Embed Size (px)
Citation preview
![Page 1: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/1.jpg)
74 THE INDIAN MEDICAL GAZETTE [Feb., 1938
THE RADIOLOGICAL EXAMINATION OF THE STOMACH AND DUODENUM
By G. GALSTAUN, m.a., d.m.r.e. (Cantab.), m.r.c.s.,
L.R.C.P. (Lond.)
Professor of Radiology, Medical College Hospitals, Calcutta
This short outline is intended as a guide to the general practitioner. Radiology has in the past few years played an increasingly important part in the diagnosis of gastric and duodenal conditions. With, improvements in apparatus the radiologist is now able to produce more and more accurate results. The reason of this is twofold. Firstly, with ample power now avail- able in modern diagnostic units, exposures are reduced to speeds of the order of one-tenth of a second or even less than half of this. Secondly, by reason of methods of graduated and controlled compression, together with a device for radio-
graphing appearances, the moment they are seen on the fluoroscope, much greater accuracy is attained. By means of these methods we are
frequently able to demonstrate ulcer craters and other anomalies, which would otherwise be com- pletely missed. Case 1 is an example where by using an
ordinary technique without compression the
appearances of the stomach and duodenum were found to be fairly normal, whereas with the serial duodenal device, with controlled compres- sion, a very distinct saccular structure was seen arising from the proximal portion of the second part of the duodenum. It. was suggested that this might be a diverticulum, which was in fact found at operation. This is only one of many examples. In other instances, by this method I have been able to demonstrate very definite ulcers of which I saw no trace in the routine
skiagrams of the stomach. The rationale of any opaque meal examina-
tion consists of a delineation of :? 1. Outline. 2. Mucosal pattern. 3. Living structure. The latter of course will be for the most part
seen in the fluoroscope.
It is important that, in order completely to
fill all crevices, the opaque meal be of a com- pletely homogeneous nature and held in proper suspension. It should not be gritty. Grit may cause spasm. Many preparations are 011 the
market, most of which fulfil these conditions.
They all consist of barium sulphate in a very fine state of division, held in suspension by either a gum or some other suitable material and variously flavoured, more often than not with chocolate.
Usually for an examination of the stomach and duodenum no purgation is necessary. Where the patient is constipated, however, it is advisable to give a mild purgative, such as two drachms of compound liquorice powder some
thirty-six hours before examination. It is essen- tial that the patient does not go to the radio-
logist in a starving state. A starved stomach is
usually in a state of spasm, rendering examina- tion of the mucosa difficult, if not impossible. In order to avoid this 1 always advise my patients to have a couple of slices of bread and butter or toast, and a cup of tea from two to three hours before coming to be examined. In certain cases where spasm is seen to be present this can be relieved by a small dose of bella- donna or an injection of atropine.
It is essential for the radiologist to be pro- vided with an accurate history of the case. It is to be remembered that radiology is merely one link in the chain of diagnosis, though usually in these cases a very important link. Such futilities, as sending a patient with a brief note ' A photo of the stomach', should be avoided. The first procedure in the x-ray examination
consists of a general survey. The lungs should always be screened. Many cases of dyspepsia can be traced to a phthisical origin. The
diaphragm should always be examined and any limitation in movement or fixation noted. It should be seen whether the liver is normal in size or enlarged. Such details as gas in the stomach or intestine should be observed. It
may be necessary in a stomach already full of secretion to empty this.
Having completed this general survey the
patient is given a small quantity of the barium emulsion. The stomach is then palpated with the gloved hand and the emulsion suitably splashed about the walls, held here and there as necessary so as to show as much as possible of the detail of the mucosa. Quite often an ulcer crater will be visualized in this way as a small residue with spider-like folds of mucous mem- brane converging on it. Such a residue will usually be found to be tender. Following this, films are taken with suitable compression by a
cone so as to show the mucosal pattern. After this a full pint of the barium emulsion
is given and the following features noted :? (a) The general contour of the stomach. (b) Tone. (c) Peristalsis.
![Page 2: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/2.jpg)
Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GALSTAUN 75
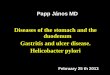
(From M. S. Stewart, Lancet, 11, 5G5, ami John Money, Lint. Med. J own.,
J3tli Nov., 1937.)
Diagrams showing the relative incidence of gastric ulcer and caicinoma.
|
15%
Ulcer. Carcinoma.
Diagrams showiDg the relative incidence of gastric ulcer and caicinonia.
Case 1.?Anterior erect. Case 1.?Anterior erect. The same case. Left antero-oblique. Erect.
The same case. Left antero-oblique. Erect.
The same case. Right antero-oblique. Erect.
The same case. Right antero-oblique. Erect.
(m
The same case. With compression. Erect. Anterior.
The same case. With compression. Erect. Anterior.
Erect. Left antero-oblique. Erect. Left antero-oblique.
![Page 3: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/3.jpg)
76 THE INDIAN MEDICAL GAZETTE "[Feb., 1938
(d) Mobility. (e) Rate of emptying. (/) Any tenderness. (g) Spasm. (h) The presence of any nicer niche or
irregularity. It is essential to examine the stomach in all
positions, not forgetting that, in certain stomachs, particularly those of the transverse type, in order to visualize the duodenal cap it will be
necessary to use the postero-oblique posture.
Having examined the stomach we next turn to the duodenal cap, which is examined in an
exactly similar manner. An examination done five hours after the
meal is always useful, as residues seen at this time are usually of some significance.
Types of stomach
It has been clearly understood for some years that the form taken by the stomach is largely a function of the subject's build or habitus. It
is extremely doubtful whether such a thing as a truly dropped stomach per se exists.
Mills in 1917 classified stomachs into three main groups :?
(a) Sthenic.?This, the normal J or ' fish
hook' type of stomach, is found in 70 per cent of cases.
(b) Hyposthenic.?A stomach of low tone
which does not grip its contents well and is
usually placed at a lower level than normally, often hanging down in the pelvis. This type of
stomach is as a rule found in long, lanky sub- jects, often poor eaters. A five-hours' residue in such a stomach is not uncommon and like the stomach itself is certainly not pathological.
(c) Hypersthenic.?This type of stomach is
usually of steer-horn shape, lying transversely across the abdomen, as textbooks of anatomy would have us believe the normal stomach does. It is found in subjects of broad and squat build- Tone is good. Peristalsis is increased, com-
pared with that of the sthenic type of stomach-
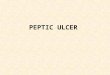
Case 2.?Au example of ' nichc and notchUlcer of the lesser curvature
and spasm.
Case 2.?An example of ' niche and notch Ulcer of the lesser curvature
and spasm.
The same case after three months after a course of Sippy diet and injections of Larostidin. Note the pointing of the ulcer crater and
absence of spasm.
The same case a fter three months after a course of Sippy diet and injections of Larostidin. Note the pointing of the ulcer crater and
absence of spasm.
Case 3.?A very large ulcer at the lower end of the lesser curvature.
Case 3.?A very large ulcer at the lower end of the lesser curvature.
The same case at five hours. The same case at five hours.
![Page 4: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/4.jpg)
Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77
Such stomachs have a relatively high acid con- tent and their owners have good appetites. More often than not in this type, in the antero-postero position, the duodenal cap usually lies behind the pylorus, giving a superimposed shadow. It can be well seen, however, with an oblique posi- tioning.
Internal structure The mucous membrane of the stomach is
thick and glandular. It is fixed along the lesser curvature and at the pylorus, being free elsewhere. The sub-mucoUs coat is lax allowing fairly free movement. The mucous membrane is thrown into multiple folds, small near the attachment at the lesser curvature, and more voluminous and deeper at the greater curvature.
At the lesser curvature is seen a hiatus in the oblique fibres of the musculature. This causes an irregular contraction forming in this situation a sort of canal?the '
Magenstrasse' of the Germans. No oxyntic cells are found here. It
*s in this locality that about 90 per cent of gas-
tric ulcers occur. , , u
The mucosal pattern of a normal stoinach
should flow in regular folds. Any marked nreg-
nlarities in these folds must be mqiur ?
In cases of ulcer they are usually s?en. , *
puckered up in a spider-like manner, the ) 1
?
the spider being the ulcer crater. \ anous '
of chronic gastritis produce coarsening anc
ularities of these folds.
Tone
The normal stomach should tend to giip its
contents and not bulge. Peptic ulcer is coi
nioner in hypo-tonic stomachs with low
contents. . .. j
A 'long' type of stomach has-been descri e
by Hurst in'which traction on the mesentery occurs. Radiological examination
in the&e Cc. .
does not show evidence of any inflamm< y
lesion and the pain associated with iem 1S'
one would expect, relieved by lyin? down.
Peristalsis The waves of peristalsis initiated at the cardia
flow towards the pylorus. At first slow and
shallow, they gather speed and depth as they reach the pylorus.
Peristalsis is not to be confused with tone. It has been shown within recent years by Graham, Cole, and other workers that peristalsis is a
function of the muscularis mucosa?, whereas tone is more the function of the muscular coats of the stomach.
Spasm (a) Cascade spasm.?The stomach- in these
cases assumes the form of a cup at the cardia from which the meal flows into the pars media. For this reason this type has been called the '
cup-spill' stomach. In most cases this appear- ance is undoubtedly of spasmodic origin and the spasm is relaxed by belladonna.
(b) Spastic incisura, or regional spasm.?This may be a reflex phenomenon or the result of an ulcer, usually in the opposite wall.
Fraenkel has described a series of cases of
very early ulceration in the lesser curvature
where, though no ulcer can be demonstrated
radiologically, there is definite spasm with lack
of peristalsis in a small section of the lesser
curvature.
Post-operative adhesions may cause either true 'spasm, or appearances simulating spasm in the stomach. It is sometimes a matter of diffi-
culty on radiographic appearances alone to
exclude malignancy in such cases. (c) Pyloro-spasm.?Spasm of the pylorus is
often caused by a pre-pyloric ulcer. It may, however, be found in some cases of duodenal ulcer and reflexly as the result of other abdom- inal inflammatory lesions. A. C. Jordan has described this condition as being often associated with other spasmodic conditions, such as cardio- spasm.
Emptying time The rate of emptying of the stomach depends
among other things on the nature of the food
/
Case 4.?Penetrating ulcer of the lesser curvature. The prone anterior position in which this skiagram was taken is often the best one to
demonstrate this type of ulcer.
Case 4.?Penetrating ulcer of the lesser curvature. The prone anterior position in which this skiagram was taken is often the best one to
demonstrate this type of ulcer.
Case 5.?Pyloric stenosis. Pre-pyloric ulcer crater demonstrated as a residue at five hours. Note the large stomach
retention.
Case 5.?Pyloric stenosis. Pre-pyloric ulcer crater demonstrated as a residue at five hours. Note the large stomach
retention.
![Page 5: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/5.jpg)
78 THE INDIAN MEDICAL GAZETTE [Feb., 1938
ingested. It is usually more rapid in the hyper- sthenic type of stomach. The stomach normally should be empty in five hours, but residues at six hours and more are not uncommon in hypo- tonia. This is not necessarily pathological. Where long retention is found in the stomach,
pyloric stenosis may ho suspected. In this con- dition it is extraordinary how long the stomach can retain its contents. There is a classic story of a patient at "St. Bartholomew's Hospital suffering from pyloric stenosis who one day vomited a large howl full of gastric contents. He stared for some time at the bowl and then exclaimed with some astonishment ' Ham ! Ham !! I ain't had ham for a fortnight !'
Hyper-secretion Hyper-secretion is easily seen on the fluores-
cent screen or skiagram by a less opaque fluid level lying over the dense barium emulsion.
Gastric ulcer
Russel Carman has estimated that 90 per cent of all gastric ulcers occur in the lesser curvature
between the cardiac orifice and the incisura
angularis. An ulcer crater may be seen on the fluoroscope
or skiagram either as a small niche or as a large diverticulum-like structure, sometimes with a
gas bubble 011 top. It may be seen as a large pyriform filling defect. The shape of the crater, if seen, will naturally correspond to the under- lying pathology. It must be borne in mind how- ever that owing to the heaping up of the mucous membrane around a gastric ulcer the size indi- cated in the skiagram is apt to be deceptive.
It has been mentioned before that gastric ulcers may be demonstrated by the spider-like converging folds of mucous membrane, showing in the mucosal pattern. A residue and tender- ness over the suspected crater are always of
significance. The fixation of the portion of the lesser curvature in very early ulcerative or pre- ulcerative states has already been mentioned. A characteristic feature very often seen in
association with an ulcer in the lesser curvature is spasm in the greater curvature opposite. In certain cases this spasm might involve almost the entire circumference of the stomach, pro- ducing a pseudo-hour-glass contraction. This, however, is not to be confused with the true
hour-glass stomach, which is the result of chronic, ulceration with cicatricial contraction. The true hour-glass contraction is always more marked in the lesser curvature, and has not the clearly-defined outlines of the pseudo-hour-glass contraction. Where an ulcer previously under observation
is seen* to lose its rounded appearance and become conical or pointed, healing is indicated.
In these cases, too, the spasm opposite is con-
siderably lessened or absent.
Pyloric ulcer or pre-pyloric ulcer This type of ulcer is usually difficult to
demonstrate. They are often shallow and not cup-like as those in the lesser curvature; as a
rule they cause pyloro-spasm, with stenosis,
<=> Case G.?Carcinoma of Ihe stomach involving Iho pylorus and most of
I ho aroator curvature.
Case G.?Carcinoma of iho stomach involving the pylorus and most of
ilio area tor curvature.
Case 7.?Duodenal ulcer. Note the deformed cap with folds of mucous membrane converging on a crater and gas bubble on top. The second
skiagram at five hours shows a residue in the crater.
Case 7.?Duodenal ulcer. Note the deformed cap with folds of mucous membrane converging on a crater and gas bubble on top. The second
skiagram at five hours shows a residue in the crater.
![Page 6: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/6.jpg)
Feb., 19381 RADIOLOGY OF STOMACH AND DUODENUM : GALSTAUN 79
which may be really due to cicatricial contrac- tion, or more often as the result of spasm.
It will be almost impossible to demonstrate a pre-pyloric ulcer with the stomach full of opaque meal. In these cases, one has to rely on indirect appearances and largely on the mucosal pattern. Indirect evidence is furnished by the spasm and the often dilated stomach, which is the result of
spasm or stenosis.
Gastric carcinoma The differential diagnosis between ulcer and
carcinoma of the stomach is very often impos- sible in the early stages of the latter by purely radiological methods. In these cases it is essen- tial carefully to consider the whole clinical pic- ture. Quite a few cases have been reported where what appeared at the first- examination to
lie a simple ulcer in the lesser curvature or pre- pyloric region has turned out 011 subsequent examination at a later period to be a cancer. The radiological signs of carcinoma of the
stomach consist of an irregular and constant
filling defect often having crescentic impressions such as those a thumb might make on putty. There is always a lack of peristalsis in the
affected area owing to the destruction of the
underlying muscularis mucosae. Where the growth is at the pylorus an irreg-
ular conical narrowing of the lumen will be
seen. In the ring type of carcinoma of the
pylorus, emptying of the stomach is rapid as
though the meal was passing through a rigid pipe. In these cases an associated ileus of the second part of the duodenum is seen in the
majority of cases. Where the growth is not
completely annular, 011 the contrary, spasm may be induced at the pylorus. The question of spasm in the stomach is
often
very confusing, in doubtful cases, alkalis and
belladonna or sometimes gentle palpation while screening will clarify things. The relative regional incidence of gastric ulcer and carcinoma
js seen in the accompanying diagrams. It will be seen that whereas the vast majority of gastric ulcers are situated in the lesser curvature, the seat of election of gastric carcinoma is in the
Pyloric region. In carcinoma of the cardiac end of the stomach, the chief clinical symptom
is dysphagia, due to stenosis at the cardiac orifice. Examination shows a filling defect at the cardia, sometimes invading the lower end of the oesophagus.
Diverticulum of the stomach These saccular excrescences are not very
common. They usually occur high up in the cardia. and have a smooth outline with no tenderness or associated spasm. They often remain filled for a considerable time.
Leather bottled stomach
This condition consists of a fibrous carcino- matosis. The stomach presents a rigid steer- horn appearance with an almost or absolutely complete lack of all peristalsis.
Gastric syphilis This is characterized by a contracted stomach
with thickened, hypertrophic*! and irregular folds of mucous membrane. Rigidity is usually present. There is no palpable tumour felt in
these cases. Often there may be an hour-glass deformity with no demonstrable ulcer crater.
Tuberculous disease of the stomach This is exceedingly rare. The radiographic
appearances are similar to those of syphilis.
Case 8.?Ulcer crater in the duodenal
cap.
Case 8.?Ulcer crater in the duodenal cap.
The same case at five hours. A very small stomach residue seen, and a
distinct residue in the ulcer crater.
The same case at, five hours. A very small stomach residue seen, and a
distinct residue in the ulcer crater.
Case 9.?Penetrating ulcer of the duodenum.
Case 9.?Penetrating ulcer of the duodenum.
![Page 7: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/7.jpg)
80 THE INDIAN MEDICAL GAZETTE [Feb., 1938
Polyposis These growths show in the skiagram as irreg-
ular rounded filling defects, usually with a
smooth outline. In extensive cases the diagnosis from malignant disease may be difficult so far as radiographic appearances alone are concerned.
Foreign bodies
Many types of foreign body may be found in the stomach. One sometimes causing a good deal of trouble in diagnosis is a hair ball. I have
on more than one occasion found a Rvle's tube
retained in the stomach.
D in p lira gmat. ic hern i a
As a rule this usually presents no difficulty in diagnosis. Prior to the giving of the opaque meal probably a large irregular collection of air will be visualized in the \thorax. On giving the
opaque emulsion it will be seen that the stomach or even more has herniated through the dia-
phragm into the thoracic cavity.
The duodenum
The first part of the duodenum, immediately beyond the pyloric ring, is seen in opaque meal examinations as a cap-shaped structure, rather like a monk's hood. Hence the term ' duodenal
cap'. Morphologically this is a part of the stomach. Ninety per cent of all duodenal ulcers occur here. The second part of the duodenum points vertically downwards curving over the liead of the pancreas to reach the third part which proceeds to the left to its continuity with the jejunum.
Filling defects Filling defects of the duodenal cap may be, as
anywhere else in the gastro-intestinal tract, the result of extrinsic or intrinsic causes.
Very often a crescentic filling defect is seen on the cap or pyloric portion of the stomach, due to pressure of the gall bladder. Often owing to deficient tone the duodenal cap is enlarged and on emptying two pouches at the base remain filled with the opaque material.
Duodenal ulcer
The only really direct sign of a duodenal ulcer consists of visualizing the ulcer niche or
crater.
Many indirect signs are of considerable value, such as :?
(1) Cicatricial contraction causing either by itself or by associated spasm a contraction in the centre of the cap, sometimes known as a ' kinuta ' or mallet-like contraction.
(2) '
Fleeting' filling of the duodenum
together with other signs of irritability.
(3) Hyper-secretion. (4) Pyloro-spasm, unaccounted for otherwise. (5) Tenderness over the cap. (6) Residues in the stomach at five hours. As in the stomach, many types of ulcer are
seen in the duodenum ranging from the flat
type of superficial ulceration following duoden- itis to deep penetrating ulcers.
Duodenitis
In this very common condition, often pro- liferative, a coarse reticulation is seen in the mucosal pattern, often associated with spasm. In many cases the cap appears contracted owing to engorgement of the mucous membrane. Tenderness is usually present. In many cases a
bubble of gas is seen at the apex of the cap in
cases of duodenitis and duodenal ulcer. Wilkie and others have pointed out what is now a com- monplace, viz, the very constant association of duodenitis with chronic appendicitis and chole-
cystitis. (Continued, at foot of opposite page)
J
M
1: Case 10.?Penetrating ulcer of the duodenal cap. Right antero-oblique
position.
Case 10.?Penetrating nicer of the duodenal cap. Right antero-obliqne
position.
Case 11.?Double penetrating ulcer at the base of the cap.
Case 11.?Double penetrating ulcer at the base of the cap.
![Page 8: The Radiological Examination of the Stomach and …...Feb., 1938] RADIOLOGY OF STOMACH AND DUODENUM : GAL8TAUN 77 Such stomachs have a relatively high acid con- tent and their owners](https://reader033.pdfslide.net/reader033/viewer/2022060308/5f09f94a7e708231d429668d/html5/thumbnails/8.jpg)
(Continued from previous pacje)
Diverticulum of the duodenum ? This when present usually occurs in the second part. It is very rarely found in the first part and occasionally in the third. These sacs are
not merely a herniation of the mucosa through weak spots in the musculature. They are prob- ably true congenital sacs and are covered by all the muscle coats of the duodenum. In the second part of the duodenum, divert-
icula; usually retain their meal for long periods often for twenty-four hours or longer.
Gastro-jejunostomy appearances AH cases of gastro-jejunostomy should be
examined as soon after operation as they are
able to get about, in order to ascertain the effi-
ciency or otherwise of the operation. It will be found in the vast majority of cases
ttiat the patient has not changed his habits and that as much meal as a rule will take the old route as the new unless something has been done to obliterate the old canal. Usually in three
weeks or so, valvular action will have been estab-
lished at the stoma.
Jejunal ulcer In 2 per cent of cases of gastro-jejunostomy,
jejunal ulcer occurs, usually within nine months ?f operation. Pain is felt soon after meals, rather lower down than in peptic ulcer and as a rule more to the left. Sometimes an ulcer crater can be demonstrated
by #-ray examination, more often not. The
disturbance of the normal relationships, together with post-operative adhesions, makes diagnosis m these cases very difficult. Indirect signs of
value are :? (1) Spasm and closure of the stoma. ^2) Hyper-secretion. (3) Persistent irregularity about the stoma. ^4) Tenderness. (5) Persistent stomach residues. The method of mucosal examination by con-
trolled pressure is of the greatest importance j here.