Embed Size (px)
Citation preview

The NICE ACS Guidelines: variation on an ESC theme? The NICE ACS Guidelines:
variation on an ESC theme?
Rob Henderson
Consultant Cardiologist
Trent Cardiac Centre
Nottingham University Hospitals
Rob Henderson
Consultant Cardiologist
Trent Cardiac Centre
Nottingham University Hospitals

MY CONFLICTS OF INTEREST ARE
Member, NICE ACS Guideline Development Group
Advisory Boards and Speaker Honoraria(Pfizer, Lilly UK, Daiichi-Sankyo UK Ltd, Boston Scientific, Cordis UK, Abbott Vascular)
MY CONFLICTS OF INTEREST ARE
Member, NICE ACS Guideline Development Group
Advisory Boards and Speaker Honoraria(Pfizer, Lilly UK, Daiichi-Sankyo UK Ltd, Boston Scientific, Cordis UK, Abbott Vascular)

UA/NSTEMI Guidance fromESC and NICE
UA/NSTEMI Guidance fromESC and NICE
ESC Guidance NICE Guidance
Publication June 2007 Pre-publication draftPublication March 2010
DevelopmentMultinational Taskforce of cardiologists
Multidisciplinary teamclinicians, information scientists, health economists, patient representatives
Perspective Clinical efficacyClinical EfficacyCost Efficacy Patient
Target Multinational, Europe NHS in England & Wales

NICE UA/NSTEMI GuidelineDevelopment Group 2008-2009
NICE UA/NSTEMI GuidelineDevelopment Group 2008-2009
John Camm, chairHuon Gray, clinical advisor, NCGCSotiris Antoniou, pharmacistLina Bakhshi, information scientistJenny Cadman, nurseEmily Crowe, research fellowMark de Belder, cardiologistJose Diaz, research fellowDavid H. Geldard, patient repRob Henderson, cardiologistMarjan Jahangiri, cardiac surgeonTaryn Krause, project managerKate Lovibond, health economistGavin Maxwell, patient repFrancis Morris, A&E physicianAlun Roebuck, nurse consultantNicola Sloan, research fellowClaire Turner, project managerRichard Underwood, cardiac imagingMark Whitbread, paramedic
John Camm, chairHuon Gray, clinical advisor, NCGCSotiris Antoniou, pharmacistLina Bakhshi, information scientistJenny Cadman, nurseEmily Crowe, research fellowMark de Belder, cardiologistJose Diaz, research fellowDavid H. Geldard, patient repRob Henderson, cardiologistMarjan Jahangiri, cardiac surgeonTaryn Krause, project managerKate Lovibond, health economistGavin Maxwell, patient repFrancis Morris, A&E physicianAlun Roebuck, nurse consultantNicola Sloan, research fellowClaire Turner, project managerRichard Underwood, cardiac imagingMark Whitbread, paramedic

NICE UA/NSTEMI GuidelineDevelopment Group 2008-2009
John Camm, chairHuon Gray, clinical advisor, NCGCSotiris Antoniou, pharmacistLina Bakhshi, information scientistJenny Cadman, nurseEmily Crowe, research fellowMark de Belder, cardiologistJose Diaz, research fellowDavid H. Geldard, patient repRob Henderson, cardiologistMarjan Jahangiri, cardiac surgeonTaryn Krause, project managerKate Lovibond, health economistGavin Maxwell, patient repFrancis Morris, A&E physicianAlun Roebuck, nurse consultantNicola Sloan, research fellowClaire Turner, project managerRichard Underwood, cardiac imagingMark Whitbread, paramedic
John Camm, chairHuon Gray, clinical advisor, NCGCSotiris Antoniou, pharmacistLina Bakhshi, information scientistJenny Cadman, nurseEmily Crowe, research fellowMark de Belder, cardiologistJose Diaz, research fellowDavid H. Geldard, patient repRob Henderson, cardiologistMarjan Jahangiri, cardiac surgeonTaryn Krause, project managerKate Lovibond, health economistGavin Maxwell, patient repFrancis Morris, A&E physicianAlun Roebuck, nurse consultantNicola Sloan, research fellowClaire Turner, project managerRichard Underwood, cardiac imagingMark Whitbread, paramedic
359 pages36 recommendations

NICE Guideline - Risk AssessmentNICE Guideline - Risk Assessment
R1 Formally assess individual risk of future adverse cardiovascular events using an established risk scoring system that predicts 6-month mortality (e.g. GRACE)
(Observational studies)
R1 Formally assess individual risk of future adverse cardiovascular events using an established risk scoring system that predicts 6-month mortality (e.g. GRACE)
(Observational studies)

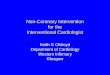
Troponin status and in-hospital mortalityas function of GRACE risk score
Troponin status and in-hospital mortalityas function of GRACE risk score
Steg et al, Am J Med 2009;122:107Steg et al, Am J Med 2009;122:107
GRACE risk score (Granger algorithm)GRACE risk score (Granger algorithm)
N=27406 non-ST-elevation ACSN=27406 non-ST-elevation ACS
Troponin positive (red bars)Troponin negative (yellow bars)In-hosp mortality (blue line)
Troponin positive (red bars)Troponin negative (yellow bars)In-hosp mortality (blue line)
00
500500
15001500
20002000
25002500
30003000
35003500
10001000
0%0%
10%10%
20%20%
30%30%
40%40%
<51<51 6666 8585 105105 125125 145145 165165 185185 205205 225225 >226>2265656 7676 9595 115115 135135 155155 175175 195195 215215
Num
ber
of p
atie
nts
Num
ber
of p
atie
nts
In-h
ospi
tal m
orta
lity
(%)
In-h
ospi
tal m
orta
lity
(%)

NICE Guideline - Risk CategoriesNICE Guideline - Risk Categories
Risk category
% of ACS population*
Guideline risk categories and predicted six-month mortality
1a 12.5% Lowest 1.5% or below
1b 12.5% Low >1.5% to 3.0%
2a 12.5% Intermediate >3.0% to 6.0%
2b 12.5% High >6.0% to 9.0%
3 & 4 50.0% Highest Over 9%
*estimated from MINAP registry
R5 Use predicted 6-month mortality to categorise the risk of future adverse cardiovascular events:
R5 Use predicted 6-month mortality to categorise the risk of future adverse cardiovascular events:

NICE Guideline - ClopidogrelNICE Guideline - Clopidogrel
R9 Offer 300mg loading dose of clopidogrel in addition to aspirin to patients with no contra-indications and predicted 6-month mortality >1.5%
(CURE, CREDO, Cuisset, PRACTICAL)
R9 Offer 300mg loading dose of clopidogrel in addition to aspirin to patients with no contra-indications and predicted 6-month mortality >1.5%
(CURE, CREDO, Cuisset, PRACTICAL)
Emerging evidence for use of 600mg in PCI patientsIn CURRENT double dose prevented 6 MI’s and 7 stent thromboses with excess of 3 extra major bleeds per 1000 PCI patients

NICE Guideline - FondaparinuxNICE Guideline - Fondaparinux
R17 Offer fondaparinux to patients who do not have a high bleeding risk, unless coronary angiography is planned within 24 hours of admission
(OASIS-5, cost effective with high certainty)
R17 Offer fondaparinux to patients who do not have a high bleeding risk, unless coronary angiography is planned within 24 hours of admission
(OASIS-5, cost effective with high certainty)

OASIS 5 - Fondaparinux vs Enoxaparin in Non-ST-elevation Acute Coronary Syndromes
OASIS 5 - Fondaparinux vs Enoxaparin in Non-ST-elevation Acute Coronary Syndromes
5.8%
2.2%
7.3%
0.9%
5.7%
4.1%
9.0%
0.4%
0%
2%
4%
6%
8%
10%
Death/MI/refractoryischaemia
Major bleeding Composite: netbenefit
Catheter relatedthrombus
Fondarinux (n=10 057)
Enoxaparin (n=10 021)
OASIS 5 investigators NEJM 2006;354:1464OASIS 5 investigators NEJM 2006;354:1464Fondarinux 2.5mg sc odEnoxaparin 1mg/kg sc bdFondarinux 2.5mg sc odEnoxaparin 1mg/kg sc bd
Non-inferiorityP=0.007
Non-inferiorityP=0.007 P<0.001P<0.001
P<0.001P<0.001
P<0. 001P<0. 001
Events at 9 days
UFH/LMWH but not Fonda inhibits contact activation pathway (FXII, XI)

Cumulative mortalityCumulative mortality
180180303000 6060 9090 150150120120
0.040.04
0.000.00
0.020.02
0.060.06
Fondarinux n=10,021Enoxaparin n=10,057Fondarinux n=10,021Enoxaparin n=10,057
OASIS 5 Investigators, NEJM 2006;354:1464OASIS 5 Investigators, NEJM 2006;354:1464
OASIS 5 - Fondaparinux vs Enoxaparin in Non-ST-elevation Acute Coronary Syndromes
OASIS 5 - Fondaparinux vs Enoxaparin in Non-ST-elevation Acute Coronary Syndromes
6.5%6.5%
5.8%5.8%
Hazard ratio 0.89 (95% CI 0.80–1.00) P=0.05
Hazard ratio 0.89 (95% CI 0.80–1.00) P=0.05C
umul
ativ
e m
orta
lity
Cum
ulat
ive
mor
talit
y

NICE Guideline - Glycoprotein Inhibitors
NICE Guideline - Glycoprotein Inhibitors
R14 Consider iv eptifibatide or tirofiban as part of the early management of patients with predicted 6-month mortality >3%, and who are scheduled to undergo angiography within 96 hours of hospital admission
R15 Consider abciximab as an adjunct to PCI for patients at intermediate or higher risk who are not already receiving a GPI or bivalirudin
(Meta-analyses: Boersma, Roffi. New RCTs: ISAR-REACT-2, ELISA-2, ACUITY-TIMING, Early-ACS, high uncertainty in cost effectiveness modeling)
R14 Consider iv eptifibatide or tirofiban as part of the early management of patients with predicted 6-month mortality >3%, and who are scheduled to undergo angiography within 96 hours of hospital admission
R15 Consider abciximab as an adjunct to PCI for patients at intermediate or higher risk who are not already receiving a GPI or bivalirudin
(Meta-analyses: Boersma, Roffi. New RCTs: ISAR-REACT-2, ELISA-2, ACUITY-TIMING, Early-ACS, high uncertainty in cost effectiveness modeling)

Upstream GPI in non-ST-elevation ACSMeta-analysis of ACUITY-TIMING & Early-ACS
Upstream GPI in non-ST-elevation ACSMeta-analysis of ACUITY-TIMING & Early-ACS
0 1 2Favours early GPI
Favours early GPI
Favours delayed GPI
Favours delayed GPI
Odds Ratio (95% CI)Odds Ratio (95% CI)Endpoint at 30 days
MI
Death
D/MI/Unplanned revasc
Unplanned revasc
Major bleed
Draft NICE guideline document Draft NICE guideline document
N=14009Thienopyridine use 64% in ACUITY, 75% in Early-ACS
Early GPI Delayed GPI
7.8% 8.8%
2.4% 2.2%
10.7% 11.8%
2.3% 2.8%
2.4% 1.8%

NICE Guideline - BivalirudinNICE Guideline - Bivalirudin
R22 Consider switching to bivalirudin, rather than adding a GPI to an alternative antithrombin, for patients: – with predicted 6-month mortality >3% and– are not already receiving a GPI or fondaparinux and – are scheduled to undergo angiography within 24 hrs
(ACUITY, REPLACE-2, cost effective with high uncertainty)
R22 Consider switching to bivalirudin, rather than adding a GPI to an alternative antithrombin, for patients: – with predicted 6-month mortality >3% and– are not already receiving a GPI or fondaparinux and – are scheduled to undergo angiography within 24 hrs
(ACUITY, REPLACE-2, cost effective with high uncertainty)

ACUITY – bivalirudin vs heparin & IIb/IIIa blocker in non-ST elevation ACS patients scheduled for invasive strategy
ACUITY – bivalirudin vs heparin & IIb/IIIa blocker in non-ST elevation ACS patients scheduled for invasive strategy
7.3%
5.7%
11.7%
7.7%
5.3%
11.8%
7.8%
3.0%
10.1%
0%
2%
4%
6%
8%
10%
12%
14%
MACE* Major bleed Net clinical outcome
UFH/Enox & GPIIbIIIa (n=4603)
Bivalirudin &GPIIbIIIa (n=4604)
Bivalirudin (n=4612)
Stone, NEJM 2006;355:2203Stone, NEJM 2006;355:2203
All patients scheduled for coronary arteriography/PCI <72hBivalirudin 0.1mk/kg bolus, 0.25mg/kg/hr infusion*Death, MI, revasc for ischaemia
All patients scheduled for coronary arteriography/PCI <72hBivalirudin 0.1mk/kg bolus, 0.25mg/kg/hr infusion*Death, MI, revasc for ischaemia
NSNS P<0.001P<0.001 P=0.015P=0.015
30 d outcomes

NICE Guideline - Invasive strategyNICE Guideline - Invasive strategy
R24 Offer coronary angiography (and follow-on PCI) within 96 hrs of admission to patients with predicted 6-month mortality >3.0% if they have no contraindications (active bleeding, comorbidity). Perform angiography as soon as possible for patients who are clinically unstable or at high ischaemic risk
R25 Offer coronary angiography to patients with low risk if ischaemia is subsequently experienced or demonstrated
(High Quality RCTs, meta-analyses)
R24 Offer coronary angiography (and follow-on PCI) within 96 hrs of admission to patients with predicted 6-month mortality >3.0% if they have no contraindications (active bleeding, comorbidity). Perform angiography as soon as possible for patients who are clinically unstable or at high ischaemic risk
R25 Offer coronary angiography to patients with low risk if ischaemia is subsequently experienced or demonstrated
(High Quality RCTs, meta-analyses)

ConclusionsConclusions
• NICE Guideline provides clinical guidance for
effective & cost-effective treatment of UA/NSTEMI
• Potentially important differences between ESC and
NICE Guidance
• NICE Guidance will change our approach to– risk stratification
– anticoagulation
– early invasive strategy
• Due for final publication March 2010
• NICE Guideline provides clinical guidance for
effective & cost-effective treatment of UA/NSTEMI
• Potentially important differences between ESC and
NICE Guidance
• NICE Guidance will change our approach to– risk stratification
– anticoagulation
– early invasive strategy
• Due for final publication March 2010