Embed Size (px)
Citation preview

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
The New LTC Survey Process: First Quarter
Cynthia De Leon Thelen MSN, BSN, RN
LTC State Administrative Manager, BCHS
Kirsten Nunham RN
Long Term Care Surveyor, BCHS

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Describe the rationale for implementing changes to the Long Term Care Survey
• Discuss an overview of the new structure
– Appendix PP
• Identify communication and information timeframes
• Identify Resources
Objectives

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Surveyors and Providers = Shared Outcomes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Surveyors and Providers
• Our roles impact the lives of Michigan residents EVERY SINGLE DAY!
• Our profession is a choice that we EQUALLY care about!
• Our shared goals result in Positive Resident Centered Outcomes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Affordable Care Act (ACA) and the Improving Medicare Post-Acute Care Transformation (IMPACT) Act
– Quality Assurance and Performance Improvement (QAPI)
– 1150B requirements for reporting reasonable suspicion of a crime
– Increased Discharge Planning requirements
– Staff Training
Regulatory Reform

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Bringing survey process into the 21st century!
• Merge of Traditional (Paper) and Quality Indicator Survey (Computer Based)
• ONE Streamlined Process for ALL states
Rationale for the change

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Principals of Person-Centered Care
• Outcome-Oriented Care
• Quality of Care
• Quality of Life
• Consistent with current Health and Safety Knowledge
Rationale for the change: Focus

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
What has NOT changed for providers

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Implemented November 28th, 2017
• ALL states went live with new LTCSP to conduct Long Term Care Surveys
The New Survey Process: Phase 2

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Collected Immediately by Survey Team
• Step 1: Census Number
• Step 2: Matrix for new admissions who reside in the facility
• https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/GuidanceforLawsAndRegulations/Downloads/Matrix-with-Instructions-Content-Unchanged.pdf
Facility Entrance: Communication Timeframes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Step 3: Alphabetical list of all residents
• Step 4: List of residents who smoke
Facility Entrance: Communication Timeframes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Most Notable:
• No formal Initial Tour with facility staff
• Surveyors conduct tour independently
• Facility staff are no longer pulled for tour
• More time spent in conversations with residents
Summary: What HAS changed for providers

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Collected Within One Hour of entrance by survey team
• Schedule of meal times, locations of dining rooms, copies of all current menus including therapeutic menus that will be served for the duration of the survey and the policy for food brought in from visitors.
• Schedule of Medication Administration times.
• Number and location of medication storage rooms and medication carts.
• The actual working schedules for licensed and registered nursing staff for the survey time period.
• List of key personnel, location, and phone numbers. Note contract staff (e.g., rehab services).
• Paid feeding assistants
Facility Entrance: Communication Timeframes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Collected within 4 hours of entrance
• Complete Matrix for all other residents
• Provide each surveyor with access to ALL resident electronic health records
• Do not exclude any information that should be part of the residents’ medical record
Facility Entrance: Communication Timeframes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• 70% of the total sample is MDS pre-selected residents chosen offsite
• 30% of the total sample is determined onsite based on observations, interviews and limited record review
Resident Sample Selection

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Total sample size is about 20% of facility census
• Resident sample may be greater due to Complaints
• Resident sample may be greater due to Facility Reported Incidents
Recertification Survey Sample Size
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Appendix PP
– Reorganized and Updated
– New F Tags
– F- tag renumbering
• First Quarter Findings
Overview of the New Structure


C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
New Resident Rights F-Tag Numbering:
• F551 Resident Representative
• F553 Participate in Planning Care
• F555 Choice of Attending Physician
• F563 Visitation
• F564 Visitation Rights
• F578 Right to Request/Refuse Treatment/ Advance Directive
• F585 Grievances
• F586 External Entities
§ 483.10 Resident Rights

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• F551 - Resident Representatives
– Previously F152
– Resident representative acts within their legal responsibility
• F553 – Participation in Care Planning
– Previously F154/F280
– Resident has the right to participate in care planning process
– Facility upholds rights
§ 483.10 Resident Rights

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• F555 – Choice of Attending Physician
– Previously F163
– Physician must be licensed to practice
• F463/F564 – Visitation
– Previously F172
– Resident’s right to visitors
– Restriction for clinical or safety reasons
– Informing of visitation rights
– Equal visitation privileges
§ 483.10 Resident Rights

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• F586 – External Entities
– Previously F168
– Communication with Federal, State, or local officials must be
allowed
§ 483.10 Resident Rights

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• F578 – Right to Request/Refuse Treatment/Advance Directive
– Previously F155
– Facility’s responsibility to assist residents in establishing advance
directives
• F585 Grievances
– Previously F165
– Grievance official responsibilities
– Facility’s responsibility to inform residents of how to file a grievance,
and to maintain records
– Grievance policy
§ 483.10 Resident Rights

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Stand alone MDS Focus Survey is gone
• MDS is now incorporated into every survey
• The new resident assessment task reviews and investigates discrepancies identified for residents’ MDS assessments
Minimum Data Set (MDS)

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
MDS Clinical Indicators
• Alzheimer’s or Dementia
• Anticoagulant with Internal Bleeding
• Anticoagulant without Internal Bleeding
• Bowel and Bladder
• Catheter with UTI
• Catheter without UTI
• Constant Pain
• Decline in ADL’s
• Dehydration
• Dialysis
• Dehydration
• Dialysis
• Falls with Major Injury
• Feeding Tube/NO Dehydration
• Feeding Tube with Dehydration
• Four (4) or More Re-hospitalizations
• Frequent Pain
• Hospice
• Insulin

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
MDS Clinical Indicators
• One (1) Re-hospitalization
• Preadmission Screening and Resident Review (PASARR)
• Major Infections
• One (1) Re-hospitalization
• Preadmission Screening and Resident Review (PASARR)
• Pressure Ulcers Facility Acquired
• Pressure Ulcers Worsening
• Restraints
• ROM Limitation/Not Receiving Therapy
• ROM Limitation/Receiving Therapy
• Tracheostomy
• Two (2) or Three (3) Re-Hospitalizations
• UTI
• Ventilator
• Wandering
• Weight Loss

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
– Facilities need to have some type of quality assurance process that ensures the accuracy of MDS data.
– Each Critical Element Pathways starts with:
“Is the MDS accurately coded?”
Key Point

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• CE Pathways are completed for EACH sampled resident
Key changes to the Survey Process

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• SNF Beneficiary Protection Notification Review
• Dining Observation
• Infection Prevention Control and Immunizations
• Kitchen Observation
• Medication Administration Observation
Critical Element Pathways

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Resident Council Interview
• Quality Assessment and Assurance (QAA) and Quality Assurance and Performance Improvement (QAPI) Plan Review
• Abuse
• Environmental Observations
Critical Element Pathways

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Sufficient and Competent Nurse Staffing Review
• Personal Funds Review
• Activities
• Activities of Daily Living (ADL)
• Behavioral and Emotional Status
Critical Element Pathways

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Urinary Catheter or Urinary Tract Infection
• Communication and Sensory Problems (Includes Hearing and Vision)
• Dental Status and Services
• Dialysis
• General (Quality of Care)
Critical Element Pathways

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Hospice and End of Life Care
• Death
• Nutrition
• Pain Recognition and Management
• Physical Restraints
• Pressure Ulcer/Injury
• Specialized Rehabilitative or Restorative Services
Critical Element Pathways

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Rehab & Restorative Services
• Respiratory Care
• Unnecessary Medications (Psychotropic Medications & Medication Regimen Review)
• Medication Storage and Labeling
• PASARR
• Hydration
• Tube Feeding Status
Critical Element Pathways

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Positioning, Mobility, ROM
• Hospitalization
• Bladder and Bowel Incontinence
• Accidents
• Neglect
• Resident Assessment
• Discharge
• Dementia Care
Critical Element Pathways

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Minimum Data Set
Critical Element
PathwaysCare Plans
Process Links: Positive Resident Outcomes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• CMS uses the terminology ‘locus of control’
• The care plan should show that the resident is making their own choices and that they have control over their daily lives.
• Focusing on person centered care plans
Care Plans

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
§ 483.21(a)(1)
Baseline Care Plan developed within 48 hours of resident
admission and contain the minimum healthcare information
necessary to care for resident, which includes:
• Initial goals
• Physician/Dietary orders
• Therapy services
• Social services
• Applicable PASRR recommendations
F655 Baseline Care Plan-New Requirement

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
§ 483.21(a)(2)
A Comprehensive Care Plan may be developed in place of
Baseline Care Plan, but must be developed within 48 hours of
admission and meet all requirements for the Comprehensive Care
Plan.
• Baseline care plan must include the resident goals for his/her care
• Enhanced involvement of the resident and/or representative
• Recognizing the residents rights related to care
F655 Baseline Care Plan

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Key Point
§ 483.21(a)(3)
A written summary of the baseline care plan must be
provided to the resident and their representative, if
applicable.

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
§ 483.21(b)(2)(i) (Formerly F280)
Comprehensive care plan must be developed within 7 days after
completion of the comprehensive assessment.
F657 Care Plan Timing and Revision
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
§ 483.21(b)(2)(ii) New Requirements for who must be on the interdisciplinary team:
• Attending physician
• A registered nurse with responsibility for the resident
• A nurse aide with responsibility for the resident - new
• A member of food/nutrition services - new
• The resident or, if applicable, their representative - new
• Other appropriate staff or professionals as determined by the resident or their
needs
New requirement to document an explanation in the medical record if attendance by the
resident or their representative is determined not practicable.
F657 Care Plan Timing and Revision

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
§ 483.21(b)(2)(iii)
New requirement: The comprehensive care plan must be
reviewed/revised after each RAI assessment.
F657 Care Plan Timing and Revision

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Care Plans should address what the resident is requesting to have done to help accomplish their goals, incorporating both personal and cultural preferences.
Key Point

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
What has changed for Surveyors

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• “User-friendly” software
• Surveyors becoming acclimated to the new LTCSP and use of the software
• How findings are documented= computerized
Computer Based Software

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Requests for electronic documents
• Software triggers potential citations
• Downtime procedures
• Basic Ergonomics
Computer Based Software
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Perceptions

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Provider resources are FREE and open to the PUBLIC
• Every facility has EQUAL access to CMS resources
• Centers for Medicare and Medicaid Services – https://www.cms.gov/Medicare/Provider-Enrollment-and-
Certification/GuidanceforLawsAndRegulations/Nursing-Homes.html
Reality

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Long Term Care Survey Process (LTCSP) Review Course
• Located on the Integrated Surveyor Training Website (ISTW)
• https://surveyortraining.cms.hhs.gov/index.aspx
Provider Resources

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Click on I am a provider
• Click on Course Catalog at the top of the page
• Type in Long Term Care Survey Process Review
• Click on Title
• Click Launch the course
Accessing LTCSP Review Course

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• LTCSP Procedure Guide
• List of Revised F-Tags/Substandard Quality of Care (SQC) F tags
• Appendix PP- Guidance to Surveyors for LTC facilities
• Appendix Q-Guidelines for Determining Immediate Jeopardy
Provider Resources

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Chapter 7 Survey and Enforcement Process for Skilled Nursing Facilities of the State Operations Manual
• Psychosocial Outcome Severity Guide
• Principals of Documentation
Provider Resources

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Long Term Care Survey Process Review Resource Documents List:https://surveyortraining.cms.hhs.gov/data/139/cf81cb17-47bf-e711-9524-0e63451df8f4/assets/Resources.pdf
Nursing Homes page at CMS.gov :https://www.cms.gov/Medicare/ProviderEnrollment-and-Certification/GuidanceforLawsAndRegulations/Nursing-Homes.html
Resource List
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Integrated Surveyor Training Website:https://surveyortraining.cms.hhs.gov/pubs/providertraining.aspx
Resident Interview Care Areas and Probes
Resident Observations Care Areas and Probes
Resident Record Review Care Areas and Probes
Representative Interview Care Areas and Probes
Resource List

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Frequently Asked Questions Related to Long Term Care Regulations, Survey Process, and Training:
• https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/GuidanceforLawsAndRegulations/Downloads/LTC-Survey-FAQs.pdf
• Updated 2/6/2018
Questions
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Appendix PP State Operations Manual (Revised 11/22/2017) [PDF, 3MB]
• List of Revised FTags [Effective November 28, 2017] [PDF, 152KB]
• S&C Memo: Revision to State Operations Manual Appendix PP for Phase 2 (Includes Training Information and Related Issues) [PDF, 121KB]
• F-Tag Crosswalk [XLSX, 495KB]
• Training for Phase 1 Implementation of New Nursing Home Regulations [PDF, 108KB]
Nursing Homes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• New Long-term Care Survey Process – Slide Deck and Speaker Notes [PPTX, 8MB]
• Entrance Conference Form Beneficiary Notice Worksheet (Updated 12/06/2017) [ZIP, 164KB]
• Entrance Conference Form Beneficiary Notice Worksheet (Updated 12/06/2017) [ZIP, 164KB]
• LTC Survey Pathways - Updated 12/13/2017 [ZIP, 2MB]
Nursing Homes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• LTCSP Procedure Guide [PDF, 1MB]
• LTCSP Initial Pool Care Areas - Updated 11/17/2017 [ZIP, 1MB]
• Survey Resources - Updated 01/18/2018 [ZIP, 10MB]
• Matrix with Instructions - Content Unchanged [PDF, 299KB]
Nursing Homes

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• CMS is the Authoritative Resource for the New Long Term Care Survey Process for Federally Certified Facilities
Summary Key Point

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
The New Emergency Preparedness Survey: First Quarter
Laura Remus, BS, REHS
Environmental Health and Safety Section Manager, BCHS
Gerald Rodabaugh, Fire Safety Supervisor, BCHS

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• List the required components of an Emergency Preparedness Plan
• Identify areas for improving a facility’s emergency preparedness survey
• Identify examples of correct and incorrect emergency preparedness plans
Objectives
C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
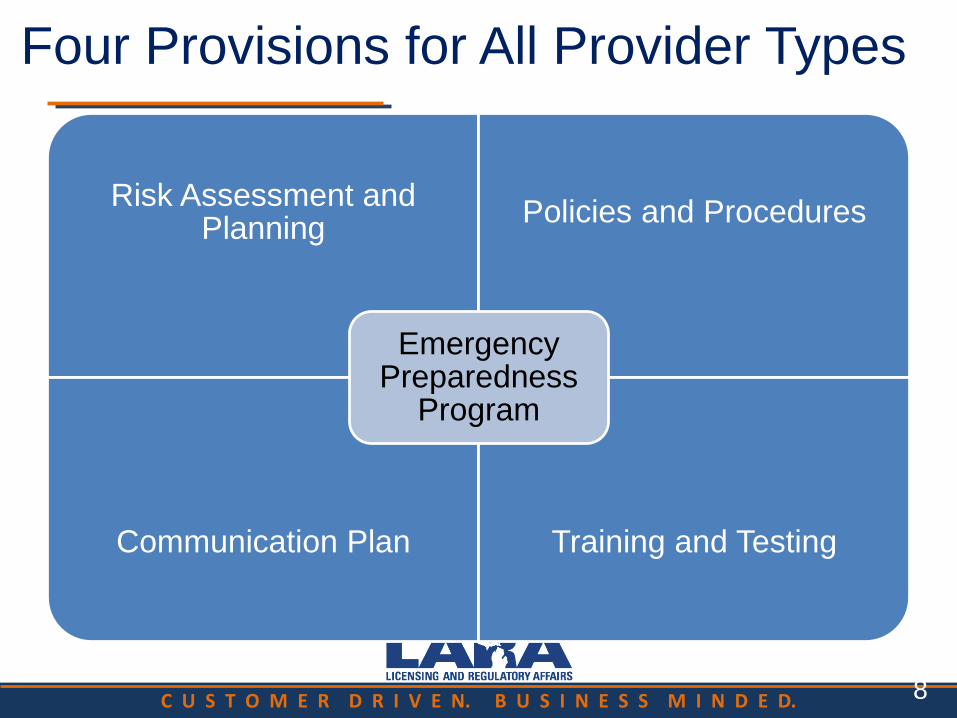
Four Provisions for All Provider Types
Risk Assessment and Planning
Policies and Procedures
Communication Plan Training and Testing
Emergency Preparedness
Program
8

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Risk Assessment and Planning
• Develop an emergency plan based on a risk
assessment.
• Perform risk assessment using an “all-hazards”
approach, focusing on capacities and capabilities.
• Update emergency plan at least annually.
9

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
All-Hazards Approach:
• An all-hazards approach is an integrated approach to
emergency preparedness planning that focuses on capacities
and capabilities that are critical to preparedness for a full
spectrum of emergencies or disasters, including internal
emergencies and a man-made emergency (or both) or natural
disaster. This approach is specific to the location of the
provider or supplier and considers the particular type of
hazards most likely to occur in their areas.
7

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
All-Hazards Approach:
• These may include, but are not limited to, care-
related emergencies, equipment and power
failures, interruptions in communications,
including cyber-attacks, loss of a portion or all
of a facility, and interruptions in the normal
supply of essentials such as water and food.

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Policies and Procedures
• Develop and implement policies and procedures
based on the emergency plan and risk
assessment.
• Policies and procedures must address a range of
issues including subsistence needs, evacuation
plans, procedures for sheltering in place, tracking
patients and staff during an emergency.
• Review and update policies and procedures at
least annually.
10

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Communication Plan
• Develop a communication plan that complies with
both Federal and State laws.
• Coordinate patient care within the facility, across
health care providers, and with state and local
public health departments and emergency
management systems.
• Review and update plan annually.
11

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Training and Testing Program
• Develop and maintain training and testing
programs, including initial training in policies and
procedures.
• Demonstrate knowledge of emergency procedures
and provide training at least annually.
• Conduct drills and exercises to test the emergency
plan.
12

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Training & Testing Program Definitions
• Facility-Based: When discussing the terms “all-hazards
approach” and facility-based risk assessments, we consider
the term “facility-based” to mean that the emergency
preparedness program is specific to the facility. Facility-based
includes, but is not limited to, hazards specific to a facility
based on the geographic location; Patient/Resident/Client
population; facility type and potential surrounding community
assets (i.e. rural area versus a large metropolitan area).
70

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• Full-Scale Exercise: A full scale exercise
is a multi-agency, multijurisdictional, multi-
discipline exercise involving functional (for
example, joint field office, emergency
operation centers, etc.) and ‘‘boots on the
ground’’ response (for example, firefighters
decontaminating mock victims).
Training & Testing Program Definitions

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Training & Testing Program Definitions
• Table-top Exercise (TTX): A table-top exercise is a group
discussion led by a facilitator, using narrated, clinically-
relevant emergency scenario, and a set of problem
statements, directed messages, or prepared questions
designed to challenge an emergency plan. It involves key
personnel discussing simulated scenarios, including
computer-simulated exercises, in an informal setting. TTXs
can be used to assess plans, policies, and procedures.
72

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Requirements Vary by Provider Type
• Long-term care facilities must share information
from the emergency plan with residents and family
members or representatives.
14

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Temperature Controls and Emergency and Standby
Power Systems
• Under the Policies and Procedures, Standard (b)
there are requirements for subsistence needs and
temperature controls.
• Additional requirements for long-term care facilities
are located within the Final Rule under Standard
(e) for Emergency Power and Stand-by Systems.
13

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Interpretive Guidelines
• Appendix Z (remember:
Z= Zombie Apocalypse)
• Are formatted into one
new Appendix within the
State Operations Manual
(SOM) applicable to all 17
provider/supplier types
17

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
• The plan has not been tested (Tag E-39)
• Emergency food within the facility does not match with the plan (Tag E-15)
• Some other policy/procedure cites
• Make the plan specific to your needs and your facility
• Organize the plan so that staff can use it when in an actual emergency
What are we seeing on surveys so far?

C U S T O M E R D R I V E N. B U S I N E S S M I N D E D.
Questions?