Embed Size (px)
Citation preview

Thoracic Surgery
The Society for Cardiothoracic Surgery in Great Britain & Ireland
FirstNational Thoracic Surgery Activity & Outcomes Report
2008
Prepared by
Richard Page ChM FRCS (CTh)
Bruce Keogh KBE, MD, FRCS, FRCP
on behalf of the Society for Cardiothoracic Surgery in Great Britain & Ireland
Robin Kinsman BSc PhD
Dendrite Clinical Systems


The Society for Cardiothoracic Surgery in Great Britain & Ireland
FirstNational Thoracic Surgery
Activity & Outcomes Report
2008
Prepared by
Richard Page ChM FRCS (CTh)
Bruce Keogh KBE MD FRCS FRCP
Society for Cardiothoracic Surgery in Great Britain & Ireland
Prepared by
Robin Kinsman BSc PhD
Dendrite Clinical Systems

�
The Society for Cardiothoracic Surgery in Great Britain & Ireland gratefully acknowledge the assistance of Dendrite Clinical Systems for
• data presentation and
• publishing this report.
Dendrite Clinical Systems Ltd is registered under the Data Protection Act; Data Protection Act Registration Register Number Z98 44 379
This document is proprietary information that is protected by copyright. All rights reserved. No part of this document may be photocopied, stored in a retrieval system, transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the permission of the publishers and without prior written consent from the Society for Cardiothoracic Surgery in Great Britain & Ireland c/o The Royal College of Surgeons, 35 / 43 Lincoln's Inn Fields, London, WC�A 3PN.
VERITY is a national venous thromboembolism registry provided as a service to medicine by sanofi-aventis.
Windows and Excel are registered trademarks of the Microsoft Corporation.
Crystal Reports is a registered trademark of Business Objects.
InDesign CS� is a registered trademark of Adobe Systems Inc.
January �008 A catalogue record for this book is available from the British Library.
ISBN 1-903968-�0-8
Published by Dendrite Clinical Systems Ltd
59A Bell Street, Henley-on-Thames, Oxfordshire RG9 �BA, United Kingdom
Phone: +44 1491 411 �88
Fax: +44 1491 411 377
E-mail: [email protected]
Printed &bound by
DENDRITECLINICAL SYSTEMS

PrefaceCardiothoracic surgeons primarily provide surgery for the heart, lung and oesophagus. We have a �5-year history of collecting activity and outcome data on the operations we perform but we have, frankly, not used the data to maximum utility. The international explosive growth in cardiac surgery coupled with events in Bristol encouraged us to take a robust and transparent approach with our cardiac surgical outcome data. This has led to a remarkable improvement in the understanding of factors influencing results and has enriched clinical audit and review in every unit in the United Kingdom.
Over the last few years we have grappled with how to do the same for thoracic surgery – surgery of the lungs and oesophagus. This report is the first step along this path. Thoracic surgery is more difficult because there are more diseases, more operative options and less clear endpoints, or measures of success. So, in this report we have simply looked at variations in activity and surgical approach between thoracic surgical units. Our early discussions were contentious in that there was concern that this publication would expose considerable and significant variations – and it has. My hypothesis is that this is good. Variation is good. Without variation in practice and outcomes there would be no progress. All science, whether molecular or clinical, exploits observation of variation to seek discovery and understanding. Variation in clinical practice is only an issue when those who observe a variation fail to adopt a neutral spirit of enquiry which seeks to establish which end of the spectrum represents better treatment for the sick. All too often we adopt a defensive approach which inhibits beneficial changes in clinical practice at one end and inhibits innovation through anxiety at the other.
This report highlights several differences in approach which reflect differing philosophical approaches to some difficult diseases. For example, on pages 46 and 63, one can see considerable differences in the open and close rate for lung and gastrointestinal cancer surgery between units. In other words, some patients are being subjected to exploratory operations to see whether anything can be done surgically. The open and close rate represents the proportion of patients who undergo an exploratory operation for whom nothing can be done. Some surgeons argue that these operations are avoidable by good pre-operative screening whilst others argue that these operations are for cancer and it is better to seek every chance rather than eliminate all hope prematurely. I hope the publication of this sort of information will stimulate debate not only on agreeing the very best screening investigations before surgery but also on the ethics and philosophy of these different approaches. This discussion will be enriched by opening the debate to the public.
There are other examples of variation which I hope will serve to stimulate debate and help us improve the quality of care we offer. But all should be seen within the context that on all the outcome measures presented in this report UK practice is of the highest international standard. The challenge is to continue to improve.
Bruce Keogh
KBE, MD, FRCS, FRCP

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
4
Intr
od
uct
ion
4
Introduction
Thoracic Surgery in the United Kingdom and Ireland
Thoracic surgery was initially developed in the early twentieth century to aid the treatment of suppurative chest diseases principally tuberculosis, bronchiectasis and empyema. Because of the particular needs of patients undergoing surgery within the chest, surgical activity gradually became concentrated in specialist hospitals serving a distinct geographical region. These Units, which came into existence in the middle part of the twentieth century, form the infrastructure for current cardiothoracic surgical services.
Following the development of antibiotics after the second world war the focus of thoracic surgical activity gradually moved away from suppurative chest disease to the management of intra-thoracic malignancies, principally lung and oesophageal cancer. With the widespread increase of cardiac surgical activity in the 1970s, thoracic surgical activity declined in many parts of the country and some diseases previously treated by thoracic surgeons were transferred to other surgical specialties.
More recently there has been a resurgence in thoracic surgery. The reasons for this are multi-factorial, but include the introduction of the NHS cancer plan in the UK, developments in the non-surgical treatment of ischaemic heart disease and changes occurring within cardiothoracic surgical practice as a whole. Traditionally all cardiothoracic surgeons were practitioners of all aspects of the speciality, a specialty encompassing the management of many varied diseases. In the early 1980s a cardiothoracic surgeon in addition to looking after patients with ischaemic heart disease and lung cancer, would also be expected (for example) to treat congenital cardiac defects, oesophageal cancer and chest wall abnormalities. As with many areas of medicine developments in the treatment of cardiothoracic conditions over the last quarter century has meant that it is impossible for a single surgeon to provide advice of a sufficiently expert nature to adequately treat all conditions within cardiothoracic surgical practice. Thus the speciality has developed to include surgeons who not only specialise in thoracic surgery alone but who have special expertise within the wider field of general thoracic surgery (e.g. oesophagogastric cancer, tracheal disease, and mesothelioma).
Currently around half of the patients seen by thoracic surgeons have proven or suspected primary lung cancer. As surgical resection is currently the best therapy for curing this disease much of the focus of thoracic surgical activity surrounds the selection and treatment of patients for resection of patients’ lung cancers. Although the surgical resection of a primary lung cancer is a major activity for all thoracic surgeons, a considerable time is spent aside from this work, not only in the clinics and multi-disciplinary lung cancer team meetings, but also in the operating theatre carrying out invasive surgical staging procedures necessary for lung cancer management (bronchoscopy, mediastinoscopy etc).
The other half of thoracic surgical time is spent on the remainder of general thoracic surgery. Each of the conditions treated has its own presentation, diagnostic pathway, work-up for surgery and choice of surgical procedures and non-surgical therapies available. Thus although thoracic surgeons are often thought of as lung cancer surgeons the reality is quite different. This diversity of practice makes for an interesting and stimulating specialty for surgeons to engage in throughout their lives.
Thoracic surgical data collection
Although less easily measurable than cardiac activity, the Society of Cardiothoracic Surgeons Thoracic Surgical Register was instituted soon after the Cardiac Surgical Register, the first reported year of activity being 1980. This initiative has been very well supported by Society members over the years, and always captured in the order of 95% of the total thoracic surgical activity occurring within the UK and Ireland. The Register has been available to members and although never published in a peer-review journal has been a useful source of reference to many groups with an interest in thoracic diseases.
The Register remained largely unchanged until �00� when the emphasis changed from a report based on pathological disease group to a summary of activity based on anatomical procedures. For example in the old Register (Appendix 1) there were ten different sites where the operation of pulmonary lobectomy could be entered, representing ten different underlying pathologies. Some of these diseases were so rare within overall thoracic surgical activity that they became of curiosity value only and did not justify the effort required for their recording. In addition there were undoubtedly inaccuracies in the collection of activity in these areas because of inconsistencies of definition between surgical Units. Nevertheless it is obviously important to capture overall activity, which is still a feature within the new Register (Appendix �). As always the only outcome measure remains in-hospital mortality. National activity only has been reported previously by the Society, although with this current report, Unit-specific activity is now available.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
5
Intro
du
ction
Between the years 1998 and �001, the Society asked for surgeon specific data returns relating to in-hospital mortality for pulmonary lobectomy for primary lung cancer. This operation was chosen as the marker for thoracic surgery as part of a wider initiative by the Society to try to standardise surgical performance for its members. However there has been a great deal of disagreement amongst clinicians as to whether this piece of data could be the used in the way it was intended. All cardiothoracic and thoracic surgeons have a high operative workload and yet may carry out comparatively few lobectomies for primary cancer. Comparisons of surgical performance are therefore flawed because of lack of numbers and the resulting very wide confidence limits when attempting to make a comparison of an individual surgeon’s results with a standard. Also there was a strong feeling that imposition of this standard by the Society would paradoxically result in poorer care for patients to ensure a surgeon’s figures could pass muster. An example of this is for the surgeon to carry out a limited resection or even a pneumonectomy in a patient at perceived high risk for surgery, when a lobectomy would be more appropriate. Also an in-hospital death after lobectomy is only rarely due to a technical error by a surgeon and is much more closely related to a patient’s pulmonary reserve prior to surgery, a factor outside the control of a surgeon. Thus principally in order to ensure that higher risk patients who could benefit from surgery were treated appropriately, the Society discontinued surgeon specific data collection for thoracic surgery.
The task of collecting the data for thoracic surgical returns to the Society has always been the responsibility of individual surgeons, with a lead surgeon in each Unit collating returns on behalf of each hospital. This has entailed a great deal of effort by many people and the Register is something that the Society and its members can rightly be proud of. Despite its limitations the Thoracic Surgical Register (along with its cardiac counterpart) has been at the vanguard of surgical data collection. Only recently have other surgical specialties turned their attention to this essential area of practice.
Guide to the report
As will be seen from the following pages the report is in two parts. The first is on overall national activity from the Register’s inception in 1980 to the end of March �005. The second section deals with Unit-specific activity for the three-year period from 1st April �00� to 31st March �005. In both sections the report is split into the following sections:
• Total activity with breakdown between open and minimally-invasive (VATS) surgery
• Lung resections with details on activity for primary lung cancer
• Pneumothorax surgery
• Oesophagogastric (upper GI) surgery with details on activity for primary oesophagogastric cancer
Limitations of the report
One of the major problems of data collection with regard to surgery is one of definitions. Even whether a post-operative death has occurred or not can be a subject for debate, for example whether the death occurs at base hospital, at another hospital where a patient has been transferred for convalescence or at home within (say) thirty days after the procedure. For the purposes of this report death after thoracic surgery (as after a cardiac operation) is defined as a death occurring at any time after primary surgery within the patient’s base hospital.
Another area which can be a problem is what constitutes major as opposed to minor thoracic surgery, a concern almost never an issue in cardiac surgery where all operations are major ones! Similarly there may be a doubt as to which category a particular operation should be assigned. A good example of this dilemma is the operation of pleuropneumonectomy for mesothelioma, which encompasses resection of pleura, lung, pericardium and diaphragm; a single entry into the category pneumonectomy for other lung conditions doesn’t seem to do justice to such a mammoth operation and can confound attempts to compare activity between Units. Minimally invasive or video-assisted thoracic surgery (VATS) is a variable feast; one surgeon’s definition of what constitutes VATS may be quite different to another’s. The Society relies on the common sense of individual surgeons when allocating operations to categories for the Register.
As will be seen the data contains no patient specific information such as age, pulmonary reserve or associated co-morbidity, all of which are known to be highly predictive of outcomes after thoracic surgery. Initiatives are already in place to include this type of data in future reports.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
6
Intr
od
uct
ion
Completeness of data collection
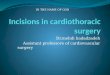
The Society can rightly be proud of the enthusiasm of surgeons in making returns from their Units for compilation of the Register; never has the number of returns from Units as a proportion of the total number of active Units fallen below 90%. The following chart illustrates the variation in this number.
Unfortunately a figure for the number of active Units in thoracic surgery is surprisingly difficult to pin down at any one time, even for such a small specialty as cardiothoracic surgery. In addition it is self evident that some patients are having surgery of a similar nature to that reported by thoracic surgeons, but under the care of a different specialty group. A good example of this is oesophageal surgery being carried out by non-thoracic surgeons such as general or ear-nose-and-throat surgeons. Several other specialty groups occasionally carry out surgery around or within the thoracic cavity, in the same way as thoracic surgeons occasionally operate outside its boundaries. There is nothing inherently wrong with this in terms of patient care although the result is a slightly skewed picture when trying to extrapolate the data contained within the Register, to activity within the United Kingdom and Ireland as a whole.
From the point of view of the Register the only activity that can be analysed is that which is sent in by surgeons working in thoracic surgical Units. The number of active thoracic surgical Units that do not send activity returns as in the preceding chart has necessarily been an estimate.
Richard Page
Thoracic Surgical Audit Lead
The Society for Cardiothoracic Surgery in Great Britain & Ireland
Returns submitted to the Register
0%
20%
40%
60%
80%
100%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f un
its
that
su
bm
itte
d r
etu
rns
to t
he
reg
iste
r
0%
20%
40%
60%
80%
100%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f un
its
that
su
bm
itte
d r
etu
rns
to t
he
reg
iste
r


The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
8
Tab
le o
f co
nte
nts
Preface 3
Introduction 4
Thoracic Surgery in the United Kingdom and Ireland 4
Thoracic surgical data collection 4
Guide to the report 5
Limitations of the report 5
Completeness of data collection 6
National activity
Total activity 12
Total surgical activity 12
Total major procedures 12
Open versus VATS procedures 13
Lung resections 14
Total lung resections 14
VATS as a proportion of all lung resections 14
Pathology for patients undergoing lung resections 15
Primary lung cancer 16
Resections for primary lung cancer 16
Type of resections for primary lung cancer 17
Open / close rates in primary lung cancer surgery 18
Mortality following surgery for primary lung cancer 19
VATS resections for primary lung cancer 21
Sleeve resections 23
Mediastinoscopy / mediastinotomy 24
Conditions other than primary lung cancer 25
Resections for other conditions 25
Surgery for pneumothorax 26
Total procedures for pneumothorax 26
Open versus VATS procedures 27
Mortality after procedures for pneumothorax 28
Surgery for upper GI disorders 29
Total activity for upper GI disorders 29
Minimally invasive resections 32
Operative mortality 32
Open / close rates in upper GI surgery 33
Contents

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
9
Table o
f con
tents
Unit-specific activity
Contributing Units 36
Organisation of the report 37
Total activity 38
Total surgical activity 38
Total major procedures 39
Open versus VATS procedures 40
Lung resections 41
Total lung resections 41
VATS as a proportion of all lung resections 42
Pathology for patients undergoing lung resections 43
Primary lung cancer 44
Resections for primary lung cancer 44
Type of resections for primary lung cancer 45
Open / close rates in primary lung cancer surgery 46
Mortality following surgery for primary lung cancer 47
VATS resections for primary lung cancer 49
Sleeve resections 52
Mediastinoscopy / mediastinotomy 53
Conditions other than primary lung cancer 54
Resections for other conditions 54
Surgery for pneumothorax 56
Total procedures for pneumothorax 56
Open versus VATS procedures 57
Mortality after procedures for pneumothorax 58
Surgery for upper GI disorders 59
Total activity for upper GI disorders 59
Minimally invasive resections 62
Operative mortality 63
Open / close rates in upper GI surgery 63
The future of thoracic surgical data collection in the United Kingdom and Ireland 66
Appendices
Appendix 1 The Thoracic Surgical Register (1980-2002) submission form 70
Appendix 2 The Thoracic Surgical Register (2002-date) submission form 79
Appendix 3 National minimum dataset for thoracic surgery & lung cancer surgery 82


National activity

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
1�
Nat
ion
al a
ctiv
ity
National activity
Total activity
Total surgical activity
This chart includes all procedures recorded excluding endoscopies. There is a trend to increased activity over the years, although this increase appears to have plateaued from �000-�001 onwards.
Total major procedures
A fairly static activity.
Total surgical activity (n=340,422)
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
Major procedures performed (n=263,345)
0
2,000
4,000
6,000
8,000
10,000
12,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
0
2,000
4,000
6,000
8,000
10,000
12,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
13
Natio
nal activity
Open versus VATS procedures
Open surgery implies operations carried out using standard major incisions such as thoracotomy. Minimally invasive surgery means much smaller incisions are used and has been part of the armamentarium of thoracic surgeons for many decades, ever since thoracoscopy was invented in the early twentieth century. In the 1980s fibre-optic endoscopy was enhanced by the addition of a video link hence the acronym VATS, which stands for Video Assisted Thoracic Surgery; as in other branches of surgery this opened up the range of procedures which became possible using minimally invasive techniques.
For the sake of continuity and simplicity throughout this report, all minimally invasive procedures are described as VATS operations.
These data (which includes minor as well as major activity) shows a clear increase in the number of minimally invasive procedures carried out within thoracic surgery.
VATS as a proportion of total workload (n=340,422)
0%
5%
10%
15%
20%
25%
30%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS
0%
5%
10%
15%
20%
25%
30%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
14
Nat
ion
al a
ctiv
ity
Lung resections
Total lung resections
This includes resections of lung for any reason both diagnostic and therapeutic, and for all pathologies.
VATS as a proportion of all lung resections
A clear increase in VATS resections is seen throughout the 1990s. A major reason for this is the introduction of diagnostic VATS lung biopsy.
Lung resections performed (n=120,521)
0
1,000
2,000
3,000
4,000
5,000
6,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f lu
ng
res
ecti
on
s
0
1,000
2,000
3,000
4,000
5,000
6,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f lu
ng
res
ecti
on
s
VATS as a proportion of all lung resections performed (n=120,521)
0%
3%
6%
9%
12%
15%
18%
21%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f lu
ng
res
ecti
on
s th
at w
ere
VA
TS
0%
3%
6%
9%
12%
15%
18%
21%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f lu
ng
res
ecti
on
s th
at w
ere
VA
TS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
15
Natio
nal activity
Pathology for patients undergoing lung resections
Although the majority of patients undergo lung resections for primary cancer, there has been a steady increase in the proportion suffering from other pathologies. Among the many and varied underlying diseases involved are included therapeutic resection for secondary cancer, benign tumours and suppurative lung disease, as well as a diagnostic resection for diffuse lung disease.
Proportion resections for patients with primary lung cancer (n=120,384)
50%
55%
60%
65%
70%
75%
80%
85%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pat
ien
ts w
ith
pri
mar
y lu
ng
can
cer
50%
55%
60%
65%
70%
75%
80%
85%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pat
ien
ts w
ith
pri
mar
y lu
ng
can
cer

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
16
Nat
ion
al a
ctiv
ity
Primary lung cancer
Resections for primary lung cancer
A slight downward trend is seen, the reasons for which are likely to be multi-factorial. Improved selection of patients for surgery is one possibility, such that patients who cannot benefit from resection of their cancer because of spread of the tumour are not subjected to surgery. A more worrying possibility is the potential effect of the rapid increase in cardiac surgical activity throughout this time period. It may be that the greater proportion of time spent by cardiothoracic surgeons on cardiac surgery led to a reduced access for patients with lung cancer to a surgeon who was prepared to help treat them.
Resections for primary lung cancer (n=87,367)
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f res
ecti
on
s fo
rp
rim
ary
lun
g c
ance
r
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f res
ecti
on
s fo
rp
rim
ary
lun
g c
ance
r

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
17
Natio
nal activity
Type of resections for primary lung cancer
There are three basic operations used to treat lung cancer. The lung is divided into anatomical lobes; lobectomy means removal of one or occasionally two lobes along with the cancer. Thus the category of lobectomy in this report includes the operation of bilobectomy - the removal of two lobes, as well as the much more commonly performed operation of removal of a single lobe. Pneumonectomy means removal of the whole of a patient’s lung and is a more dangerous and destructive operation than a lobectomy. A limited resection includes the techniques of wedge and segmentectomy and means removal of less than a lobe. These operations are considered to have a reduced chance of curing a patient’s lung cancer than a lobectomy. They are generally reserved for patients with poor pulmonary reserve or other comorbidity, for whom a surgeon considers that a lobectomy would carry an inordinately high risk.
The chart shows a clear trend to a reduction in the proportion of pneumonectomies, implying recognition of its dangers by surgeons and better selection of patients for surgery to treat their cancer. There has been a slight rise in the proportion of limited resections; this is likely to be due to a willingness by surgeons to offer higher risk patients a chance of cure of their cancer given improvements in surgical and anaesthetic techniques and post-operative care.
Type of resection for primary lung cancer (n=86,160)
Pneumonectomy Lobectomy
Wedge / segmentectomy
0%
20%
40%
60%
80%
100%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s
0%
20%
40%
60%
80%
100%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
18
Nat
ion
al a
ctiv
ity
Open / close rates in primary lung cancer surgery
This describes a situation when a patient is taken to the operating theatre with the intention of removing their lung cancer, but this proves impossible or inappropriate. The patient therefore undergoes a general anaesthetic and major chest incision without any therapeutic benefit.
There has always been vigorous discussion surrounding the issue of open and close surgery for cancer. On the one hand it is a painful and potentially dangerous undertaking with devastating emotional consequences and should be avoided at all costs; the opposite view is that an open and close rate of zero reflects some patients being denied the possibility of potentially curative surgery.
The open and close rate for lung cancer surgery has reduced dramatically throughout the life of the Register. This undoubtedly reflects more accurate pre-operative staging, especially with the introduction of routine CT scanning in the late 1980s.
Open / close rates in surgery for primary lung cancer (n=87,367)
0%
4%
8%
12%
16%
20%
24%
28%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Op
en /
clo
se r
ate
0%
4%
8%
12%
16%
20%
24%
28%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Op
en /
clo
se r
ate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
19
Natio
nal activity
Mortality following surgery for primary lung cancer
As described previously, operative death is defined as death occurring after surgery within base hospital. The higher operative mortality after pneumonectomy is well shown. Limited resections have the lowest death rates despite the likelihood that these patients had a higher incidence of limited pulmonary reserve. There is a suggestion from the charts that hospital death rates have declined over the years, presumably reflecting more appropriate selection of patients for surgery, improving surgical and anaesthetic techniques, and better post-operative care.
Mortality after pneumonectomy for primary lung cancer (n=26,363)
0%
2%
4%
6%
8%
10%
12%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
0%
2%
4%
6%
8%
10%
12%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
Mortality after lobectomy for primary lung cancer (n=52,663)
0%
1%
2%
3%
4%
5%
6%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
6%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�0
Nat
ion
al a
ctiv
ity
Mortality after wedge resection for primary lung cancer (n=7,134)
0%
1%
2%
3%
4%
5%
6%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
6%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�1
Natio
nal activity
VATS resections for primary lung cancer
Although VATS wedge resections constitute a significant minority of resections for lung cancer resections, the more technically demanding VATS lobectomy has remained a rarity when considering activity throughout the country as a whole.
VATS as a proportion of all resections for primary lung cancer (n=87,367)
0%
1%
2%
3%
4%
5%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS
0%
1%
2%
3%
4%
5%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
��
Nat
ion
al a
ctiv
ity
VATS as a proportion of all wedge resections / segmetectomies for primary lung cancer (n=7,134)
0%
4%
8%
12%
16%
20%
24%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS
0%
4%
8%
12%
16%
20%
24%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS
VATS as a proportion of all lobectomies for primary lung cancer (n=51,615)
0%
1%
2%
3%
4%
5%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS
0%
1%
2%
3%
4%
5%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�3
Natio
nal activity
Sleeve resections
This refers to an operation where in addition to a lobectomy a section of the main air passage to the lung is also removed. Although this can be a more technically demanding operation than a standard lobectomy it has the major advantage of preventing the need for a pneumonectomy, with its potential for adverse short and long-term sequelae. Despite being an ideal compromise operation for some patients the anatomical situations for which it can be used are unusual when set against the overall activity. Specific data on sleeve resections has only been collected since the year 1989-1990
Sleeve resections as a proportion of all resections for primary lung cancer (n=54,434)
0%
1%
2%
3%
4%
5%
1989
-90
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f res
sect
ion
sth
at w
ere
slee
ve r
esec
tio
ns
0%
1%
2%
3%
4%
5%
1989
-90
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f res
sect
ion
sth
at w
ere
slee
ve r
esec
tio
ns

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�4
Nat
ion
al a
ctiv
ity
Mediastinoscopy / mediastinotomy
These two diagnostic operations are carried out through small incisions, principally to biopsy lymph nodes within the chest. This can be of major importance when selecting patients for lung cancer surgery..
The Register collects activity for these procedures without differentiation as to the disease the patient is ultimately proved to be suffering from. Although lung cancer may represent the largest disease group of patients undergoing mediastinoscopy or mediastinotomy, many other conditions may be diagnosed, both malignant and non-malignant in nature. Therefore the mediastinoscopy / mediastinotomy rate as a proportion overall number of lung cancer resections should be interpreted with caution. Nevertheless there has been a marked increase in the number of procedures carried out, which will in part reflect more thorough lung cancer staging prior to resection. The increasing rate mirrors the decreasing rate of open / close operations for lung cancer.
Mediastinoscopy / mediastinotomy as a proportion of all resections for primary lung cancer (n=56,865)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%19
80
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Med
iati
no
sco
py
/ med
iati
no
tom
y ra
teco
mp
ared
wit
h t
ota
l nu
mb
ers
of
rese
ctio
ns
for
pri
mar
y lu
ng
can
cer
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%19
80
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Med
iati
no
sco
py
/ med
iati
no
tom
y ra
teco
mp
ared
wit
h t
ota
l nu
mb
ers
of
rese
ctio
ns
for
pri
mar
y lu
ng
can
cer

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�5
Natio
nal activity
Conditions other than primary lung cancer
Resections for other conditions
As described earlier in the report (see page 15), there has been a steady increase in this activity. The increasing number of VATS resections reflects confidence in the technique of VATS lung biopsy for diffuse disease as well as the excision biopsy of indeterminate and often benign pulmonary nodules.
Lung resections for conditions other than primary lung cancer (n=33,017)
0
300
600
900
1,200
1,500
1,800
2,100
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f lu
ng
res
ecti
on
s
0
300
600
900
1,200
1,500
1,800
2,100
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f lu
ng
res
ecti
on
s
VATS as a proportion of all resections for conditions other than primary lung cancer (n=33,017)
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�6
Nat
ion
al a
ctiv
ity
Surgery for pneumothorax
Total procedures for pneumothorax
The number of procedures carried out to either prevent recurrent pneumothoraces or to repair a persistent air leak from the lung has risen steadily, especially since the introduction of VATS techniques, the latter forming the majority of operations soon after introduction of VATS in the mid 1990s. This increase in overall activity probably reflects awareness of the safety and advantages of pneumothorax surgery by thoracic surgeons, as well as increasing referrals from physicians for consideration of surgery. It is likely also that the advent of VATS techniques was responsible for an increase in referrals, despite continued debate within the thoracic surgical community as to whether or not VATS techniques can offer similar long-term results to more traditional open surgery.
Procedures for pneumothorax (n=26,566)
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�7
Natio
nal activity
Open versus VATS procedures
VATS as a proportion of all procedures for pneumothorax (n=26,566)
0%
10%
20%
30%
40%
50%
60%
70%
80%
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
9
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS
0%
10%
20%
30%
40%
50%
60%
70%
80%
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
9
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
s th
at w
ere
VA
TS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�8
Nat
ion
al a
ctiv
ity
Mortality after procedures for pneumothorax
Although at first sight VATS seems to be a safer technique than open surgery for pneumothorax, this difference in operative mortality undoubtedly reflects differences in the type of patient being subjected to the two techniques. Primary spontaneous pneumothorax occurs in young otherwise fit patients without underlying lung disease, and can easily be treated with VATS with almost no deaths. In contrast a secondary pneumothorax occurring in conditions such as emphysema frequently requires open surgery to be successful and the higher death rate reflects the increased comorbidity in these patients.
Mortality after surgery for pneumothorax (n=18,362 & n=8,204 respectively)
Open VATS
0%
1%
2%
3%
4%
5%
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
1980
-198
1
1981
-198
2
1982
-198
3
1983
-198
4
1984
-198
5
1985
-198
6
1986
-198
7
1987
-198
8
1988
-198
9
1989
-199
0
1990
-199
1
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
�9
Natio
nal activity
Surgery for upper GI disordersAlthough surgical treatment of diseases of the proximal gastrointestinal organs (upper GI surgery) has become a subspecialty of general surgery over the last decade, surgery of the oesophagus has historically been part of the practice of cardiothoracic surgeons. As well as treating oesophageal cancer thoracic surgeons have been active in the management of benign oesophageal diseases such as hiatus hernia, reflux disease and oesophageal motility disorders.
Total activity for upper GI disorders
There has been a marked decrease in overall activity in this area in thoracic surgical Units, especially since the mid-1990s when upper GI surgeons began to take responsibility for treating oesophageal as well as gastric cancer. However there are many more influences at work here. The introduction of the flexible gastroscope in the 1970s allowed the development of the medical sub-specialty of gastroenterology. There followed rapid access endoscopy services which diverted the necessity for diagnosis of oesophageal diseases away from increasingly centralised thoracic surgeons working in specialised Units. Referrals for surgical opinions with regard to all types of oesophageal disease became diverted away from thoracic surgeons to more easily accessible upper GI surgeons working alongside gastroenterologists in local hospitals.
As well as changing medical specialisation, these changes reflect changing patterns of treatment for some diseases. With the development of superior medical therapies for peptic ulcer and gastro-oesophageal reflux disease, the need for surgery in these conditions has become much less common. To compensate for this reducing workload, general and latterly specialist upper GI surgeons have extended their practice to include the treatment of oesophageal cancer which has shown a marked increase in incidence over the last thirty years. These important developments explain the reduction of upper GI activity in the thoracic surgical community, particularly over the last decade.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
30
Nat
ion
al a
ctiv
ity
Total procedures for upper GI disorders (n=44,883)
0
500
1,000
1,500
2,000
2,500
3,00019
80
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
0
500
1,000
1,500
2,000
2,500
3,00019
80
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
Resections for upper GI cancer (n=19,131)
0
200
400
600
800
1,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
0
200
400
600
800
1,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
31
Natio
nal activity
Other major upper GI procedures (n=25,704)
0
400
800
1,200
1,600
2,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s
0
400
800
1,200
1,600
2,000
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Nu
mb
er o
f pro
ced
ure
s

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
3�
Nat
ion
al a
ctiv
ity
Minimally invasive resections
Minimally invasive surgery for oesophageal cancer treatment using a combination of thoracoscopy and laparoscopy remains a novel therapy at the present time. As will be seen later in the report, this technique is only carried out in one thoracic Unit within the UK.
Operative mortality
Generally speaking the procedure of oesophageal cancer resection carries the highest operative mortality of any elective operation. Despite falling activity, operative mortality for oesophagectomy when carried out under the auspices of thoracic surgery has steadily fallen over the lifetime of the Register and remains enviably very low. Undoubtedly this is less to do with surgical technique than the well-developed infrastructure for looking after patients undergoing chest surgery in thoracic surgical Units.
VATS as a proportion of all resections for upper GI cancer (n=19,131)
0%
2%
4%
6%
8%
10%
12%
14%
16%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
sth
at w
ere
VA
TS
0%
2%
4%
6%
8%
10%
12%
14%
16%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Per
cen
tag
e o
f pro
ced
ure
sth
at w
ere
VA
TS
Mortality after procedures for upper GI disorders (n=19,131)
0%
4%
8%
12%
16%
20%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate
0%
4%
8%
12%
16%
20%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Cru
de
mo
rtal
ity
rate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
33
Natio
nal activity
Open / close rates in upper GI surgery
As explained in the section on lung cancer open and close, the appropriate rate for this intervention is somewhat debatable. With respect to the Register, open and close in the context of upper GI cancer is vulnerable to the problem of variability of definition. For example some surgeons carry out a laparoscopy or thoracoscopy prior to an oesophageal resection and if the examination appears unfavourable will then not proceed to a major incision; thus the patient suffers very little following the intervention. Nevertheless, the Society feels that this is an important end-point to report in the context of surgical management of cancer..
Open / close rates in surgery for upper GI disorders (n=19,131)
0%
4%
8%
12%
16%
20%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Op
en /
clo
se r
ate
0%
4%
8%
12%
16%
20%
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
-199
2
1992
-199
3
1993
-199
4
1994
-199
5
1995
-199
6
1996
-199
7
1997
-199
8
1998
-199
9
1999
-200
0
2000
-200
1
2001
-200
2
2002
-200
3
2003
-200
4
2004
-200
5
Period
Op
en /
clo
se r
ate


Unit-specific report

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
36
Un
it-s
pec
ific
acti
vity
Unit-specific activity
Contributing UnitsThe following data form a report on activity for the three-year period running from the beginning of April �00� to the end of March �005. Thirty-six out of a possible forty Units were able to send data returns for this period. Although some of the non-returning Units carry out a substantial amount of thoracic surgery, the Society estimates that the report encompasses at least 95% of the activity carried out within the United Kingdom and Ireland in terms of the number of patient-based procedures.
City Hospital Thoracic surgical audit lead
Aberdeen Royal Infirmary Mr Hussein El Shafei
Belfast Royal Victoria Hospital Mr Alastair Graham
Birmingham Heartlands Hospital Mr Pala Rajesh
Blackpool Victoria Hospital Mr John Au
Bristol Royal Infirmary Mr Anthony Morgan
Cardiff University Hospital of Wales Mr Peter O’Keefe
Cork University Hospital Mr Tom Aherne
Coventry University Hospital Mr Joseph Marzouk
Dublin St James’s Hospital Mr Vincent Young
Edinburgh Royal Infirmary Mr William Walker
Exeter Royal Devon and Exeter Mr Richard Berrisford
Glasgow Western Infirmary Mr Alan Kirk
Hull Castle Hill Hospital Mr Michael Cowen
Leeds St James’s Hospital Mr Kostas Papagiannopoulos
Leicester Glenfield Hospital Mr David Waller
Liverpool The Cardiothoracic Centre Mr Richard Page
London Barts and the London Mr Alan Wood
London Guys and St Thomas’s Mr Robert Cameron
London Hammersmith Hospital Mr Prakash Punjabi
London Harefield Hospital Mr Edward Townsend
London King’s College Hospital Mr Michael Marrinan
London Royal Brompton Hospital Mr George Ladas
London St George’s Hospital Mr Robin Kanagasaby
London St Mary’s Hospital Mr Rex Stanbridge
London The Heart Hospital Mr Shyam Kolvekar
Manchester Royal Infirmary Mr Daniel Keenan
Manchester South Manchester University Mr Rajesh Shah
Middlesbrough James Cook Hospital Mr Andrew Owens
Newcastle Freeman Hospital Mr Sion Barnard
Norwich University Hospital Mr Marc Van Leuvan
Nottingham City Hospital Mr David Beggs
Oxford John Radcliffe Hospital Mr Chandi Ratnatunga
Papworth Papworth Hospital Mr Andrew Ritchie
Sheffield Northern General Hospital Mr David Hopkinson
Southampton General Hospital Mr Khalid Amer
Stoke-on-Trent North Staffordshire University Mr Christopher Smallpeice

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
37
Un
it-specifi
c activity
The following four hospitals were unable to contribute to the Register, although the Society is aware of significant thoracic surgical activity being carried out for the period �00�-�005:
• Bradford Royal Infirmary (ceased activity in �004)
• Glasgow Royal Infirmary
• Hairmyers Hospital, Glasgow
• Plymouth Royal Infirmary
Organisation of the reportWhen constructing the charts the hospital Units are sorted according to activity, starting with hospitals having the least activity progressing downwards to those with the highest activity. This order changes depending on a Unit’s contribution to a specific operation. For example Birmingham Heartlands Hospital carries out the most procedures for lung cancer, whereas Guy’s and St Thomas’s is by far the most active in terms of pneumothorax surgery. Thus data points on the appropriate charts for these two hospitals are located at the foot of the y-axes. This order is maintained when comparing differences in types of surgery; for example when comparing open versus VATS surgery between Units the busiest Units overall in the area of concern remain at the foot of the charts.
Caution should be used when attempting to interpret differences in activity between Units for the following reasons:
1. Some Units cover a much wider geographical area and/or population than others so will inevitable carry out more procedures.
�. The report has made no distinction between Units carrying out cardiac surgery in addition to thoracic surgery and those with a solely thoracic practice.
3. It is known that respiratory diseases in general are more prevalent in some parts of the country than others, which will govern the need for thoracic surgery within a particular Unit serving that area. For example, cities such as Liverpool and Glasgow have some of the highest incidences of lung cancers, not only in the United Kingdom, but also throughout the world so it is entirely appropriate that Units located in these areas should have a busier thoracic surgical practice.
4. It may well be that differences in activity reflect different resources available for thoracic surgery, i.e. a post-code lottery of treatment. This concern cannot be explored further in this report. As with activity within any specialised area of medicine although the numerator (e.g. the number of resections carried out for lung cancer per thoracic surgical Unit) may be easily measurable, the denominator (in this example the number of cases of lung cancer within the base population) is usually unknown with any real accuracy. Although it is tempting and indeed important to reflect on this issue the Society urges that this report is only used as a guide when comparing lung cancer resection rates or indeed any area of thoracic surgical practice throughout the country.
The charts follow exactly the same order as in the section on national activity; the accompanying text in that section should be used to aid interpretation as necessary. Additional text is supplied for clarity as needed.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
38
Un
it-s
pec
ific
acti
vity
Total activity
Total surgical activity
Total surgical activity; financial years 2003-2005 (n=45,429)
0 500 1,000 1,500 2,000 2,500 3,000 3,500
Birmingham
Liverpool
Edinburgh
Brompton
Newcastle
Hull
Southampton
Harefield
Guy's / St Thomas's
Leeds
Belfast
Sheffield
Norwich
Wythenshawe
Bristol
St Georges
The Heart Hospital
Nottingham
Cardiff
Papworth
Blackpool
Leicester
Glasgow
Exeter
Coventry
Dublin
Bart's & the London
Hammersmith
Manchester Royal Informary
Aberdeen
Stoke
Middlesborough
Cork
St Mary's
Kings College Hospital
Oxford
Un
it
Number of procedures
0 500 1,000 1,500 2,000 2,500 3,000 3,500
Birmingham
Liverpool
Edinburgh
Brompton
Newcastle
Hull
Southampton
Harefield
Guy's / St Thomas's
Leeds
Belfast
Sheffield
Norwich
Wythenshawe
Bristol
St Georges
The Heart Hospital
Nottingham
Cardiff
Papworth
Blackpool
Leicester
Glasgow
Exeter
Coventry
Dublin
Bart's & the London
Hammersmith
Manchester Royal Informary
Aberdeen
Stoke
Middlesborough
Cork
St Mary's
Kings College Hospital
Oxford
Un
it
Number of procedures

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
39
Un
it-specifi
c activity
Total major procedures
Major procedures performed; financial years 2003-2005 (n=45,429)
0 500 1,000 1,500 2,000 2,500 3,000
Birmingham
Liverpool
Edinburgh
Brompton
Southampton
Harefield
Guy's / St Thomas's
Hull
Newcastle
Belfast
Sheffield
Wythenshawe
Leeds
Bristol
The Heart Hospital
Nottingham
Norwich
St Georges
Cardiff
Papworth
Blackpool
Leicester
Exeter
Bart's & the London
Glasgow
Dublin
Coventry
Middlesborough
Manchester Royal Informary
Hammersmith
Aberdeen
Stoke
St Mary's
Cork
Kings College Hospital
Oxford
Un
it
Number of procedures
0 500 1,000 1,500 2,000 2,500 3,000
Birmingham
Liverpool
Edinburgh
Brompton
Southampton
Harefield
Guy's / St Thomas's
Hull
Newcastle
Belfast
Sheffield
Wythenshawe
Leeds
Bristol
The Heart Hospital
Nottingham
Norwich
St Georges
Cardiff
Papworth
Blackpool
Leicester
Exeter
Bart's & the London
Glasgow
Dublin
Coventry
Middlesborough
Manchester Royal Informary
Hammersmith
Aberdeen
Stoke
St Mary's
Cork
Kings College Hospital
Oxford
Un
it
Number of procedures

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
40
Un
it-s
pec
ific
acti
vity
Open versus VATS procedures
There is substantial variation in the adoption of VATS techniques throughout the UK. This variation becomes even more marked when assessing individual operations such as pneumothorax operations or limited lung resections. This phenomenon has been reported previously by Sedrakyan and colleagues 1 in a publication analysing data taken from the Register. It is likely that the variation in the use of VATS relates more to individual surgeon preference rather than availability of facilities
VATS as a proportion of total workload;financial years 2003-2005 (n=45,429)
0% 10% 20% 30% 40% 50% 60% 70%
Birmingham
Liverpool
Edinburgh
Brompton
Newcastle
Hull
Southampton
Harefield
Guy's / St Thomas's
Leeds
Belfast
Sheffield
Norwich
Wythenshawe
Bristol
St Georges
The Heart Hospital
Nottingham
Cardiff
Papworth
Blackpool
Leicester
Glasgow
Exeter
Coventry
Dublin
Bart's & the London
Hammersmith
Manchester Royal Informary
Aberdeen
Stoke
Middlesborough
Cork
St Mary's London
Kings College Hospital
Oxford
Un
it
Percentage of lung resections that were VATS
0% 10% 20% 30% 40% 50% 60% 70%
Birmingham
Liverpool
Edinburgh
Brompton
Newcastle
Hull
Southampton
Harefield
Guy's / St Thomas's
Leeds
Belfast
Sheffield
Norwich
Wythenshawe
Bristol
St Georges
The Heart Hospital
Nottingham
Cardiff
Papworth
Blackpool
Leicester
Glasgow
Exeter
Coventry
Dublin
Bart's & the London
Hammersmith
Manchester Royal Informary
Aberdeen
Stoke
Middlesborough
Cork
St Mary's London
Kings College Hospital
Oxford
Un
it
Percentage of lung resections that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
41
Un
it-specifi
c activity
Lung resections
Total lung resections
.
Lung resections performed; financial years 2003-2005 (n=15,654)
0 200 400 600 800 1,000 1,200 1,400
Birmingham
Liverpool
Brompton
Edinburgh
Newcastle
Hull
Sheffield
Cardiff
Southampton
Harefield
Leicester
Papworth
Bart's & the London
Bristol
Nottingham
Guy's / St Thomas's
Wythenshawe
The Heart Hospital
Belfast
Norwich
Leeds
St Georges
Glasgow
Dublin
Blackpool
Coventry
Hammersmith
Middlesborough
Aberdeen
Stoke
Exeter
Manchester Royal Informary
St Mary's London
Cork
Kings College Hospital
Oxford
Un
it
Number of lung resections
0 200 400 600 800 1,000 1,200 1,400
Birmingham
Liverpool
Brompton
Edinburgh
Newcastle
Hull
Sheffield
Cardiff
Southampton
Harefield
Leicester
Papworth
Bart's & the London
Bristol
Nottingham
Guy's / St Thomas's
Wythenshawe
The Heart Hospital
Belfast
Norwich
Leeds
St Georges
Glasgow
Dublin
Blackpool
Coventry
Hammersmith
Middlesborough
Aberdeen
Stoke
Exeter
Manchester Royal Informary
St Mary's London
Cork
Kings College Hospital
Oxford
Un
it
Number of lung resections

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
4�
Un
it-s
pec
ific
acti
vity
VATS as a proportion of all lung resections
There appears to be no relationship between the number of lung resections carried out per Unit and the frequency of the use of minimally invasive techniques.
VATS as a proportion of all lung resections performed; financial years 2003-2005 (n=14,990)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Birmingham
Liverpool
Brompton
Edinburgh
Newcastle
Hull
Sheffield
Cardiff
Southampton
Harefield
Leicester
Bart's & the London
Papworth
Bristol
Nottingham
Guy's / St Thomas's
The Heart Hospital
Norwich
Belfast
Wythenshawe
Leeds
St Georges
Glasgow
Blackpool
Dublin
Coventry
Middlesborough
Hammersmith
Aberdeen
Exeter
Stoke
Manchester Royal Informary
St Mary's London
Cork
Kings College Hospital
Oxford
Un
it
Percentage of lung resections that were VATS
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Birmingham
Liverpool
Brompton
Edinburgh
Newcastle
Hull
Sheffield
Cardiff
Southampton
Harefield
Leicester
Bart's & the London
Papworth
Bristol
Nottingham
Guy's / St Thomas's
The Heart Hospital
Norwich
Belfast
Wythenshawe
Leeds
St Georges
Glasgow
Blackpool
Dublin
Coventry
Middlesborough
Hammersmith
Aberdeen
Exeter
Stoke
Manchester Royal Informary
St Mary's London
Cork
Kings College Hospital
Oxford
Un
it
Percentage of lung resections that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
43
Un
it-specifi
c activity
Pathology for patients undergoing lung resections
This chart shows wide variation in the pathology of lung resections. Although definitions may have a bearing on this undoubtedly some Units are much more active than others in their involvement lung resections for secondary malignancy, suppurative lung disease and lung biopsies.
Proportion resections for patients with primary lung cancer;financial years 2003-2005 (n=15,654)
0% 20% 40% 60% 80% 100%
Birmingham
Liverpool
Brompton
Edinburgh
Newcastle
Hull
Sheffield
Cardiff
Southampton
Harefield
Leicester
Papworth
Bart's & the London
Bristol
Nottingham
Guy's / St Thomas's
Wythenshawe
The Heart Hospital
Belfast
Norwich
Leeds
St Georges
Glasgow
Dublin
Blackpool
Coventry
Hammersmith
Middlesborough
Aberdeen
Stoke
Exeter
Manchester Royal Informary
St Mary's London
Cork
Kings College Hospital
Oxford
Un
it
Percentage of patients with primary lung cancer
0% 20% 40% 60% 80% 100%
Birmingham
Liverpool
Brompton
Edinburgh
Newcastle
Hull
Sheffield
Cardiff
Southampton
Harefield
Leicester
Papworth
Bart's & the London
Bristol
Nottingham
Guy's / St Thomas's
Wythenshawe
The Heart Hospital
Belfast
Norwich
Leeds
St Georges
Glasgow
Dublin
Blackpool
Coventry
Hammersmith
Middlesborough
Aberdeen
Stoke
Exeter
Manchester Royal Informary
St Mary's London
Cork
Kings College Hospital
Oxford
Un
it
Percentage of patients with primary lung cancer

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
44
Un
it-s
pec
ific
acti
vity
Primary lung cancer
Resections for primary lung cancer
Resections for primary lung cancer; financial years 2003-2005 (n=10,047)
0 100 200 300 400 500 600 700 800
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Harefield
Bristol
Leicester
Southampton
Belfast
St Georges
Nottingham
Brompton
Norwich
Glasgow
Papworth
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Number of resections for primary lung cancer
0 100 200 300 400 500 600 700 800
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Harefield
Bristol
Leicester
Southampton
Belfast
St Georges
Nottingham
Brompton
Norwich
Glasgow
Papworth
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Number of resections for primary lung cancer

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
45
Un
it-specifi
c activity
Type of resections for primary lung cancer
Pneumonectomy rates are generally low throughout the country. However there are some major differences in the proportion of limited (i.e. wedge or segmentectomy) resections throughout the country. This may reflect a greater proportion of patients with poor pulmonary reserve in Units such as Leeds, which has the highest proportion of limited resections. Or it may reflect greater belief in the value of a limited resection in smaller lung cancers as a way of preserving pulmonary parenchyma.
Type of resection for primary lung cancer; financial years 2003-2005 (n=9,816)
Pneumonectomy Lobectomy
Wedge / segmentectomy
0% 20% 40% 60% 80% 100%
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Bristol
Harefield
Leicester
Southampton
St Georges
Nottingham
Belfast
Norwich
Brompton
Papworth
Glasgow
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Percentage of procedures
0% 20% 40% 60% 80% 100%
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Bristol
Harefield
Leicester
Southampton
St Georges
Nottingham
Belfast
Norwich
Brompton
Papworth
Glasgow
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Percentage of procedures

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
46
Un
it-s
pec
ific
acti
vity
Open / close rates in primary lung cancer surgery
This chart shows wide variations across the country. Some Units report zero open / close operations with others reporting rates as high as �0% of the total number of lung resections. Given that the overall average for the country is in the order of 6% there are a number of explanations for this variation:
1. As explained in the section on national activity (see page 18) there is always vigorous debate as to what the appropriate rate for open / close operations should be in lung cancer surgery. Those surgeons who argue for a high rate say that it is better to carry out a thoracotomy and see if a patient is operable, but, if not, to avoid the additional trauma and morbidity of a lung resection when it can be of no benefit to the patient, for example because of extensive lymph node metastases. They argue that a zero rate is likely to be due to some patients having aggressive and ultimately unhelpful surgery. The opposite view is that it is virtually always beneficial to a patient who has undergone a thoracotomy to have their tumour resected as long as it can be achieved with safety.
�. The national open / close rate has fallen steadily throughout the last twenty-five years (see page 18); it is likely that this is due to improvements in the pre-operative selection of patients for surgery. It also likely that these improvements have been adopted at differing rates throughout the country. The data in this report extend between the years �00� and �005, and much will have happened to improve patient management throughout this time and since, with innovations such as lung cancer multi-disciplinary teams, higher resolution CT scanners and the introduction of PET-CT scanning. As these innovations extend across the country it is likely that the open / close rates will become less variable relative to the national mean.
3. Especially in small volume Units a small change in the number of open / close operations will make a large impact on the percentage reported. Data collection inaccuracies could be responsible for an exaggeration of this effect.
Open / close rates in surgery for primary lung cancer;financial years 2003-2005 (n=10,046)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
0 100 200 300 400 500 600 700 800
Number of procedures
Op
en /
clo
se r
ate
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
0 100 200 300 400 500 600 700 800
Number of procedures
Op
en /
clo
se r
ate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
47
Un
it-specifi
c activity
Mortality following surgery for primary lung cancer
Encouragingly there is very little difference in operative mortality throughout the country, and no apparent volume effect. Treasure � has shown this in a previous publication based on data taken from the Register. The Society agrees with his conclusion that thoracic or cardiothoracic surgeons who are adept in carrying out major chest operations on a regular basis within high-volume cardiothoracic surgical Units can produce equally low mortalities for lung cancer resections irrespective of the volume of individual procedures carried out per surgeon. This presumably implies that it is principally the selection of the patients for surgery rather than the technical skill of a surgeon which determines the operative result. This has long been recognised by thoracic surgeons, but unfortunately is beyond the scope of this report to investigate further.
Mortality after pneumonectomy for primary lung cancer; financial years 2003-2005 (n=1,510)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
0 20 40 60 80 100 120 140
Number of procedures
Mo
rtal
ity
rate
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
0 20 40 60 80 100 120 140
Number of procedures
Mo
rtal
ity
rate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
48
Un
it-s
pec
ific
acti
vity
Mortality after wedge resection / segmentectomy for primary lung cancer; financial years 2003-2005 (n=1,371)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
0 20 40 60 80 100 120 140 160 180 200
Number of procedures
Mo
rtal
ity
rate
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
0 20 40 60 80 100 120 140 160 180 200
Number of procedures
Mo
rtal
ity
rate
Mortality after lobectomy for primary lung cancer; financial years 2003-2005 (n=6,932)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
1%
2%
3%
4%
5%
6%
7%
8%
0 100 200 300 400 500 600
Number of procedures
Mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
6%
7%
8%
0 100 200 300 400 500 600
Number of procedures
Mo
rtal
ity
rate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
49
Un
it-specifi
c activity
VATS resections for primary lung cancer
Although some Units (notably Edinburgh and St Mary’s) are obviously enthusiastic practitioners of VATS lobectomy this remains a rare activity in most Units. VATS wedge resection is more popular and more evenly distributed throughout the country.
VATS as a proportion of all resections for primary lung cancer; financial years (n=6,932)
0% 20% 40% 60% 80% 100%
Liverpool
Birmingham
Newcastle
Sheffield
Edinburgh
Guy's / St Thomas's
Hull
Wythenshawe
Bart's & the London
Cardiff
Leicester
Harefield
Southampton
St Georges
Brompton
Bristol
Nottingham
Belfast
Glasgow
Norwich
Papworth
Leeds
Middlesborough
Dublin
Blackpool
Manchester Royal Informary
The Heart Hospital
Stoke
Coventry
Exeter
Cork
St Mary's London
Hammersmith
Aberdeen
Kings College Hospital
Oxford
Un
it
Percentage of procedures that were VATS
0% 20% 40% 60% 80% 100%
Liverpool
Birmingham
Newcastle
Sheffield
Edinburgh
Guy's / St Thomas's
Hull
Wythenshawe
Bart's & the London
Cardiff
Leicester
Harefield
Southampton
St Georges
Brompton
Bristol
Nottingham
Belfast
Glasgow
Norwich
Papworth
Leeds
Middlesborough
Dublin
Blackpool
Manchester Royal Informary
The Heart Hospital
Stoke
Coventry
Exeter
Cork
St Mary's London
Hammersmith
Aberdeen
Kings College Hospital
Oxford
Un
it
Percentage of procedures that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
50
Un
it-s
pec
ific
acti
vity
VATS as a proportion of all lobectomies for primary lung cancer; financial years 2003-2005 (n=6,932)
0% 20% 40% 60% 80% 100%
Liverpool
Birm'hamHeartlands
Newcastle
Sheffield
Edinburgh
Guy's/StThom
Hull
Manch Wyth
Bart's/London
Cardiff
Leicester
Harefield
Southampton
StGeorges
Brompton
Bristol
Nottingham
Belfast
Glasgow West
Norwich
Papworth
Leeds
Middlesborough
Dublin StJam
Blackpool
Manch RI
UCLH/Middsx
Stoke
Coventry
Exeter
Cork
StMary's
Hammersmith
Aberdeen
Kings
Oxford
Un
it
Percentage of procedures that were VATS
0% 20% 40% 60% 80% 100%
Liverpool
Birm'hamHeartlands
Newcastle
Sheffield
Edinburgh
Guy's/StThom
Hull
Manch Wyth
Bart's/London
Cardiff
Leicester
Harefield
Southampton
StGeorges
Brompton
Bristol
Nottingham
Belfast
Glasgow West
Norwich
Papworth
Leeds
Middlesborough
Dublin StJam
Blackpool
Manch RI
UCLH/Middsx
Stoke
Coventry
Exeter
Cork
StMary's
Hammersmith
Aberdeen
Kings
Oxford
Un
it
Percentage of procedures that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
51
Un
it-specifi
c activity
VATS as a proportion of all wedge resections / segmetectomies for primary lung cancer; financial years 2003-2005 (n=1,371)
0% 20% 40% 60% 80% 100%
Leeds
Birmingham
Sheffield
Bristol
Hull
Cardiff
Harefield
Guy's / St Thomas's
The Heart Hospital
Liverpool
Belfast
Leicester
Nottingham
Southampton
Newcastle
Coventry
St Georges
Brompton
Exeter
Norwich
Bart's & the London
Glasgow
Wythenshawe
Blackpool
Papworth
Middlesborough
Hammersmith
Stoke
Aberdeen
Edinburgh
Cork
Kings College Hospital
Dublin
St Mary's London
Un
it
Percentage of procedures that were VATS
0% 20% 40% 60% 80% 100%
Leeds
Birmingham
Sheffield
Bristol
Hull
Cardiff
Harefield
Guy's / St Thomas's
The Heart Hospital
Liverpool
Belfast
Leicester
Nottingham
Southampton
Newcastle
Coventry
St Georges
Brompton
Exeter
Norwich
Bart's & the London
Glasgow
Wythenshawe
Blackpool
Papworth
Middlesborough
Hammersmith
Stoke
Aberdeen
Edinburgh
Cork
Kings College Hospital
Dublin
St Mary's London
Un
it
Percentage of procedures that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
5�
Un
it-s
pec
ific
acti
vity
Sleeve resections
Sleeve resections as a proportion of all resections for primary lung cancer; financial years 2003-2005 (n=10,047)
0% 2% 4% 6% 8% 10% 12% 14% 16%
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Harefield
Bristol
Leicester
Southampton
Belfast
St Georges
Nottingham
Brompton
Norwich
Glasgow
Papworth
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Percentage of resections that were sleeve resections
0% 2% 4% 6% 8% 10% 12% 14% 16%
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Harefield
Bristol
Leicester
Southampton
Belfast
St Georges
Nottingham
Brompton
Norwich
Glasgow
Papworth
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Percentage of resections that were sleeve resections

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
53
Un
it-specifi
c activity
Mediastinoscopy / mediastinotomy
Some interesting variations between Units although in all likelihood being due to the frequency of procedures for investigating conditions other than primary lung cancer as explained in the section on national activity.
Mediastinoscopy / mediastinotomy as a proportion of all resections for primary lung cancer;
financial years 2003-2005 (n=10,047 resections)
0.0 0.5 1.0 1.5 2.0 2.5
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Harefield
Bristol
Leicester
Southampton
Belfast
St Georges
Nottingham
Brompton
Norwich
Glasgow
Papworth
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Ratio of mediatinoscopy or mediastinotomy to total resections
0.0 0.5 1.0 1.5 2.0 2.5
Birmingham
Liverpool
Sheffield
Newcastle
Hull
Edinburgh
Guy's / St Thomas's
Cardiff
Bart's & the London
Leeds
Wythenshawe
Harefield
Bristol
Leicester
Southampton
Belfast
St Georges
Nottingham
Brompton
Norwich
Glasgow
Papworth
Middlesborough
Blackpool
Dublin
The Heart Hospital
Coventry
Exeter
Manchester Royal Informary
Stoke
Cork
Aberdeen
St Mary's London
Hammersmith
Oxford
Kings College Hospital
Un
it
Ratio of mediatinoscopy or mediastinotomy to total resections
Increasing numb
ers of lung resections

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
54
Un
it-s
pec
ific
acti
vity
Conditions other than primary lung cancer
Resections for other conditions
Lung resections for conditions other than primary lung cancer; financial years 2003-2005 (n=5,607)
0 100 200 300 400 500
Birmingham
Brompton
Liverpool
Southampton
Edinburgh
Papworth
The Heart Hospital
Newcastle
Hull
Harefield
Nottingham
Leicester
Cardiff
Bristol
Bart's & the London
Hammersmith
Sheffield
Norwich
Belfast
Aberdeen
Coventry
Dublin
Glasgow
Blackpool
Wythenshawe
Stoke
St Georges
St Mary's London
Manchester Royal Informary
Exeter
Guy's / St Thomas's
Kings College Hospital
Oxford
Leeds
Middlesborough
Cork
Un
it
Number of lung resections
0 100 200 300 400 500
Birmingham
Brompton
Liverpool
Southampton
Edinburgh
Papworth
The Heart Hospital
Newcastle
Hull
Harefield
Nottingham
Leicester
Cardiff
Bristol
Bart's & the London
Hammersmith
Sheffield
Norwich
Belfast
Aberdeen
Coventry
Dublin
Glasgow
Blackpool
Wythenshawe
Stoke
St Georges
St Mary's London
Manchester Royal Informary
Exeter
Guy's / St Thomas's
Kings College Hospital
Oxford
Leeds
Middlesborough
Cork
Un
it
Number of lung resections

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
55
Un
it-specifi
c activity
VATS as a proportion of all resections for conditions other than primary lung cancer; financial years 2003-2005 (n=5,607)
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Birmingham
Brompton
Liverpool
Southampton
Edinburgh
Papworth
The Heart Hospital
Newcastle
Hull
Harefield
Nottingham
Leicester
Cardiff
Bristol
Bart's & the London
Hammersmith
Sheffield
Norwich
Belfast
Aberdeen
Coventry
Dublin
Glasgow
Blackpool
Wythenshawe
Stoke
St Georges
St Mary's London
Manchester Royal Informary
Exeter
Guy's / St Thomas's
Kings College Hospital
Oxford
Leeds
Middlesborough
Cork
Un
it
Percentage of procedures that were VATS
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Birmingham
Brompton
Liverpool
Southampton
Edinburgh
Papworth
The Heart Hospital
Newcastle
Hull
Harefield
Nottingham
Leicester
Cardiff
Bristol
Bart's & the London
Hammersmith
Sheffield
Norwich
Belfast
Aberdeen
Coventry
Dublin
Glasgow
Blackpool
Wythenshawe
Stoke
St Georges
St Mary's London
Manchester Royal Informary
Exeter
Guy's / St Thomas's
Kings College Hospital
Oxford
Leeds
Middlesborough
Cork
Un
it
Percentage of procedures that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
56
Un
it-s
pec
ific
acti
vity
Surgery for pneumothorax
Total procedures for pneumothorax
Most surgeons are agreeable on the indications for surgical intervention for pneumothorax, i.e. persisting air leak, two or more episodes, and certain occupational groups. Nevertheless there is probably a large unmet need in pneumothorax surgery throughout the country as a whole, especially with respect to secondary pneumothorax. Guys and St Thomas’ are a clear outlier in this comparison, and presumably reflects the commitment of this Unit to providing a comprehensive pneumothorax service for patients rather than differing indications for surgery. This chart also highlights the inconsistencies in data collection and recording of activity. It is inconceivable that Wythenshawe and Exeter carried out almost no surgery for pneumothorax, but for whatever reason their data returns haven’t reflected this. Hopefully as data collection improves anomalies such as this will disappear.
Procedures for pneumothorax; financial years 2003-2005 (n=4,334)
0 100 200 300 400 500 600 700
Guy's / St Thomas's
Birmingham
Leeds
Liverpool
Harefield
Newcastle
Hull
Southampton
Brompton
Edinburgh
Cardiff
Belfast
The Heart Hospital
Sheffield
Middlesborough
St Georges
Norwich
Bart's & the London
Nottingham
Dublin
Coventry
Bristol
Blackpool
Aberdeen
Manchester Royal Informary
Leicester
Cork
Glasgow
St Mary's London
Papworth
Stoke
Kings College Hospital
Oxford
Exeter
Wythenshawe
Un
it
Number of procedures
0 100 200 300 400 500 600 700
Guy's / St Thomas's
Birmingham
Leeds
Liverpool
Harefield
Newcastle
Hull
Southampton
Brompton
Edinburgh
Cardiff
Belfast
The Heart Hospital
Sheffield
Middlesborough
St Georges
Norwich
Bart's & the London
Nottingham
Dublin
Coventry
Bristol
Blackpool
Aberdeen
Manchester Royal Informary
Leicester
Cork
Glasgow
St Mary's London
Papworth
Stoke
Kings College Hospital
Oxford
Exeter
Wythenshawe
Un
it
Number of procedures

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
57
Un
it-specifi
c activity
Open versus VATS procedures
There is a suggestion of a trend to more VATS surgery being carried out in the Units with higher activity.
VATS as a proportion of all procedures for pneumothorax; financial years 2003-2005 (n=4,334)
0% 20% 40% 60% 80% 100%
Guy's / St Thomas's
Birmingham
Leeds
Liverpool
Harefield
Newcastle
Hull
Southampton
Brompton
Edinburgh
Cardiff
Belfast
The Heart Hospital
Sheffield
Middlesborough
St Georges
Norwich
Bart's & the London
Nottingham
Dublin
Coventry
Bristol
Blackpool
Aberdeen
Manchester Royal Informary
Leicester
Cork
Glasgow
St Mary's London
Papworth
Stoke
Kings College Hospital
Oxford
Exeter
Wythenshawe
Un
it
Percentage of procedures that were VATS
0% 20% 40% 60% 80% 100%
Guy's / St Thomas's
Birmingham
Leeds
Liverpool
Harefield
Newcastle
Hull
Southampton
Brompton
Edinburgh
Cardiff
Belfast
The Heart Hospital
Sheffield
Middlesborough
St Georges
Norwich
Bart's & the London
Nottingham
Dublin
Coventry
Bristol
Blackpool
Aberdeen
Manchester Royal Informary
Leicester
Cork
Glasgow
St Mary's London
Papworth
Stoke
Kings College Hospital
Oxford
Exeter
Wythenshawe
Un
it
Percentage of procedures that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
58
Un
it-s
pec
ific
acti
vity
Mortality after procedures for pneumothorax
Mortality after open procedures for pneumonectomy; financial years 2003-2005 (n=1,200)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
5%
10%
15%
20%
25%
30%
35%
0 20 40 60 80 100 120 140
Number of procedures
Mo
rtal
ity
rate
0%
5%
10%
15%
20%
25%
30%
35%
0 20 40 60 80 100 120 140
Number of procedures
Mo
rtal
ity
rate
Mortality after VATS procedures for pneumonectomy; financial years 2003-2005 (n=3,134)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
1%
2%
3%
4%
5%
6%
7%
8%
0 100 200 300 400 500 600
Number of procedures
Mo
rtal
ity
rate
0%
1%
2%
3%
4%
5%
6%
7%
8%
0 100 200 300 400 500 600
Number of procedures
Mo
rtal
ity
rate

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
59
Un
it-specifi
c activity
Surgery for upper GI disorders
Total activity for upper GI disorders
As explained in the previous section, oesophagogastic surgery is field of reducing activity for thoracic surgery as a whole. Many Units previously very active in this area have stopped contributing altogether and the service has been absorbed by upper GI surgeons in the locality. In contrast other Units have continued their involvement and activity for �003-�005 remains as high as anywhere in the country. The organisation of this type of surgery continues to change. The Society for Cardiothoracic Surgery believes that an integrated approach to patient management, drawing on the expertise of multiple specialty groups, is the best way for optimising patient care and improving outcomes; the Association of Upper Gastrointestinal Surgeons shares this view. Thus the model of thoracic surgeons working alongside and not in competition with upper GI surgeon has to be an improved way of working; achieving this multi-disciplinary model remains a difficult goal to achieve in many parts of the country.
Total major procedures for upper GI disease;financial years 2003-2005 (n=1,775)
0 50 100 150 200 250
Nottingham
Liverpool
Exeter
Belfast
Norwich
Birmingham
Harefield
Coventry
Edinburgh
Southampton
St Georges
Hull
Papworth
Blackpool
Leeds
Guy's / St Thomas's
Aberdeen
Sheffield
Glasgow
Bristol
Leicester
Brompton
Middlesborough
Wythenshawe
The Heart Hospital
Cork
Manchester Royal Informary
Bart's & the London
Dublin
Newcastle
Stoke
Un
it
Number of procedures
0 50 100 150 200 250
Nottingham
Liverpool
Exeter
Belfast
Norwich
Birmingham
Harefield
Coventry
Edinburgh
Southampton
St Georges
Hull
Papworth
Blackpool
Leeds
Guy's / St Thomas's
Aberdeen
Sheffield
Glasgow
Bristol
Leicester
Brompton
Middlesborough
Wythenshawe
The Heart Hospital
Cork
Manchester Royal Informary
Bart's & the London
Dublin
Newcastle
Stoke
Un
it
Number of procedures

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
60
Un
it-s
pec
ific
acti
vity
As can be seen from the charts, fewer Units carry out surgery for upper GI disorders than contribute to the totality of general thoracic surgery. Some thoracic Units have contributed only very small volumes of activity in the period reported. In the field of oesophageal surgery where there is an accepted and proven relationship between hospital volume and outcome (regardless of the specialty of the operating surgeon) a very low volume of activity should probably not be sustained independently. Nevertheless, thoracic surgeons and other staff working in thoracic Units will always have particular areas of expertise which colleagues in other specialties can draw on in optimising the care of patients with all types of oesophagogastric disease.
Resections for upper GI cancer;financial years 2003-2005 (n=1,001)
0 20 40 60 80 100 120 140 160
Liverpool
Nottingham
Norwich
Coventry
Harefield
Birmingham
Exeter
Belfast
Edinburgh
Southampton
Hull
Papworth
Blackpool
St Georges
Guy's / St Thomas's
Glasgow
Leeds
Aberdeen
Wythenshawe
Brompton
Leicester
Sheffield
Newcastle
The Heart Hospital
Un
it
Number of procedures
0 20 40 60 80 100 120 140 160
Liverpool
Nottingham
Norwich
Coventry
Harefield
Birmingham
Exeter
Belfast
Edinburgh
Southampton
Hull
Papworth
Blackpool
St Georges
Guy's / St Thomas's
Glasgow
Leeds
Aberdeen
Wythenshawe
Brompton
Leicester
Sheffield
Newcastle
The Heart Hospital
Un
it
Number of procedures

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
61
Un
it-specifi
c activity
Major procedures for upper GI disorders other than cancer;financial years 2003-2005 (n=663)
0 10 20 30 40 50 60 70 80 90
Belfast
Exeter
Nottingham
Birmingham
Liverpool
Norwich
St Georges
Harefield
Edinburgh
Southampton
Leeds
Papworth
Coventry
Hull
Blackpool
Bristol
Guy's / St Thomas's
Sheffield
Aberdeen
Leicester
Middlesborough
Brompton
Cork
Glasgow
Manchester Royal Informary
The Heart Hospital
Bart's & the London
Dublin
Stoke
Un
it
Number of procedures
0 10 20 30 40 50 60 70 80 90
Belfast
Exeter
Nottingham
Birmingham
Liverpool
Norwich
St Georges
Harefield
Edinburgh
Southampton
Leeds
Papworth
Coventry
Hull
Blackpool
Bristol
Guy's / St Thomas's
Sheffield
Aberdeen
Leicester
Middlesborough
Brompton
Cork
Glasgow
Manchester Royal Informary
The Heart Hospital
Bart's & the London
Dublin
Stoke
Un
it
Number of procedures

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
6�
Un
it-s
pec
ific
acti
vity
Minimally invasive resections
Exeter is one of the most active Units in the country in this new area of practice.
VATS as a proportion of all resections for upper GI cancer;financial years 2003-2005 (n=1,001)
0% 20% 40% 60% 80% 100%
Liverpool
Nottingham
Norwich
Coventry
Harefield
Birmingham
Exeter
Belfast
Edinburgh
Southampton
Hull
Papworth
Blackpool
St Georges
Guy's / St Thomas's
Glasgow
Leeds
Aberdeen
Wythenshawe
Brompton
Leicester
Sheffield
Newcastle
The Heart Hospital
Un
it
Percentage of procedures that were VATS
0% 20% 40% 60% 80% 100%
Liverpool
Nottingham
Norwich
Coventry
Harefield
Birmingham
Exeter
Belfast
Edinburgh
Southampton
Hull
Papworth
Blackpool
St Georges
Guy's / St Thomas's
Glasgow
Leeds
Aberdeen
Wythenshawe
Brompton
Leicester
Sheffield
Newcastle
The Heart Hospital
Un
it
Percentage of procedures that were VATS

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
63
Un
it-specifi
c activity
Operative mortality
Open / close rates in upper GI surgery
Mortality after resections for upper GI cancer; financial years 2003-2005 (n=1,001)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
5%
10%
15%
20%
25%
30%
0 20 40 60 80 100 120 140
Number of procedures
Mo
rtal
ity
rate
0%
5%
10%
15%
20%
25%
30%
0 20 40 60 80 100 120 140
Number of procedures
Mo
rtal
ity
rate
Open close rates in resections for upper GI Cancer; financial years 2003-2005 (n=1,001)
Unit 99% lower alert 99.9% lower alarm
average rate 99% upper alert 99.9% upper alarm
0%
5%
10%
15%
20%
25%
30%
0 20 40 60 80 100 120 140
Number of procedures
Op
en /
clo
se r
ate
0%
5%
10%
15%
20%
25%
30%
0 20 40 60 80 100 120 140
Number of procedures
Op
en /
clo
se r
ate


Conclusions

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
66
Un
it-s
pec
ific
acti
vity
1. Sedrakyan A, van der Meulen J, Lewsey J, Treasure T. Variations in use of video assisted thoracic surgery in the United Kingdom. BMJ. �004; 329 (7473): 1011-101�.
�. Treasure T, Utley M, Bailey A. Assessment of whether in-hospital mortality for lobectomy is a useful standard for the quality of lung cancer surgery: retrospective study. BMJ. �003; 327 (7409): 73.
3. Berrisford R, Brunelli A, Rocco G, Treasure T, Utley M, audit and guidelines committee of the European Society of Thoracic Surgeons; European Association of Cardiothoracic Surgeons. The European thoracic Surgery Database project: modelling the risk of in-hospital death following lung resection. Eur J Cardiothoracic Surg. �005; 28 (2): 306-311
4. Wright CD, Edwards FH. The Society of Thoracic Surgeons general thoracic surgery database. Ann Thorac Surg. �007; 83 (2): 893-4.
References
The future of thoracic surgical data collection in the United Kingdom and IrelandIn recent years there has been a great deal of debate in the cardiac surgical community as to what type of data should be collected and to how that data could be utilised for the benefit of patients and the health professions as a whole. Thoracic surgeons have (at times somewhat thankfully!) been on the sidelines of this debate as have surgeons form other specialties and have observed the debate with some trepidation. Nevertheless, the vast majority of thoracic surgeons believe that the methods of collection of data on operative activity established over the last twenty-five years are very useful in many ways and that they should continue.
The current report is based on activity at a national and hospital level collected as a register with no patient-specific details such as age, pulmonary reserve, pathology or other factors known to impact on the outcome of an operation in terms of complications or death after surgery. The Society has agreed a dataset (see Appendix 3) to allow for a report on such issues within United Kingdom and Ireland thoracic surgical practice. This dataset is very similar to that used by other national and international organisations 3, 4, some of whom have already produced initial reports. Already a substantial number of Units in both Great Britain and Ireland have the facilities to collect information for the Society dataset, allowing for a future report with a comparable level of detail as is currently available for cardiac surgery activity.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
67
Un
it-specifi
c activity


Appendices

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
70
Ap
pen
dic
es
Appendices
Appendix 1 The Thoracic Surgical Register (1980-2002) submission form
Name of hospital
Total Deaths
A Lung tumours - Primary malignant
1 Pneumonectomy including sleeve pneumonectomy
� Lobectomy, bilobectomy
3 Sleeve resection lobectomy
4 Segmentectomy, wedge resection
5 Any pulmonary resection with resection of chest wall
6 Exploratory thoracotomy - no resection
B Lung tumours - Secondary malignant
1 Pneumonectomy including sleeve pneumonectomy
� Lobectomy, bilobectomy
3 Sleeve resection lobectomy
4 Segmentectomy, wedge resection
5 Exploratory thoracotomy - no resection
C Lung tumours - Benign i
1 Pneumonectomy
� Lobectomy, bilobectomy
3 Sleeve resection ± lobectomy
4 Segmentectomy, wedge resection
5 Exploratory thoracotomy - no resection
D1 Mesothelioma
1 Thoracotomy with insertion of pleuro-peritoneal shunt
� Thoracotomy with pleural biopsy pleurodesis
3 Thoracotomy + resection of tumour
4 Thoracotomy + resection of tumour + lung ± diaphragm
D2 Other pleural malignancy ii
1 Thoracotomy with insertion of pleuro-peritoneal shunt
� Thoracotomy with pleural biopsy ± pleurodesis
3 Thoracotomy + resection of tumour
4Thoracotomy + resection of tumour + resection of lung tissue ± diaphragm (including pleuropneumectomy)
i. Including those of intermediate malignancy e.g. carcinoid not hamartoma; see K1.
ii. Including chylothorax, but excluding empyema.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
71
Ap
pen
dices
iii. Including chylothorax, but excluding empyema.
iv. Excluding TB.
Name of hospital
Total Deaths
E Benign pleural pathology iii
1 Thoracotomy with insertion of pleuro-peritoneal shunt
� Thoracotomy with pleural biopsy ± pleurodesis
3 Thoracotomy + resection of tumour
4 Thoracotomy + resection of lung tissue (includes pleuropneumonectomy)
F Pneumothorax
1 Thoracotomy with closure of air leak (i.e. staple,glue,suture etc)
� Thoracotomy with closure of air leak + pleurodesis
3 Thoracotomy with closure of air leak + pleurectomy
4 Thoracotomy with closure of air leak + decortication
5 Thoracotomy with closure of air leak + excision of bulla or bullae
6 Tube thoracostomy and pleurectomy
7 Median sternotomy & bilateral proc's (not volume reduction surgery; see K8)
G Pleuropulmonary sepsis iv
1 Rib resection +/- open drainage ( include fenestration)
� Empyema - decortication
3 Lung abscess - resection ie segment,wedge,lobe etc.
4 Bronchiectasis - resection
5 Resection and decortication
6 Thoracoplasty
7 Tube thoracostomy and fibrinolysis
8 Pedicled muscle flap transfer for empyema
9 Closure of broncho-pleural fistula
H Tuberculosis
1 Thoracotomy and biopsy (incl.excision biopsy)
� Pulmonary resection (less than a pneumectomy)
3 Pulmonary resection i.e.pneumonectomy +/-pleura
4 Thoracoplasty
5 Pulmonary resection and thoracoplasty
6 Open pleural biopsy
7 Thoracotomy and decortication for empyema
8 Thoracotomy and resection for aspergillus

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
7�
Ap
pen
dic
es
v. Excluding TB and those specified in section H.vi. Please see cardiac register.
Name of hospital
Total Deaths
I Other inflammatory lung conditions v
1 Pneumonectomy
� Lobectomy, bilobectomy
3 Segmentectomy, wedge resection
4 Thoracotomy with biopsy (include open lung biopsy)
5 Thoracotomy for infolded lung, Blesovsky's syndrome
6 Thoracotomy for hydatid disease
J Trauma
1 Thoracotomy for haemorrhage
� Thoracotomy for lung injury
3 Thoracotomy for tracheobronchial injury
4 Thoracotomy for diaphragamatic rupture
5 Thoracotomy for cardiac injury
6 Thoracotomy for injury to aorta and or great vessels
7 Thoracotomy for fixation of rib or sternal fracture
8 Thoracotomy for endobronchial foreign body
9 Management of chest wall trauma with or without ventilatory support
10 Thoracotomy and decortication of haemothorax (delayed)
11 Thoracotomy for traumatic chylothorax
K Other lung conditions
1 Thoracotomy for hamartoma
� Thoracotomy for all lung cysts and congenital lobar emphysema
3 Thoracotomy for sequestration
4 Thoracotomy for A/V malformations
5 Thoracotomy for congenital vascular bands
6 Other specify i.e., bronchoplasty
7 Thoracotomy unilateral for lung reduction surgery
8 Median sternotomy for bilateral lung reduction surgery
9 Clamshell bilateral thoracotomy for lung reduction surgery
L Lung transplantation vi

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
73
Ap
pen
dices
vii. Excluding direct invasion by lung cancer; see A5.
viii. Excluding trauma.
Name of hospital
Total Deaths
M Chest wall conditions
1 Correction of pectus deformity
� Primary chest wall tumours
�a Chest wall etc
�b Chest wall and any lung resection
3 Secondary chest wall tumours vii
3a Excision of chest wall
3b Excision of chest wall and any lung resection
4 Excision of costal cartilage/s
5 Excision of xyphoid
6 Resection of sternum ± cartilage ± chest wall ( for primary tumour )
7 Removal of pectus bar
8 Biopsy of chest wall lesion
9 Excision of chest wall sepsis (include sternum ± cartilage, ribs etc.)
10 Surgery for cervical rib / thoracic inlet syndrome
N Diaphragmatic conditions viii
Diaphragamatic tumour
Diaphragamatic hernia, congenital
Thoracotomy and plication of diaphragm
O Mediastinal condition
1 Neurogenic tumour excision
� Foregut reduplication cysts (bronchial and oesophageal)
3 Other mediastinal cysts - specify
4 Retrosternal goitre
5 Thymoma with myasthenia
6 Thymoma without myasthenia
7 Other medistinal tumour excision - specify
8 Thymectomy for myasthenia gravis
9 Surgery for pleuro-pericardial cyst
10 Thoracotomy for thoracic duct ligation
11 Surgery for terato-dermoid of mediastinum
1� Surgery for lipoma or liposarcoma of mediastinum
13 Surgery of giant lymphoma of mediastinum
14 Surgery for mediastinal parathyroid adenoma
15 Other tumours not otherwise specified

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
74
Ap
pen
dic
es
ix. Includes carinal resection.
x. Not performed thorascopically.
Name of hospital
Total Deaths
P Trachial conditions ix
1 Tracheal tumours primary and secondary resection
� Tracheal tumours primary & secondary resection & carina (+ any lung resection)
3 Tracheal stenosis resection (acquired / benign / congenital )
4 Tracheal stenosis resection (acquired / benign / congenital ± carinal resection)
Q Other conditions (specify) x
1 Pericardial window
� Pericardectomy (also see cardiac surgery return)
3.1 Dorsal spine discectomy / decompression
3.� Spinal fusion
3.3 Excision of dorsal spine tumour
4 Dorsal sympathectomy
5 Correction of kyphoscoliosis
R Oesophageal malignant tumours
1 Oesophageal resection
� Oesophageal resection,pharynx ± larynx
3 Bypasss procedure using any conduit
4 Oesophageal resection with interpositon of colon or jejunum (not free graft)
5 Intubation pulsion (inoperable laparotomy etc)
6 Intubation traction
7 Exploration only by any route, i.e., inoperable
8 Staging laparotomy
S Oesophageal benign tumours
1 Excision without oesophagectomy
� Oesophagectomy
3 Exploration only ± biopsy
T Achlasia and other motility disorders
1 Myotomy
� Myotomy with anti-reflux operation
3 Diverticulectomy ± myotomy
U Upper sphincter disorders
1 Excision of pouch ± myotomy
� Myotomy alone with or without divertulopexy
3 Per oral stapling - DOHLMANS procedure

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
75
Ap
pen
dices
Name of hospital
Total Deaths
V1 Reflux conditions
1 Hiatus hernia repair (all techniques)
� Hiatus hernia repair with gastroplasty
3 Oesophageal resection
4 Oesophageal bypass
5 Biliary diversion
6 Circumferential myotomy
V11 Recurrent reflux conditions
1 Hiatus hernia repair (all techniques)
� Hiatus hernia repair with gastroplasty
3 Oesophageal resection
4 Oesophageal bypass
5 Biliary diversion
6 Circumferential myotomy
W Oesophageal injury
1 Thoracotomy for removal of foreign body
� Thoracotomy for perforation / spontaneous / other trauma
3 Repair of spontaneous rupture (Boerhaave's)
4 Resection of spontaneous rupture
5 Repair of instrumental perforation (rigid or flexible scope / bougie / balloon etc.)
6 Resection of instrumental perforation
7 Other specify
8 Chest drain and or local drainage (i.e., neck) + conservative treatment
X Oesophageal atresia / fistula (congenital)
1 Closure of fistula +/- defunctioning gastrotomy
� Primary anastomosis
3 Staged reconstruction using any conduit
Y Gastric conditions xi
1 Resection of any gastric malignancy - partial or total gastrectomy
� Bypass for gastric malignancy (ie linitis plastica)
3 Feeding jejunostomy or gastrostomy
4 Gastrostomy
5 Pyloroplasty (for delayed gastric emptying )
xi. Formerly other oesophageal conditions (specify).

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
76
Ap
pen
dic
es
Name of hospital
Total Deaths
Z Endoscopic section xii
Z11�0 Diagnostic bronchoscopy (includes biopsy)
Therapeutic bronchoscopy total
Z11�1 Foreign body removal
Z11�� Dilatations
Z11�3 Curettage with diathermy and / or forceps
Z11�4 Laser resections
Z11�5 Brachytherapy i.e., endobronchial radiotherapy
Z11�6 Stenting
Z11�7 Cryotherapy
Z11�8 Other
Z11�9 Glue to BPF
Upper GI endoscopies
Z1��0 Diagnostic (includes biopsy)
Therapeutic total
Z1��1 Foreign body removal
Z1��� Dilatations
Z1��3 Curettage with diathermy ± forceps
Z1��4 Laser resections
Z1��5 Brachytherapy
Z1��6 Pulsion intubation any type of stent
Mediastinal
Z13�1 Mediastinoscopy (cervical)
Z13�� Anterior mediastinotomy
Minor procedures
Z��1 Tracheostomy (standard)
Z��� Mini-tracheostomy
Z��3 Per-cutaneous tracheostomy
Z��4 Removal of sternal wires
Z��5 Intercostal drains
Z��6 Secondary resuture of any wound
xii. Not VATS; see separate section.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
77
Ap
pen
dices
Name of hospital
Total Deaths
Video Assisted Surgery (VATS); pulmonary
Wedge resection total
PU1 Lung biopsy for diffuse disease
PU� Biopsy of isolated pulmonary nodule
Resection of primary lung neoplasm total
PU3 Benign
PU4 Malignant
PU5 Resection of metastasis
Major lung resections
Lobectomy totals
LR1 Primary neoplasm
LR� Secondary neoplasm
LR3 Inflammatory disease
Pneumonectomy totals
LR4 Primary neoplasm
LR5 Secondary neoplasm
LR6 Inflammatory disease
Bullae / empyema
VB1 Bullectomy
LVR1 Lung volume reduction surgery unilateral
LVR� Lung volume reduction surgery bilateral (same anaesthetic)
Pleural
Pneumothorax total
PL1 Closure of air leak xiii + blebectomy
PL� Closure of air leak xiii + blebectomy +chemical pleurodesis
PL3 Closure of air leak xiii + blebectomy+mechanical abrasion
PL4 Closure of air leak xiii + blebectomy+pleurectomy
Pleural effusion / pleural neoplasm total
PL5 Pleural biopsy
PL6 Pleural biopsy + chemical pleurodesis ie plain or iodised talc
PL7 Pleurectomy
PL8 Drainage of empyema ± debridement
PL9 Removal of tumour
PL10 Insertion of shunt ± any procedure
xiii. Staple, stitch, glue etc.

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
78
Ap
pen
dic
es
Name of hospital
Total Deaths
Pericardial
PE1 Pericardial fenestration
PE� Excision of pericardial cyst
PE3 Pericardiectomy
Mediastinal
ME1 Mediastinal gland biopsy / staging
ME� Mediastinal tumour biopsy
ME3 Mediastinal tumour excision
ME4 Thoracic duct ligation (clip)
Trauma
TR1 Assesment of intrathoracic trauma
TR� Evacuation of haematoma ± clot
Neural
NE1 Sympathectomy
NE� Splanchnic nerve ablation
Video Assisted Surgery (VATS); oesophageal
OE1 Heller's myotomy
OE� Extended myotomy
OE3 Laparoscopic Heller's
OE4 Laparoscopic Nissen fundoplication ± repair of hiatus hernia
OE5 Laparoscopic hiatus hernia repair
OE6 Thoracoscopic mobilisation of oesophagus
OE7 Thoracoscopic / laparoscopic oesophagectomy
OE8 Repair of ruptured oesophagus
OE9 Excision of leiomyoma
OE10 Laparoscopy for staging of gastric / oesophageal cancer ± biopsy

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
79
Ap
pen
dices
Appendix 2 The Thoracic Surgical Register (2002-date) submission form
Name of hospital
Total Deaths
A Lung resections - Primary malignant
1 Pneumonectomy including sleeve pneumonectomy
� Lobectomy, bilobectomy
3 Sleeve resection lobectomy
4 Segmentectomy, wedge resection
5 Any pulmonary resection with resection of chest wall, diaphragm etc
6 Exploratory thoracotomy - no resection
B Lung resections - Other
1 Pneumonectomy
� Lobectomy, bilobectomy
3 Sleeve resection lobectomy
4 Segmentectomy, wedge resection
5 Any pulmonary resection with resection of chest wall, diaphragm etc
C Pleural procedures
1 Thoracotomy + decortication
� Thoracotomy + pleural symphysis ± closure of air leak
3 Thoracotomy + other pleural procedures
D Chest wall / diaphragmatic procedures
1 Major
� Minor
E Mediastinal
1 Resection of mediastinal mass / tumour
� Mediastinoscopy / mediastinotomy
3 Other mediastinal procedure
D Oesophageal / gastric procedures
1 Oesophago-gastric resection/bypass - malignant
� Oesophago-gastric resection/bypass - non-malignant
3 Other major oesophagogastric
4 Exploration only by any route, ie inoperable
5 Minor oesophagogastric
E Other procedures
1 Major
� Minor

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
80
Ap
pen
dic
es
Name of hospital
Total Death
VATS A Lung resections - Primary malignant
1 Wedge resection
� Lobectomy
3 Pneumonectomy
VATS B Lung resections - Other
1 Wedge resection
� Lobectomy
3 Pneumonectomy
VATS C Pleural procedures
1 Closure of air leak ± pleural symphysis
� Any other pleural procedures
VATS D Chest wall / diaphragmatic procedures
1 All
VATS E Mediastinal conditions
1 Resection of mediastinal mass / tumour
� Other mediastinal procedure
VATS F Oesophageal / gastric procedures
1 Therapeutic
� Diagnostic
VATS G Other procedures
1 All
Z Endoscopic procedures (not VATS)
1 Diagnostic bronchoscopy / oesophagoscopy
� Therapeutic bronchoscopy / oesophagoscopy

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
81
Ap
pen
dices

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
8�
Ap
pen
dic
es
Appendix 3 National minimum dataset for thoracic surgery & lung cancer surgery
Ground rules and guiding principles
The unit of entry is an operative episode, but this may include more than one procedure. Thus if the patient has any combination of
• bronchoscopy / mediastinoscopy / lung resection
• VATS / thoracotomy
the individual procedures are recorded and can be retrieved, but are within the operative episode.
There are two levels of detail
• Core data is collected on all cases.
• More detailed information is collected on lung cancer cases. In due course more detail may be collected on any subsets of interest and these may be chosen locally.
Data should be "1" for the item if applicable. There is no need for "0" or "N".
If there is date required enter in the DDMMYYYY format.
Core data
Collected on all cases; lines 1-76 and 1�4-13�
1. Centre identification
�. NHS number
3. Hospital number
4. Post code
5. Date of Birth
6. Sex
7. Date of Operation
8. Date of surgical referral
9. Date of first surgical assessment
10. No longer required
11. No longer required
Operative priority
Select a single choice from:
1�. Elective – standard booked admission for surgery
13. Urgent – decision to operate on next available list
14. Emergency – operation arranged outside scheduled list
Surgical strategy
Reasons for the operation taking place; there may be more than one:
15. Diagnostic - to diagnose the condition
16. Staging or assessment – to stage a neoplasm or to assess the progress of the condition
17. Therapeutic – to cure, alleviate or palliate
More than one is allowed, for example:
• Mediastinoscopy – maybe diagnostic and staging
• VATS pleural biopsy and pleural biopsy – diagnostic and therapeutic
• Thoracotomy, frozen section and proceed - diagnostic and therapeutic

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
83
Ap
pen
dices
Pathological category
It is the pathological category (based on what used to be called the surgical sieve) of the aetiology of the condition for which surgery is being performed. They include specific commonly occurring thoracic diagnoses. This is visited twice, at the time of the surgical procedure and again at discharge when it is revised. Multiple answers
are allowed. Enter "1" if applicable:
18. Congenital
19. Trauma / accident
�0. Primary cancer lung (known or probable)
�1. Oesophageal cancer
��. Mesothelioma
�3. Other primary thoracic malignancy
�4. Malignant disease other (secondary, recurrent or metastatic)
�5. Carcinoid
�6. Benign neoplasms
�7. Empyema (include all aetiologies of pleural sepsis)
�8. Parenchymal lung disease
�9. Vascular lesion
30. Pneumothorax
31. Pleural effusion
3�. Other
Multiple entries are allowed. You may have to deal with an empyema where the initiating problem was trauma (stabbing for example). Both are worth retrieving to count trauma and to count empyema so enter both. The data analyst can recognise that the operative episode was single.
Procedure type
Multiple entries are appropriate if performed in the same session. Select the options that best describe the operation as a whole – if there was more than one procedure, enter each. The data analyst can see that they are part of a single operative episode. The purpose of the data collected here is to indicate service volume and
workload.
33. Endoscopy; bronchoscopy / oesophagoscopy ± biopsy
34. Endoscopy; bronchoscopy / oesophagoscopy + any other procedure
35. Drain insertion
36. Other minor procedure (of the scale of node biopsies)
37. Mediastinoscopy and / or mediastinotomy
38. Other intermediate procedure (of the scale of rib resection)
39. VATS
40. Thoracotomy
41. Median sternotomy
4�. Other major incision

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
84
Ap
pen
dic
es
Primary organ / system targeted
Select the main target organ(s) of the operation. This is an anatomical list
More than one may be entered, but coincidental surgery, such as chest wall if that is purely the route of access, will not be helpful in data analysis.
43. Aorta and / or great vessels
44. Chest wall
45. Diaphragm
46. Lung
47. Mediastinum
48. Oesophagus
49. Pericardium
50. Pleura
51. Thymus
5�. Thyroid
53. Trachea and / or main bronchi
54. Other
Named operations
Select the procedure(s) performed at this operation. Thus pleural biopsy and pleurodesis can both be entered. This is not a comprehensive list but is derived from the registry list of operations performed more than about fifty or so times per annum and/or which are well defined set piece procedures.
55. Lobectomy (any indication)
56. Lobectomy (complex) with chest wall etc or bilobectomy
57. Pneumonectomy (any indication)
58. Sub lobar lung resection wedge or segmentectomy
59. Mediastinoscopy / mediastinotomy
60. Pneumothorax surgery (any technique)
61. Lung volume reduction and / or bullectomy
6�. Pleurodesis for effusion
63. Pleural biopsy (any technique)
64. Decortication
65. Oesophageal resection (any)
66. Hiatus hernia surgery (any)
67. Pectus surgery
68. Sympathectomy
69. Thymectomy for myasthenia
70. Thymectomy for thymoma
71. Thyroid surgery
7�. Bronchoscopy
73. Oesophagoscopy
74. Chest drain insertion
75. Other (enter)

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
85
Ap
pen
dices
Lung cancer data set (76-123)76. Is this operation for Lung cancer (core dataset)
If the answer is "No" proceed to Discharge section.
If the answer is "Yes" answer specialised questions for lung cancer surgery. Omit where data is not available. Do not estimate. If data are too incomplete to analyse it’s better that we know that.
Pre-operative diagnostic staging of primary lung cancer
77. CT
78. MRI
79. PET
80. Tissue diagnosis pre-operatively (includes bronchoscopic, FNA, CT needle and cytology as long as it is regarded as proof of cancer)
Histological diagnosis
81. Small cell
8�. NSCLC
83. Squamous
84. Adeno
85. Undifferentiated
86. Broncheoalveolar
87. Other or further information (write in)
Preoperative staging
88. T stage
89. N stage
90. M stage
Neoadjuvant therapy
91. Chemotherapy pre-operatively
9�. Radiotherapy pre -operatively
Pulmonary risk factors
93. Measured FEV1
94. %predicted FEV1 (an algorithm can be included to calculated this)
95. Measured FVC
96. % Predicted FVC
97. Diffusion capacity by DLCO
98. Never smoked
99. Pack years

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
86
Ap
pen
dic
es
Non-pulmonary risk factors
100. Height (the patient’s height in centimetres – enter as whole number).
101. Weight (the patient’s weight in kilograms – enter to one decimal place).
10�. Urea (mmol l-1)
103. Creatinine (mmol l-1)
104. Hb (g dl-1)
105. Insulin dependent diabetes
106. Ischaemic heart disease
107. Cardiac failure
108. Previous stroke
109. Steroid therapy
110. Anticoagulation with warfarin or equivalent therapy
111. Performance (ECOG)
11�. ASA Grade (American Society of Anaesthetists grade)
Surgical resection performed
113. Frozen section taken for diagnosis
114. Frozen section for staging
115. Left upper lobe
116. Left lower lobe
117. Right upper lobe
118. Middle lobe
119. Right lower lobe
1�0. Sublobar resection (whether wedge or segment)
pTNM staging
1�1. T stage
1��. N stage
1�3. M stage
Core data continued …
Discharge (core and lung cancer datasets)
1�4. No complications
1�5. Reintubation or ITU admission; DDMMYYYY
1�6. Date of discharge from ITU; DDMMYYYY
1�7. IPPV
1�8. Air leak >7 days
1�9. Infection requiring longer hospital stay
130. Further surgery within the same admission
131. Date of discharge / death (core dataset)
13�. Death; "Yes" or "No" (provide cause on death certificate)

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
87
Ap
pen
dices
Notes

The Society for Cardiothoracic Surgery in Great Britain & IrelandFirst National Thoracic Surgery Database Report 2008
88
Ap
pen
dic
es
Notes


The Society for Cardiothoracic Surgery
Mr Richard Page
Consultant Thoracic Surgeon
The Cardiothoracic Centre
Thomas Drive
Liverpool L14 3PE
United Kingdom
Phone +44 (0) **** *** ***
Fax +44 (0) **** *** ***
email [email protected]
Dendrite Clinical Systems
Dr Peter K.H. Walton
Managing Director
59A Bell Street
Henley-on-Thames
Oxfordshire RG9 2BA
United Kingdom
Phone +44 (0) 1491 411 288
Fax +44 (0) 1491 411 377
email [email protected]
www.e-dendrite.com