Embed Size (px)
Citation preview
I Clin Pathol 1995;48:325-329
The prevalence of lymphoid follicles inHelicobacter pylon associated gastritis in patientswith ulcers and non-ulcer dyspepsia
A M Zaitoun
Department ofHistopathology,Al Qassimi Hospital,Sharjah,United Arab EmiratesA M Zaitoun
Correspondence to:Dr A M Zaitoun,Mayday Healthcare NHSTrust, Mayday RoadThornton Heath,Surrey, CR7 7YE.
Accepted for publication10 May 1994
AbstractAims-To determine the prevalence oflymphoid follicles in Helicobacter pyloripositive and negative gastritis in antraland body type gastric mucosa in patientswith non-ulcer dyspepsia (NUD), duo-denal ulcer, or gastric ulcer; to correlatefollicle presence with patient age; to eval-uate the correlation between the pre-valence of lymphoid follicles and activeand inactive gastritis and its severity; andto assess the positive predictive value oflymphoid follicle prevalence with respectto H pyloni infection.
ta#f
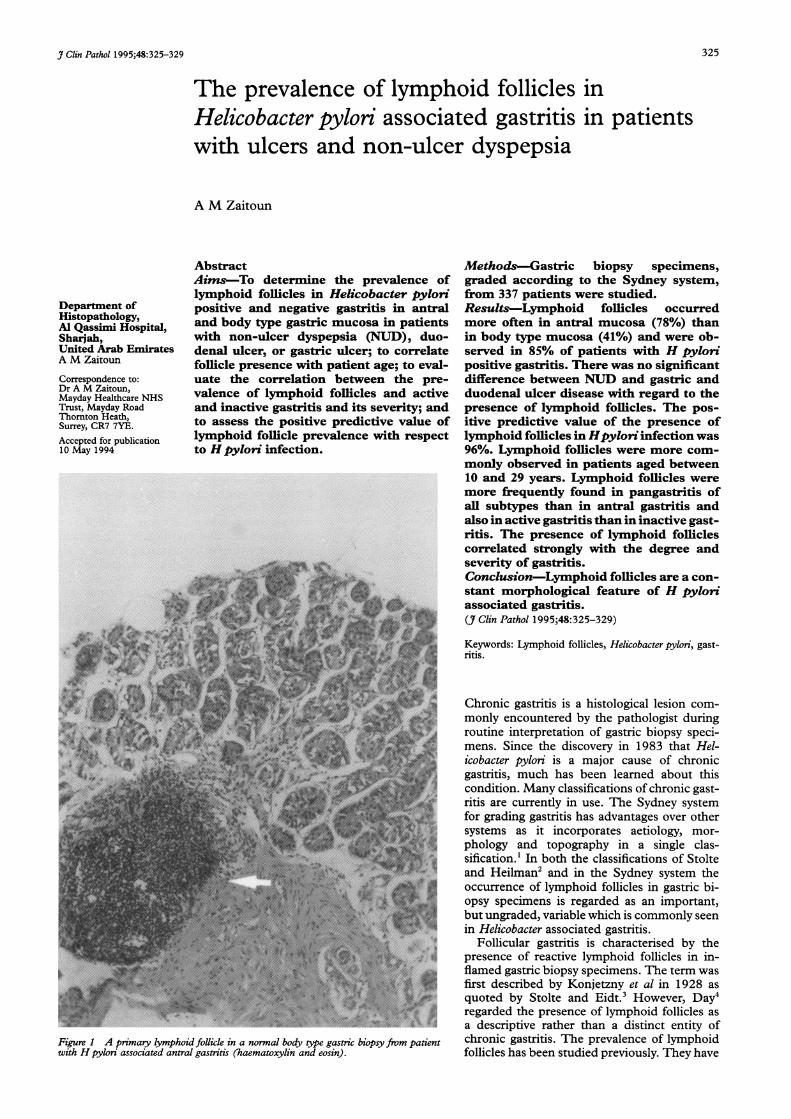
Figure 1 A primary lymphoid follicle in a normal body type gastric biopsy from patientwith H pylori associated antral gastritis (haematoxylin and eosin).
Methods-Gastric biopsy specimens,graded according to the Sydney system,from 337 patients were studied.Results-Lymphoid follicles occurredmore often in antral mucosa (78%) thanin body type mucosa (41%) and were ob-served in 85% of patients with H pylonpositive gastritis. There was no significantdifference between NUD and gastric andduodenal ulcer disease with regard to thepresence of lymphoid follicles. The pos-itive predictive value of the presence oflymphoid follicles in Hpylon infection was96%. Lymphoid follicles were more com-monly observed in patients aged between10 and 29 years. Lymphoid follicles weremore frequently found in pangastritis ofall subtypes than in antral gastritis andalso in active gastritis than in inactive gast-ritis. The presence of lymphoid folliclescorrelated strongly with the degree andseverity of gastritis.Conclusion-Lymphoid follicles are a con-stant morphological feature of H pylonassociated gastritis.(_7 Clin Pathol 1995;48:325-329)
Keywords: Lymphoid follicles, Helicobacter pylon, gast-ritis.
Chronic gastritis is a histological lesion com-monly encountered by the pathologist duringroutine interpretation of gastric biopsy speci-mens. Since the discovery in 1983 that Hel-icobacter pylori is a major cause of chronicgastritis, much has been learned about thiscondition. Many classifications of chronic gast-ritis are currently in use. The Sydney systemfor grading gastritis has advantages over othersystems as it incorporates aetiology, mor-phology and topography in a single clas-sification.' In both the classifications of Stolteand Heilman2 and in the Sydney system theoccurrence of lymphoid follicles in gastric bi-opsy specimens is regarded as an important,but ungraded, variable which is commonly seenin Helicobacter associated gastritis.
Follicular gastritis is characterised by thepresence of reactive lymphoid follicles in in-flamed gastric biopsy specimens. The term wasfirst described by Konjetzny et al in 1928 asquoted by Stolte and Eidt.3 However, Day4regarded the presence of lymphoid follicles asa descriptive rather than a distinct entity ofchronic gastritis. The prevalence of lymphoidfollicles has been studied previously. They have
325

Zaitoun
p.,.
4*
.eb,,1 {2 ktJjj*: A
8*N, -! 8
At.
* t * i ° '!; }s~~~~~~~~~~~~~~~~~~~~~~~~~~~~#. ...;
X,... s . . . 9 t . .'~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.....
8a *~ abg
....~~~~.........
*s~~~~~~~~~~~~~~~~~~~~~~~~~~~...0s ..; i . .
.:-b.*i .e ;,< :
* < ~~~~~~~~~~~~~~'. i. i ...............,i........-.
Figure 2 Primary lymphoid follicle in an antral biopsy specimen from a patient with Hpylori associated gastritis (haematoxylin and eosin).
been identified in 27.4%,5 54%3 and 66%6of patients with H pylori associated gastritis.However, the occurrence of lymphoid folliclesis not restricted to Hpylori associated gastritis.5In a more recent study7 careful examination ofmultiple specimens revealed lymphoid folliclesin the gastric mucosa of all patients with Hpylon infection. The frequency of lymphoidfollicles was found to be higher in the antrumthan the body in patients with duodenal andgastric ulcer disease.78The aims of this study were to evaluate
the occurrence of lymphoid follicles in gastricbiopsy specimens from patients with pepticulcer disease and non-ulcer dyspepsia (NUD);to study the correlation between the formationof lymphoid follicles, the age of the patients,and the activity and severity of gastritis; and toassess the positive predictive value of lymphoidfollicles with respect to H pylori infection.
i;'~MethodsPatients with ulcer disease and NUD attendingfive gastroenterology clinics in the northern
! region of the United Arab Emirates (UAE)were included in this study. Of the biopsy
i specimens taken, 337 fulfilled the criteria ofthe Sydney system for gastritis and were usedin this study.9 Patients were also grouped ac-cording to their clinical condition: NUD, duo-denal ulcer, or gastric ulcer. Biopsy specimenswere fixed in 10% formaldehyde and routinely
-¶uprocessed. Paraffin wax sections were cut intosections 4 pim thick. Each slide contained threeto five sections (nine to 15 sections examined).All specimens contained the full thickness of
gI.. the mucosa and muscularis mucosae. Sectionswere stained with haematoxylin and eosin,Diff-3 stain10 and alcian blue/periodic acid-Schiff stain (AB/PAS). Graded variables in-cluded the density of H pyloni organisms, in-flammation, activity, atrophy, and intestinalmetaplasia, which were classified as describedpreviously.' Each variable was divided into
-* three grades (grades I, II and III). The to-pographical patterns of Helicobacter associatedgastritis were also assessed.'9
Primary (lymphoid aggregate) and secondary(with germinal centres) lymphoid follicles wereassessed in all biopsy specimens (figs 1-3). Thepresence of one or more primary or secondarylymphoid follicles in the antrum and/or bodymucosa in any one patient was regarded as apositive result. The prevalence of lymphoidfollicles was correlated with the clinical con-dition, the age of the patient, the three gradesof activity in the antrum and body, and thegrade of severity of gastritis. The latter wasobtained from the mean combined values ofthe grades ofHpylori, inflammation and activityin both the antral and body mucosa. Patientswith gastric malignancies (lymphoma or car-cinoma) were excluded from the study andnone ofthe patients had tuberculosis or Crohn'sdisease.
STATISTICSDifferences between the groups were evaluatedusing the X2 test with Yates' correction. Theresults were considered significant if p<0 05(two tailed probability). The positive predictivevalue for lymphoid follicles in patients with Hpylori infection was obtained using the followingformula:
Positive predictive value= true positive x 100true positive + false positive
where false positive indicates idiopathic gastritiswith lymphoid follicles. The correlation be-tween the prevalence of lymphoid follicles andthe grade and severity of gastritis was assessedusing regression line analysis (r=0 91, twotailed probability p=0 0019, intercept a=57'43, slope b=6-16).
ResultsIn all gastric biopsy specimens examined thepercentage of secondary lymphoid follicles was
326P'.1.
-I.-
Lymphoid follicles in H pylori gastitis
on
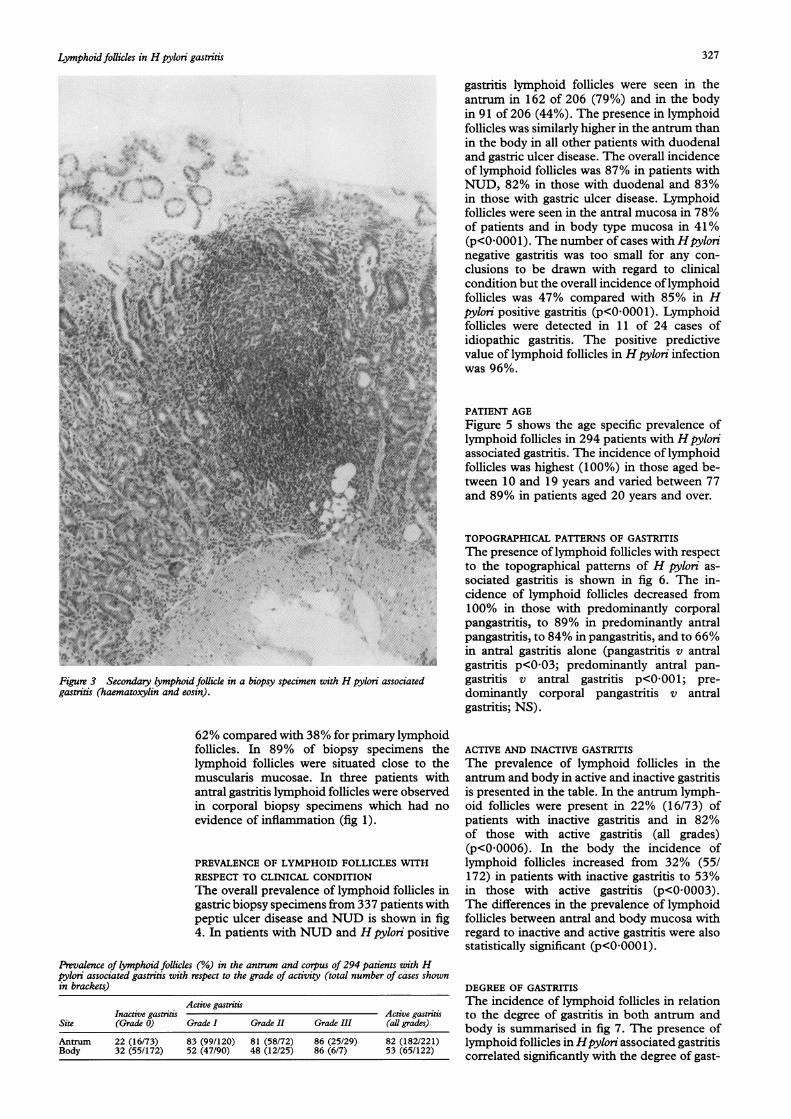
Figure 3 Secondary lymphoid follicle in a biopsy specimen with H pylori associatedgastritis (haematoxylin and eosin).
62% compared with 38% for primary lymphoidfollicles. In 89% of biopsy specimens thelymphoid follicles were situated close to themuscularis mucosae. In three patients withantral gastritis lymphoid follicles were observedin corporal biopsy specimens which had noevidence of inflammation (fig 1).
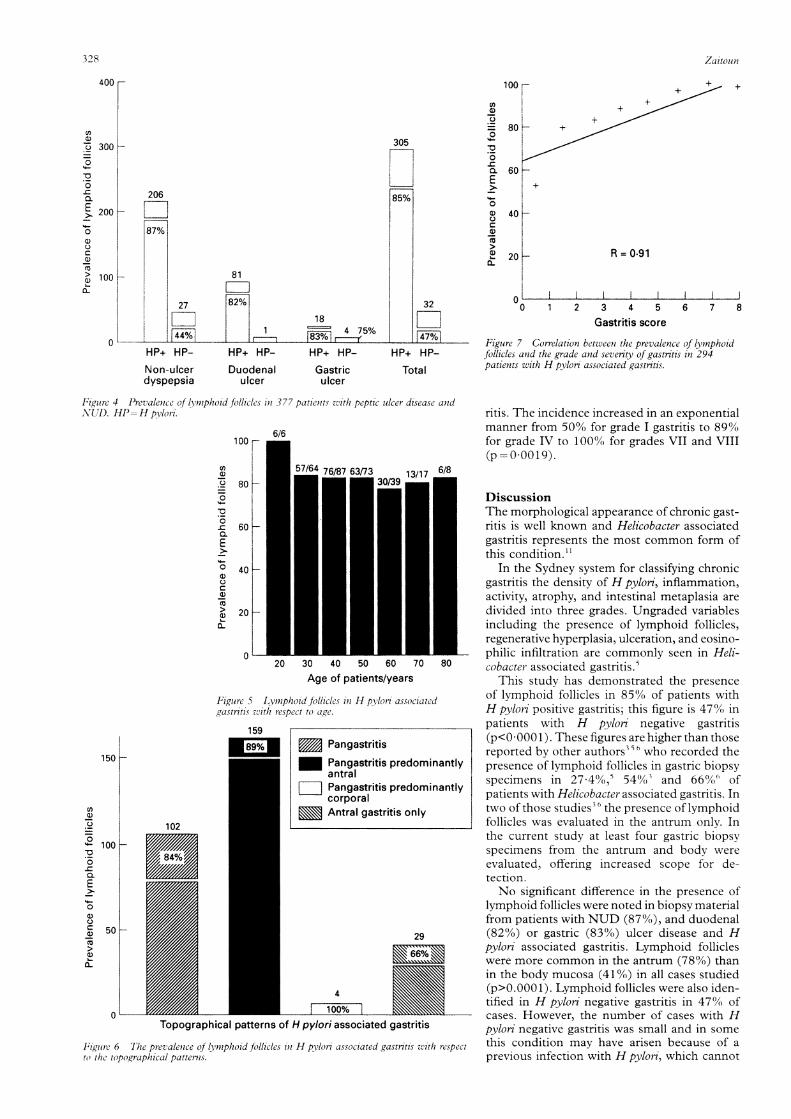
PREVALENCE OF LYMPHOID FOLLICLES WITHRESPECT TO CLINICAL CONDITIONThe overall prevalence of lymphoid follicles ingastric biopsy specimens from 337 patients withpeptic ulcer disease and NUD is shown in fig4. In patients with NUD and Hpylori positive
Prevalence of lymphoid follicles (%) in the antrum and corpus of 294 patients with Hpylon associated gastntis with respect to the grade of activity (total number of cases shownin brackets)
Active gastritisInactive gasttis Active gastritis
Site (Grade 0) Grade I Grade II Grade III (all grades)
Antrum 22 (16/73) 83 (99/120) 81 (58/72) 86 (25/29) 82 (182/221)Body 32 (55/172) 52 (47/90) 48 (12/25) 86 (6/7) 53 (65/122)
gastritis lymphoid follicles were seen in theantrum in 162 of 206 (79%) and in the bodyin 91 of 206 (44%). The presence in lymphoidfollicles was similarly higher in the antrum thanin the body in all other patients with duodenaland gastric ulcer disease. The overall incidenceof lymphoid follicles was 87% in patients withNUD, 82% in those with duodenal and 83%in those with gastric ulcer disease. Lymphoidfollicles were seen in the antral mucosa in 78%of patients and in body type mucosa in 41%(p<0O00 1). The number of cases with Hpylorinegative gastritis was too small for any con-clusions to be drawn with regard to clinicalcondition but the overall incidence oflymphoidfollicles was 47% compared with 85% in Hpylon positive gastritis (p<00001). Lymphoidfollicles were detected in 11 of 24 cases ofidiopathic gastritis. The positive predictivevalue of lymphoid follicles in Hpylori infectionwas 96%.
PATIENT AGEFigure 5 shows the age specific prevalence oflymphoid follicles in 294 patients with Hpyloriassociated gastritis. The incidence of lymphoidfollicles was highest (100%) in those aged be-tween 10 and 19 years and varied between 77and 89% in patients aged 20 years and over.
TOPOGRAPHICAL PATTERNS OF GASTRITISThe presence oflymphoid follicles with respectto the topographical patterns of H pylori as-sociated gastritis is shown in fig 6. The in-cidence of lymphoid follicles decreased from100% in those with predominantly corporalpangastritis, to 89% in predominantly antralpangastritis, to 84% in pangastritis, and to 66%in antral gastritis alone (pangastritis v antralgastritis p<003; predominantly antral pan-gastritis v antral gastritis p<0001; pre-dominantly corporal pangastritis v antralgastritis; NS).
ACTIVE AND INACTIVE GASTRITISThe prevalence of lymphoid follicles in theantrum and body in active and inactive gastritisis presented in the table. In the antrum lymph-oid follicles were present in 22% (16/73) ofpatients with inactive gastritis and in 82%of those with active gastritis (all grades)(p<0 0006). In the body the incidence oflymphoid follicles increased from 32% (55/172) in patients with inactive gastritis to 53%in those with active gastritis (p<0 0003).The differences in the prevalence of lymphoidfollicles between antral and body mucosa withregard to inactive and active gastritis were alsostatistically significant (p<0 0001).
DEGREE OF GASTRITISThe incidence of lymphoid follicles in relationto the degree of gastritis in both antrum andbody is summarised in fig 7. The presence oflymphoid follicles in Hpylori associated gastritiscorrelated significantly with the degree of gast-
327
.1- -
4.i,4.
.1.'.," ,
'... . .4"I., I
328
100
81l
27 82%
1 118
4 75%
305
85%
U)0
0.
-
00.C
0~
0
c
a)
>-
80~
,+>,/~~~~~
60 _+
40 H
20 H
oL032
F4-7%-HP+ HP- HP+ HP- HP+ HP- HP+ HP-
Gastriculcer
Total
R = 0-91
1 2 3 4 5Gastritis score
6 7 8
Figure 4 Prevalence of lvnzphoid follicles in 377 patienits azith peptic ulcer disease as,NUD. HP=H p,lori.
100
a,)01)0.5_0
0.
E0
0)0C0)
0
0
80
60
40
20
0
6/6
20 30 40 50 60 70Age of patients/years
Figuire 5 Lymnphoid follicles inl H pylon' associatedgastnrtis zlth respect to age.
159
8% E PangastritisPangastritis predomin;antral
E Pangastritis predomin;corporalAntral gastritis only
102
29
4
100%
Topographical patterns of H pylori associated gastritis
84
Figlurec 6 The prevalenice of lysnphoid follicles in H pyloni associated gastrntis with re.
to thc topographical patterns.
ritis. The incidence increased in an exponentialmanner from 50% for grade I gastritis to 89%for grade IV to 100% for grades VII and VIII(p= 00019).
8
DiscussionThe morphological appearance of chronic gast-ritis is well known and Helicobacter associatedgastritis represents the most common form ofthis condition.1
In the Sydney system for classifying chronicgastritis the density of H pylon', inflammation,activity, atrophy, and intestinal metaplasia aredivided into three grades. Ungraded variablesincluding the presence of lymphoid follicles,regenerative hyperplasia, ulceration, and eosino-philic infiltration are commonly seen in Heli-
° cobacter associated gastritis.'This study has demonstrated the presence
of lymphoid follicles in 85% of patients withH pylori positive gastritis; this figure is 47' inpatients with H pylon' negative gastritis(p<0 000 1). These figures are higher than thosereported by other authors '6 who recorded the
itly presence of lymphoid follicles in gastric biopsyspecimens in 274%, 540%S3 and 66%` of
ntly patients with Helicobacter associated gastritis. Intwo of those studies36 the presence of lymphoidfollicles was evaluated in the antrum onlv. Inthe current study at least four gastric biopsyspecimens from the antrum and body wereevaluated, offering increased scope for de-tection.No significant difference in the presence of
lymphoid follicles were noted in biopsy materialfrom patients with NUD (87%), and duodenal(82%) or gastric (83%) ulcer disease and Hpylon' associated gastritis. Lymphoid follicleswere more common in the antrum (78%) thanin the body mucosa (410%) in all cases studied(p>0.000 1). Lymphoid follicles were also iden-tified in H pylon' negative gastritis in 47% ofcases. However, the number of cases with Hpylon negative gastritis was small and in some
spect this condition may have arisen because of aprevious infection with H pylorn, which cannot
400
300 HU,
.5
0.E
0
0)
0aca)
>
206
[87200 H
100 H
0
Non-ulcer Duodenaldyspepsia ulcer
Figure 7 Correlation between the prevalence of lyinphoidfollicles and the grade and seven't of gastritis in 294patients with H pylori associated gastnrtis.
150 K iar
0)
)
V0
'.
20E
0
c0)
Q)L-
100 K
50 H
0
Il1III-
Zai'toUll
Id
Lymphoid follicles in H pylori gastritis
be evaluated by histological methods alone.'2The positive predictive value of lymphoid foll-icles in H pylori infection was 96%. This is inaccord with a recent study by Genta et al7 whofound that lymphoid follicles were present ingastric biopsy specimens from all patients in-fected with Hpyloni, detected using the mappedgastric biopsy specimen technique.The results of this study confirm the findings
of two recent studies78 which showed that theprevalence of lymphoid follicles was higher inthe antral mucosa than the body mucosa inpatients with duodenal and gastric ulcer dis-ease. In addition, the current study dem-onstrated similar findings in patients withNUD. A possible explanation for the lowerprevalence of lymphoid follicles in the bodymucosa may be related to the degree of gastricinflammation which is higher in the antrumthan the body.9 The presence of lymphoid foll-icles in all cases of predominantly corporalpangastritis (fig 6) supports such a hypothesis.The formation of lymphoid follicles in H
pylon associated gastritis occurred in 100% ofpatients aged between 10 and 19 years. Mahonyand Littlewood'3 reported that lymphoid foll-icles are a prominent feature of biopsy speci-mens from paediatric patients with H pyloriassociated antral gastritis and correlate wellwith the presence of antral nodularity on en-doscopy. In another study follicular gastritiswas seen in 10 of 11 paediatric patients withantral nodularity'4 giving a sensitivity of 96-4%for the diagnosis of H pylori infection in thepaediatric age group.'5 The incidence oflymph-oid follicles decreased to 89% in patients agedbetween 20 and 29 years and to approximately82% thereafter.Another important finding of this study is
the significant correlation between the to-pographical pattern of Hpylori associated gast-ritis and the presence of lymphoid follicles.Predominantly antral pangastritis was as-sociated with lymphoid follicles in 89% ofspecimens compared with 66% for antral gast-ritis alone (p<0.0008).A significant difference in the presence of
lymphoid follicles between inactive and activegastritis was noted in both the antrum (22 v82%; p<00006) and body (32 v 53%;p<0.0003). These results are in accord withthose reported previously.36The data suggest that the relation between
the presence of lymphoid follicles and the de-gree of gastritis is linear (r= 0 91). The higherdegree of gastritis, the higher the incidence oflymphoid follicles. These results are also inkeeping with those reported by other authors.6Some authors5'6'7 have reported that many
ofthe lymphoid follicles are present deep withinthe gastric mucosa, as was the case in this studywhere 89% of the lymphoid follicles (primaryand secondary) occurred very close to the baseof gastric mucosa. Thus, most lymphoid foll-
icles, if not all, originate in the lower part ofthe mucosa close to the muscularis mucosae.This may be explained by the presence of alymphatic vessel plexus in the deeper part of themucosa. Similar findings have been observed inexperimental animals.'6 Radin et al'6 found thatlymphoid follicle formation was most prom-inent in the antrum and close to basal borderof the lamina propria.
In conclusion, lymphoid follicles are a con-stant feature of H pylon infection. There wasno difference in the prevalence of lymphoidfollicles in patients with NUD, duodenal ulceror gastric ulcer disease. The positive predictivevalue of lymphoid follicles in Hpylori infectionwas 96%. Lymphoid follicles were detectedmore frequently in the antrum than in the body.They were also more frequent in the seconddecade of life and in active gastritis more thanin inactive gastritis. The presence of lymphoidfollicles was strongly correlated with the degreeand severity ofgastritis. Lymphoid follicles werepresent in uninflamed body mucosa frompatients with Hpylori associated antral gastritis.
1 Price AB. The Sydney System: Histological division. JGastroenterol Hepatol 1991;6:209-22.
2 Stolte M, Heilmann KL. New classification of gastritis.Leber Magen Darm 1989;19:220-6.
3 Stolte M, Eidt S. Lymphoid follicles in antral mucosa:immune response to Campylobacter pylori. Jf Clin Pathol1989;42:1269-71.
4 Day DW. The stomach. In: Morson BC, ed. Alimentarytract. Volume 3. Systemic pathology. Edinburgh: ChurchillLivingstone, 1987:149-228.
5 Wyatt JI, Rathbone BJ. Immune response of the gastricmucosa to Campylobacter pylori. Scand J Gastroenterol1988;23(Suppl 142):44-9.
6 Hauke C, Grabner W, Grosse M, Stolte M. Lymph follicleformation and development of intestinal metaplasia inantrum mucosa as a reaction to Helicobacter pylori in-fection [in German]. LeberMagen Darm 1991;21:156-60.
7 Genta RM, Hamner HW, Graham DY Gastric lymphoidfollicles in Helicobacter pylori infection: Frequency, dis-tribution and response to triple therapy. Hum Pathol 1993;24:577-83.
8 Eidt S, Stolte M. Prevalence of lymphoid follicles andaggregates in Helicobacter pylori gastritis in antral andbody mucosa. J Clin Pathol 1993;46:832-5.
9 Zaitoun AM. Histological study of chronic gastritis fromthe United Arab Emirates using the Sydney system ofclassification. 7 Clin Pathol 1994;47:810-15.
10 Zaitoun AM. Use of Romanowsky type (Diff-3) stain fordetecting Helicobacter pylori in smears and tissue sections.J Clin Pathol 1992;45:448-9.
11 Dixon MF. Helicobacter pylori and chronic gastritis. In:Rathbone BJ, Heatley RV, eds. Helicobacter pylon andgastroduodenal disease. 2nd edn. Oxford: Blackwell Sci-entific Publications, 1992:124-39.
12 Kames WEJ, Samlof IM, Siurala M, Kekki M, SipponenP, Kim SWR, et al. Positive serum antibody and negativetissue staining for Helicobacter pylori in subjects withatrophic body gastritis. Gastroenterology 199 1;101: 167-74.
13 Mahony MJ, Littlewood JM. Helicobacter pylori in a pae-diatric population. In: Rathbone BJ, Heatley RV, eds.Helicobacter pylon and gastroduodenal disease. 2nd edn.Oxford: Blackwell Scientific Publications, 1992;177-86.
14 De Giacomo C, Fiocca R, Villani L, Lisato L, Licardi G,Diegoli N, et al. Helicobacter pylori infection and chronicgastritis. Clinical, serological and histological correlationsin children treated with amoxicillin and colloidal bismuthsubstrate. J Pediatr Gastroenterol Nutr 1990;11:310-16.
15 Conti-Nibali S, Sferlazzas C, Fera MT, Saitta G, TedeschiA, Magazzu G. Helicobacter pylori infection: a simplifieddiagnostic approach. Am J Gastroenterol 1990;85:1573-5.
16 Radin MJ, Eaton KA, Krakowka S, Morgan DR, Lee A,Otto G, et al. Helicobacter pylori gastritis infection inGnotobiotic Beagle Dogs. Infect Immun 1990;58:2606-12.
17 Wotherspoon AC, Ortiz-Hidalgo C, Falzon MR, IsaacsonPT. Helicobacter pylori-associated gastritis and primaryB-cell gastric lymphoma. Lancet 1991;338:1175-6.
329












![Research Paper Clinicopathological and …hyperplastic lymphoid follicles, mitotically active germinal centers with well-defined lymphocytic mantles [2]. The pathogenesis of NLH remains](https://img.pdfslide.net/doc/110x75/5e84349d77fd3b74c21aa82f/research-paper-clinicopathological-and-hyperplastic-lymphoid-follicles-mitotically.jpg)