Embed Size (px)
DESCRIPTION
PROMISE P erformance R eporting and O utcomes M easurement to I mprove the S tandard of care at E nd-of-life. The PROMISE team HPC meeting, St Louis May 12, 2009. Objectives:. To introduce the PROMISE center To explain PROMISE: Methods Reports To describe where PROMISE is going; and - PowerPoint PPT Presentation
Citation preview

PROMISEPerformance Reporting and Outcomes
Measurement to Improve the Standard of care at End-of-life
The PROMISE team
HPC meeting, St Louis
May 12, 2009

Objectives:
To introduce the PROMISE centerTo explain PROMISE:
» Methods» Reports
To describe where PROMISE is going; andTo identify ways in which we’ll need your help

PROMISE goals:
To identify and reduce unwanted variation in the quality of end-of-life care for veterans.
To define and disseminate processes of care that contribute to improved outcomes for veterans near the end of life and their families.

What is PROMISE?
The quality measurement center for the CELC Initiative
Based at the Philadelphia VAMC Center for Health Equity Research and Promotion
Funded through the CELC to provide:» A voice for veterans/families» Actionable data that can guide facility-
VISN- and national-level planning and strategy.

What does PROMISE deliver?
Data for facilities about the quality of end-of-life care they provide» Timely feedback» Understandable reports» Meaningful benchmarks
Practical guidance for HPC programsUseful evaluations for CELC Initiative
leadership

Framework for PROMISE data: Domains of care (from NCP guidelines)
Physical aspects of careSocial aspects of careSpiritual, religious, and existential aspects
of careCultural aspects of care Care of the imminently dying patientPsychological and psychiatric aspects of
care (including bereavement)

Framework for PROMISE data: Aspects of care
Processes of care (from chart reviews)
Outcomes (Families’ perceptions of care)
Currently (Q1 FY09) 43 facilities:» ~800 interviews/quarter» ~1600 chart
reviews/quarter

Processes of care: Chart review
Sample:» Inpatient deaths» Excluding “unexpected” deaths (e.g. ER, suicide,
homicide, OR for outpatient procedure)
Deaths identified using VISN data (multiple overlapping samples)
Remote chart reviews via Global CPRS

Processes of care: (examples)
Pain assessment within 24 hours of last admission
Palliative care consultation noteDocumentation of a surrogate or that a
surrogate could not be foundChaplain contact with veteran/familySocial work noteDocumentation of a bereavement contact

Processes of care: Documentation of a surrogate decision-maker

Outcomes of care: The Bereaved Family Survey
BFS: OMB-approved survey derived from the Family Assessment of Treatment at End-of-life (FATE)
14-item telephone survey administered to the veteran’s NOK 6-10 weeks after death
Procedure:» Predefined algorithm for contacts (NOK first choice)» Initial letter with opt-out provision» Telephone contact» Opportunity for family members to refer to alternate

Outcomes of care: 12 multiple-choice BFS items
Pain management (1)Communication (Providers gave enough
information in an understandable way and took time to listen) (3)
Veteran didn’t receive unwanted treatment (1)Providers were kind, caring, and respectful (1)Family was told what to expect in the veteran’s
last hours of life (1) Veteran’s personal care needs were met (1)Spiritual support, emotional support (pre/post) (3)Enough help with funeral arrangements (1)

Outcomes of care: BFS scoring
All items are either dichotomous or frequency-based» Did you receive as much help as you needed with…
» How often did the health care providers who took care of [veteran]…
Responses dichotomized (Best possible response vs. all others).
BFS and item scores reflect a proportion of the time that the veteran/family received the best possible care.

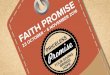
BFS scores: 43 facilities
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Facility

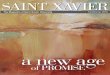
Families’ perceptions of bereavement support: 43 facilities
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Facility

Quarterly VISN-level reports
Categories match NCP domainsReports broken down by facility (Process and
outcome measures)Compared to sample benchmark (pooled
mean of top facilities)Hypertext links to:
» Best Practices on PROMISE website» SharePoint tools (Luhrs)

Additional data…responses to 2 open-ended questions
“The hospice unit was the best part of the care that [veteran] got in the whole 14 years that he was going to the VA.”
“We really depended on the palliative team—they were wonderful.”
“Everyone was very helpful, but especially [NP on PCCT]. She was always there, always available. We wouldn’t have made it without her.”

Additional data…referrals for unmet needs
Unmet needs identified in interviews:» Bereavement
» Questions about care
» Questions about benefits
Referred to VISN coordinator and/or facility patient advocate (with family permission).
Gives us:» An opportunity to meet needs and to leave families with
a good impression of the VA
» Valuable data about needs for improvement

Can you give us even more data?

Additional data…
Aggregate (broken down) data available to each VISN
“Raw” data available on requestMenu-driven custom reports online (at
PROMISE website)» “Mean BFS score in our ICU, with and without
palliative care”» “Mean bereavement score in our VISN, with and
without a bereavement contact”

Using the PROMISE report: 6 rules
1. Don’t panic
2. Focus! (Look at individual items)
3. Ask: Do you have enough data? (Two quarters’ worth)
4. Use common sense (does this score make sense?)
5. Select one item to improve that has:1. A low score
2. An obvious action plan
6. Be skeptical about changes

Interpreting changes:What happened in these facilities?
A facility improves its BFS score from 45 to 60 in 3 months
Answer: NothingA facility improves its bereavement score from
49 to 65 in 3 monthsAnswer: A social worker dedicated to
bereavement calls; educational materials for family; a condolence letter for all deaths.
Lesson: Be critical about scores and changes

Closing the loop: Bringing the veteran’s and family’s voice back to
the bedside

Help us close the loop (1-2)
1. “Success stories” solicited from field» Structured description via web-based form (Through
PROMISE website)» Submit descriptions of:
• Good scores
• Improvements
• How you’re using PROMISE data
2. “QI Registry” tracking single-facility interventions» Structured description of goal, intervention, and expected
outcome submitted via web-based form (Through PROMISE website)

Help us close the loop (3)
3. “QI Collaboratives” that track multiple-facility interventions» Best Practices reviewed/selected by advisory
panels (Carol Luhrs and Therese Cortez)» Designated leader» Organized schedule» Technical assistance» Measurement/analysis by PROMISE» Tailored feedback

PROMISE Implementation
Guidelines/ Expert opinion

PROMISE goals:
To identify and reduce unwanted variation in the quality of end-of-life care for veterans.
To define and disseminate processes of care (“Best Practices”) that contribute to improved outcomes for veterans near the end of life and their families.

Progress and next steps
Rollout:» 7 VISNs on board FY08» Goal: 12 in FY09; 21 in FY10
Dissemination: PROMISE website coming onlineMeasurement:
» Refine process measures» Implement Success Stories; QI registry; Collaboratives

PROMISE website:www.cherp.research.va.gov/PROMISE
(Non-VA site: www.caringforveterans.org)Find out more about PROMISERegister a QI initiativeBrag about a success storyJoin a QI collaborativeLearn about best practices (coming soon)