Embed Size (px)
Citation preview
Endocrine Diseases
Qiao Li, MD, PhD Dept of Pathology & Laboratory Medicine Faculty of Medicine University of Ottawa
[email protected] 613 562 5800 Ext. 8491
The Pathological Basis of Disease - Graduate Course CMM 5001
Q L
• Endocrine System • Adrenal Gland
– Anatomy Histology & Function – Steroid Hormones – Addison’s Disease – Cushing Syndrome – Clinical Case Presentation
Outline
Q L
• The Components • The Origin • The Microscopic Structure • Merocrine Secretion • Neuroendocrine System
Endocrine System
Q L
• Anatomy, Histology & Function • Steroid Hormones • Addison’s Disease • Cushing’s Syndrome • Clinical Case Presentation
Adrenal Gland
Q L
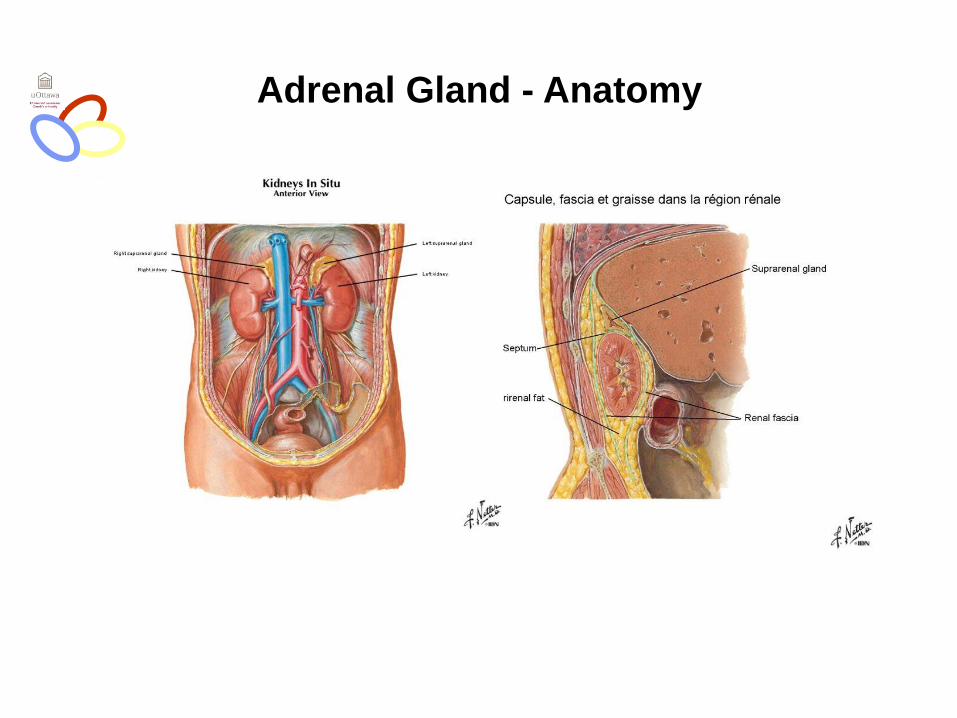
Adrenal Gland - Anatomy
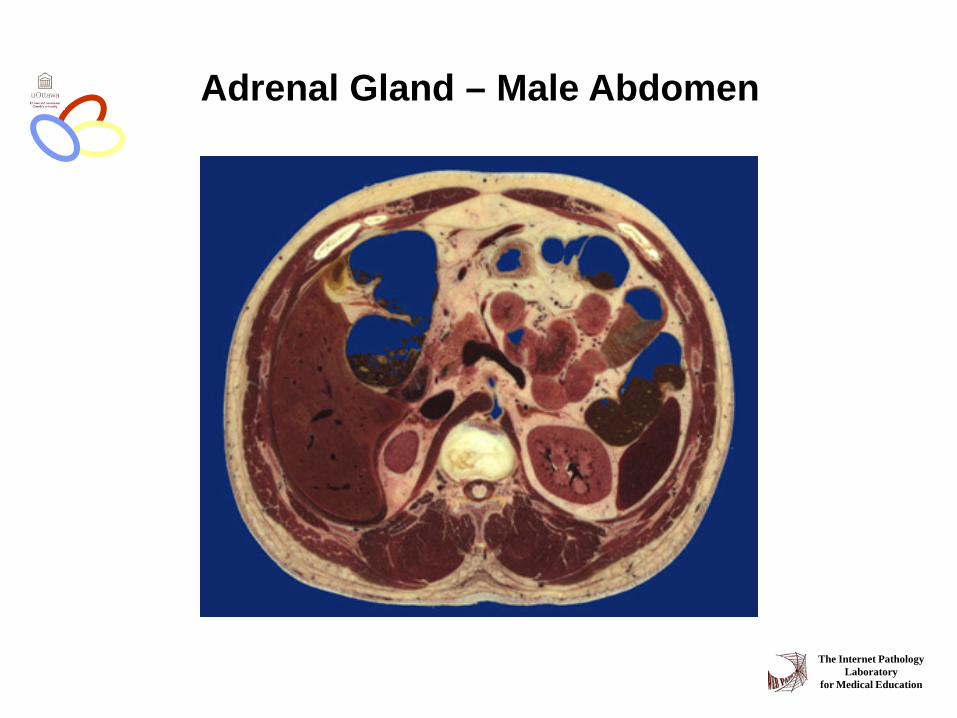
Adrenal Gland – Male Abdomen
The Internet Pathology Laboratory
for Medical Education

Adrenal Gland - CT

Adrenal Gland - MRI

Adrenal Gland – in situ
The Internet Pathology Laboratory
for Medical Education
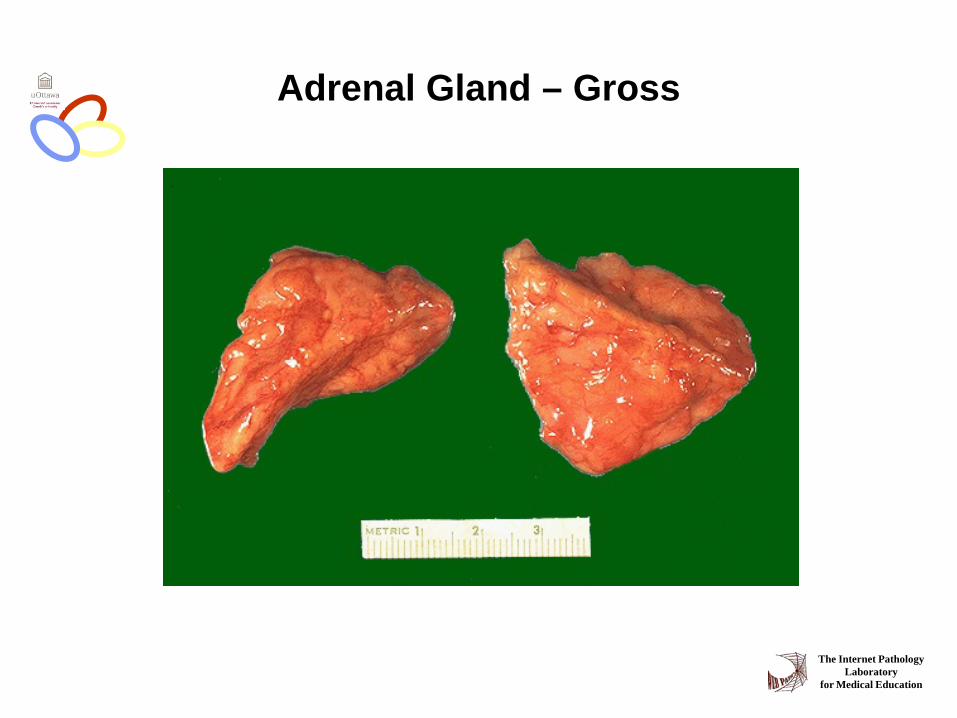
Adrenal Gland – Gross
The Internet Pathology Laboratory
for Medical Education

Adrenal Gland – Cut Surface
The Internet Pathology Laboratory
for Medical Education
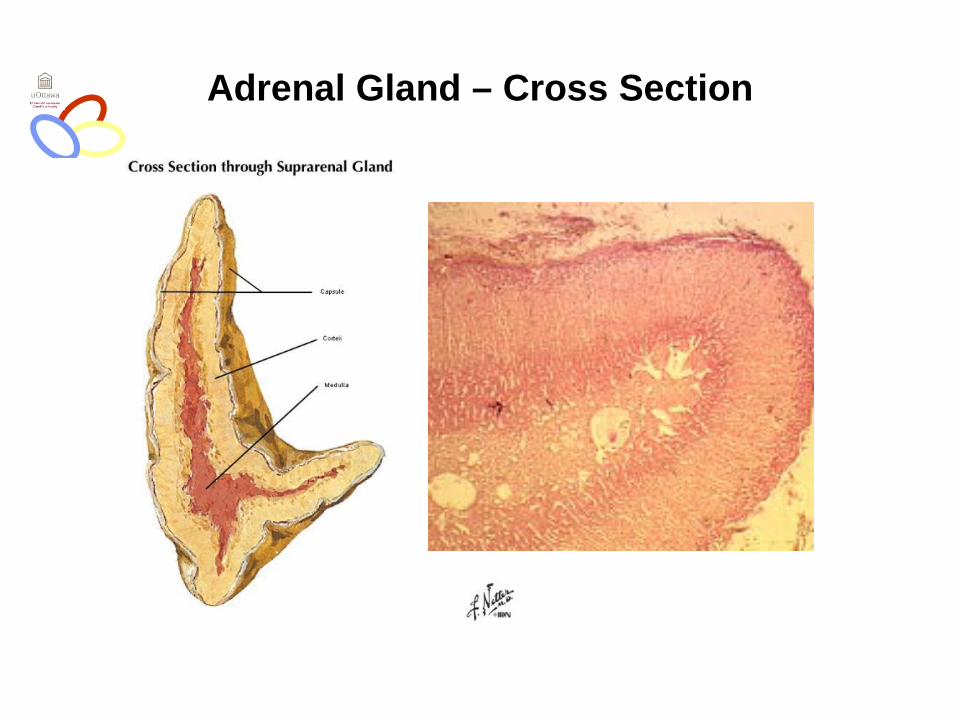
Adrenal Gland – Cross Section

Capsule
Periadrenal fat Zona glomerulosa
Zona fasciculata
Zona reticularis
Medulla
Adrenal Gland – Low Power
The Internet Pathology Laboratory
for Medical Education

Adrenal Gland – Low & High Power
Q L
Adrenal Gland
Q L
• Anatomy, Histology & Function • Steroid Hormones • Addison’s Disease • Cushing’s Syndrome • Clinical Case Presentation

Adrenal Cortex Steroids
glomerulosa Mineralocorticoids Aldosterone salt and water homeostasis
fasiculata Glucocorticoids Cortisol carbohydrate metabolism
reticularis Sex Steroids Androgens minimal effects
Q L
O
O
CH2OH
O
O
Zone Class Representative Physiologic Effects
CH2OH
O
O O
CH

Adrenal Steroidogenesis
Adrenal Gland - Milestones
1552: Bartholomaeus Eustachius - adrenal glands on copper plates 1936: Edward Kendall and Tadeus Reichstein - isolation and synthesis of cortisone 1949: Edward Kendall and Philip Showalter Hench
- effects of cortisone and ACTH on arthritis 1950: Kendall, Reichstein & Hench - Nobel Prize “for their discoveries relating
to the hormones of the adrenal cortex, their structure and biological effects"
Q L
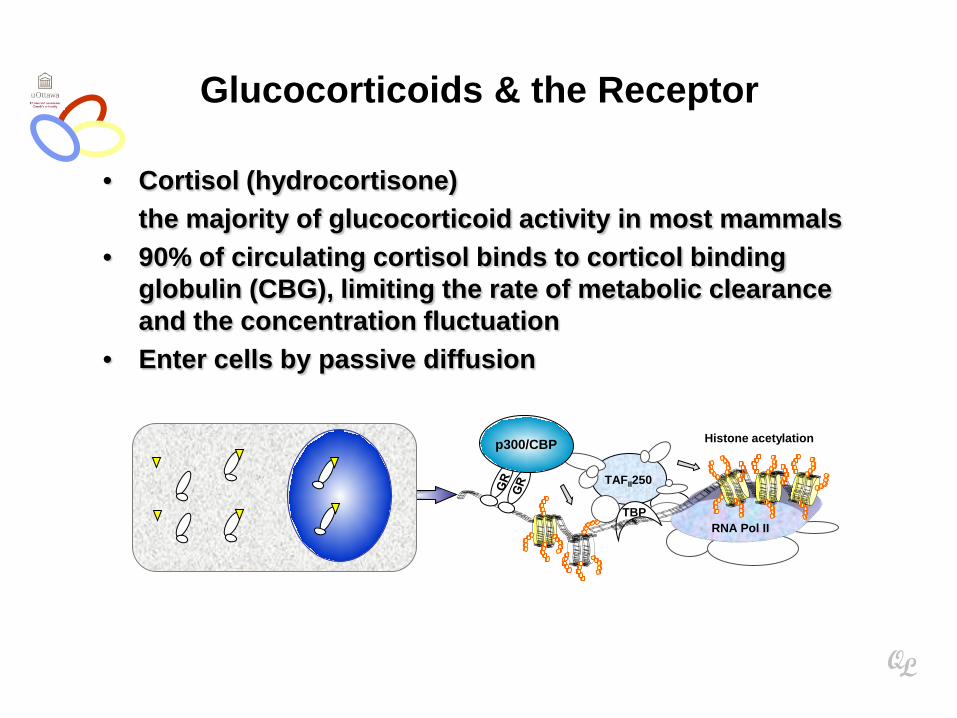
Glucocorticoids & the Receptor
• Cortisol (hydrocortisone) the majority of glucocorticoid activity in most mammals • 90% of circulating cortisol binds to corticol binding
globulin (CBG), limiting the rate of metabolic clearance and the concentration fluctuation
• Enter cells by passive diffusion
Histone acetylation
TAFII250
RNA Pol II
p300/CBP
TBP
Q L

Effects and Usage of Glucocorticoids
• Carbohydrate, proteins and fat metabolism increase gluconeogenesis muscle breakdown lipolysis
• Anti-inflammatory and immunosuppressive
• Medical Application: arthritis, dermatitis autoimmune diseases. fear phobic
Q L
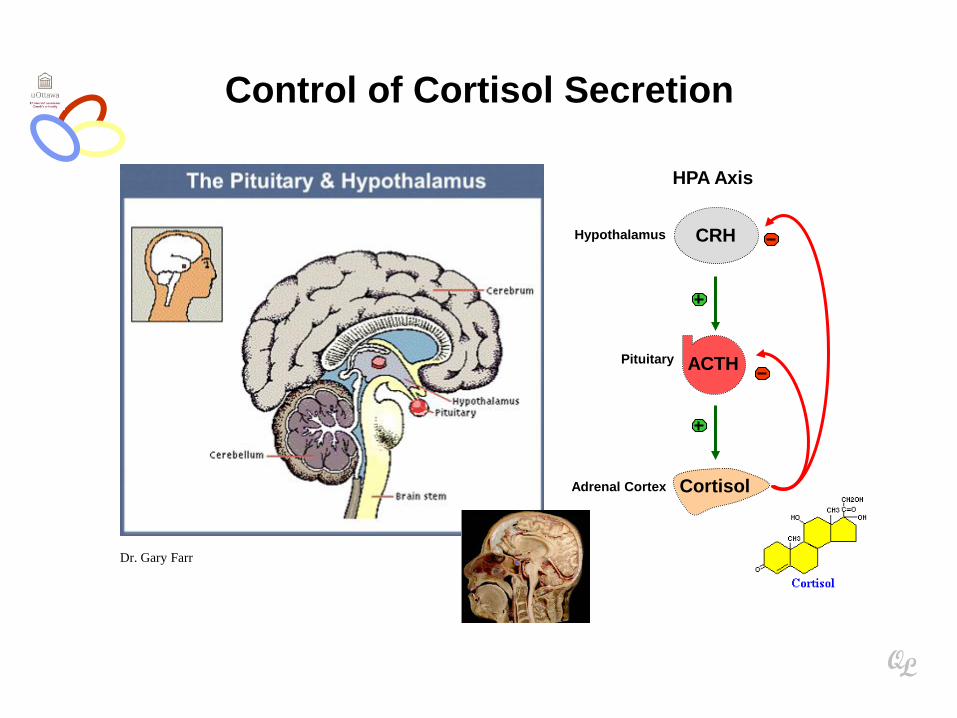
Control of Cortisol Secretion
Dr. Gary Farr
Q L
Hypothalamus
ACTH
CRH
Cortisol
Pituitary
Adrenal Cortex
HPA Axis
Adrenal Gland
Q L
• Anatomy, Histology & Function • Steroid Hormones • Addison’s Disease • Cushing’s Syndrome • Clinical Case Presentation
* General languor and debility * Remarkable feebleness of the heart's action * Peculiar change in the color of the skin
Chronic adrenocortical insufficiency progressive destruction of 90%of cortex
Addison’s Disease
Q L
Extreme weakness and fatigue Unintentional weight loss Loss of appetite Darkening of the skin Low blood pressure, dizziness or fainting Craving for salt Nausea, diarrhea, vomiting Irritability, depression
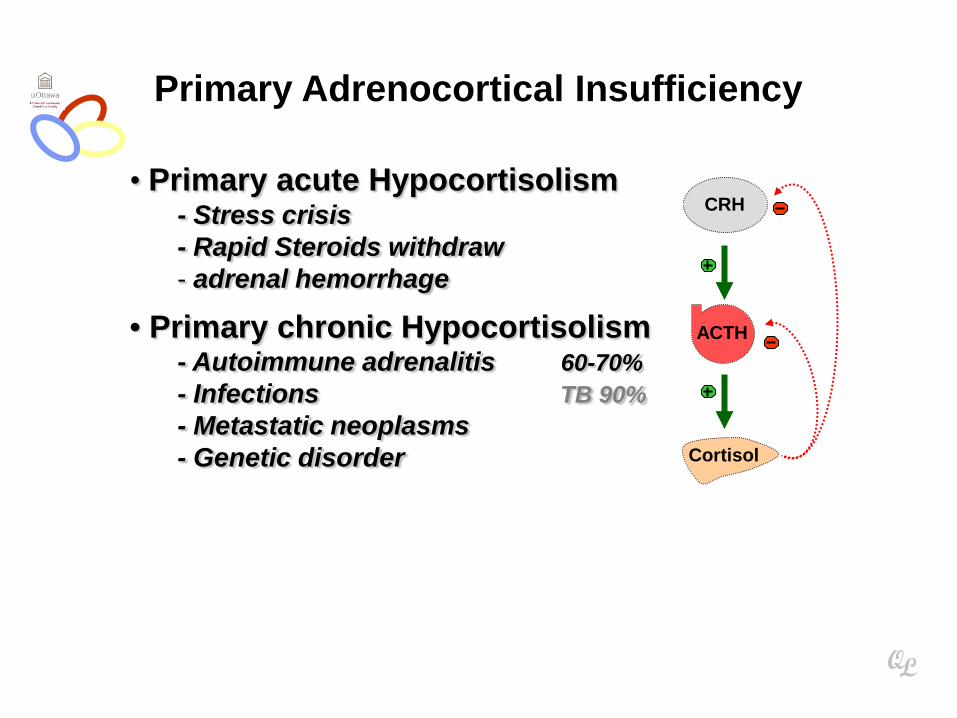
• Primary acute Hypocortisolism - Stress crisis - Rapid Steroids withdraw - adrenal hemorrhage
• Primary chronic Hypocortisolism - Autoimmune adrenalitis 60-70% - Infections TB 90% - Metastatic neoplasms - Genetic disorder
Primary Adrenocortical Insufficiency
Q L
ACTH
CRH
Cortisol
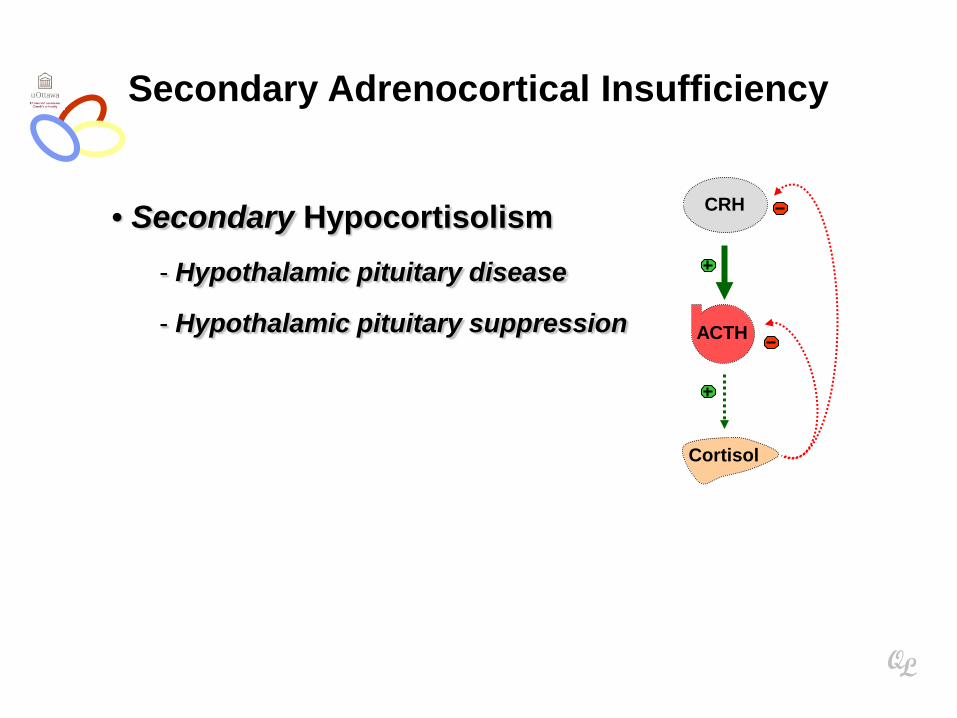
• Secondary Hypocortisolism - Hypothalamic pituitary disease
- Hypothalamic pituitary suppression
Secondary Adrenocortical Insufficiency
Q L
ACTH
CRH
Cortisol
Glucocorticoid replacement
Mineralocorticoid replacement
Prevent adrenal crisis
Medic Alert bracelet
Management
Q L
ACTH
CRH
Cortisol
For people with Addison’s Disease
* prior to 1930, 90% died within 5 years
* from late 1930, much better prognosis
* since late 1950, normal life span
Prognosis
Q L
• Anatomy, Histology & Function • Steroid Hormones • Addison’s Disease • Cushing’s Syndrome • Clinical Case Presentation
Adrenal Gland
Q L

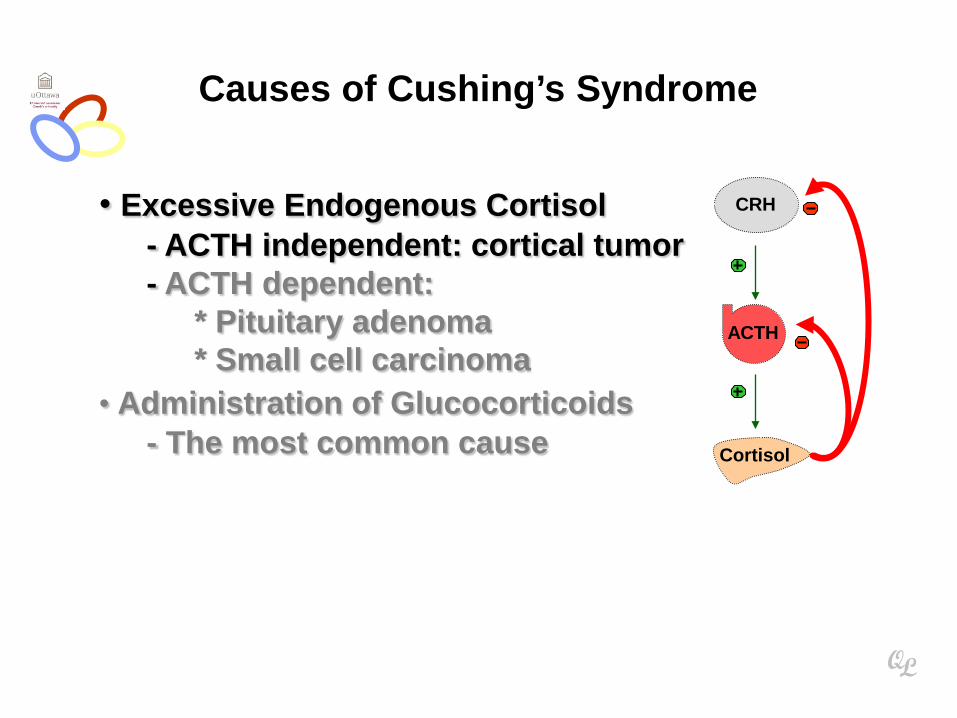
• Excessive Endogenous Cortisol - ACTH independent: cortical tumor - ACTH dependent:
* Pituitary adenoma * Small cell carcinoma
• Administration of Glucocorticoids - The most common cause
Cushing’s Syndrome
Q L
ACTH
CRH
Cortisol

Causes of Cushing’s Syndrome
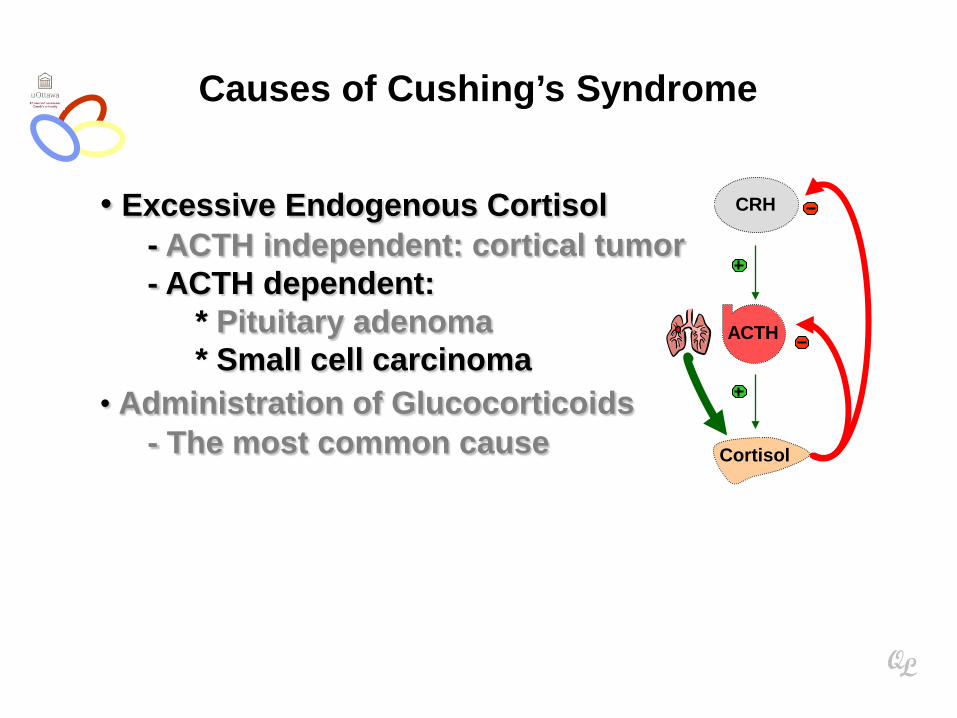
• Excessive Endogenous Cortisol - ACTH independent: cortical tumor - ACTH dependent:
* Pituitary adenoma * Small cell carcinoma
• Administration of Glucocorticoids - The most common cause
Causes of Cushing’s Syndrome
Q L
ACTH
CRH
Cortisol

• Excessive Endogenous Cortisol - ACTH independent: cortical tumor - ACTH dependent:
* Pituitary adenoma * Small cell carcinoma
• Administration of Glucocorticoids - The most common cause
Causes of Cushing’s Syndrome
Q L
ACTH
CRH
Cortisol
• Excessive Endogenous Cortisol - ACTH independent: cortical tumor - ACTH dependent:
* Pituitary adenoma * Small cell carcinoma
• Administration of Glucocorticoids - The most common cause
Causes of Cushing’s Syndrome
Q L
ACTH
CRH
Cortisol

• Excessive Endogenous Cortisol - ACTH independent: cortical tumor - ACTH dependent:
* Pituitary adenoma * Small cell carcinoma
• Administration of Glucocorticoids - The most common cause
Causes of Cushing’s Syndrome
Q L
ACTH
CRH
Cortisol

• Central Obesity (trunk & upper back) 85-90% • Moon face 85% • Weakness and fatigability 85% • Hirsutism 75% • Hypertension 75% • Plethora 75% • Glucose intolerance / diabetes 70 / 20% • Osteoprosis 75% • Moodiness, irritability or depression 75-80% • Menstrual abnormalities 70% • Skin striae (sides of lower abdomen) 50%
Clinical Manifestations

24-hour urine free cortisol level am & pm cortisol * for loss of diurnal rhythm, Hall mark Low-dose Dex suppression * identify Cushing's Syndrome High-dose Dex suppression * identify Cushing’s Disease
Screening Tests
Q L
ACTH
CRH
Cortisol

Low-dose Dex suppression Day 1: 1 mg of Dex is given at 11 pm Day 2: 0.5 mg of Dex every 6 hrs for 48 hrs High-dose Dex suppression Day 1: a baseline cortisol measured at am 8 mg of Dex is given at 11 pm Day 2: 2 mg of Dex every 6 hrs for 48 hrs. blood cortisol at 8 am on day 2 urinary cortisol for 3 days
Dexamethasone Suppression Test
Q L
ACTH
CRH
Cortisol
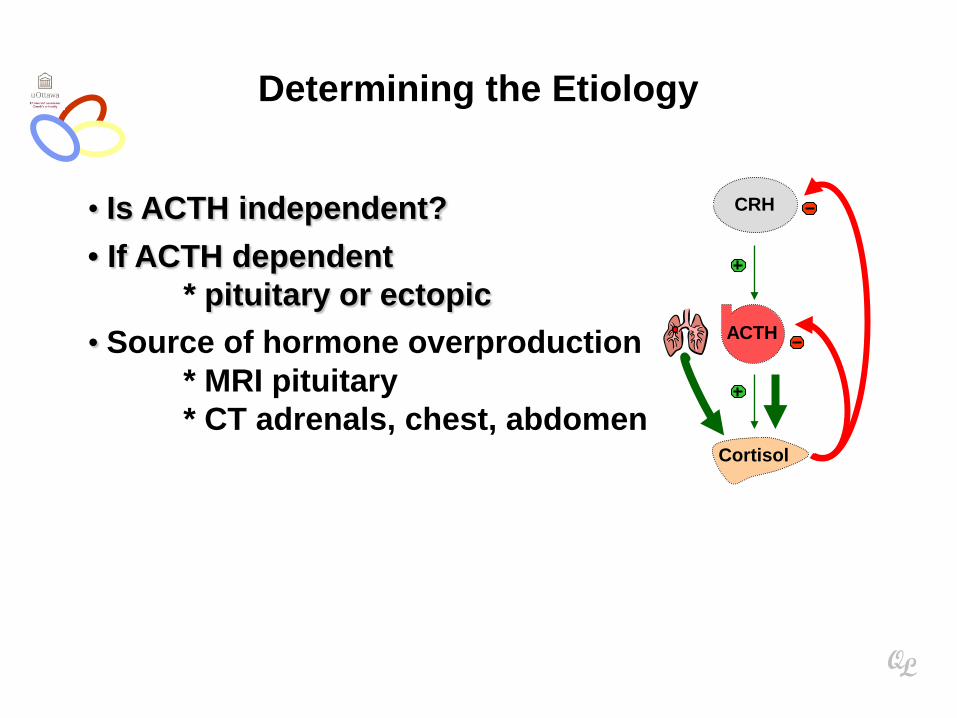
• Is ACTH independent?
• If ACTH dependent * pituitary or ectopic
• Source of hormone overproduction * MRI pituitary * CT adrenals, chest, abdomen
Determining the Etiology
Q L
ACTH
CRH
Cortisol

Adrenal Gland - Adenoma

Adrenal Gland - Mass

Adrenal Gland - Adenoma
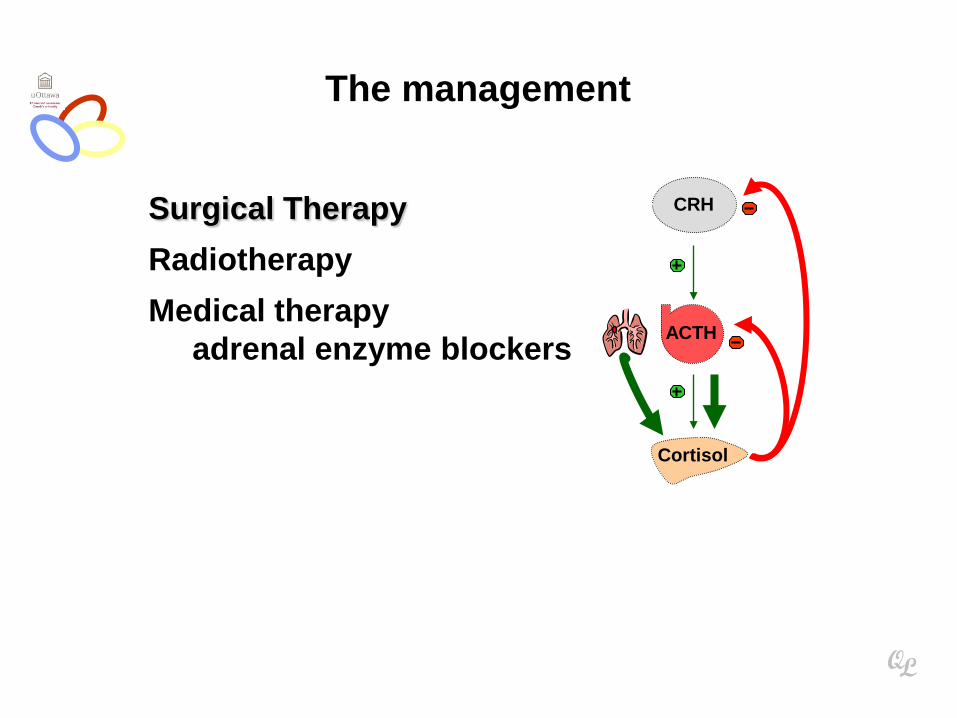
Surgical Therapy
Radiotherapy
Medical therapy adrenal enzyme blockers
The management
Q L
ACTH
CRH
Cortisol

Adrenal Gland
Q L
• Anatomy, Histology & Function • Steroid Hormones • Addison’s Disease • Cushing’s Syndrome • Clinical Case Presentation
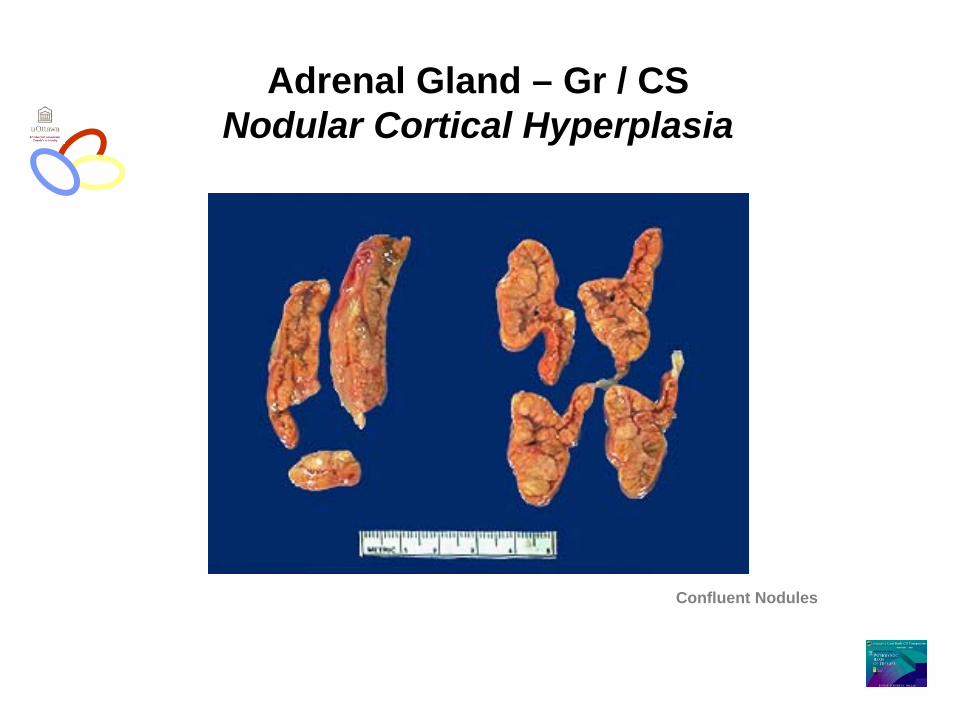
Adrenal Gland – Gr / CS Nodular Cortical Hyperplasia
Confluent Nodules

Nodule
Adrenal Gland – Low Power Nodular Cortical Hyperplasia
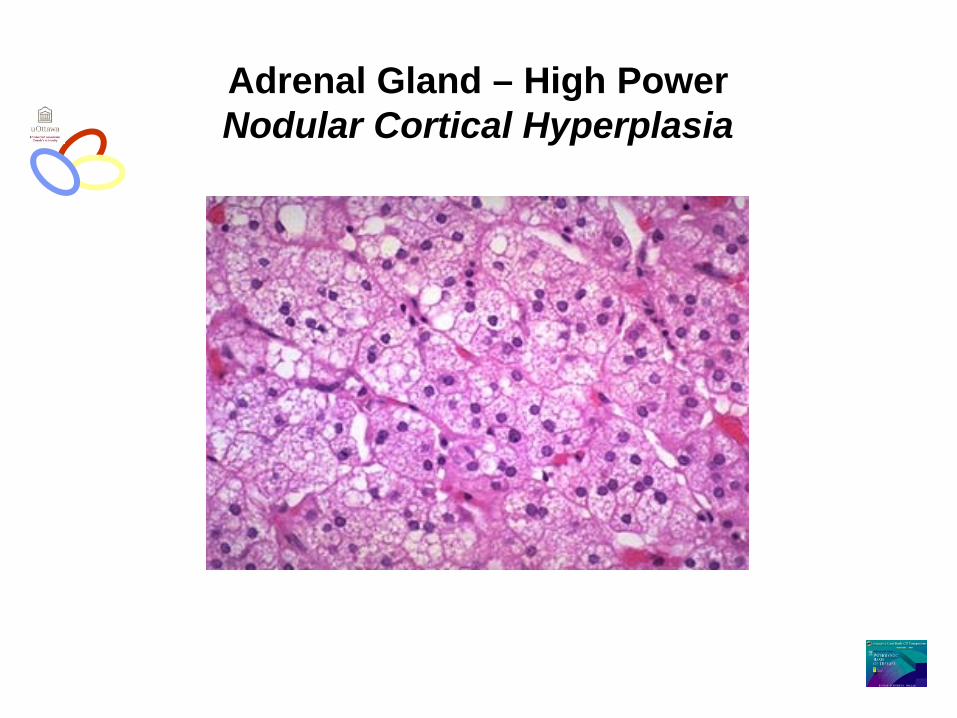
Adrenal Gland – High Power Nodular Cortical Hyperplasia
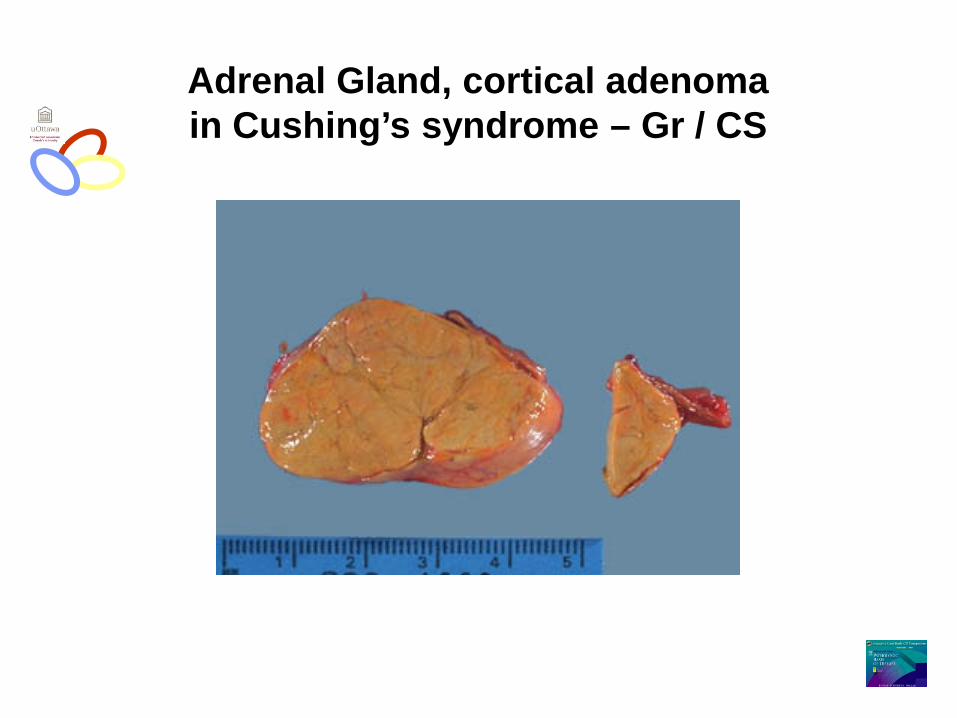
Adrenal Gland, cortical adenoma in Cushing’s syndrome – Gr / CS

Adrenal Gland, cortical adenoma - LP
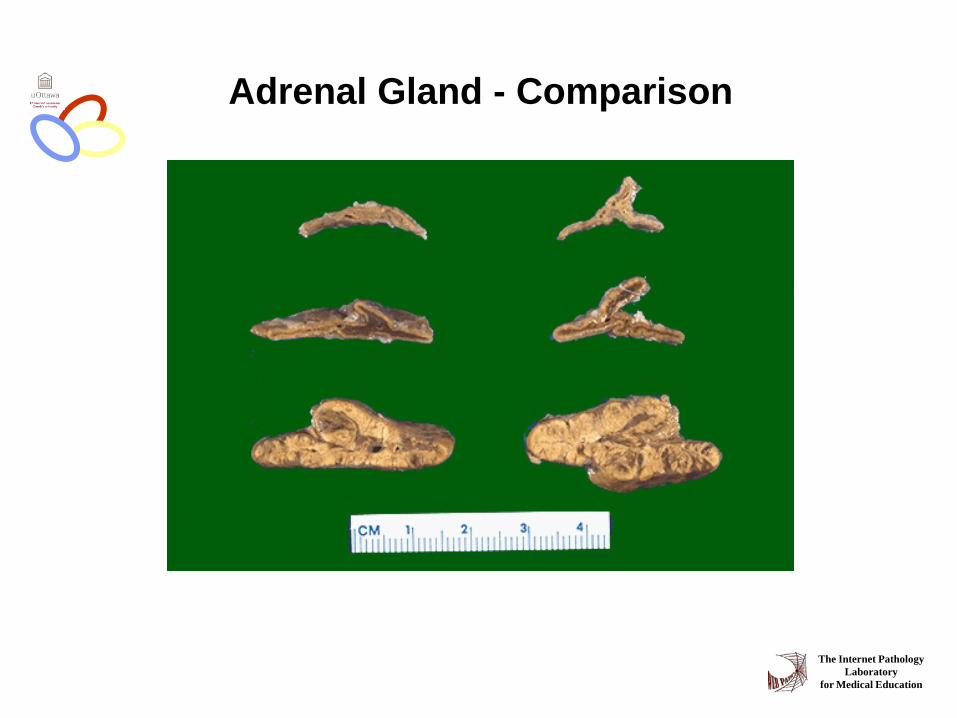
Adrenal Gland - Comparison
The Internet Pathology Laboratory
for Medical Education

Resources
• Pathologic Basis of Disease Robbins & Cotran 7th Edition
• Basic Pathology Robins 7th Edition
• Handbook of Clinical Pathology 2nd Edition
Q L