Embed Size (px)
Citation preview

[page 78] [Pediatric Reports 2012; 4:e20]
The Prune Belly syndrome:urological aspects andlong-term outcomes of a rare diseaseVahudin Zugor,1 Günter E. Schott,2Apostolos P. Labanaris11Department of Urology and PediatricUrology-Prostate Center Northwest,St. Antonius Medical Center, Gronau;2Deparment of Urology, University ofErlangen Medical Center, Erlangen,Germany
Abstract
Prune-Belly syndrome is a disorder charac-terized by the following triad of symptoms:deficiency of the abdominal muscles, malfor-mations of the urinary tract and bilateral cryp-torchidism. This study included a total of 16patients. The findings included clinical charac-teristics, diagnostics, therapy and long-termclinical outcomes. All patients were asked tocomplete a questionnaire and, in some cases,were given further examination. All patientswere diagnosed with congenital aplasia of theabdominal wall and a variety of urogenital mal-formations. Cryptorchidism was present in 11patients (68.8%), malformations of theprostate in 3 (18.8%), urethral malformationsin 8 (50%) and mega-ureter in 14 patients(87.5%). A mega-bladder was observed in 13patients (81.3%). Distinctive renal malforma-tions, such as renal dysplasia, in 3 patients(18.8%) and hydronephrosis in 9 patients(56.3%), respectively. Abdominoplasty was per-formed on 4 patients (25%). Urethral surgerywas performed in 10 patients (62.5%). Sevenpatients (43.8%) required ureter surgery, mostof which involved re-implantation of the ureterand, in some cases, additional ureter model-ing. Renal surgery was performed on 5patients. Four patients with non-functioningkidneys with hydronephrosis underwent anephrectomy and one patient pyeloplasty. Wedemonstrate that successful treatment is pos-sible even in cases of serious and complexmalformations, such as those of the Prune-Belly syndrome. Treatment must be tailored tothe individual patient. The severity of the renaldysplasia is the main prognostic factor.
Introduction
Prune-Belly syndrome (PBS) is a rare mal-formation disorder (1 in 40,000 live births),
affecting almost exclusively males (>95%),and characterized by a triad of clinical featuresincluding urinary tract anomalies, abdominalwall deficiency and bilateral cryptorchidism.Nowadays, not as many children with PBS areseen in clinical practice as in the past, mainlydue to prenatal ultrasound and subsequentpregnancy termination of affected cases.
The protruding hypoplastic abdominal walllooks like a dried prune, hence the namePrune-Belly.1-5 However, abortive forms areoften also presented in which hypoplasia of theabdominal wall is not particularly severe.Malformations of the urinary tract are due todysplasia of the smooth muscles of the renalpelvis and of the ureters, as well as of the pro-static part of the urethra. Depending on typeand severity, the syndrome presents with threedifferent clinical manifistations: i) the non-viable oliguric form with severe kidney dyspla-sia; ii) a serious form consisting of markedrenal dysplasia, with mega-ureters, mega-vesi-cles, and progressive renal failure; and iii) themore favorable form with moderate renal dys-plasia and different degrees of enlargement ofthe ureters and bladder.1,3,5
Prune-Belly syndrome is a complex malfor-mation disorder with wide variability in sever-ity and clinical manifestations. A thoroughexamination, usually as regular follow-upanalyses, should establish the diagnosis anddetermine the perinatal management. Thisdiagnosis should be considered when prenatalabdominal wall deficiencies have been con-firmed.6,7
The purpose of this study is to present ourclinical experience with children proven to havePrune-Belly syndrome, as well as to outline thesurgical treatment options that can be used.
Materials and Methods
All clinical records of patients with Prune-Belly syndrome who were treated at theErlangen Pediatric Urology departmentbetween 1970 and 2006 were again analyzedretrospectively. Questionnaires were sent outto all patients, some of whom (7 children)underwent further examination. Statisticalanalysis was carried out with the SPSS pro-gram. A total of 16 patients were included inthe study. Findings cover clinical characteris-tics, diagnostics, therapy, and long-term clini-cal outcome.
Results
The sample population consisted of 16patients in whom Prune-Belly syndrome hadbeen clinically verified. There were 14 male
(86.7%) and 2 female (13.3%) patients.Survival rate after ten years was 93.7%. At thetime of diagnosis, average age was 7.4 yearsand median age 9.3 years. The youngestpatient was 1.2 years old and the oldest 12.9years old. Mean follow-up time was 17 years.Prune-Belly syndrome had been clinically con-firmed in all patients. All children had beendiagnosed with congenital aplasia of theabdominal wall and a variety of urogenital mal-formations. Cryptorchidism was present in 11children (68.8%), malformations of theprostate in 3 (18.8%), urethral malformationsin 8 (50%) and mega-ureter in 14 (87.5%) chil-dren. A mega-bladder was observed in 13 chil-dren (81.3%). Distinctive renal malformations,such as renal dysplasia in 3 children (18.8%)and hydronephrosis in 9 children (56.3%)(Table 1). Other related malformations, suchas atrial septum defect (ASD), patent ductusarteriosus (PDA), spina bifida occulta andclub-foot were found in a total of 5 children(31.2.%) (Table 1).
These patients did not receive homoge-neous treatment and they were treated overdifferent time periods. Our methodology wasoften individually targeted, geared towardstreating the clinical symptoms and congenitalurogenital malformations according to severityand form. Abdominoplasty was performed in 4children (25%). Urethral surgery was per-formed in 10 children (62.5%). We first carriedout a variety of endoscopic procedures in orderto ensure a regular urine flow (in 50% ofcases). Open urethral surgeries, such as ure-thralplasty and correction of epispadia, wereperformed in 2 children (12.6%). Bladder sur-gery was necessary in 10 children (62.5%);bladder reduction surgery was the most com-mon procedure performed (31.3%) (Table 2).Seven children (43.8%) had to undergo ureter
Pediatric Reports 2012; volume 4:e20
Correspondence: Apostolos P. Labanaris, ProstateCenter Northwest, Department of Urology andPediatric Urology, St. Antonius Medical Center,Moellenweg 22, 48599 Gronau, Germany.Tel. +49.2562.915.7114 - Fax: +49.2562.915.2105.E-mail: [email protected]
Key words: Prune-Belly syndrome, diagnosis,therapeutic options, surgical treatment.
Received for publication: 30 May 2011.Revision received: 17 November 2011.Accepted for publication: 18 November 2011.
This work is licensed under a Creative CommonsAttribution NonCommercial 3.0 License (CC BY-NC 3.0).
©Copyright V. Zugor et al., 2012Licensee PAGEPress, ItalyPediatric Reports 2012; 4:e20doi:10.4081/pr.2012.e20
[Pediatric Reports 2012; 4:e20] [page 79]
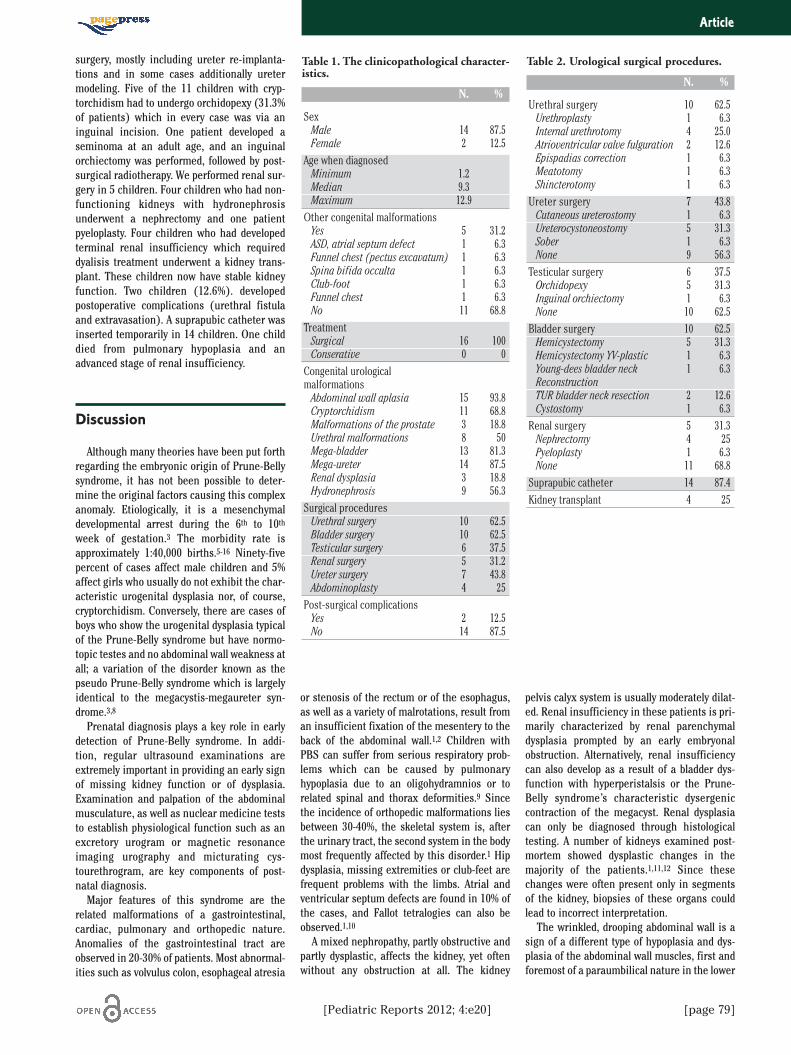
surgery, mostly including ureter re-implanta-tions and in some cases additionally uretermodeling. Five of the 11 children with cryp-torchidism had to undergo orchidopexy (31.3%of patients) which in every case was via aninguinal incision. One patient developed aseminoma at an adult age, and an inguinalorchiectomy was performed, followed by post-surgical radiotherapy. We performed renal sur-gery in 5 children. Four children who had non-functioning kidneys with hydronephrosisunderwent a nephrectomy and one patientpyeloplasty. Four children who had developedterminal renal insufficiency which requireddyalisis treatment underwent a kidney trans-plant. These children now have stable kidneyfunction. Two children (12.6%). developedpostoperative complications (urethral fistulaand extravasation). A suprapubic catheter wasinserted temporarily in 14 children. One childdied from pulmonary hypoplasia and anadvanced stage of renal insufficiency.
Discussion
Although many theories have been put forthregarding the embryonic origin of Prune-Bellysyndrome, it has not been possible to deter-mine the original factors causing this complexanomaly. Etiologically, it is a mesenchymaldevelopmental arrest during the 6th to 10th
week of gestation.3 The morbidity rate isapproximately 1:40,000 births.5-16 Ninety-fivepercent of cases affect male children and 5%affect girls who usually do not exhibit the char-acteristic urogenital dysplasia nor, of course,cryptorchidism. Conversely, there are cases ofboys who show the urogenital dysplasia typicalof the Prune-Belly syndrome but have normo-topic testes and no abdominal wall weakness atall; a variation of the disorder known as thepseudo Prune-Belly syndrome which is largelyidentical to the megacystis-megaureter syn-drome.3,8
Prenatal diagnosis plays a key role in earlydetection of Prune-Belly syndrome. In addi-tion, regular ultrasound examinations areextremely important in providing an early signof missing kidney function or of dysplasia.Examination and palpation of the abdominalmusculature, as well as nuclear medicine teststo establish physiological function such as anexcretory urogram or magnetic resonanceimaging urography and micturating cys-tourethrogram, are key components of post-natal diagnosis.
Major features of this syndrome are therelated malformations of a gastrointestinal,cardiac, pulmonary and orthopedic nature.Anomalies of the gastrointestinal tract areobserved in 20-30% of patients. Most abnormal-ities such as volvulus colon, esophageal atresia
or stenosis of the rectum or of the esophagus,as well as a variety of malrotations, result froman insufficient fixation of the mesentery to theback of the abdominal wall.1,2 Children withPBS can suffer from serious respiratory prob-lems which can be caused by pulmonaryhypoplasia due to an oligohydramnios or torelated spinal and thorax deformities.9 Sincethe incidence of orthopedic malformations liesbetween 30-40%, the skeletal system is, afterthe urinary tract, the second system in the bodymost frequently affected by this disorder.1 Hipdysplasia, missing extremities or club-feet arefrequent problems with the limbs. Atrial andventricular septum defects are found in 10% ofthe cases, and Fallot tetralogies can also beobserved.1,10
A mixed nephropathy, partly obstructive andpartly dysplastic, affects the kidney, yet oftenwithout any obstruction at all. The kidney
pelvis calyx system is usually moderately dilat-ed. Renal insufficiency in these patients is pri-marily characterized by renal parenchymaldysplasia prompted by an early embryonalobstruction. Alternatively, renal insufficiencycan also develop as a result of a bladder dys-function with hyperperistalsis or the Prune-Belly syndrome’s characteristic dysergeniccontraction of the megacyst. Renal dysplasiacan only be diagnosed through histologicaltesting. A number of kidneys examined post-mortem showed dysplastic changes in themajority of the patients.1,11,12 Since thesechanges were often present only in segmentsof the kidney, biopsies of these organs couldlead to incorrect interpretation.
The wrinkled, drooping abdominal wall is asign of a different type of hypoplasia and dys-plasia of the abdominal wall muscles, first andforemost of a paraumbilical nature in the lower
Article
Table 2. Urological surgical procedures.
N. %
Urethral surgery 10 62.5Urethroplasty 1 6.3Internal urethrotomy 4 25.0Atrioventricular valve fulguration 2 12.6Epispadias correction 1 6.3Meatotomy 1 6.3Shincterotomy 1 6.3
Ureter surgery 7 43.8Cutaneous ureterostomy 1 6.3Ureterocystoneostomy 5 31.3Sober 1 6.3None 9 56.3
Testicular surgery 6 37.5Orchidopexy 5 31.3Inguinal orchiectomy 1 6.3None 10 62.5
Bladder surgery 10 62.5Hemicystectomy 5 31.3Hemicystectomy YV-plastic 1 6.3Young-dees bladder neck 1 6.3ReconstructionTUR bladder neck resection 2 12.6Cystostomy 1 6.3
Renal surgery 5 31.3Nephrectomy 4 25Pyeloplasty 1 6.3None 11 68.8
Suprapubic catheter 14 87.4Kidney transplant 4 25
Table 1. The clinicopathological character-istics.
N. %
SexMale 14 87.5Female 2 12.5
Age when diagnosedMinimum 1.2Median 9.3Maximum 12.9
Other congenital malformationsYes 5 31.2ASD, atrial septum defect 1 6.3Funnel chest (pectus excavatum) 1 6.3Spina bifida occulta 1 6.3Club-foot 1 6.3Funnel chest 1 6.3No 11 68.8
TreatmentSurgical 16 100Conserative 0 0
Congenital urologicalmalformationsAbdominal wall aplasia 15 93.8Cryptorchidism 11 68.8Malformations of the prostate 3 18.8Urethral malformations 8 50Mega-bladder 13 81.3Mega-ureter 14 87.5Renal dysplasia 3 18.8Hydronephrosis 9 56.3
Surgical proceduresUrethral surgery 10 62.5Bladder surgery 10 62.5Testicular surgery 6 37.5Renal surgery 5 31.2Ureter surgery 7 43.8Abdominoplasty 4 25
Post-surgical complicationsYes 2 12.5No 14 87.5

[page 80] [Pediatric Reports 2012; 4:e20]
half of the abdomen. The defect is attributed tothe first lumbar myotome. The coarse folds ofthe abdomen look like a dried prune.3 Anotherdistinct feature of this syndrome is cryp-torchidism. The reason for the undescendedtestes remains unknown. Mechanical factors,such as the greatly overextended bladder or thefaulty development of the inguinal canal,allegedly account for this.11,13,14 The crytorchidtestes have a favorable histology. Tissue in thetestes of PBS patients is no different from thatfound in intra-abdominal testes. The stem cellcount in the first year of age, in particular, iscomparable to that of normal testes.11,15
In most cases, bladder capacity is two to fourtimes larger, the detrusor muscle is thickenedand, in cases of an objective infravesicalobstruction, not trabeculated. The trigonum isenlarged in most cases, and has lateral andoften refluxing ostia and paraostial diverticula.The bladder neck is open. In other cases, thedeficient urodynamics are shown by the sheerpresence of a high volume of residual urine.Vesicoureteral reflux is found in 75% of ca -ses.1,3,8
The ureters are typically elongated, and therelated dilatation is mostly more pronouncedthan when there are only obstructive mega-ureters. Obstructive ureteral kinks exhibitingadditional stenoses and consecutive dilatationare often found. Peristalsis is underdevelopedand often inefficient. Histological analyses fre-quently confirm the existence of structural dis-turbances in the entire abdominal wall.3 Thealterations are typically more marked in thedistal section of the ureter than in the proxi-mal part.
Treatment of Prune-Belly syndrome is a sub-ject of controversy. In earlier times, due to thelack of experience with this very complex dis-order, a conservative strategy advocating sur-gery followed by a wait-and-see approach wasthe recommended line of action. The main goalof any treatment is, of course, preserving kid-ney function.3,11,15,16 Treatment options dependon the clinical picture. They can range frommaintaining a wait-and-see approach whileconducting regular urine checkups, to per-forming primary major corrective surgery andprocedures for temporary urine diversion,such as a cutaneous ureteroileostomy withsubsequent surgical reconstruction. However,as is well-known, reconstruction in the case ofnewborns makes no sense or is actually con-traindicated since at this age the bladder is notyet fully developed, thus increasing the risk ofobstruction after the uretero-cystoneostomyhas been performed. Greater stabilization ofthe upper urinary tract can be achieved inmany cases by performing procedures for moreprolonged drainage at the bladder level, prefer-ably a cystostomy.5,16 The timing of surgerymust be assessed on an individual basis anddetermined as part of the patient’s clinical
progress. These procedures can be consideredin cases of, for example, vesico-urethral refluxand/or obstructive uropathy, in which there isthe risk of further deterioration in renal func-tion. Some authors advocate performing a ure-throcystoscopy, if necessary, with urethrotomyin order to rule out an infravesical obstruction.
Abdominoplasty no longer plays the decisiverole in surgical therapy that was presumed informer times. Physical therapy can indeedachieve equally good or bad results.17-18 If nec-essary, tapering with reimplantation of the twodilated ureters should be performed, and bothcryptorchid testicles mobilized during theorchidopexy that takes place during abdominalwall surgery.12-19 Woodard, who has made a sig-nificant contribution in this field, advocatesinfravesical desobstruction wherever one mayoccur, excision of the surplus parts of bothmega-ureters, modeling, antirefluxing neosto-my in the bladder, and, likewise, excision of thediverticular upper half of the bladder.Orchidopexy completes this extensive majorsurgery. However, although this treatment,known as total reconstruction, has been broad-ly accepted, it is a very aggressive procedureand requires a great deal of surgical experiencein pediatric urology. In fact, this approach hasnow been abandoned, even by Woodard him-self, due to the high morbidity and mortalityrate in infants undergoing total reconstruction.
Little is known about which children withPBS can benefit from extensive reconstructiveprocedures. Some authors advocate a purelyconservative approach, given that the morphol-ogy and function of the urinary tract, as well asthe abdominal wall malformations, mayimprove with age. Many pediatric urologistswould agree that PBS represents a low pres-sure, dialated, non-obstructed system that inmany cases does not require surgery. Thispoint needs to be stressed; we have movedfrom aggressive surgery to medical manage-ment for many of these children. Of course,some children will need surgery for obstruc-tion, but this is becoming less common than inthe past. Many studies confirm that treatmentfor PBS should be tailored individually. A majorstudy in Brazil has confirmed that various uro-logically invasive procedures performed in 32children with PBS achieved good long-termresults.20-21 Renal transplants also secure goodresults in terms of function, as reported in aJapanese study of children with PBS.22
Conclusions
Our experience has shown that, with asound diagnosis and depending on the clinicalprogress, adequate, effective treatment can beoffered even in cases of serious and complexmalformations, such as Prune-Belly syndrome.
If the disorder follows a progressive course, anaggressive surgical approach has proven to beclearly more effective than a nihilistic treat-ment path or a wait-and-see strategy.Treatment, however, has to be tailored individ-ually and specific indications for surgeryassessed accordingly.
In the light of the comparatively sparse liter-ature available and of the great diversity of phe-notypes these malformations have, it is notpossible to determine with certainty whetherthe surgical procedures adopted do indeed havea decisive impact on the long-term outcome ofthese children in terms of renal prognosis or,for that matter, quoad vitam prognosis.
References
1. Duckett JW, Snow BW. Prune-Belly-Syndrom. In: R Hohenfellner, JW Thüroff,H Schulte-Wissermann (eds.)Kinderurologie in Klinik und Praxis,Stuttgart, 1986, pp 348-65.
2. Shah D, Sharma S, Faridi MM, Mishra K.VACTERL association with Prune-Bellysyndrome. Indian Pediatr 2004;41:845-7.
3. Schott G, Herrlinger A, Willital G. Theprune-belly syndrome. Urologe A 1982;21:322-6.
4. Van Ahlen H, Brühl P. Current views ofprune belly syndrome Urologe A 1988;27:207-13.
5. Harley LM, Chen Y, Rattner WH. Prunebelly syndrome. J Urol 1972;108:174-6.
6. Greskovich FJ 3rd, Nyberg LM Jr. Theprune belly syndrome: a review of its etiol-ogy, defects, treatment and prognosis. JUrol 1988;140:707-12.
7. Woods AG, Brandon DH. Prune belly syn-drome. A focused physical assessment.Adv Neonatal Care 2007;7:132-43
8. Sigel A, Schrott KM. Congenital megau-reter and its implications Urologe A1982;21:312-7
9. Crompton CH, MacLusky IB, Geary DF.Respiratory function in the prune-bellysyndrome. Arch Dis Child 1993;68:505-6.
10. Adebonojo FO. Dysplasia of the anteriorabdominal musculature with multiplecongenital anomalies. Prune belly or triadsyndrome. J Natl Med Assoc 1991;265:1179.
11. Kamel MH, Thomas AA, Al-Mufarrej FM, etal. Deceased-donor kidney transplantationin prune belly syndrome. Urology 2007;69:666-9.
12. Patil KK, Duffy PG, Woodhouse CR,Ransley PG. Long-term outcome of Fowler-Stephens orchiopexy in boys with prune-belly syndrome. J Urol 2004;171:1666-9.
13. Docimo SG, Moore RG, Kavoussi LR.Laparoscopic orchidopexy in the prune
Article

[Pediatric Reports 2012; 4:e20] [page 81]
belly syndrome: a case report and reviewof the literature. Urology 1995;154:1513-5.
14. Hutson JM, Beasley SW. Embryologicalcontroversies in testicular descent. SeminUrol 1988;6:68-73
15. Woodard JR, Parrott TS. Orchiopexy in theprune belly syndrome Br J Urol 1978;50:348-51.
16. Grapin-Dagorno C, Boubnova J, Ulinski T,et al. (2007) Renal transplantation in chil-dren with lower urinary tract dysfunctionBull Acad Natl Med 2007;191:569-81
17. Levine E, Taub PJ, Franco I. Laparoscopic-assisted abdominal wall reconstruction inprune-belly syndrome. Ann Plast Surg2007;58:162-5.
18. Monfort G, Guys JM, Bocciardi A, et al. Anovel technique for reconstruction of theabdominal wall in the prune belly syn-drome. J Urol 1991;146:639-40.
19. Bogart MM, Arnold HE, Greer KE. Prune-belly syndrome in two children and reviewof the literature. Pediatr Dermatol 2006;23:342-5
20. Dénes FT, Arap MA, Giron AM, et al.Comprehensive surgical treatment ofprune belly syndrome: 17 years' experi-ence with 32 patients. Urology 2004;64:789-93
21. Diao B, Diallo Y, Fall PA, et al. Prune Bellysyndrome: epidemiologic, clinic and ther-apeutic aspects. Prog Urol 2008;18:470-4.
22. Fusaro F, Zanon GF, Ferreli AM, et al.Renal transplantation in prune-belly syn-drome. Transpl Int 2004;17:549-52.
Article