Embed Size (px)
Citation preview

Br. J. Surg. Vol. 62 (1975) 356-359
The relationship of anaemia to gastric secretion more than 15 years after vagotomy and gastro-enterostomy E . J . W H E L D O N , C. W. VENABLES A N D IVAN D. A. JOHNSTON*
SUMMARY Iron deficiency anaemia is common following vagotomy and gastro-enterostomy, and this study has shown that all the anaemic patients had low gastric secretion.
After correction of their anaemia, gastric secretion was increased, but was still very low, and when these levels were compared with secretion in f i t non-anaemic patients it was found that the latter group had a significantly higher secretion, and that a high proportion of them showed evidence of incomplete vagotomy.
These results suggest that there is a relationship between the levels of gastric secretion in patients afier vagotomy and gastro-enterostomy and the development of anaemia. It may be that inadequate gastric secretion impairs the release of efemental iron from the diet and its subsequent absorption.
PARrIAL gastrectomy, whether Polya or Billroth I, is known to be associated with a high incidence of anaemia developing a number of years after operation. This anaemia has been shown to be mainly due to iron deficiency (Hobbs, 1961). The incidence of anaemia varies widely (from 10 to 80 per cent) in different series, and Deller et al. (1962) calculated an average of 28 per cent from 33 reports. Macrocytic anaemia was reported by these workers in only 1.5 per cent of patients, but Jones et al. (1962) reported an incidence of 16 per cent. A study carried out by Mollin and Hines in 1964 found serum vitamin Rlz and folk acid deficiencies in more than 25 per cent of their patients.
There has been a great deal of investigation into the possible causes of the iron deficiency anaemia following partial gastrectomy. Little evidence has been produced to indicate that these patients take an inadequate amount of iron in their diets. It would seem possible, therefore, that the anaemia might be caused by impaired absorption. It has been suggested by Stevens et al. (1959) that patients after partial gastrectomy are unable to increase dietary iron absorption in the presence of iron deficiency anaemia, whereas iron deficient patients who have not had gastric surgery are able to do so. Other workers have shown that absorntion of both ferrous and ferric salts in anaemic patients after gastrectomy is as good as in anaemic patients who have not undergone surgery (Baird and Wilson, 1959). It would appear that postgastrectomy patients might have a limited ability to break down the protein complex of dietary iron, and it has been suggested that gastric secretion facilitates this break- down (Goldberg et al., 1963; Jacobs et al., 1966).
All this work was carried out on patients following partial gastrectomy, and it was felt that loss of the gastric reservoir and glandular tissue might be responsible for the development of nutritional disturbances. It was hoped that with vagotomy and drainage these problems would not arise. Unfortun- ately, several workers have shown that a similar incidence of anaemia occurs following this operation (Burge and Pick, 1958; Cox et al., 1964).
A recent study of 230 patients who had undergone vagotomy and gastro-enterostomy more than 15 years previously (Wheldon et al., 1970) showed that this operation was associated with a high incidence of iron deficiency anaemia (30 per cent). There was no evidence of macrocytosis in any of the patients, and serum vitamin Blz levels were all within the normal range. When these patients were reviewed at 10 years after surgery (Feggetter and Pringle, 1963), the incidence of iron deficiency anaemia was 10 per cent. Anaemia after vagotomy and drainage develops later and is less severe than that recorded after gastrectomy (Jones et al., 1962).
It would appear that alteration in gastric secretion might play an important role in the development of iron deficiency anaemia, and a study was designed to investigate this.
Table I: DETAILS OF THE TWO GROUPS IN THE PRESENT STUDY
Anaemic Non-anaemic
( n = 12) (n= 11) group group
Age (yr) 5 5 . 8 1 8.4 55.6f5.9 Weight (kg) 60.2 5 10.3 68,5+6.2 Haemoglobin (silo0 ml) 8.5* 1.1 14.6k0.6 Time since vagotomy (yr) 17.1 1 1.6 17.5 f 1.7 Length of history before 8.2f 6.5 6.8 f 3.0
vaeotomv fvr) All results given as mean +s.d.
Patients and methods Twenty-three patients were investigated (Table I ) . Twelve had haemoglobin levels below 10 g/lOO ml (70 per cent) at the time of their review and their mean level was 8.4g/100ml (58.9 per cent). There was no obvious cause of anaemia in these patients, e.g. haemorrhoids, positive occult blood or any obvious disease associated with anaemia. A dietician calculated the mean daily iron intake of each patient,
* Department of Surgery, University of Newcastle upon Tync, Royal Victoria Infirmary, Newcastle upon Tyne.
356

Anaemia after vagotomy and gastro-enterostomy
400
350 E
,z 300
Y $ 250-
- .c
- Vl m
a M
- i 2oo- - 5 150- a 3
v
; loo- t
a ._ w
2 50-
and all the patients took more than the minimum daily requirement of 10 mg, the mean being 16.1 mg.
The remaining I 1 patients were selected because at the time of their review they were completely well and had normal haemoglobin levels (mean value 14.6 g/ 100ml). The two groups were comparable for age, length of history before operation and length of
There was a difference in the mean weights of the two groups: 68.5 kg in the non-anaemic patients and 60.2 kg in the anaemic patients. This was partly explained by the fact that there were 2 women in the anaemic group, and there were no women of com- parable status in the non-anaemic group. The actual weights of the patients in this study were compared with their standard weights calculated from their age, sex and height (Kemsley et al., 1962). There was no significant difference between their actual and standard weights in the two groups. There was no alteration in the weights of the anaemic patients after correction of their anaemia. Haemoglobin was estimated by the cyanmethaemoglobin method, and serum iron by AutoAnalyzer.
The acid and pepsin secretory response to penta- gastrin (6.0 pg/kg hi.) and to insulin (0.2 u./kg i.v.) was assessed in all the patients either by separate tests or by a combined pentagastrin/insulin test (Venables, 1972). Gastric secretion was collected by a ‘washout’ technique in all but one patient ; this technique allowed an estimate of uncollected secretion to be made. Acid was measured as total titratable acidity to pH 7.0 using an automatic titrimeter (Radiometer), and pepsin was measured as total peptic activity at pH 2.1 using a modification of Hunt’s (1948) technique with albumin (Fr. V) as substrate and expressing results as equivalent to the peptic activity produced by a known amount of crystalline pepsin (Sigma 1 : 60000). The outputs of acid and pepsin were calculated for the hour after pentagastrin stimulation and the peak 30-minute output after insulin.
As it could be argued that any secretory changes found were due to the presence of anaemia (Stone, 1968), the anaemia was corrected by the administration of oral ferrous gluconate 200 mg three times daily. At the end of 3 months’ treatment the mean haemo- globin had risen from 58.9 to 95.3 per cent, and the serum iron from 31.5 pg/lOO ml to 96.8 pg/lOO ml. Repeat pentagastrin tests were carried out at this time.
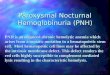
Results Estimation of acid and pepsin secretion before correction of the anaemia (Fig. I ) revealed that only 2 patients had acid outputs of more than 1 mEq/h and the mean output was only 0.6 mEq/h. Pepsin output was also markedly reduced, as 3 patients had no measurable pepsin response and the highest output was only 23.4 mg/h with a mean of 8.2 mg/h.
Three months later, after correction of the anaemia, there was a significant increase in the gastric secretion (P<O.O1). All but 2 patients had an increase in both acid and pepsin output. Six patients now had acid outputs of more than 1 mEq/h, but the mean response
follow-up.
-
-
-
a
Before After treatment treatment
80
- L M 70 E
5 60
- c
VI m M
50 a M
40 0 - - P
30 a Y
$ 20 - w a d 10
Before
h . r
LU IT
E - 30 5
$ 25
v
Y c W
:20-
8
4 ’ 0 -
c ._
= 15- P Y 3
0
a
a
e
.fter
-
-
treatment treatment
Fig. 1. Effects of correction of anaemia on gastric secretion. Acid output, P<OO1 (u. = 25.5). Pepsin output, P<:O.OOl
Anaemic Non-anaemic Anaemic after after treatment treatment
0
a
Ion-anaemic
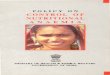
Fig. 2. Comparison of the gastric secretion of anaemic and non-anaemic patients. Acld output, Pt0.001 (u. = 9.5). Pepsin output, PiO.001 (u. = 14).
was still low at only 1.55 mEq/h. Pepsin output showed a threefold rise from a mean of 8.2 to 27.3
The results obtained after correction of the anaemia were compared with those obtained in our non- anaemic group (Fig. 2). Only 3 of the non-anaemic patients showed acid outputs similar to those of the anaemic group and one of these had not had a ‘washout’ pentagastrin test so that the secretory response was probably an underestimate. The mean acid output in the non-anaemic group was 9.2 mEq/h and the pepsin output was 119.3 mg/h. These differ- ences are highly significant ( P < 0.001).
mg/h.
26 357

E. J. Wheldon et al.
Table 11: ASSESSMENT OF COMPLETENESS OF VAGOTOMY IN THE NON-ANAEMIC PATIENTS
Test No. of patients
Hollander >20 mEq/l (positive) <:20 mEq/l (negative)
Insulin: pentagastrin acid ratio ; 45% <45%
9 2
4 I
An attempt was made to assess the completeness of vagotomy in all the patients studied. This was done in two ways: either by the rise in acid concentration of more than 20 mEq/l after insulin stimulation (Hollander, 1946) or by an acid ratio of more than 45 per cent, calculated from the acid output response to insulin and pentagastrin (Venables, 1972). In the anaemic patients it was difficult to assess the complete- ness of vagotomy by either technique, as the acid out- puts were so low. It was not possible, therefore, to say with certainty whether this low response was due to complete vagal section or to loss of secretory cells. Of the non-anaemic group (Table if), 9 showed a rise in acid concentration of more than 20 mEq/l, thus fulfilling Hollander’s criteria for incomplete vagotomy, and 4 of these had acid ratios of more than 45 per cent, suggesting that the vagotomy was definitely incomplete.
Discussion In our earlier study of patients who had undergone vagotomy and gastro-enterostomy more than 15 years previously (Wheldon et al., 1970) it was shown that iron deficiency anaemia was almost as common as that reported after gastrectomy. This was disappoint- ing as it had been hoped thatpreservation of the gastric reservoir function of the stomach would prevent this complication.
One possible cause for this anaemia was a reduced iron intake, but dietary analysis failed to demonstrate this, supporting the findings of others (Pulvertaft and Cox, 1969).
Another mechanism could have been the bypassing of the duodenum in these patients, as Wallenskin (1958) suggested that this would reduce absorption from the duodenum and proximal jejunum. However, all our anaemic patients responded rapidly to oral ferrous gluconate, suggesting that this was not true for elemental iron.
Jacobs et al. (1966) have demonstrated that gastric secretion facilitates iron absorption. As dietary iron is not normally in its elemental form but bound to protein as an iron-protein complex, it is possible that the anaemia could be related to an inability to split this complex due to an effect of the operation upon gastric secretion. The present study was designed to investigate this possibility.
Because it might be argued that any secretory changes we found in our anaemic patients were due to the anaemia and not the cause of it, we repeated our secretory tests following correction of the iron
deficiency and were able to confirm the findings of Stone (1968) that secretion of both acid and pepsin rose significantly after correction of the anaemia. However, even this increased secretory response was far lower than that found in our non-anaemic group.
Goldberg et al. (1963) suggested that ‘acid’ alone facilitated iron absorption, but Hines et al. (1967) felt that pepsin secretion was more important as this was capable of splitting the food iron-protein complex when activated by a fall in pH. Koepke and Stewart (1964) suggested that there was a factor present in gastric juice, similar to intrinsic factor, that enhanced iron absorption.
Whichever of the above possibilities is correct, it is likely that vagotomy will alter their roles as it results in a reduction of all gastric juice constituents.
Another possible cause for the reduction in gastric secretion found in our anaemic patients has been suggested by Williams (1964). He has postulated that the duodenal and bile juice reflux associated with a gastro-enterostomy may result in chronic gastritis, glandular atrophy and subsequent hyposecretion. Such a suggestion would explain why anaemia is less common after pyloroplasty where reflux is less (Wastell, 1969). It is of interest to note how many of our non-anaemic group had evidence of residual vagal function on insulin testing. This capacity to secrete acid may have protected the stomach from the effects of the reflux of alkaline secretion, and this in turn may have prevented mucosal atrophy.
Finally, it could be suggested that the increased rate of gastric emptying found after vagotomy and drainage (Owren, 1953 ; McKelvey, 1970) prevented the adequate mixing of gastric juice and food, reducing the liberation of elemental iron from the food while it was in contact with the iron-absorbing area of the small intestine. Incomplete vagotomy, even though it maintains a higher level of gastric secretion, cannot be the only factor. as several non- anaemic patients had no evidence of residual vagal function after insulin stimulation.
Acknowledgements We wish to thank Professor A. L. Latner and the Department of Clinical Biochemistry, University of Newcastle upon Tyne, for their assistance with this study, Staff Nurse M. Curd for performing many of the secretory studies, Mrs M. Foster for her secre- tarial assistance and the members of the Department of Surgery for their assistance throughout the study.
References BAIRD I. MCL. and WILSON G. M. ( 1 959) The pathogenesis
of anaemia after partial gastrectomy. Q. J . Med. 28, 21-41.
BURGE H. and PICK E. J. (1959) Long term results of vagotomy and gastroenterostomy in chronic duodenal ulceration. BY. Med. J. 1, 613-615.
cox A. G., BOND M. R. , PODMORE D. A. and ROSE D. P. (1964) Aspects of nutrition after vagotomy and gastrojejunostomy. BY. Med. J. 1, 465-469.
358

Anaemia after vagotomy and gastro-enterostomy
DELLER D. J., RICHARDS w. c. D. and WITTS L. J. (1962) Changes in the blood after partial gastrectomy with special reference to vitamin BIZ. Q. J. Med.
FEGGETTER G. Y. and PRINGLE R. (1963) Long-term results of bilateral vagotomy and gastrojejuno- stomy for chronic duodenal ulcer. Surg. Gynecol. Obstet. 116, 175-179.
GOLDBERG A., LOCHEAD A. c. and DAGG J. H. (1963) Histamine-fast achlorhydria and iron absorption. Lancet 1, 848-850.
HINES J. D., HOFFBRAND A. v. and MOLLIN D. L. (1967) The hematologic complications following partial gastrectomy. Am. J. Med. 43, 555-569.
HOBBS J. R. (1961) Iron deficiency after partial gastrec- tomy. Gut 2, 141-149.
HOLLANDER F. (1946) The insulin test for presence of intact nerve fibres after vagal operations for peptic ulcer. Gastroenterology 7, 607-614.
HUNT J. N. (1948) A method of estimating peptic activity in gastric contents. J. Biochem. 42, 104- 109.
JACOBS A., RHODES J., PETERS D. K., CAMPBELL H. and ESKINS J. D. (1966) Gastric acidity and iron absorption. Br. J. Haematol. 12, 728-736.
COOKE w. T. and STAMMERS F. A. R. (1962) Peptic ulceration. Some haematological and metabolic consequencesof gastricsurgery. Lancet 2,425428.
KEMSLEY W. F. F., BlLLEWICZ W. Z. and THOMSON A. M. (1962). A new weight-for-height standard based on British anthropometric data. Br. J. Prev. SOC. Med. 16, 189-195.
KOEPKE J. A. and STEWART w. B. (1964) Role of gastric secretion in iron absorption. Proc. SOC. Exp. Biol. Med. 115, 927-929.
31, 89-102.
JONES C. T., WILLIAMS J. A., COX E. V., MEYNELL M. J.,
MCKELVEY s. T. D. (1970) Gastric incontinence and post-vagotomy diarrhoea. Br. J. Surg. 57,74 1-747.
MOLLIN D. L. and HINES J. D. (1964) Observations on the nature and pathogenesis of anaemia following partial gastrectomy. Proc. R. SOC. Med. 57, 575- 580.
OWREN P. A. (1953) The pathogenesis and treatment of iron deficiency anaemia after partial gastrec- tomy. Acta Chir. Scand. 104, 206-214.
PULVERTAFT c. N. and cox A. G. (1969) Effects of vagotomy on haemopoiesis. In: WILLIAMS A. J. and cox A. G. (ed.) After Vagotomy. London, Butterworths, pp. 150-156.
L. M. and FINCH c. A. (1959) Iron metabolism in patients after partial gastrectomy. Ann. Swg.
STONE J. R. (1968) Gastric secretory response to iron therapy. Gut 9, 99-105.
VENABLES c. w. (1972) An assessment of the value of measuring uncollected gastric secretion during routine secretion studies in man. Br. J . Surg. 59, 473477.
WALLENSTEIN s. (1958) Iron absorption after Bilroth I and I1 partial gastrectomy. Acta Chir. Scand.
WASTELL c . (1969) Long-term clinical and metabolic effects of vagotomy with either gastrojejunostomy or pyloroplasty. Ann. R. Coll. Surg. Engl. 45,193- 21 1
WHELDON E. J., VENABLES c. w. and JOHNSTON I. D. A. (1970) Late metabolic sequelae of vagotomy and gastroenterostomy. Lancet 1, 437-440,
WILLIAMS J. A. (1964). Effects of upper gastro-intestinal surgery on blood formation and bone metabolism. Br. J. Surg. 51, 125-135.
STEVENS M. D., PIRZIO-BIROLI G., HARKINS H. N., NYHUS
149, 534-538.
115, 270-275.
359