Chronic Disease Management • Medication(s)• Clinic appointments• Scheduled laboratory tests• Eligibility procedures
Adherence
• Viral suppression• Primary care• Prevention• Mental and Behavioral Health• Self-care
Health and Wellness
7
7
Patient, Provider, and System Factors That May Negatively Influence HIV Self-Management
Holtzman. Drugs. 2015;75:445. Mugavero. Clin Infect Dis. 2011;52:S238.
§ Distrust of healthcare system§ Alcohol/substance use§ Mental health needs§ Distress and trauma§ Patient experience§ Isolation and lack of support
system
8
8
11/18/20
5
Mind Mapping
9
Mental Health and HIV
9
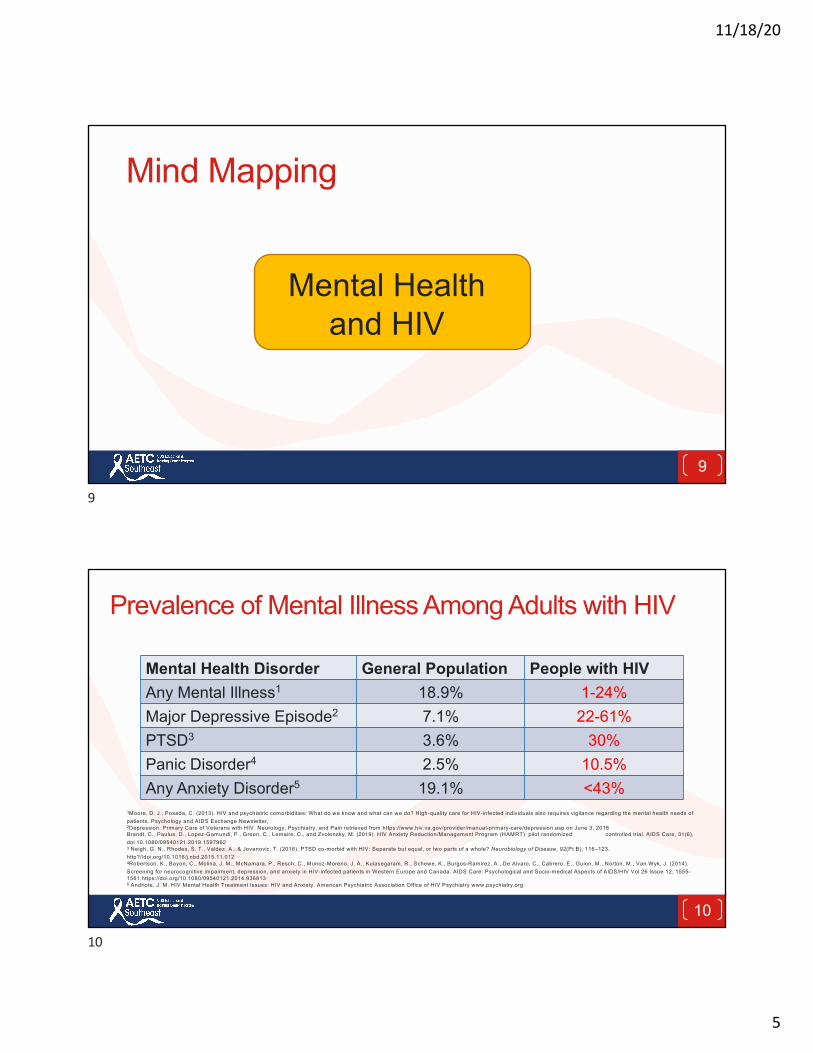
Prevalence of Mental Illness Among Adults with HIV
Mental Health Disorder General Population People with HIVAny Mental Illness1 18.9% 1-24%Major Depressive Episode2 7.1% 22-61%PTSD3 3.6% 30%Panic Disorder4 2.5% 10.5%Any Anxiety Disorder5 19.1% <43%
1Moore, D. J., Posada, C. (2013). HIV and psychiatric comorbidities: What do we know and what can we do? High-quality care for HIV-infected individuals also requires vigilance regarding the mental health needs of patients. Psychology and AIDS Exchange Newsletter, 2Depression. Primary Care of Veterans with HIV. Neurology, Psychiatry, and Pain retrieved from https://www.hiv.va.gov/provider/manual-primary-care/depression.asp on June 3, 2018Brandt, C., Paulus, D., Lopez-Gamundi, P., Green, C., Lemaire, C., and Zvolensky, M. (2019). HIV Anxiety Reduction/Management Program (HAMRT): pilot randomized controlled trial. AIDS Care, 31(6), doi 10.1080/09540121.2019.15979623 Neigh, G. N., Rhodes, S. T., Valdez, A., & Jovanovic, T. (2016). PTSD co-morbid with HIV: Separate but equal, or two parts of a whole? Neurobiology of Disease, 92(Pt B), 116–123. http?//doi.org/10.1016/j.nbd.2015.11.0124Robertson, K., Bayon, C., Molina, J. M., McNamara, P., Resch, C., Munoz-Moreno, J. A., Kulasegaram, R., Schewe, K., Burgos-Ramirez, A., De Alvaro, C., Cabrero, E., Guion, M., Norton, M., Van Wyk, J. (2014). Screening for neurocognitive impairment, depression, and anxiety in HIV-infected patients in Western Europe and Canada. AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIV Vol 26 Issue 12, 1555-1561 https://doi.org/10.1080/09540121.2014.9368135 Andriote, J. M. HIV Mental Health Treatment Issues: HIV and Anxiety. American Psychiatric Association Office of HIV Psychiatry www.psychiatry.org
10
10
11/18/20
6
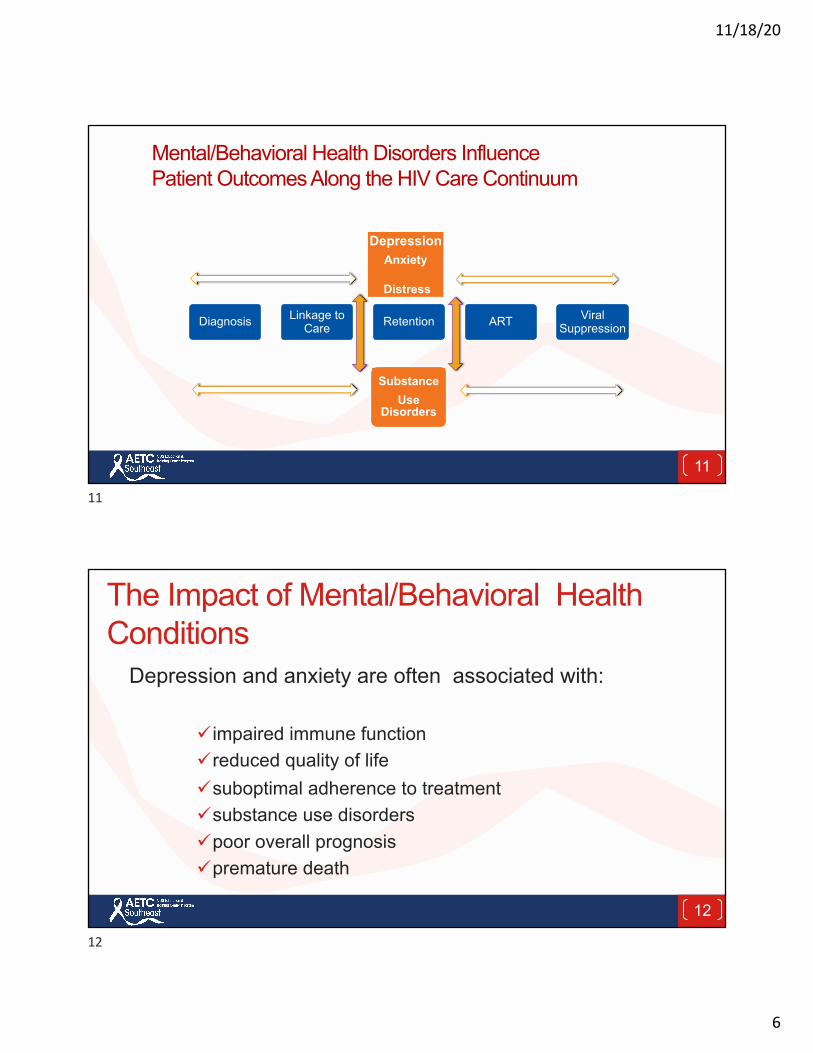
Mental/Behavioral Health Disorders Influence Patient Outcomes Along the HIV Care Continuum
Diagnosis Linkage to Care Retention ART Viral
Suppression
Substance Use
Disorders
DepressionAnxiety
Distress
11
11
The Impact of Mental/Behavioral Health Conditions
Depression and anxiety are often associated with:
ü impaired immune function üreduced quality of life üsuboptimal adherence to treatmentüsubstance use disorders üpoor overall prognosis üpremature death
12
12
11/18/20
7
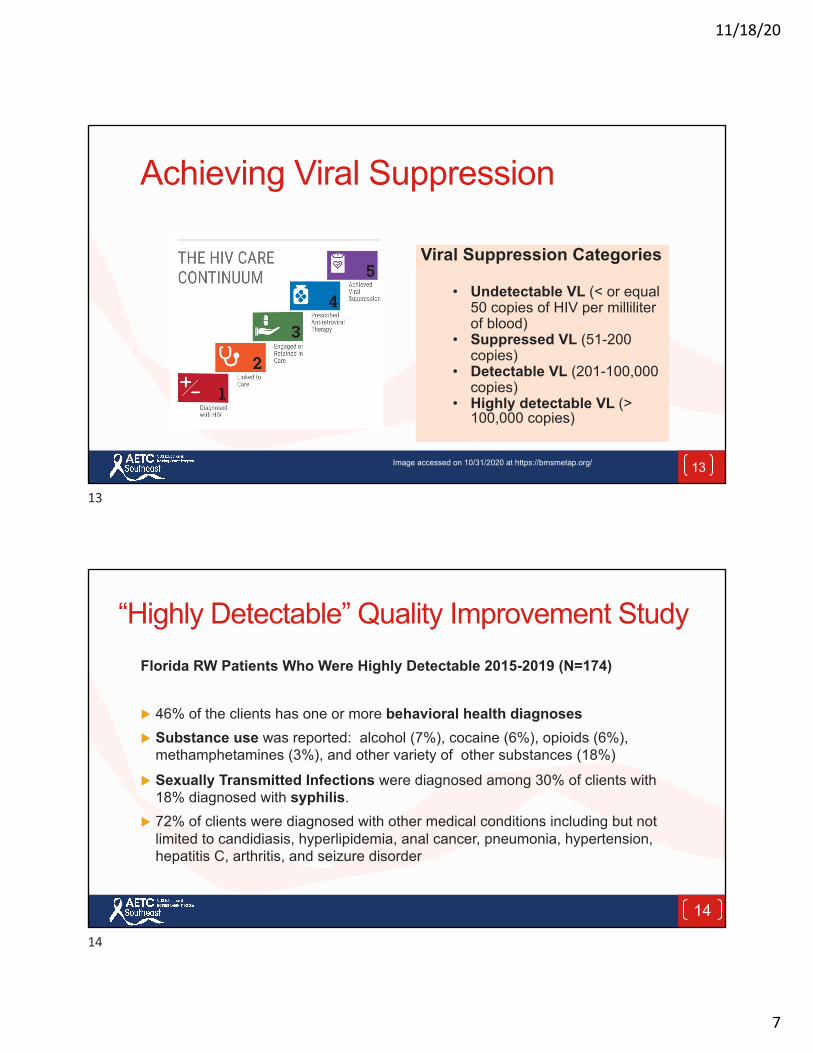
Achieving Viral Suppression
Viral Suppression Categories
• Undetectable VL (< or equal 50 copies of HIV per milliliter of blood)
• Suppressed VL (51-200 copies)
• Detectable VL (201-100,000 copies)
• Highly detectable VL (> 100,000 copies)
13Image accessed on 10/31/2020 at https://bmsmetap.org/
13
“Highly Detectable” Quality Improvement Study
14
Florida RW Patients Who Were Highly Detectable 2015-2019 (N=174)
u 46% of the clients has one or more behavioral health diagnosesu Substance use was reported: alcohol (7%), cocaine (6%), opioids (6%),
methamphetamines (3%), and other variety of other substances (18%)
u Sexually Transmitted Infections were diagnosed among 30% of clients with 18% diagnosed with syphilis.
u 72% of clients were diagnosed with other medical conditions including but not limited to candidiasis, hyperlipidemia, anal cancer, pneumonia, hypertension, hepatitis C, arthritis, and seizure disorder
14
11/18/20
8
Balancing Mental Health in HIV Treatment and Care
Patient Strengths
Most Common
Mental Health Disorders
Trauma
Substance Use Disorders
Anxiety
Depression
Personality Strengths
Resiliency and social support
15
15
Depression: Most common health disorder among PWH
Longitudinal study of 5927 patients receiving HIV care for 1-6 years Consecutive depression screenings conducted 2005-2015
§ 50% spent less than 34 months of the 10-year study depressed; 3.6% were depressed the entire time period
§ For every 25% increase in days depressed, there was an 8% increase in missed appointments AND 5% increase in likelihood of having a detectable viral load
There is an association between mood disorders and HIV treatment outcomes.
(2014) Psychiatry and Clinical Neurosciences: Pence, B. & Bengtson, A. (2018) Improvements in depression and changes in quality of life among HIV-infected adults, Aug 8, AIDS Care. 16
16
11/18/20
9
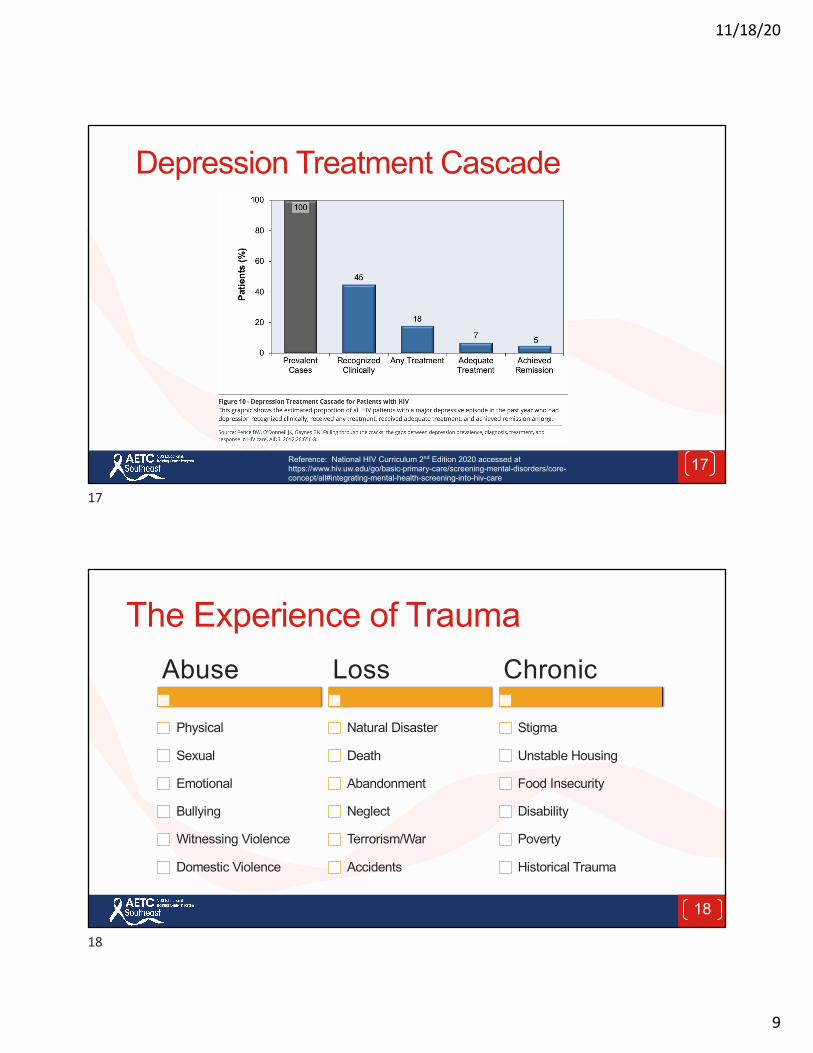
Depression Treatment Cascade
17Reference: National HIV Curriculum 2nd Edition 2020 accessed at https://www.hiv.uw.edu/go/basic-primary-care/screening-mental-disorders/core-concept/all#integrating-mental-health-screening-into-hiv-care
17
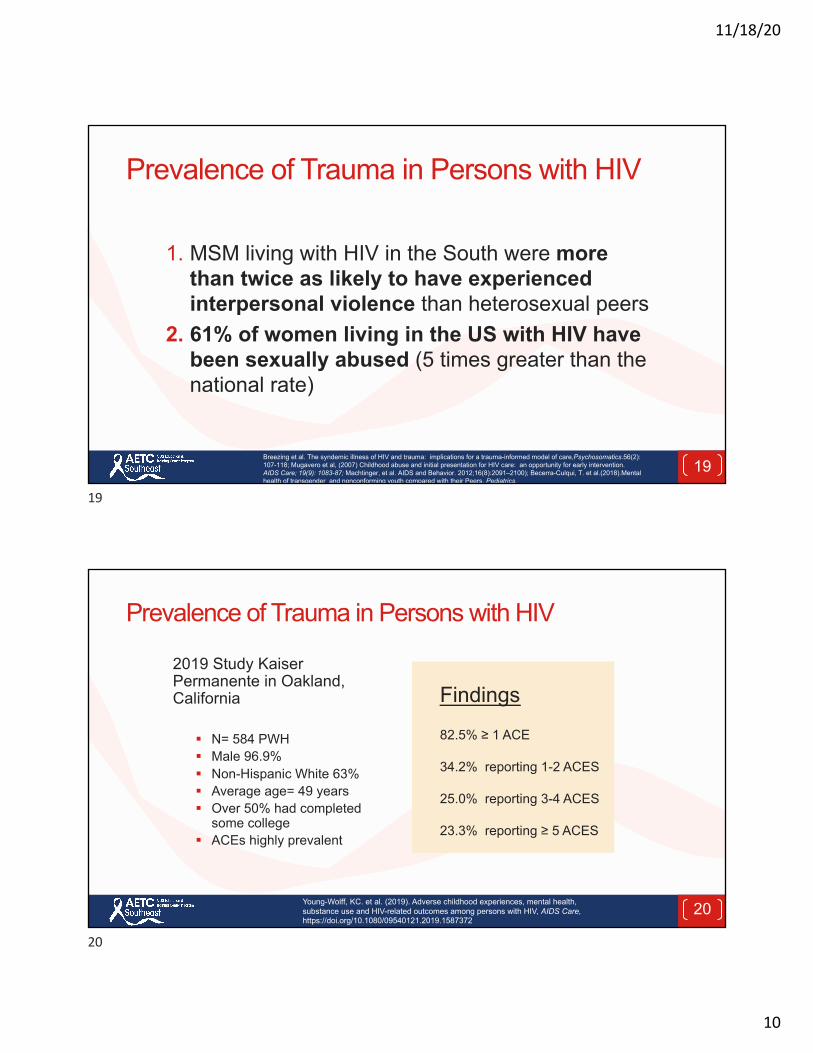
The Experience of Trauma
18
Abuse
Physical
Sexual
Emotional
Bullying
Witnessing Violence
Domestic Violence
Loss
Natural Disaster
Death
Abandonment
Neglect
Terrorism/War
Accidents
Chronic
Stigma
Unstable Housing
Food Insecurity
Disability
Poverty
Historical Trauma
18
11/18/20
10
Prevalence of Trauma in Persons with HIV
1. MSM living with HIV in the South were more than twice as likely to have experienced interpersonal violence than heterosexual peers
2. 61% of women living in the US with HIV have been sexually abused (5 times greater than the national rate)
Breezing et al. The syndemic illness of HIV and trauma: implications for a trauma-informed model of care,Psychosomatics.56(2): 107-118; Mugavero et al, (2007) Childhood abuse and initial presentation for HIV care: an opportunity for early intervention. AIDS Care; 19(9): 1083-87; Machtinger, et al. AIDS and Behavior. 2012;16(8):2091–2100); Becerra-Culqui, T. et al.(2018).Mental health of transgender and nonconforming youth compared with their Peers, Pediatrics.
19
19
Prevalence of Trauma in Persons with HIV
2019 Study Kaiser Permanente in Oakland, California
§ N= 584 PWH§ Male 96.9%§ Non-Hispanic White 63%§ Average age= 49 years§ Over 50% had completed
some college§ ACEs highly prevalent
Findings
82.5% ≥ 1 ACE
34.2% reporting 1-2 ACES
25.0% reporting 3-4 ACES
23.3% reporting ≥ 5 ACES
20Young-Wolff, KC. et al. (2019). Adverse childhood experiences, mental health, substance use and HIV-related outcomes among persons with HIV, AIDS Care, https://doi.org/10.1080/09540121.2019.1587372
20
11/18/20
11
HIV AND COVID-19Mental and Behavioral Health Concerns
21
21
The Influence of COVID-19 on Emotional Health
22Images accessed on 11/15/2020 at www. pixabay.com
22
11/18/20
12
Mind Mapping
23
Social Distancing
23
COVID-19 Related Mental Health Concerns§ Interpersonal and domestic violence§ Social isolation and loneliness§ Sleep difficulties § Post traumatic symptoms§ Moral distress§ Grief § Anxiety§ Depression
24
24
11/18/20
13
Presence of Trauma Symptoms During COVID-19 Pandemic
COVID-19 is a traumatic life event§ PTSD Checklist for DSM-5 (20-item self-report measure)§ Pittsburg Sleep Quality Index§ Wuhan, China§ N=285§ 54.4% female, 45.6 male§ 52.3% > 35 years of age
§ 60.7% some college
25Reference: Nianqi Liu et al. (2020). Prevalence and predictors of PTSS during COVID-19 outbreak in Chinahardest-hit areas: Gender differences matter .Psychiatry Research, May.
25
Presence of Trauma Symptoms During COVID-19 Pandemic
§ Nearly 1 in 10 people (7%) reported post traumatic stress symptoms (PTSS)
§ Prevalence slightly higher in women in the domains of re-experiencing, negative alterations in cognition or mood, and hyper-arousal
§ Subjective sleep quality correlated with PTSS Scores (better sleep= fewer traumatic stress symptoms)
26Reference: Nianqi Liu et al. (2020). Prevalence and predictors of PTSS during COVID-19 outbreak in Chinahardest-hit areas: Gender differences matter .Psychiatry Research, May.
26
11/18/20
14
Mind Mapping
27
Grief
27
Disruptive and Confusing Times
28
28
11/18/20
15
Supporting Mental/Behavioral Health Needs
1. Safety2. Screening3. Access
29
29
SAFETYTrauma Informed Care
30
30
11/18/20
16
Mind Mapping
31
Emotional Safety
31
Trauma Informed OrganizationA trauma-informed service organization:
§ Realizes widespread impact of trauma and understands potential paths for recovery
§ Recognizes signs and symptoms of trauma in clients, staff, and others involved with the system
§ Responds by fully integrating knowledge about trauma into policies, procedures, and practices
§ Seeks to actively resist re-traumatization
Reference: Substance Abuse and Mental Health Services Administration (SAMHSA, 2014) 32
32
11/18/20
17
Trauma Informed Organizations Support Emotional Safety
Scanned with CamScanner
§ Regain emotional control § Stabilize and reduce risk-
taking behaviors § Experience security and
hopefulness
33
33
Polling Question Using a scale of 0-10, with 0 being a clinic/agency having no formal trauma-informed practices, policies or procedures and 10 being a clinic/agency that has a formal and comprehensive trauma-informed system of care with written practices, policies and procedures, choose a number that describes your clinic or organization.
34
34
11/18/20
18
Mind Mapping
35
Asking for Help
35
Proactive Emotional Support
§ Regularly scheduled check-ins§ Real-time virtual and in-person ”huddles” to identify
concerns and unmet needs that provide a ”bridge” to more intensive mental health services
§ Screening
36
36
11/18/20
19
SCREENINGMental and Behavioral Health Symptom
37
37
Mind Mapping
38
Depression Screening Tool
38
11/18/20
20
Report Card: Screening for Depression in HIV Care
Besides identifying an increased risk for depression in HIV, numerous studies show that depression and anxiety in HIV disease is under-recognized and undertreated.
Asch SM, Kilourne AM, Gifford AL, et al. Underdiagnosis of depression in HIV: who are we missing? J Gen Intern ed:2003;18:450-460.Pyne JM, Asch SM, Lincourt K, et al. Quality indicators for depression care in HIV patients. AIDS Care.2008;20:1075-1083
39
39
Screening and Assessment: What is the Difference?
Screening differs from assessment:
§ Screening is a method to evaluate the possible existence of a particular behavioral health problem.
§ Assessment is a method to define the nature of that problem, determine a diagnosis, and develop appropriate treatment recommendations to address the problem or diagnosis.
40
40
11/18/20
21
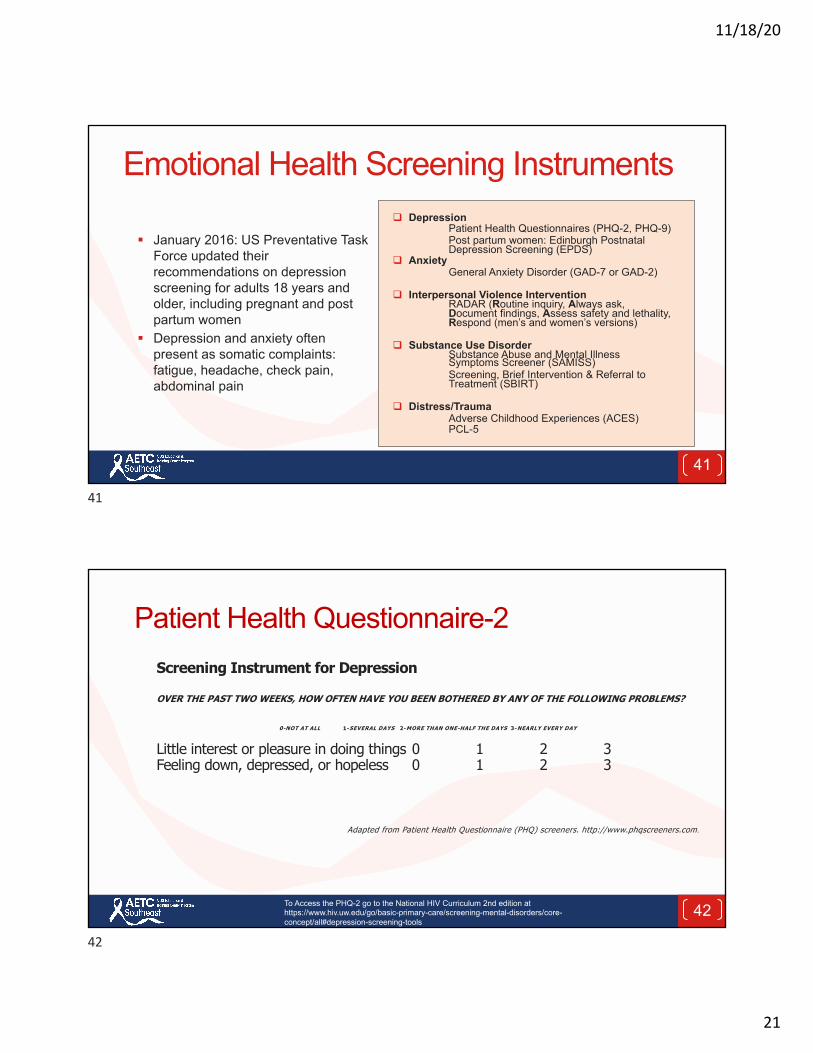
Emotional Health Screening Instruments
§ January 2016: US Preventative Task Force updated their recommendations on depression screening for adults 18 years and older, including pregnant and post partum women
§ Depression and anxiety often present as somatic complaints: fatigue, headache, check pain, abdominal pain
q DepressionPatient Health Questionnaires (PHQ-2, PHQ-9)Post partum women: Edinburgh Postnatal Depression Screening (EPDS)
q AnxietyGeneral Anxiety Disorder (GAD-7 or GAD-2)
q Interpersonal Violence InterventionRADAR (Routine inquiry, Always ask, Document findings, Assess safety and lethality, Respond (men’s and women’s versions)
q Substance Use DisorderSubstance Abuse and Mental Illness Symptoms Screener (SAMISS)Screening, Brief Intervention & Referral to Treatment (SBIRT)
q Distress/TraumaAdverse Childhood Experiences (ACES) PCL-5
41
41
Patient Health Questionnaire-2Screening Instrument for Depression
OVER THE PAST TWO WEEKS, HOW OFTEN HAVE YOU BEEN BOTHERED BY ANY OF THE FOLLOWING PROBLEMS?
0-NOT AT ALL 1-SEVERAL DAYS 2-MORE THAN ONE-HALF THE DAYS 3-NEARLY EVERY DAY
Little interest or pleasure in doing things 0 1 2 3Feeling down, depressed, or hopeless 0 1 2 3
Adapted from Patient Health Questionnaire (PHQ) screeners. http://www.phqscreeners.com.
42To Access the PHQ-2 go to the National HIV Curriculum 2nd edition at https://www.hiv.uw.edu/go/basic-primary-care/screening-mental-disorders/core-concept/all#depression-screening-tools
42
11/18/20
22
“I’m Not Depressed, I’m Just Stressed”PHQ-9 GAD-7
43
43
GAD-2
44To access the GAD-2 go to https://www.hiv.uw.edu/page/mental-health-screening/gad-2
44
11/18/20
23
IPV Screens: RADAR for Women/Men
RADAR: Women RADAR: Men
45http://www.opdv.ny.gov/professionals/health/radar.pdf
45
Adverse Childhood Experiences(ACES) Questionnaire and PCL-5
46
46
11/18/20
24
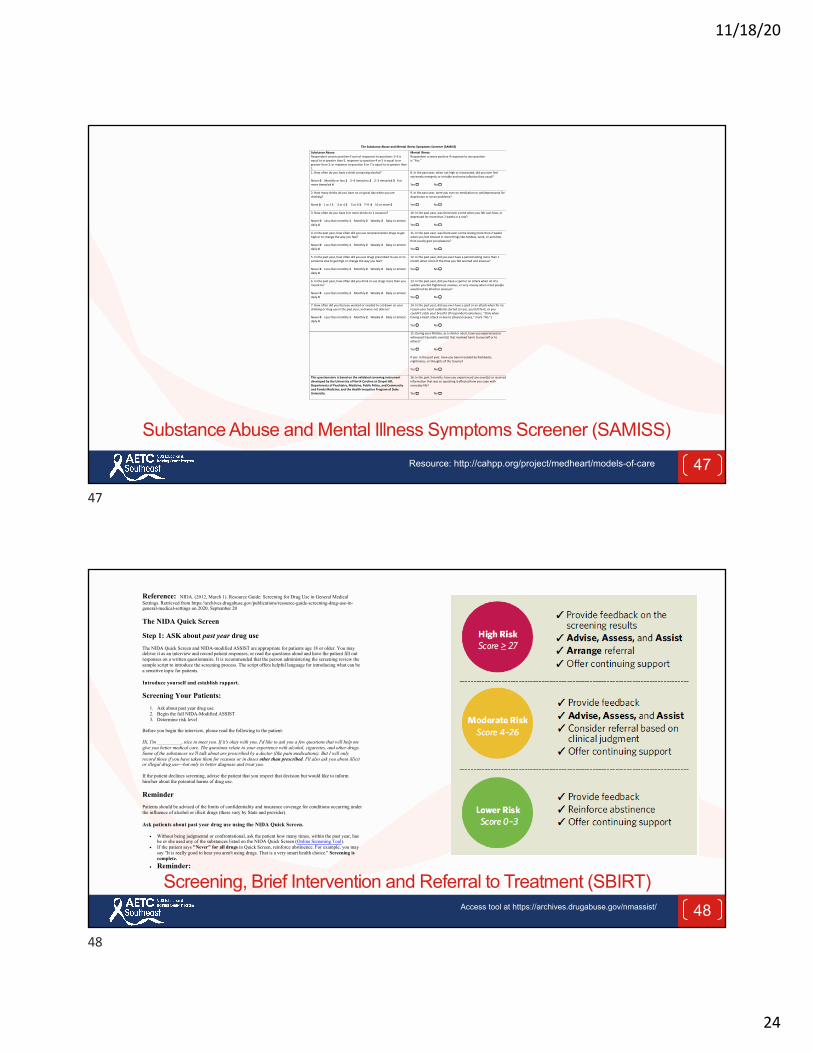
Substance Abuse and Mental Illness Symptoms Screener (SAMISS)
47Resource: http://cahpp.org/project/medheart/models-of-care
The Substance Abuse and Mental Illness Symptoms Screener (SAMISS)
Substance Abuse: Respondent screens positive if sum of responses to questions 1–3 is equal to or greater than 5, response to question 4 or 5 is equal to or greater than 3, or response to question 6 or 7 is equal to or greater than 1.
Mental Illness: Respondent screens positive if response to any question is ‘‘Yes.’’
1. How often do you have a drink containing alcohol? Never 0 Monthly or less 1 2–4 times/mo 2 2–3 times/wk 3 4 or more times/wk 4
8. In the past year, when not high or intoxicated, did you ever feel extremely energetic or irritable and more talkative than usual? Yes !!!! No !!!!
2. How many drinks do you have on a typical day when you are drinking? None 0 1 or 2 1 3 or 4 2 5 or 6 3 7–9 4 10 or more 5
9. In the past year, were you ever on medication or antidepressants for depression or nerve problems? Yes !!!! No !!!!
3. How often do you have 4 or more drinks on 1 occasion? Never 0 Less than monthly 1 Monthly 2 Weekly 3 Daily or almost daily 4
10. In the past year, was there ever a time when you felt sad, blue, or depressed for more than 2 weeks in a row? Yes !!!! No !!!!
4. In the past year, how often did you use nonprescription drugs to get high or to change the way you feel? Never 0 Less than monthly 1 Monthly 2 Weekly 3 Daily or almost daily 4
11. In the past year, was there ever a time lasting more than 2 weeks when you lost interest in most things like hobbies, work, or activities that usually give you pleasure? Yes !!!! No !!!!
5. In the past year, how often did you use drugs prescribed to you or to someone else to get high or change the way you feel? Never 0 Less than monthly 1 Monthly 2 Weekly 3 Daily or almost daily 4
12. In the past year, did you ever have a period lasting more than 1 month when most of the time you felt worried and anxious? Yes !!!! No !!!!
6. In the past year, how often did you drink or use drugs more than you meant to? Never 0 Less than monthly 1 Monthly 2 Weekly 3 Daily or almost daily 4
13. In the past year, did you have a spell or an attack when all of a sudden you felt frightened, anxious, or very uneasy when most people would not be afraid or anxious? Yes !!!! No !!!!
7. How often did you feel you wanted or needed to cut down on your drinking or drug use in the past year, and were not able to? Never 0 Less than monthly 1 Monthly 2 Weekly 3 Daily or almost daily 4
14. In the past year, did you ever have a spell or an attack when for no reason your heart suddenly started to race, you felt faint, or you couldn’t catch your breath? (If respondent volunteers, ‘‘Only when having a heart attack or due to physical causes,’’ mark ‘‘No.’’) Yes !!!! No !!!!
15. During your lifetime, as a child or adult, have you experienced or witnessed traumatic event(s) that involved harm to yourself or to others? Yes !!!! No !!!! If yes: In the past year, have you been troubled by flashbacks, nightmares, or thoughts of the trauma? Yes !!!! No !!!!
This questionnaire is based on the validated screening instrument developed by the University of North Carolina at Chapel Hill, Departments of Psychiatry, Medicine, Public Policy, and Community and Family Medicine; and the Health Inequities Program of Duke University.
16. In the past 3 months, have you experienced any event(s) or received information that was so upsetting it affected how you cope with everyday life? Yes !!!! No !!!!
47
Screening, Brief Intervention and Referral to Treatment (SBIRT)48
Reference: NIDA. (2012, March 1). Resource Guide: Screening for Drug Use in General Medical Settings. Retrieved from https://archives.drugabuse.gov/publications/resource-guide-screening-drug-use-in-general-medical-settings on 2020, September 20
The NIDA Quick Screen
Step 1: ASK about past year drug use
The NIDA Quick Screen and NIDA-modified ASSIST are appropriate for patients age 18 or older. You may deliver it as an interview and record patient responses, or read the questions aloud and have the patient fill out responses on a written questionnaire. It is recommended that the person administering the screening review the sample script to introduce the screening process. The script offers helpful language for introducing what can be a sensitive topic for patients.
Introduce yourself and establish rapport.
Screening Your Patients:
1. Ask about past year drug use 2. Begin the full NIDA-Modified ASSIST 3. Determine risk level
Before you begin the interview, please read the following to the patient:
Hi, I'm __________, nice to meet you. If it's okay with you, I'd like to ask you a few questions that will help me give you better medical care. The questions relate to your experience with alcohol, cigarettes, and other drugs. Some of the substances we'll talk about are prescribed by a doctor (like pain medications). But I will only record those if you have taken them for reasons or in doses other than prescribed. I'll also ask you about illicit or illegal drug use—but only to better diagnose and treat you.
If the patient declines screening, advise the patient that you respect that decision but would like to inform him/her about the potential harms of drug use.
Reminder Patients should be advised of the limits of confidentiality and insurance coverage for conditions occurring under the influence of alcohol or illicit drugs (these vary by State and provider).
Ask patients about past year drug use using the NIDA Quick Screen.
• Without being judgmental or confrontational, ask the patient how many times, within the past year, has he or she used any of the substances listed on the NIDA Quick Screen (Online Screening Tool).
• If the patient says "Never" for all drugs in Quick Screen, reinforce abstinence. For example, you may say "It is really good to hear you aren't using drugs. That is a very smart health choice." Screening is complete.
• Reminder:
Access tool at https://archives.drugabuse.gov/nmassist/
48
11/18/20
25
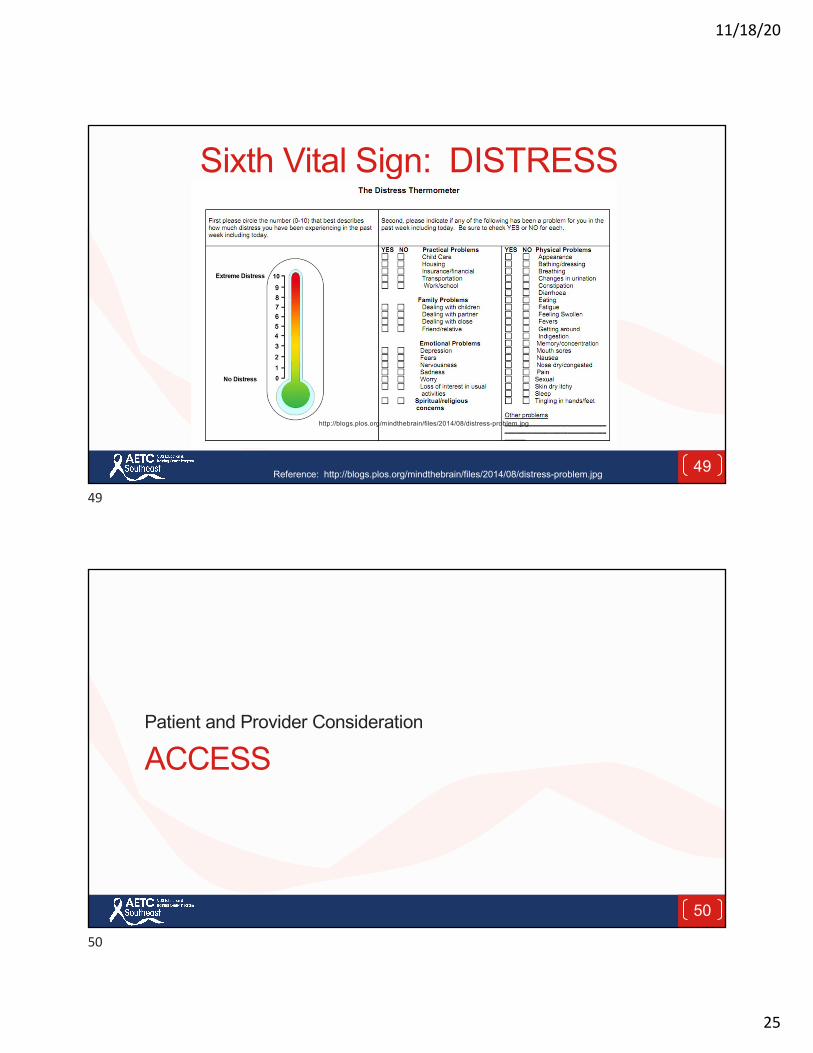
Sixth Vital Sign: DISTRESS
http://blogs.plos.org/mindthebrain/files/2014/08/distress-problem.jpg
Reference: http://blogs.plos.org/mindthebrain/files/2014/08/distress-problem.jpg 49
49
ACCESSPatient and Provider Consideration
50
50
11/18/20
26
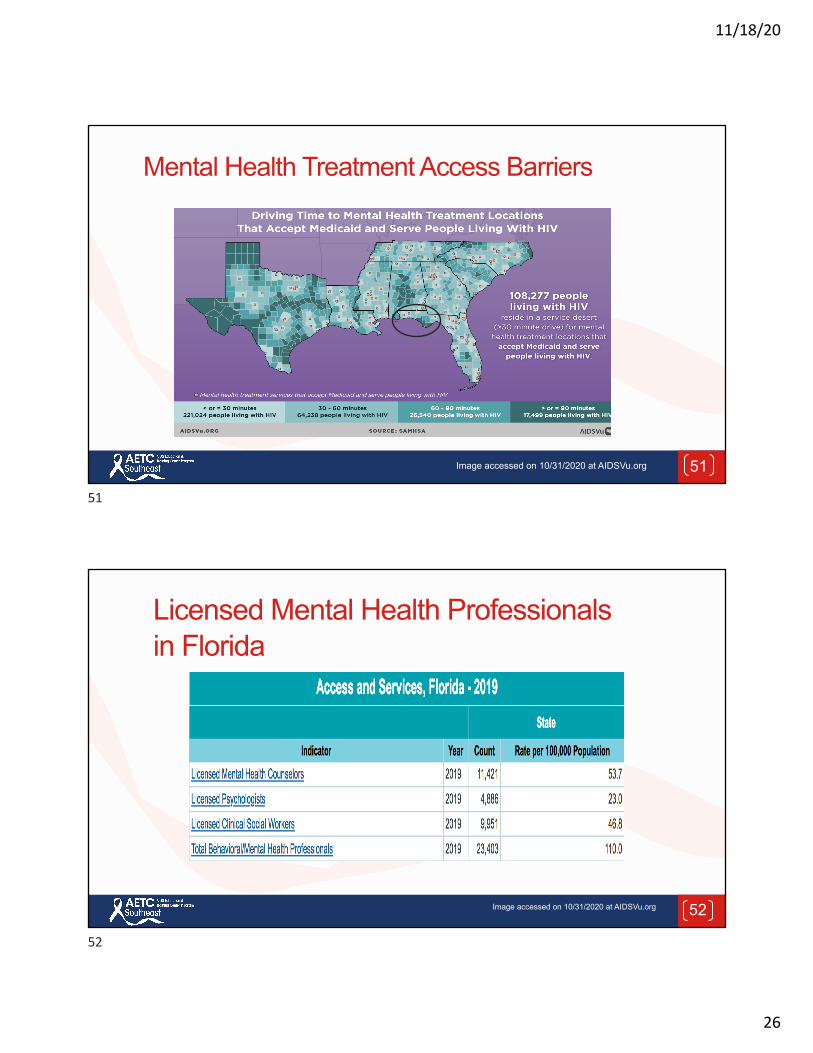
Mental Health Treatment Access Barriers
51Image accessed on 10/31/2020 at AIDSVu.org
51
Licensed Mental Health Professionals in Florida
52Image accessed on 10/31/2020 at AIDSVu.org
52
11/18/20
27
Mental/Behavioral Health Service Delivery Models
Siloed Services Integrated Services
53Images accessed on 11/16/2020 at http://www.clipartpanda.com
53
Opportunities Promising advances have been made to integrate mental health care into HIV primary care that include but are not not limited to § Collaborative Model§ Task-shifting§ Stepped care interventions§ Public awareness campaigns that normalize
whole health care to reduce stigma and psychological distress
54Reference: Remien, Robert H.; Stirratt, Michael J.; Nguyen, Nadiaa; Robbins, Reuben N.; Pala, Andrea N.; Mellins, Claude A. Mental health and HIV/AIDS, AIDS: July 15, 2019 - Volume 33 -Issue 9 - p 1411-1420
54
11/18/20
28
Reframe Mental/Behavioral Health for Consumers, Providers and Staff
Emotional Fitness§ Focus on strengths and
resilience building§ Integrate emotional fitness into
whole health HIV primary care§ Stay connected to HIV care
55Reference: Accessed on 11/1/2020 at https://www.journeyworks.com/Emotional-Fitness-8-Tips-for-a-Stronger-You/productinfo/5804/
JourneyWorks Publishing (2016)
55
Integrative Models of Care
§ Better health outcomes
§ “Whole health” perspective
§ Reduced stigma § Improved access to
health care § Improved retention
and ARV adherence
Accessed on 2/16/2019 at https://pixabay.com/en/icon-medical-illness-health-1674909/ 56
56
11/18/20
29
Collaborative Model Co-location of HIV Primary Care Services and Behavioral Health Services
§ Behavioral health specialists work side-by-side with HIV primary care providers
§ Behavioral health specialists visit the HIV primary care clinic several days a week to provide assessments, treatment and follow-up
§ Behavioral health specialists work in the same building or across the street from the HIV primary care providers
57
57
Task Shifting
Shift responsibilities for mental/behavioral health screening from highly qualified health workers to health workers with less training and fewer qualifications
58Image accessed on 11/1/2020 at https://pixabay.com/illustrations/hands-holding-letters-red-task-2886016/
58
11/18/20
30
Stepped-care Intervention Model
Triage intervention intensity based upon observed
patient need
Example: If a patient does not benefit from a level intervention provided by a specially trained community health worker providing cognitive behavioral therapy for depression and ART adherence, they are triaged to a more intensive treatment provided by a licensed professional (nurse or mental health counselor)
59Image accessed on 11/1/2020 at https://pixabay.com/illustrations/search/levels%20of%20care/
59
Integrated Programs Encourage Patient and Employee Self-Care
60Image accessed on 6/13/2020 at www.pixabay.com.
60
11/18/20
31
Integrated Programs Work to Build Employee and Patient Resiliency
61
61
Encourage Connections and Support Circles
62
62

11/18/20
32
Encourage the Practice of Self Care
Sleep is Self Care
63Image accessed on 10/18/2020 at https://pixabay.com/illustrations/bed-sleep-meditate-meditation-1013957/
63
Cultivate Ways to Be More Calm
64
64
11/18/20
33
Grounding Intervention
65
BREATH FEET BODY
65
661-minute times for relaxation: Utube video https://youtu.be/wMFbBct-p7c
66
11/18/20
34
Lines of Connection During Social Distancing
67Image accessed on 11/17/2020 at www.pixabay.com
67
Mind Mapping
68
Integrated HIV Care
68
11/18/20
35
Provide Safety, Screening and AccessWhat patients don’t share with us hurts them, so healthcare organizations must focus on providing:
§ Non-judgmental whole person healthcare systems and processes§ Routine screening for emotional symptoms and conditions during
in person and virtual care visits§ Trauma informed care, with timely and responsible referrals to
mental and behavioral health professionals § Integrated care practices that support and routinize discussions
about emotional health and emotional fitness
69
69
Questions and Discussions
70
70
11/18/20
36
Speaker Contact Information
Debbie Cestaro-Seifer, MS, RN, NC-BC, CTP
Email: [email protected]
71
71