Embed Size (px)
Citation preview

The Myths of Heart Failure with Preserved Ejection
Fraction: A misunderstood disease in search
of a therapyScott D. Solomon, MD
The Edward D. Frohlich Distinguished Chair Professor of Medicine
Harvard University Director, Noninvasive Cardiology Brigham and Women’s Hospital

DISCLOSURES
• Dr. Solomon has received research Support from Abbott, Amgen, Bayer, Boston Scientific, Daichi-Sankyo, Novartis, NHLBI, NCI, and has consulted for Novartis, Bayer

The Two Faces of Heart Failure
HFrEF HFpEF
Heart Failure Definition• The inability to provide adequate cardiac
output to the body at rest or with exertion, or to do so only in the setting of elevated cardiac filling pressures.
•Clinically: A clinical syndrome characterized by breathlessness, fatigue and edema caused by an abnormality of the heart
-E. Braunwald modified by B. Borlaug and M. Redfield

Distribution of EF in Hospitalized Patients With Heart Failure
EF 4
0-50
%
Fonarow G et al. JACC. 2007; 50:768-777.
EF ≥
50
%
OPTIMIZE-HF Registry, N=41,267
EF ≤
40
%

Similar Signs and Symptoms in Patients with HFpEF and HFrEF
HFpEFHFrEF
35
30
25
20
15
10
5
0
%
Edema Orthop- nea
PND Restdyspnea
S3 Crackles JVP>6 cm
Cardio-megaly
CHARM Investigators

MYTH #1
HFpEF is very benign compared with HFrEF
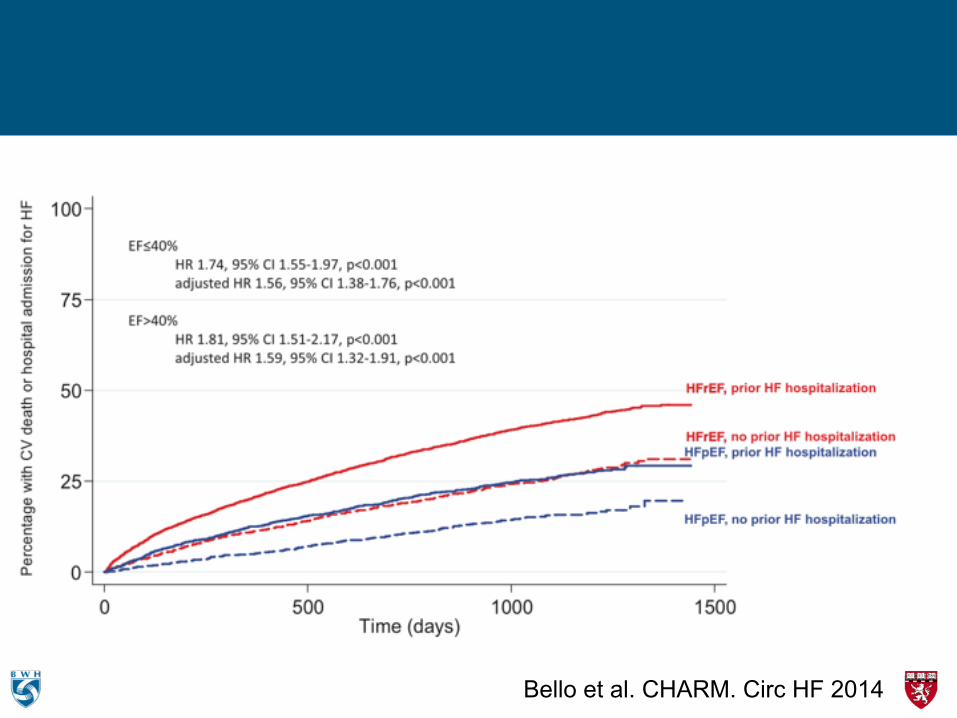
Bello et al. CHARM. Circ HF 2014

Survival rates have improved for HFrEF, but not for HFpE F
• The survival rate among patients with a discharge diagnosis of HFpEF has not changed significantly over time1
– Among patients with HFrEF, the likelihood of survival increased from 1987 to 2001
Sur
viva
l
1.0
0.8
0.6
0.4
0.2
0
Patients with reduced ejection fraction Patients with preserved ejection fraction
0 1 2 3 4 5 Year
1987–1991 1992–1996 1997–2001
Sur
viva
l
1.0
0.8
0.6
0.4
0.2
0 0 1 2 3 4 5
Year
p=0.005 p=0.36
1987–1991 1992–1996 1997–2001
▪ Advances in the management of patients with HFrEF have resulted in a significant extension of life expectancy, but this is not the case for patients with HFpEF2
1. Owan et al. N Engl J Med 2006;355:251–9; 2. Blanche et al. Swiss Med Wkly 2010;140:66–729
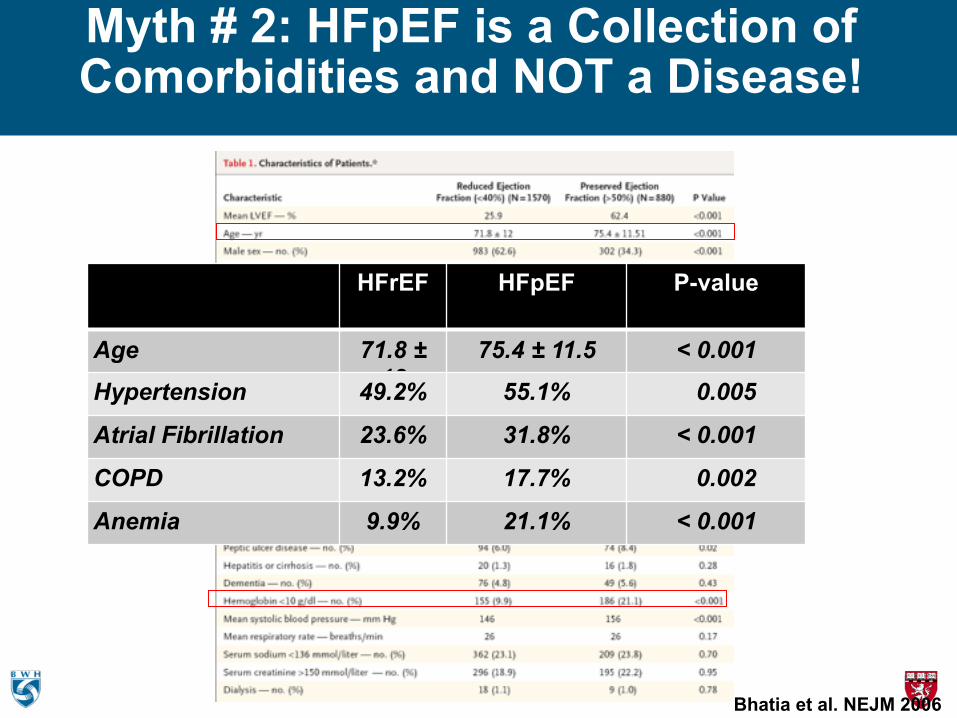
Myth # 2: HFpEF is a Collection of Comorbidities and NOT a Disease!
Bhatia et al. NEJM 2006
HFrEF HFpEF P-value
Age 71.8 ± 12
75.4 ± 11.5 < 0.001
Hypertension 49.2% 55.1% 0.005
Atrial Fibrillation 23.6% 31.8% < 0.001
COPD 13.2% 17.7% 0.002
Anemia 9.9% 21.1% < 0.001

HF Hospitalization and Mortality Higher in HFpEF than in Studies of Similar Comorbidity
0
17,5
35
52,5
70
ACCORD ACTION PEACE HOPE ALLHAT CHARM-P
MortalityHF Hosp

MYTH #3
HFpEF is Caused by Diastolic Dysfunction

Age Dependence of Myocardial Relaxation Velocity in Normals
40 50 60 70 80 904
8
12
16
20
24
Age (Years)
Late
ral E
' (cm
/sec
)
Henein et al. EHJ. 2002;23:162–171.

High Prevalence of Diastolic Dysfunction Regardless of Clinical Status
0
12,5
25
37,5
50
Healthy Co-Morbid HFpEF
5,52,31,6
424242 4341
26
10
15
30
NormalMild DDModerate DDSevere DD
• No DM, HTN, CHD, HF
n = 371 n = 4,555 n = 474
E’ = 7.5 ± 1.9, E/E’ = 9.1 ± 3.0 NT-proBNP = 90 (83,97)
E’ = 6.9 ± 1.9, E/E’ = 10.2 ± 3.8 NT-proBNP = 120 (116, 123)
E’ = 6.7 ± 1.9, E/E’ = 11.2 ± 4.7 NT-proBNP = 209 (188, 232)
Shah et al AHA 2012

Diastolic Dysfunction is Ubiquitous with Aging and Cannot Account for HFpEF

Myth # 5: Systolic Function is Normal in HFpEF
Longitudinal Strain most likely represents Function of subendocardial myofiber bands
Shah A. & Solomon SD. Myocardial Deformation Imaging. Circulation 2012

Myocardial Strain in Normals, HTN, HFpEF and HFrEF
Normal (n=50)
Hypertension and Diastolic dysfunction
(n=300)PARAMOUNT1
(n=~200) MADIT-CRT2 (n=1077)
-34-32-30-28-26-24-22-20-18-16-14-12-10
-8-6-4-20
Myo
card
ial S
train
(%)
Longitudinal Strain Circumferential Strain
TOPCAT3
(n=~438)
1Kraigher-Krainer E, JACC 2013 2Knappe D, Circ HF 2011 3 TOPCAT Unpublished
No HF HFpEF HFrEF
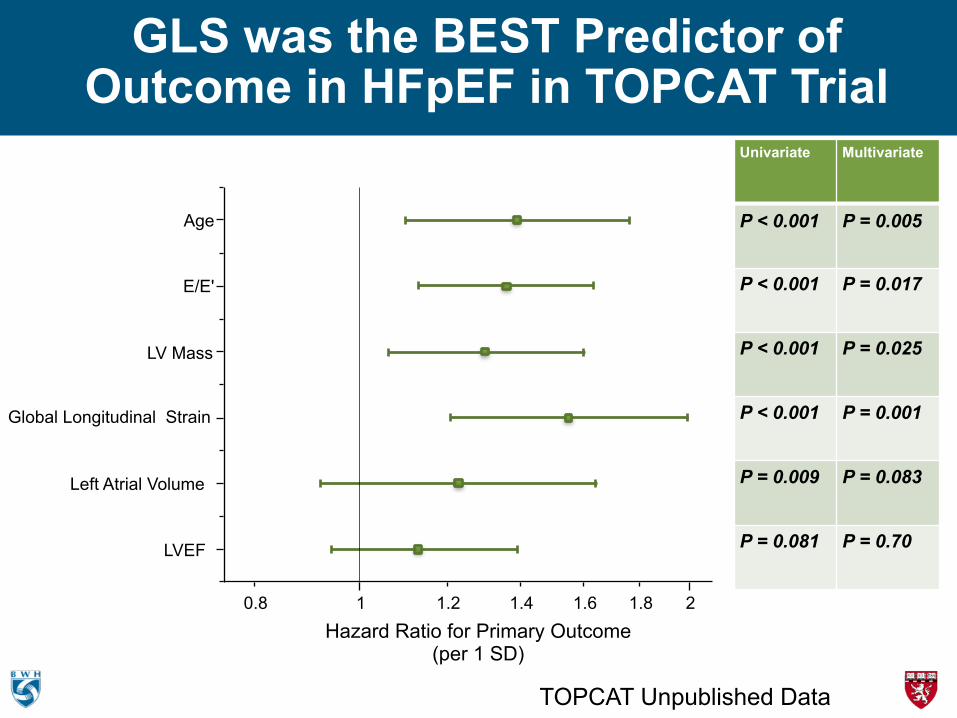
GLS was the BEST Predictor of Outcome in HFpEF in TOPCAT Trial
LVEF
Left Atrial Volume
Global Longitudinal Strain
LV Mass
E/E'
Age
0.8 1 1.2 1.4 1.6 1.8 2
Hazard Ratio for Primary Outcome (per 1 SD)
Univariate Multivariate
P < 0.001 P = 0.005
P < 0.001 P = 0.017
P < 0.001 P = 0.025
P < 0.001 P = 0.001
P = 0.009 P = 0.083
P = 0.081 P = 0.70
TOPCAT Unpublished Data

MYTH #5
There is no Evidenced Based Treatment for HFpEF

THIS ONE IS TRUE!
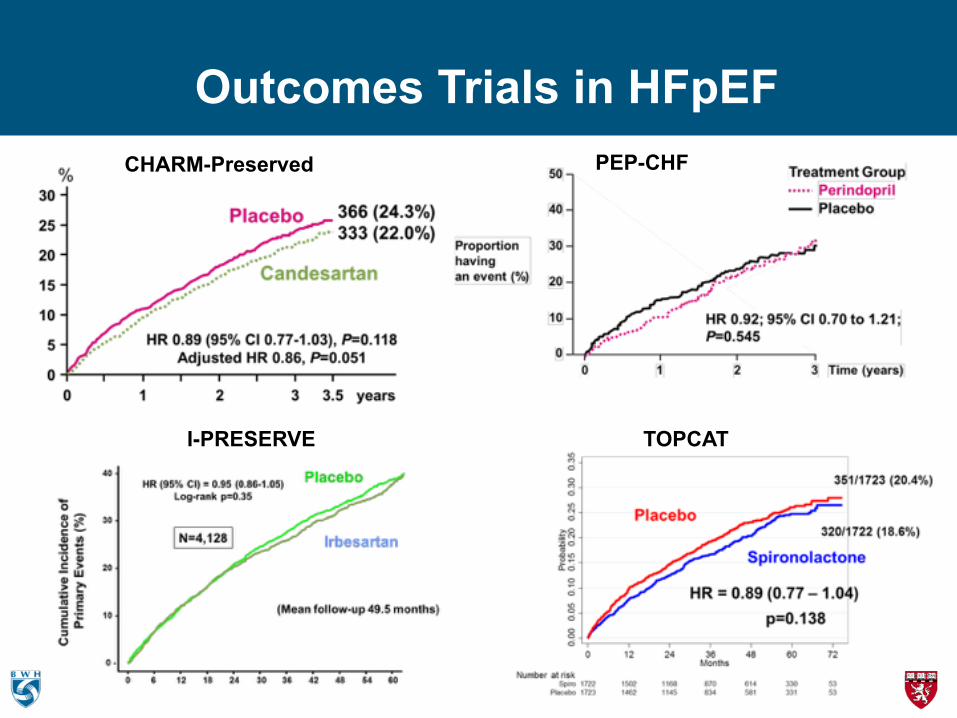
Outcomes Trials in HFpEFCHARM-Preserved PEP-CHF
I-PRESERVE TOPCAT

Spironolactone
Placebo
HR = 0.89 (0.77 – 1.04) p=0.138
351/1723 (20.4%)
320/1722 (18.6%)
TOPCAT: 1°Outcome (CV Death, HF Hosp, or Resuscitated Cardiac Arrest)
Pfeffer et al. NEJM 2014;370(15):1383-92
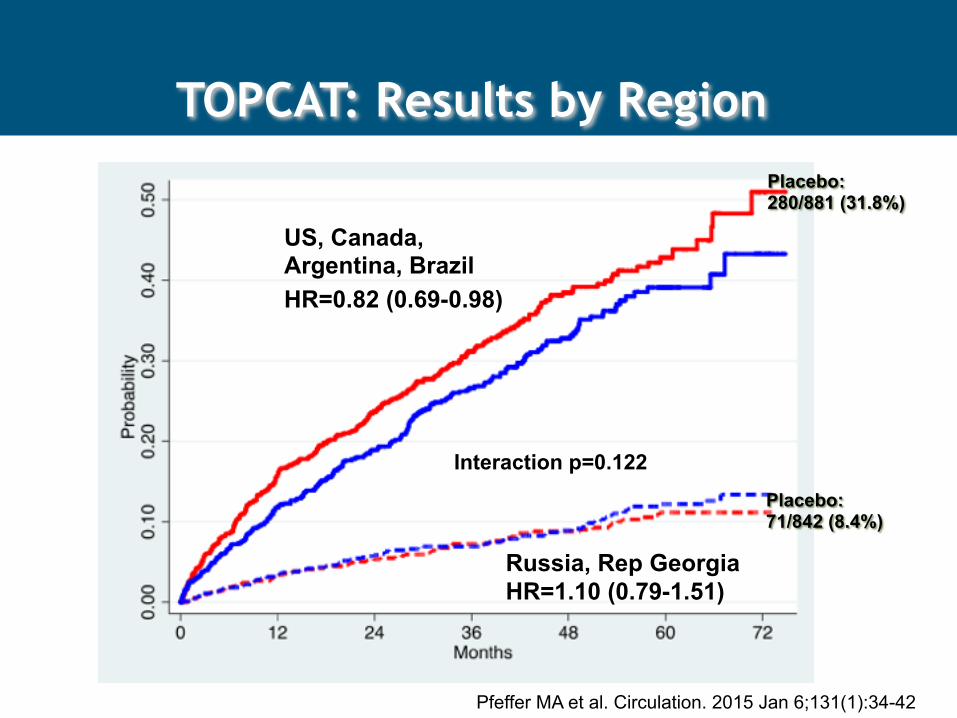
HR=0.82 (0.69-0.98)
HR=1.10 (0.79-1.51)
Interaction p=0.122
US, Canada, Argentina, Brazil
Russia, Rep Georgia
Placebo: 280/881 (31.8%)
Placebo: 71/842 (8.4%)
TOPCAT: Results by Region
Pfeffer MA et al. Circulation. 2015 Jan 6;131(1):34-42

TOPCAT: Benefit of Spironolactone Diminishes with Increasing Ejection Fraction
Solomon SD et al. Eur Heart J. 2015
Primary Outcome HF Hospitalization
2012 ESC Guidelines for Heart Failure Treatment
• No treatment has yet been shown, convincingly, to reduce morbidity and mortality in patients with HF-PEF.
• Diuretics are used to control sodium and water retention and relieve breathlessness and oedema as in HF-REF.
• Adequate treatment of hypertension and myocardial ischaemia is also considered to be important, as is control of the ventricular rate in patients with AF (see Section

Current Treatment of HFpEF
•Symptomatic Treatment with Diuretics
• Treatment of Hypertension
•Rate control in Atrial Fibrillation (? Maintain SR)
• Treat Ischemia
• ? Spironolactone

Soluble Guanylate Cyclase stimulator Heart Failure Studies: The SOCRATES Program
SOCRATES-REDUCED SOCRATES-PRESERVED
Design
2 Phase II, randomized, parallel-group, placebo-controlled, double-blind,
dose finding phase IIb studies of 4 dose regimens of the oral sGC stimulator vericiguat over 12 weeks
Inclusion Criteria
Worsening chronic heart failure requiring hospitalization (or IV diuretic for HF) with initiation after clinical stabilization
LVEF <45% LVEF ≥45% Left atrial (LA) enlargement
Primary Outcome
NT-proBNP at 12 weeks
NT-proBNP / LA vol. at 12 weeks (split α: each p<0.025)
Enrollment 410 patients in 5 arms 470 patients in 5 arms
Study status FPFV Nov 29, 2013 FPFV Nov 6, 2013
CT.gov ID NCT01951625 NCT01951638

SOCRATES-Preserved: Primary ResultsNo reduction in log-NT-proBNP or in LAV at week 12
compared with placebo
Data are mean ± standard error for the per-protocol analysis sets
Placebo 1.25 mg 2.5 mg 2.5 to 5 mg 2.5 to 10 mg Pooled dose groups
0.20
0.10
0.00
–0.10
–0.20
Cha
nge
in le
ft at
rial v
olum
e (m
L) 2
0
–2
–4
–6
Placebo 1.25 mg
2.5 mg
2.5 to 5 mg
2.5 to 10 mg
Pooled2.5/5/10
mg
Placebo 1.25 mg
2.5 mg
2.5 to 5 mg
2.5 to 10 mg
Pooled2.5/5/10
mg

NEAT-HFpEF: No Difference in Primary or Secondary Endpoints
(including 6 min walk, QOL, NT-proBNP)
Isosorbide Mononitrate with dose up-titration (30 to 120 mg/day over 4 weeks) vs. placebo in crossover design

AT1 receptor
Angiotensinogen (liver secretion)
Angiotensin I
Angiotensin II
NH
N
NN
N
O
OH
O
Valsartan
OH
ONH
OOH
O
Renin Angiotensin System
Vasoactive Peptide System
Vasodilation ! blood pressure ! sympathetic tone !aldosterone levels ! fibrosis ! hypertrophy Natriuresis/Diuresis
Inactive fragments
XNeprilysin
Vasoconstriction " blood pressure " sympathetic tone " aldosterone " fibrosis " hypertrophy
X
Heart Failure
LCZ696pro-BNP
NT-pro BNP
ANP BNP CNP
Adrenomedullin Bradykinin Substance P (angiotensin II)
Sacubitril (AHU377)↓
LBQ657
LCZ696 is a novel crystalline complex
consisting of the molecular moieties of valsartan and sacubitril in an equimolar
ratio
LCZ696 – A first-in-class Angiotensin Receptor Neprilysin Inhibitor – Simultaneously Inhibits NEP and the RAS

PARAMOUNT: Study Design
Primary objective NT pro-BNP reduction from baseline at 12 weeks
Secondary objectives
▪ Echocardiographic measures of diastolic function, left atrial size, LV size and function, PASP ▪ HF symptoms, Clinical composite assessment and Quality of life (KCCQ) ▪ Safety and tolerability
LCZ696 100 mg BID
LCZ696 50 mg BID
Valsartan 40 mg BID
1 week 10 weeks2 weeks
Placebo run-in
Discontinue ACEI or ARB therapy one day prior to randomization
LCZ696 200 mg BID
Valsartan 80 mg BID Valsartan 160 mg BID
1 week
Prior ACEi/ARB use discontinued
6 month extension
Baseline randomization visit and visit at end of 12 weeks of core study
Week Visit
-21
0 2
213 4
127
4 865 8 9 10 11
18 24 30 36
Clinicaltrials.gov NCT00887588
301 patients randomized
Solomon et al. ESC Hotline 2012 Lancet 2012

PARAMOUNT: Significant Improvement in Several Domains
Weeks Post Randomization
LCZ696
Valsartan
0 5 10 200
300
400
500
600
700
800
900
1000
NTp
roB
NP
(pg/
ml)
LCZ696/Valsartan: 0.77 (0.64, 0.92) P = 0.005
p = 0.063
12
783 (670,914)
862 (733,1012) 835 (710, 981)
605 (512, 714)
Left Atrial Volume
12 Weeks 36 Weeks
-6 -5 -4 -3 -2 -1 0 1 2
Cha
nge
in L
eft A
trial
Vol
ume
(ml)
Valsartan LCZ696
P = 0.18 P = 0.003
Worsened Unchanged Improved
LCZ696 Valsartan LCZ696 Valsartan 0 10 20 30 40 50 60 70 80 90
100 110
Per
cent
of P
atie
nts
Week 12 Week 36
P = 0.11 P = 0.05
Improvement in NT-proBNP Improvement in Left Atrial Size
Improvement in NYHA Class
Solomon et al. Lancet 2012

Target patient population: ∼4,600 patients with symptomatic HF (NYHA Class II–IV) and LVEF ≥45%
up to 2 weeks ~240 weeks
Valsartan 160 mg BID
LCZ696 200 mg BIDLCZ696 100 mg BID
On top of optimal background medications for co-morbidities (excluding ACEIs and ARBs)
Primary outcome: CV death and total (first and recurrent) HF hospitalizations (anticipated ~1,721 primary events)
Valsartan 80 mg BID*Screening
3–8 weeks
Active run-in period
Double-blind treatment periodRandomization 1:1
Steering Cmt: S. Solomon, co-Chair, J. McMurray, Co-Chair, I. Anand, F. Zannad, A. Maggioni, M. Packer, M. Zile, B. Pieske, J. Rouleau, M. Redfield, C. Lam, D. Van Veldhuisen, F. Martinez, J. Ge, H. Krum, M. Pfeffer

SPRINT: BP Lowering Reduces Adverse Outcomes
HF Hospitalization Reduced 38%
SPRINT Investigators. N Engl J Med 2015

Heart Failure Hospitalizations Reduced Substantial with the SGLT-2 Inhibitor Empaglifozin
Fitchett et al. Eur Heart J 2016
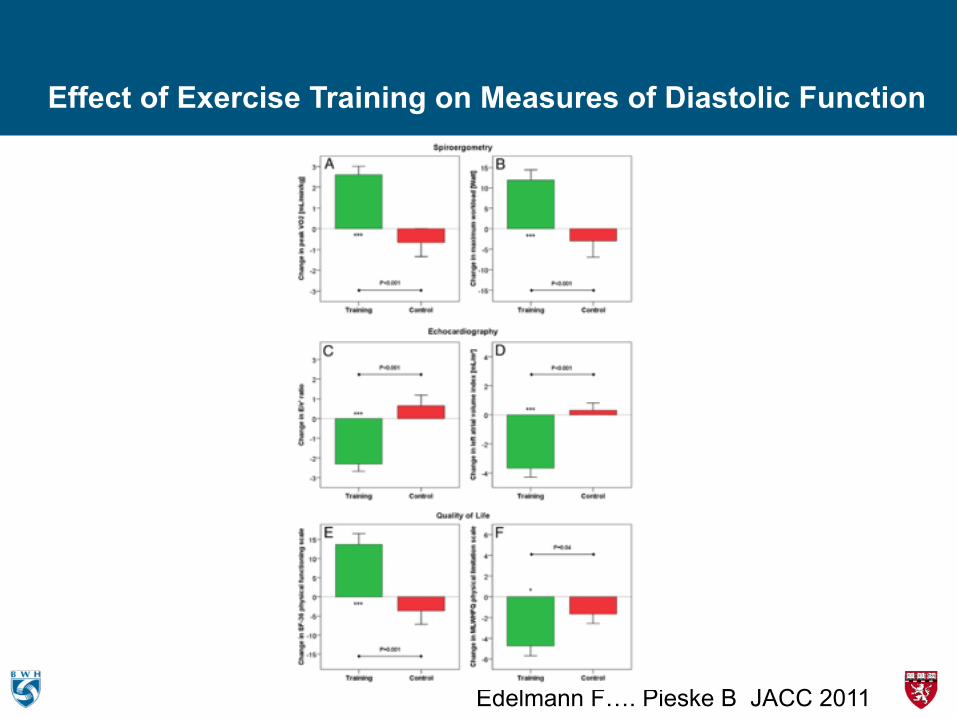
Effect of Exercise Training on Measures of Diastolic Function
Edelmann F…. Pieske B JACC 2011

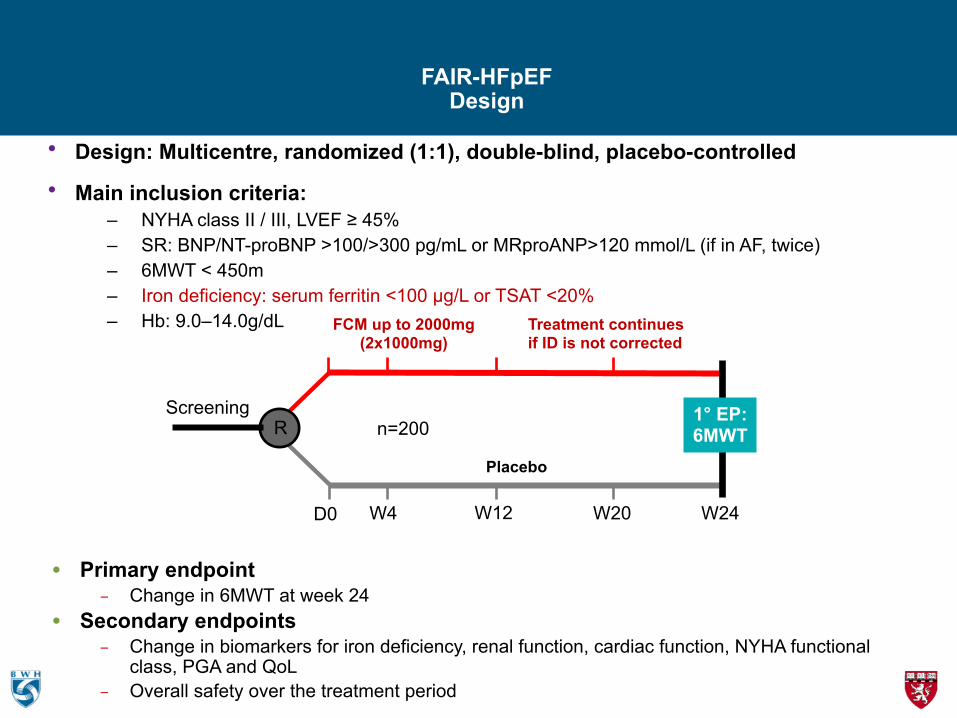
• Primary endpoint – Change in 6MWT at week 24
• Secondary endpoints – Change in biomarkers for iron deficiency, renal function, cardiac function, NYHA functional
class, PGA and QoL – Overall safety over the treatment period
FAIR-HFpEFDesign
• Design: Multicentre, randomized (1:1), double-blind, placebo-controlled • Main inclusion criteria:
– NYHA class II / III, LVEF ≥ 45% – SR: BNP/NT-proBNP >100/>300 pg/mL or MRproANP>120 mmol/L (if in AF, twice) – 6MWT < 450m – Iron deficiency: serum ferritin <100 µg/L or TSAT <20% – Hb: 9.0–14.0g/dL
Placebo
n=200Screening
R
D0
1° EP: 6MWT
W4 W12 W20 W24
FCM up to 2000mg (2x1000mg)
Treatment continues if ID is not corrected

Inter-Atrial Shunt Device - Concept
• Abnormal LV relaxation results in elevated Left Atrial Pressure (LAP) and pulmonary edema
• Transcatheter implant to create a small1 permanent interatrial shunt
• Shunt allows blood to move from the higher pressure LA to the lower pressure more compliant right side, reducing LAP without compromising LV cardiac output
1 Qp:Qs ratio (Pulmonary to Systemic flow ratio): 1.2-1.3
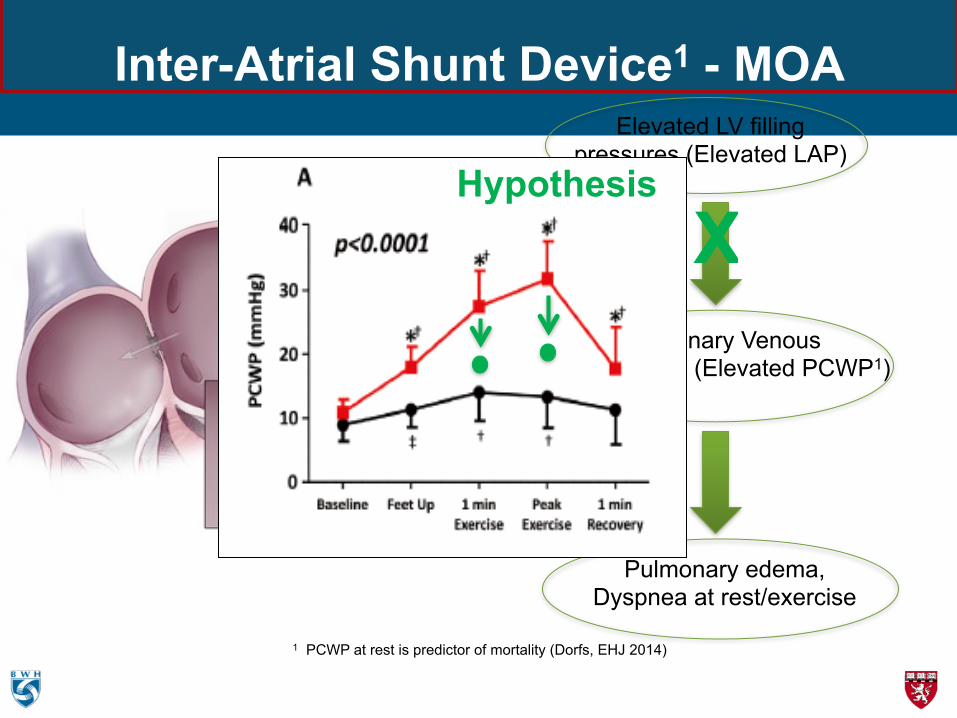
Inter-Atrial Shunt Device1 - MOA
1 PCWP at rest is predictor of mortality (Dorfs, EHJ 2014)
Elevated LV filling pressures (Elevated LAP)
Pulmonary Venous hypertension (Elevated PCWP1)
Pulmonary edema, Dyspnea at rest/exercise
XHypothesis

41
6 months Effectiveness
endpoints
Hasenfuβ, et al The Lancet Vol 387 March 26, 2016

42
6 months Efficacy Endpoints
Hasenfuβ, et al The Lancet Vol 387 March 26, 2016


Conclusions• HFpEF is alive, and not well.
• It is a heterogeneous disorder, associated with comborbidities but accounts for half of heart failure
• The cardiac phenotype is broader than we previously thought
• Diastolic dysfunction CANNOT account for the disorder and abnormalities of systole are becoming more recognized
• There is no “evidenced-based” therapy currently, but there are promising potential therapies being tested





















![WHITEPAPER Heart Failure with Preserved Ejection Fraction ... · dysfunction, chronic obstructive pulmonary disorder [COPD], obesity, and diabetes mellitus [DM]) implicated in tissue](https://img.pdfslide.net/doc/110x75/5ed59f691b7fdd786a1b5a58/whitepaper-heart-failure-with-preserved-ejection-fraction-dysfunction-chronic.jpg)







